1. Introduction
In the AIEOP LH-2004 protocol’s de-escalation of chemoradiotherapy for pediatric and adolescent Hodgkin lymphoma (cHL), risk stratification for patients at higher risk of disease progression or relapse became fundamental to identify candidates for less intensive treatment. Using the current standard of care for pediatric/adolescent cHL, patients allocated to three treatment groups (TG) with both the number of cycles and the addition of radiotherapy depending on the stage, and the computed tomography and positron emission tomography (PET)-guided response assessments [
1,
2]. TG1 included stage IA or IIA without bulky mediastinal disease or pulmonary hilar lymph node involvement and less than four positive lymph node regions. TG3 included patients considered to be at Ann Arbor stage IIIB or stage IV, or bulky mediastinal disease, whatever the stage. Patients not meeting the criteria for either TG1 or TG3 were included in TG2. Patients were then sub-classified as A or B based on whether or not they had an unexplained fever (temperature above 38 °C), and/or weight loss (>10% over six months), and/or night sweats. Allocation to a TG was followed by restaging with PET/CT [
2]. Patients assigned to TG1 received three courses of ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine). Patients in TG2 received four courses of COPP (cyclophosphamide, vincristine, procarbazine, prednisone)/ABV, plus two cycles of IEP (ifosfamide, etoposide, and prednisone) for patients with a partial response (PR). Patients in TG3 received up to six courses of COPP/ABV if they achieved a complete response (CR). In the case of a PR, TG3 patients received two additional courses of IEP + RT depending on their response quality. RT was administered to the nodal regions involved, delivering from 14.4 Gy in patients who obtained a CR and 25.2 Gy in those obtaining a PR at the end of chemotherapy. Patients classified as low risk (TG1) and with a CR at the end of their chemotherapy omitted RT [
1,
3]. Although the outcomes were excellent, with a >10-year freedom-from-progression (FFP) rate of 72.18% and overall survival (OS) of 89.47% in our series, some patients’ diseases progressed or relapsed. These outcomes required that other prognostic indicators plus TG might be needed to optimize the treatment. However, at present few studies had examined molecular and laboratory parameters available at diagnosis to personalize the therapy before the interim response to therapy on PET/CT in children and adolescents with cHL.
We recently found an association between the biological factor HLA-G+3027 C>A single nucleotide polymorphism (SNP) and a shorter FFP in LH-2004 patients [
4]. In this study, considering a longer follow-up (median 6.37 instead of the previous 2.95 years) and 66 additional patients, we have developed a molecular algorithm named FPR (final prognostic rank) that combines the biological HLA-G+3027 SNP and other hematological/biochemical markers with the TG criteria. This FPR model would help clinicians in selecting the best initial treatment for their patients before PET/CT evaluation.
2. Materials and Methods
2.1. Study Cohorts
We analyzed 133 patients with HL aged 13 ± SEM 0.32 (range 3 to 18) years, treated according to the AIEOP LH-2004 between 2004 and 2017 [
1]. AIEOP’s HL Study Group, and the ethics committee at the Azienda Ospedaliera di Bologna, Policlinico San Orsola-Malpighi (n°20/2004/0) approved the study protocol. The parents or legal guardians of all patients gave written informed consent.
Ethics Statement: This study was carried out in strict accordance with the principles expressed in the Declaration of Helsinki. It was approved by the ethics committee of the Azienda Ospedaliera di Bologna, Policlinico San Orsola-Malpighi (protocol No. 20/2004/0) and by the ethics committees of all participating institutions: Centro di Riferimento Oncologico di Aviano, Prot. N°206/D; Azienda Ospedaliera Spedali Civili di Brescia, Prof. Francesco De Ferrari, seduta del 13/09/2005; Azienda U.S.L. N.8 Cagliari Prot. N°146/CE/04; Comitato di etica per la ricerca scientifica biomedica, per la buona pratica clinica e per la sperimentazione dei farmaci, Dott. Ubaldo Rosati, approved pt 12 all’O.d.g. riguardo prot LH 2004, in data 15/07/2004; Comitato etico Provinciale di Modena, Pratica n°53144/04; Servizio Sanitario Nazionale Azienda Ospedaliera di rilievo Nazionale, ”Santobono-Pausillipon” Delibera del Direttore Generale N°422 del 16.06.2005; Second universit‘a degli Studi di Napoli, Prot. N°624 del 16.12.2004; dell’Azienda di Rilievo56Nazionale e di Alta Specializzazione Ospedale Civico e Benfratelli, G.Di Cristina e57M.Ascoli—Palermo, Reg. Sper. N°56/1 del 04/05/2004; Comitato Etico Indipendente58(IRB/IEC), Prot. N°23219 del 23/09/2004; Azienda Ospedaliera Pisana Comitato di Bioetica, Studio n°1888/2005; Comitato Etico per la Sperimentazione Clinica della Provincia di Padova, codice studio CE 908P.
