
New Targets for PET Imaging of Myeloma
by
 , , , and
, , , and
Mona-Elisabeth Revheim
1,2,* ,
,
Caroline Stokke
1,3,
Jakob Nordberg Nørgaard
2,4,
Hilde Feiring Phillips
1,
Alexander Gul Sherwani
1,
Fredrik Schjesvold
4,5 and
and
James P. Connelly
1 1
Division of Radiology and Nuclear Medicine, Oslo University Hospital, P.O. Box 4950, Nydalen, 0424 Oslo, Norway
2
Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Problemveien 7, 0315 Oslo, Norway
3
Department of Physics, University of Oslo, Problemveien 7, 0315 Oslo, Norway
4
Oslo Myeloma Center, Oslo University Hospital, P.O. Box 4950, Nydalen, 0424 Oslo, Norway
5
KG Jebsen Center for B Cell Malignancies, University of Oslo, P.O. Box 4950, Nydalen, 0424 Oslo, Norway
*
Author to whom correspondence should be addressed.
Hemato 2021, 2(4), 727-738; https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040049
Submission received: 1 November 2021
/
Revised: 27 November 2021
/
Accepted: 30 November 2021
/
Published: 2 December 2021
(This article belongs to the Special Issue Current and Upcoming Diagnostics and Prognostics in Multiple Myeloma)
Abstract
:Recent advances in the treatment of multiple myeloma (MM) have increased the need for accurate diagnosis and detection of minimal residual disease (MRD), disease characterization and localization, and response evaluation and prognostication. Positron emission tomography (PET)/computed tomography (CT) imaging combines molecular and morphological information and has been shown to be especially valuable in this disease. The most frequently used PET tracer in MM is the glucose analog 18F-fluorodeoxyglucose ([18F]FDG). [18F]FDG PET/CT has a sensitivity for detection of MM between 80% to 100% and is currently the main imaging modality for assessing treatment response and for determining MRD. However, 18F-FDG PET/CT has some limitations, and imaging with alternative tracers that may overcome these constraints should be further explored. This article discusses new targets for PET/CT imaging in the assessment of MM.
1. Introduction
Multiple myeloma (MM) is a clonal B cell disorder characterized by a monoclonal plasma cell population in bone marrow with bone pain, hypercalcemia, anemia, and kidney dysfunction as clinical signs. Bone involvement is the most predominant aspect in patients with MM, and 90% of the patients develop lytic bone lesions [1].
With advances in effective treatment options for multiple myeloma (MM), many patients achieve complete response after first-line treatment, but relapse is very common. This emphasizes the need for more sensitive imaging methods for accurate diagnosis and detection of minimal residual disease (MRD) [2,3,4]. Bone marrow aspiration and biopsy are used at diagnosis and for the assessment of MRD [5,6]. Since most of MM patients have a patchy and irregular infiltration of plasma cells, such assessment based on a limited number of samples is prone to sampling errors as the biopsies may not be representative for the disease. Bone marrow aspiration and biopsy also do not identify extra-medullary spread [1,7,8]. Thus, whole body positron emission tomography-computed tomography (PET/CT) imaging based on [18F]fluorodeoxyglucose ([18F]FDG) is recommended by the International Myeloma Working Group for patchy and extramedullary disease in MM [4,9]. The sensitivity and specificity of [18F]FDG PET/CT is reported to be between 80% to 100% for the detection of both medullary and extra-medullary disease [9,10]. Moreover, [18F]FDG PET/CT predicts outcome in MM [11,12]. In patients with conventionally defined complete response after treatment, [18F]FDG PET/CT negativity has been confirmed as an independent predictor of both prolonged progression free survival (PFS) and overall survival (OS) [12,13,14]. Another study has shown that [18F]FDG PET performed before maintenance treatment was the best predictor for OS [15]. [18F]FDG PET/CT is therefore considered as the reference imaging technique for therapeutic evaluation because it can be performed much earlier than MRI, which lacks specificity [16].