The inclusion criteria required biological samples for genetic analysis of HLA-G SNP, a set of hematological and biochemical parameters (i.e., erythrocyte sedimentation rate, albumin, ferritin, hemoglobin, white blood cell (WBC) count, neutrophils, eosinophils, basophils, lymphocytes, monocytes, and platelets); TG groups; World Health Organization (WHO) histological classification of HL (i.e., HD of unclassifiable subtype; MC, mixed cellularity; LRCHL, lymphocyte-rich cHL; NS, nodular sclerosis); sex; and age. Compared with our previous report on HLA-G SNP [
4], the present study concerns a median follow-up about three years longer (median 5.55 years (interquartile range (IQR) 4.09–7.93)), 66 new cases, and hematological and biochemical parameters. Among the 133 patients considered, 37 had a progressive or relapsing disease (27.8%), and 14 died (10.53%) during the follow-up period.
Table 1 reports the characteristics of the patients.
2.2. Study Design
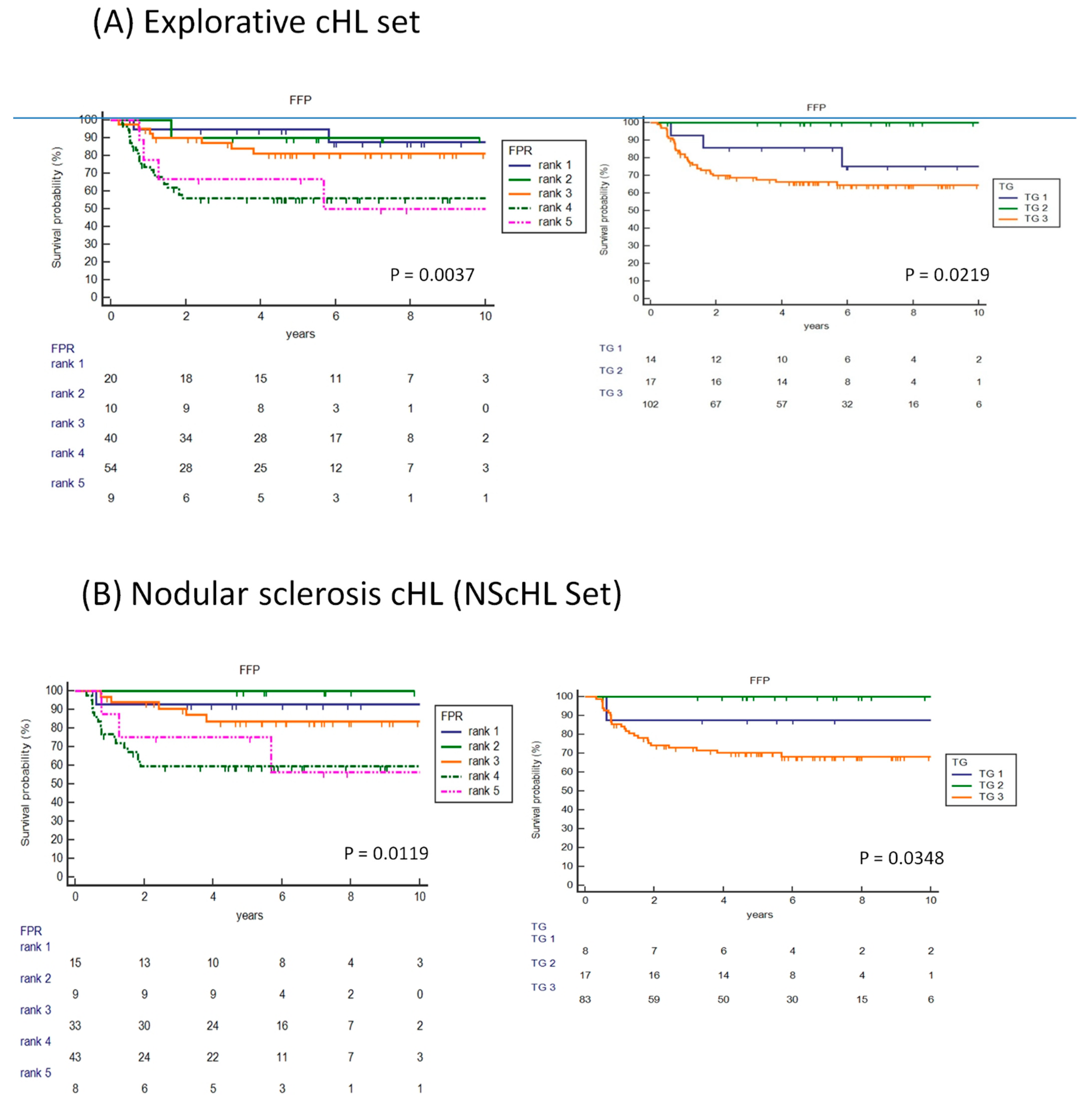
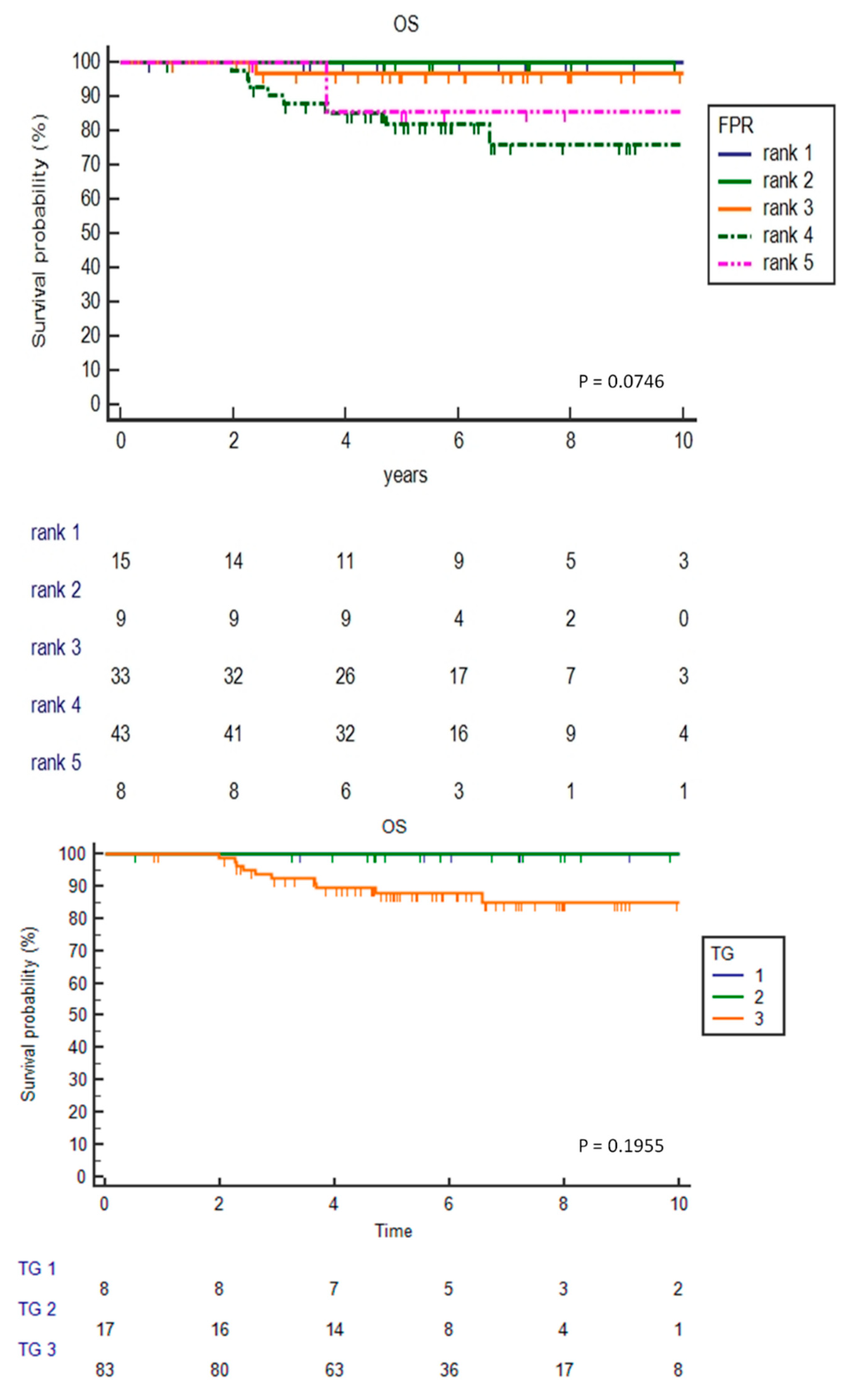
The study included four steps: (1) develop the FPR score pooling for FFP; (2) assess the FPR algorithm overall for the 133 patients with HL (explorative set) and in the 108 histological NS-restricted cHL patients (NS-set); (3) compare the assigned FPR and TG data for FFP in the explorative cHL and NScHL sets; and (4) apply the FPR scoring system to patients’ OS, and interim PET/CT response in the setting of cHL with the NS histotype.