Nonetheless, [18F]FDG PET/CT has several limitations. FDG is a glucose analog and there is physiological uptake in several organs including bone marrow and brain that can reduce the effectiveness of the tracer. [18F]FDG PET/CT has low sensitivity in early or diffuse bone marrow infiltration [17]. False positive lesions may be seen because of inflammation, recent use of chemotherapy, fractures and post-surgical areas, and anemia may cause a significant and diffuse increase in bone marrow uptake. Falsely negative lesions may occur in the skull due to high brain uptake, hyperglycemia, or following administration of high-dose steroids. Furthermore, hexokinase-2 (HK-2) deficiency has been suggested to explain false negativity in 10–15% of MM patients [18]. The HK-2 catalyzes the first step of glycolysis, trapping [18F]FDG in the cells. Consequently, in patients with a low expression of HK-2 [18F]FDG PET will not be an appropriate tool to evaluate MRD. On the other hand, a study by Abe et al. consisting of 90 consecutive patients found that low HK-2 expression-associated false negative [18F]FDG PET/CT was associated with relatively better prognosis in patients with newly diagnosed MM, suggesting that this phenomenon may still support the established [18F]FDG PET/CT-based prognostication [19].
Developments in nuclear medicine may offer new perspectives for MM imaging with PET, and other PET tracers may enter clinical practice and overcome some of the limitations of [18F]FDG. Several other PET tracers have been proposed in patients with MM and can be divided between established relatively non-specific tracers and novel tracers more specific for plasma cell disorders. This article discusses new targets for PET/CT imaging in the assessment of MM beyond [18F]FDG.
2. New Targets
Molecular imaging has made significant progress in the last decade and various targets for myeloma have been proposed. Lipid, amino acid, and nucleoside analogue tracers are unspecific tracers that have been used in different malignant diseases and reflect greater uptake in proliferating cells. Applying these established tracers to MM as a new indication has shown potential for a better detection rate than [18F]FDG. More recently, some specific targets for plasma cell disorders have been tested for diagnosis and therapy, e.g., using the theragnostic pair strategy where both the diagnostic tracer and therapeutic agent use the same target specific moiety but with different radionuclides (ideally radioisotopes), allowing imaging or radiotherapy. In particular the targets of chemokine receptor 4 (CXCR4) and the differentiation cluster 38 (CD38) seem promising for both diagnostics with PET and therapeutic purposes with molecular radiotherapy.
Several case reports and small studies have shown the ability to target myeloma lesions with non-FDG PET tracers, and a brief overview of radiotracers used for PET imaging in MM patients is given in Table 1.
3. Unspecific Tracers for PET Imaging in MM
3.1. Amino Acid Tracers
Amino acid tracers are particularly attractive as biomarkers, in part due to a possible mechanism of uptake in MM cells in the production of immunoglobulins. [11C]methionine is the most explored amino acid tracer, and high uptake in plasma cells has been observed [20,21].
Several small clinical studies have shown higher sensitivity in detection of focal lesions, bone marrow affection, extramedullary disease, and a more precise measurement of tumor burden and disease activity using [11C]methionine compared to [18F]FDG.
In a study from 2013, 20 patients with active plasma cell malignancy were imaged with both [18F]FDG and [11C]methionine. The uptake of [11C]methionine tended to be higher, and two patients were accurately diagnosed only with [11C]methionine. Potential upstaging was needed in six of 11 positive patients because more abnormal lesions were depicted with [11C]methionine. The patient-based sensitivity, specificity, and accuracy of [11C]methionine for restaging were reported to be 89%, 100%, and 93%, in comparison to [18F]FDG with 78%, 100%, and 86% [22]. In a later study with 78 patients from two institutions, [11C]methionine detected focal lesions in 59 patients (76%), whereas only 47 patients (60%) were detected with [18F]FDG. Accordingly, disease activity would have been missed in 12 patients. Inter-reader agreement for 11C-methionine was also higher than for [18F]FDG [23]. Reports of whole-body tumor burden and metabolism investigations are scarce for MM, but some studies performed for [18F]FDG have concluded that total metabolic tumor volume (MTV) and total lesion glycolysis (TLG) are predictive for progression-free survival and overall survival [24,25]. A study comparing MTV and TLG between [11C]methionine and [18F]FDG concluded that [11C]methionine is a more sensitive marker for the assessment of myeloma tumor burden than [18F]FDG [26]. It is evident that markers of total tumor burden—once standardized—have potential to improve the assessment performance for several tracers. In another study, 19 patients with MM (n = 18) or solitary bone plasmacytoma (n = 1) underwent both [11C]choline and [11C]methionine PET/CT. [11C]methionine demonstrated higher lesion-to-muscle ratios and detected more intramedullary MM lesions in eight patients. In 12 patients, respective tracer uptake in the iliac crest was correlated with the extent of malignant bone marrow plasma cell infiltration for both tracers [27]. These data suggest [11C]methionine PET/CT to be more sensitive than [11C]choline PET/CT for the detection of MM lesions. Unfortunately, the use of [11C]methionine is limited by a short half-life (20 min), and thus the radiopharmaceutical needs to be produced with an on-site cyclotron.