For the first step, we performed an early comparison of receiver operating characteristic (ROC) curve analysis using age and hematological/biochemical data as variables at diagnosis to select the best condition associated with PD/R and its cutoff value corresponding to the highest chi-square.
2.3. Clinical Trial Registration Information
AIEOP’s HL Study Group, and the ethics committee at the Azienda Ospedaliera di Bologna, Policlinico San Orsola-Malpighi (n°20/2004/0) approved the study protocol.
2.4. HLA-G Genotyping
Genomic DNA was extracted from peripheral blood using the DNeasy kit (Qiagen). The 3′-UTR of the HLA-G gene was then amplified by PCR using the following specific primer 50-TGTGAAACAGCTGCCCTGTGT-30, and reverse 50-GTCTTCCATTTATTTTGTCTCT-30 [
5]. We used the Direct BigDye Terminator sequencing to sequence the amplification products. The data were analyzed using the Assign SBT software version 3.27b (Conexio Genomics, Fremantle, Australia) [
6]. For every single individual, we annotated the polymorphic sites.
2.5. Endpoints and Statistical Analysis
The primary endpoint was the period of FFP, defined as the time relapsing between the date of diagnosis and that of disease progression or relapse, or the latest follow-up for patients with no recurrent disease. Patients were stratified using TG and the FPR scoring system and used in the Kaplan–Meier analysis.
Response to therapy was defined as complete (CR) when there was no clinical, radiological (ultrasound or CT), or radio-isotopic evidence of disease after three cycles of chemotherapy (TG1) or after four cycles of chemotherapy (TG2/TG3). Complete response (CR) was defined as the absence of clinical, radiological (ultrasound and CT scan evaluation), and radio-isotopic evidence of disease. Bulky mediastinal involvement was considered in CR with a reduction of ≥75% of the volume and negative Gallium scan or 18FDG-PET. Partial response (PR) was defined as an incomplete tumor volumetric reduction. Progressive disease (PD) was defined as disease progression during first-line chemotherapy or within three months from stopping therapy. Criteria were either an increase in tumor size in previously involved sites and/or involvement of a new site. Relapse (R) was defined as a pathologically confirmed recurrence of HL after three months from stopping therapy. Patients who survived were censored at the date of their latest follow-up.
We used the Shapiro–Wilk test to check for the normality of the continuous variables distribution and the non-parametric Mann–Whitney test to see if two independent samples derived from the same population. To identify the best variables associated with PD/R, we used the comparison of ROC curves. ROC curve analysis determined the best cutoff for the variable. The laboratory/hematological variable showing the highest ROC AUC was entered in the FFP Cox’s regression model with the TG number and the HLA-G SNP, using a backward selection. In the FPR multivariate model, the hazard ratios of each variable identified the weights for each variable. Subjects in the overall samples were categorized into five risk strata (rank 1 to rank 5) using FPR total points. Kaplan–Meier analyses using the FPR ranks and TG groups showed the FFP and OS survival distribution; the chi-squared test established the FPR model efficacy for tumor response on interim PET/CT evaluation (MedCalc statistical software version 19.0.4).
2.6. Data-Sharing Statement
All patients from their parents or legal guardians gave written informed consent.