[18F]fluoro-ethyl-tyrosine ([18F]FET) is an amino acid tracer used in the diagnosis of brain tumors [28]. As for [11C]methionine, [18F]FET is taken up and incorporated into newly synthesized proteins [21]. In a study from Czyz et al. with a mixed cohort of newly diagnosed myeloma, post-therapy and post-relapse patients, 64 lesions were found using CT and 83 lesions using [18F]FET PET [29]. A low-dose CT served as a standard of reference in this study. In six patients, the number of lesions using CT and [18F]FET was the same, and two had more lesions with the [18F]FET than with the CT. Patients with both very good partial remission and complete remission had no FET-positive lesions. Fourteen out of 15 patients with active relapsed myeloma had 47 FET-positive lesions; CT assessment of the same group showed 282 lesions. For one patient, [18F]FET detected active relapse that was not seen at CT. With a half-life of 110 min for fluorine-18, a cyclotron on-site is not mandatory for [18F]FET PET/CT and can be performed in all PET/CT centers. However, the data from cell lines have shown a rather low relative uptake of [18F]FET compared to [11C]metionine and [18F]FDG, both of which surpass [18F]FET 7- to 20-fold and 3.5- to 5-fold, respectively [21].
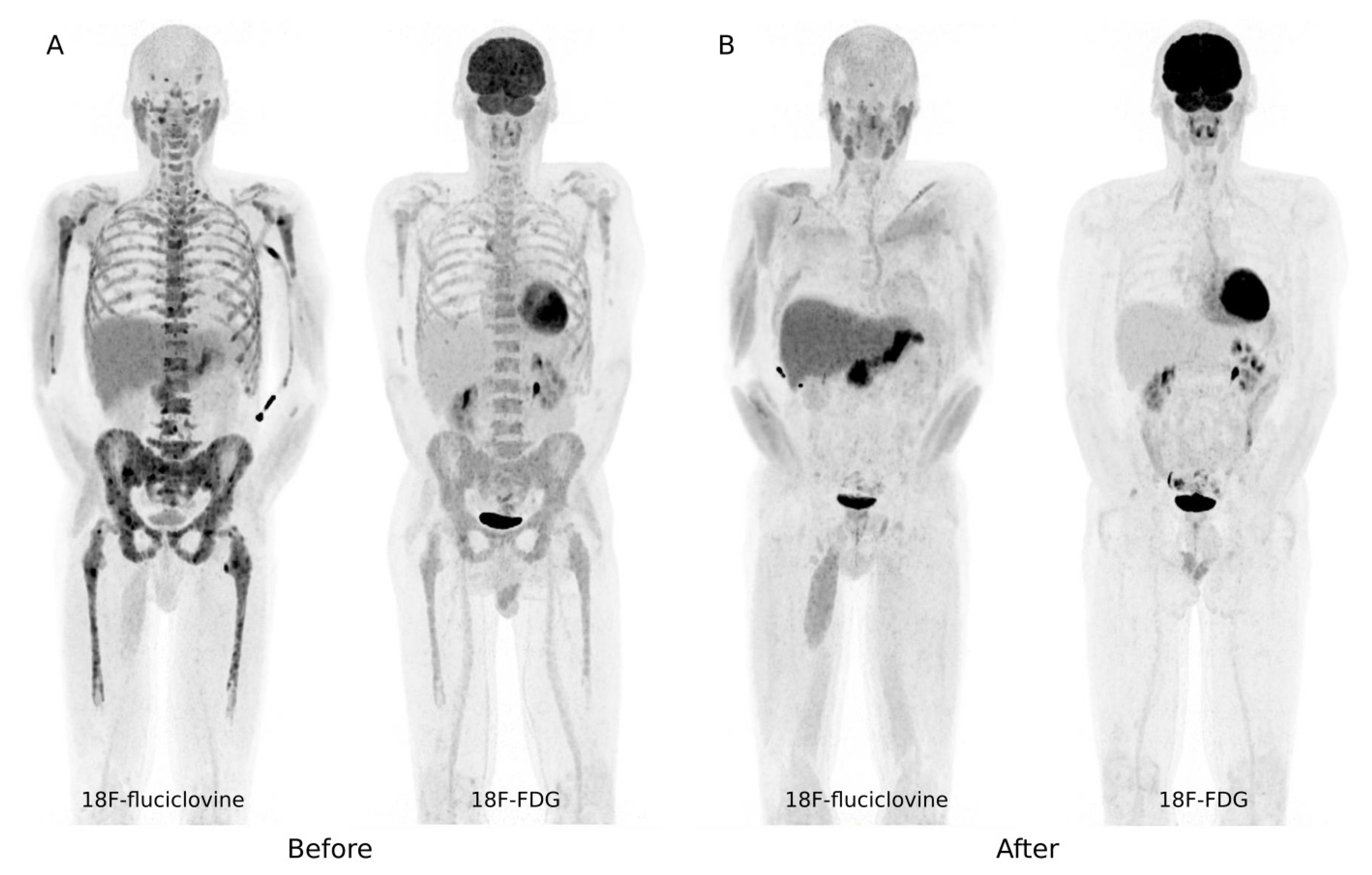
Another amino acid tracer for PET imaging of myeloma that has recently gained attraction is [18F]fluciclovine. [18F]fluciclovine is analogous to leucine [30] and has demonstrated similar uptake patterns to [11C]methionine [31]. [18F]fluciclovine is approved by the Food and Drug Administration for detection of prostate cancer recurrence in patients with elevated PSA levels [32]. In a recently presented study, [18F]fluciclovine identified a non-prostate neoplasm in 2.7% of patients with prostate cancer, including cases of MM [33]. In a prospective pilot study consisting of 13 MM patients imaged with [18F]FDG PET and [18F]fluciclovine PET/CT before and after first-line treatment with standard induction therapy and autologous stem cell transplantation (ASCT), [18F]fluciclovine showed significantly higher uptake and/or detected more lesions in seven out of 13 patients compared to [18F]FDG, and in three patients only the [18F]fluciclovine PET/CT was positive. All patients with positive [18F]fluciclovine PET/CT showed good treatment response three months after ASCT, but [18F]FDG was not able to evaluate response in four of 13 patients (Figure 1). There was a correlation between the quantitative uptake at [18F]fluciclovine PET at baseline and percentage of malignant plasma cells in local crista biopsies, but no correlation was seen between [18F]FDG uptake and percentage of malignant cells [34]. [18F]fluciclovine has the advantageous 18F halflife of 110 min compared to [11C]methionine (20 min), and thus [18F]fluciclovine may be a valuable PET amino acid tracer for MM patients in the future.
3.2. Lipid Tracers
Choline is a component of phosphatidylcholine and an indicator of the synthesis of plasma membranes. Choline can be labelled with both 11C and 18F, and “Choline PET” is used in clinical practice mainly in the diagnosis of prostate cancer. As early as 2007, Nanni et al. reported that 11C-choline appeared to be more sensitive than [18F]FDG in the detection of myeloma lesions [35]. In their pilot study consisting of 10 patients with MM, [11C]choline detected 37 bone lesions whereas [18F]FDG detected only 22 bone lesions. The uptake intensity was also higher for [11C]choline than for [18F]FDG [35]. Later, another pilot study compared [18F]fluorocholine and [18F]FDG in 21 patients with suspected relapsing or progressive multiple myeloma. Their findings were in agreement with Nanni et al., the uptake intensity was higher for [18F]fluorocholine and [18F]fluorocholine detected 75% more bone foci compared to [18F]FDG. Of note, interobserver agreement on the total number of bone foci was very high, with a kappa coefficient of 0.81 for [18F]FDG and 0.89 for [18F]fluorocholine [36].
Another lipid tracer, [11C]acetate, was originally used to study myocardial oxygen metabolism and to evaluate myocardial perfusion, and later in oncology, mainly in prostate cancer. Acetate is rapidly metabolized into acetyl-CoA in human cells. In this form it can either enter into the tricarboxylic acid cycle for the production of energy, as occurs in the myocardium, or take part in cell membrane lipid synthesis, as occurs in tumor cells. [11C]acetate PET has also shown superiority to [18F]FDG in the detection of focal and diffuse symptomatic MM. In a study of 35 patients with confirmed and untreated MM imaged with both [11C]acetate and [18F]FDG PET, [11C]acetate PET identified significantly more patients with diffuse and focal symptomatic MM and was negative in patients with indolent smoldering MM and monoclonal gammopathy of unknown significance (MGUS) [37].
A similar comparison by Lin et al. in 15 untreated MM patients before and after induction treatment confirmed the findings from Ho et al., where [11C]acetate had a higher detection rate for both diffuse and focal myeloma lesions at diagnosis than for [18F]FDG [38]. Furthermore, at staging, all 15 patients had diffuse myeloma involvement upon bone marrow examination with 30–90% of plasma cell infiltrates. Diffuse infiltration was detected in all of them (100%) using [11C]acetate with a positive correlation between bone marrow uptake values and percentages of plasma cell infiltrates (r = +0.63, p = 0.01). In contrast, a diagnosis of diffuse infiltration was detected in only six patients (40%) with [18F]FDG.
Although both [11C]choline/[18F]fluorocholine and [11C]acetete have potential in imaging MM, their use and availability have been limited. Moreover, in a recently published article by Lapa et al., [11C]methionine PET was demonstrated to be superior to [11C]choline PET. In this study of 18 patients with a history of MM and one patient with solitary bone plasmacytoma, [11C]methionine detected more intramedullary MM lesions with higher lesion to muscle ratios than [11C]choline PET [27].
3.3. Nucleoside Tracers
Nucleoside analog tracers have been explored as markers for assessing tumor growth. The uptake of such tracers are indirectly related to the rate of DNA synthesis and can reflect the high cell cycling activity [39]. Accordingly, these aspects have gained interest also in the imaging of MM, and different nucleoside analogs have been investigated in preclinical studies [40]. The nucleoside analog [18F]fluorothymidine has been suggested to be helpful in visualizing hematologic disorders including MM [39], and Okasaki et al. conducted a study comparing the nucloside analog tracer [11C]thiothymidine with the performance of [11C]methionine and [18F]FDG in 55 lytic lesions [41]. The [11C]methionine and [11C]thiothymidine reveal more positive lesions than [18F]FDG, but there were no significant differences between the [11C]methionine and [11C]thiothymidine findings. Although this study revealed better sensitivity with nucleoside analogues compared to [18F]FDG, the use of nucloside analogues seems not to have gained further foothold in imaging of MM.