CINECA, a non-profit external consortium, collected the patient-sensitive data in a dedicated database (Professor A. Pession, protocol LH-2004, Sper. Clin. n°20/2004).
4. Discussion
In the present study, we assessed the prognostic factors and outcomes of young (<18 years old) patients with a cHL treated with the AIEOP LH2004 protocol. In addition to the TG criteria used, the proposed PRF model included two additional variables obtained at the diagnosis time: HLA-G+3027 C>A genotype and absolute neutrophil count (>8 × 109/L). These factors revealed a significant adverse prognostic value in terms of FFP, a tendency with a quite significant effect on overall survival, and a potential improvement in high-risk groups (rank 4 and rank 5) to determine the relapse during the follow-up compared to PET-scan assessment.
To our knowledge, this is the first report to highlight the value of associating a hematological factor and a biological HLA-G SNP factor with TG to guide a risk-adapted treatment. When comparing the Kaplan–Meier curves for FFP obtained using the two different models (PRF and TG), the PRF model resulted in the best predictive model in both the cHL and the NScHL sets (
Figure 2A,B). Neutrophil count >8 × 10
9/L indicates neutrophilia, a condition frequently present in cHL [
7,
8]. Neutrophilia usually increases during acute inflammation, and thus in cHL, this condition could reflect a systemic inflammatory response, which is considered an important component of tumor progression [
9,
10]. Moreover, neutrophils are involved in the immune response, as an important part of the tumor microenvironment, which plays a central role in cHL pathogenesis [
11,
12,
13]. Neutrophil counts and neutrophil/lymphocyte ratio (NLR) have been proposed as prognostic factors in several solid and hematological tumors, including adults with cHL [
14,
15,
16,
17,
18,
19,
20]. A recent study demonstrated that NLR could predict clinical outcomes in PET-negative adult patients with cHL [
21].
The pathogenic hypothesis is that the main enzymes secreted by neutrophils, in particular arginase and collagenase/gelatinase, may have a role in tumor immune escape and growth. Arginase has a potent immunosuppressive effect on tumor-infiltrating T-cells by reducing the arginine availability in the micro-ambient conditions necessary for cytotoxic T-cells function and proliferation [
8,
22,
23,
24,
25]. Gelatinase is a proteolytically active metalloproteinase (MMP) capable of degrading the extracellular matrix constituents and the basement membrane, contributing to tumor growth, angiogenesis, and metastasis [
26]. Indeed, abnormally high levels of gelatinase are reported associated with poor prognosis in several cancers [
27,
28]. Neutrophil gelatinase was also found to affects immune response in healthy donors by inducing an HLA-G+-mediate regulatory T-cell proliferation [
29].
FRP score incorporated a biological factor, i.e., the HLA-G SNP, to potentiate the TG-guided therapies. A functional role of HLA-G had yet to be demonstrated, although previously an association with cHL prognosis has been reported [
30]. The HLA-G+3027 A variant, which only occurs in the HLA-G 3′-UTR 7 haplotype, is a sequence-dependent macromolecular variant able to reduce HLA-G mRNA expression through interaction with specific cellular miRNA [
31,
32,
33,
34]. An interaction between released HLA-G molecules and their ILT leukocyte receptors present on the hematological cells had been hypothesized to produce the reduction of the cell proliferation in hematopoietic malignancy [
35,
36]. Moreover, HLA-G molecules may condition the tumor microenvironment’s nature, thus inhibiting the proliferation and activity of immune cells present in the tumor microenvironment and probably involved in the cHL growth [
37,
38]. Some sexual hormones like β-estradiol, progesterone, and prolactin as well as glucocorticoids (dexamethasone, hydrocortisone) may influence HLA-G transcription [
39,
40,
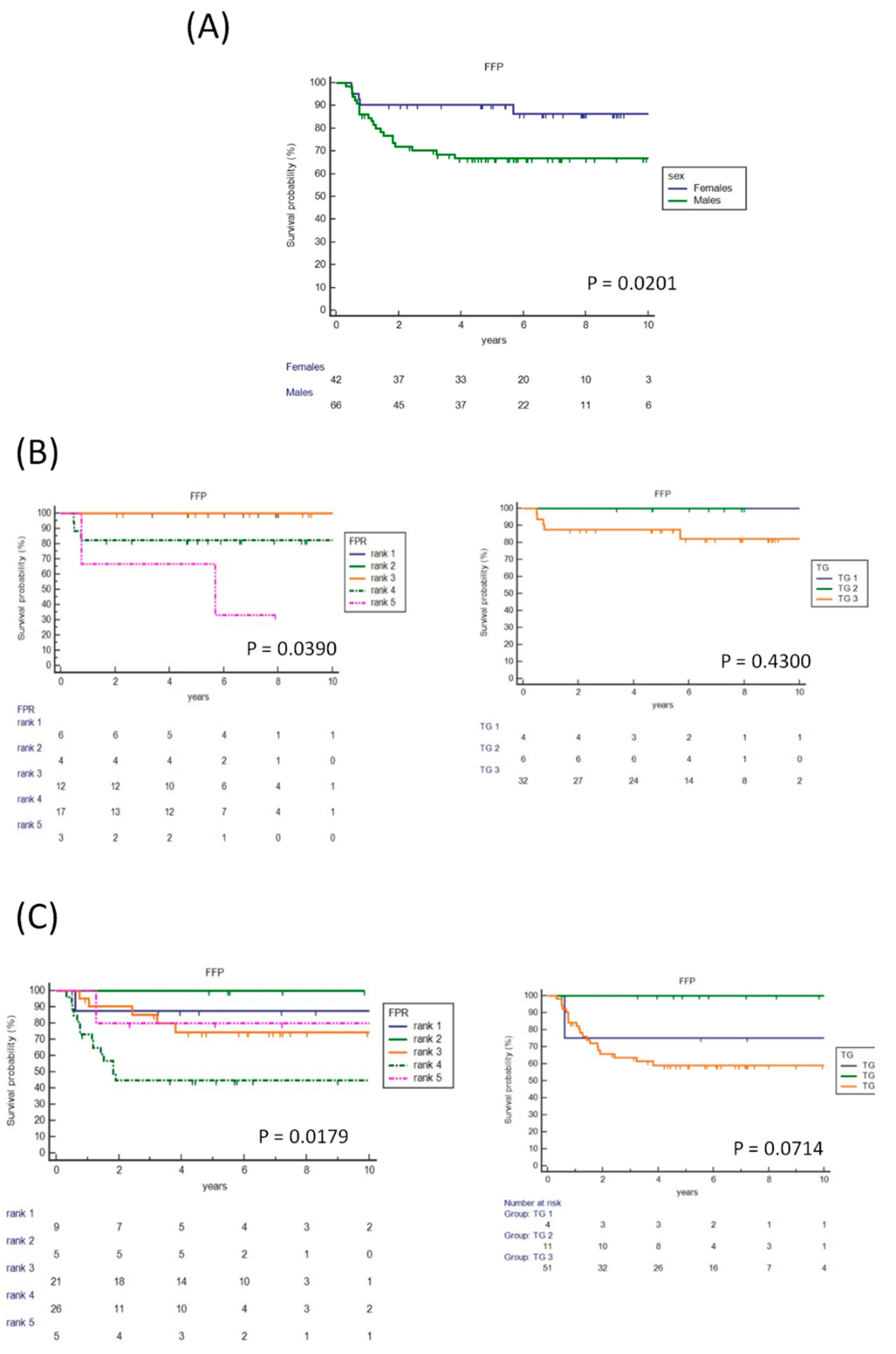
41]. Whether these hormones may induce HLA-G expression in cHL and whether they have a role in the sex-related difference in FFP survival that we found in the NScHL most-frequent histological cHL subtype (
Figure 3) are unknown and require further studies.
The FPR scoring system includes the generally used TG choice for treatment and two additional variables: a single SNP test and a minimally-invasive neutrophil count, both obtained at diagnosis from a single peripheral blood sample and quickly experimentally performed.
In our series, HLA-G SNP and neutrophil count availability may reinforce the TG assessment of patients, and could identify at diagnosis patients who may benefit from an optimized treatment before the interim PET/CT scan assessment. Indeed, the data shown in
Table 5B indicated an increase in the sensitivity (81.82%) of the FPR model to individualized patients at high risk of FFP, compared to that obtained with the PET scan (66.67%).
Although our results need to be confirmed by additional studies, they may suggest to clinicians the best treatment option before of PET/CT scan imaging, and FPR score could be used to refine treatment at the time of PET/CT stratification, with the hope of increasing the FFP time and reducing any excessive treatment.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}