3.4. Other Tracers
The bone involvement in MM has high impact on prognosis and quality of life in patients with MM. The detection and assessment of bone disease and its extent are challenging when [18F]FDG has clear limitations. The PET tracer [18F]fluoride (administrated as sodium [18F]fluoride) is deposited at the sites of micro-calcification due to physicochemical exchange of the 18F- ion with the hydroxyl group in hydroxyapatite and reflects the early phase of the calcification process. [18F]fluoride is a highly sensitive and specific radiotracer biomarker of bone remodeling [42], and a high uptake and distribution in newly diagnosed MM patients have been suggested to have prognostic significance. There are, however, somewhat divergent results in [18F]fluoride PET/CT studies for this patient population, but their methodology in the assessment of uptake and extent also differ. Zedeh et al. used an adaptive thresholding algorithm that automatically calculated the total metabolic active volume in 37 patients with suspected treatment demanding MM and found that a high metabolic active volume was associated with inferior overall survival [43]. Reports from another study with dynamic imaging of 47 untreated, symptomatic MM patients also found that a pathological uptake pattern on [18F]fluoride PET/CT had a shorter progression-free survival (PFS) compared to those with a physiological scan, but none of the PET uptake parameters were correlated to survival [44]. The same study also found only a moderate correlation between uptake parameters from [18F]fluoride with bone marrow plasma cell infiltration rate and concluded that [18F]fluoride PET probably has a limited role at least as a single-use PET approach in MM.
Methods for targeted imaging of vasculature have also been explored for imaging myeloma. VEGF 1 receptors are uniformly expressed in myeloma leading to tumor angiogenesis [45], and the antibody bevacizumab is directed to the VEGF receptor. The PET tracer [89Zr]bevacizumab has shown uptake in vascular tumors [46] and is being evaluated in an ongoing study in myeloma patients with relapse (Clinicaltrials.gov (accessed on 28 October 2021); NCT01859234). Tumor vasculature also expresses prostate-specific membrane antigen (PSMA), which is a transmembrane glycoprotein with catalytic properties, named glutamate carboxypeptidase II. PSMA is not specific for prostate cancer, but has proven useful because it is highly overexpressed in prostate cancer cells in about 95% of these patients [47,48]. PSMA can be labelled with either gallium-68 or fluorine-18 and can be imaged with PET. [68Ga]Ga-PSMA’s ability to image MM has been reported and is interesting given possible use as a theragnostic pair with, e.g., [177Lu]PSMA. However, with development of more specific and promising targets in the imaging of MM, PSMA PET may be of limited value and needs further evaluation.
4. Specific Tracers for Plasma Cell Disorders
Receptor targeting tracers and antibody targeting tracers (also referred to as immuno-PET) specific for plasma cell tumor cells are independent of metabolic processes and may provide earlier and more specific assessment of MM. These two approaches have shown great promise and are currently investigated for diagnostic and therapeutic use.
4.1. Chemokine Receptor 4
The chemokine receptor 4 (CXCR4) is a G-protein-coupled receptor expressed on hematopoietic stem and progenitor cells in the bone marrow. CXCR4 is involved in the process of cell migration and in the return of hematopoietic stem cells to the bone marrow, angiogenesis, and cell proliferation. CXCR4 expression is associated with disease progression and poor prognosis in MM [49]. Approximately two thirds of patients overexpress the receptor on the myeloma cell surface [50], and this has been shown to be correlated with progression and outcome [49]. Pentixafor is a peptide with high affinity for CXCR4, and is a very promising tracer. Pentixafor can be labelled with both gallium-68 for PET imaging and with a beta-emitting isotop, e.g., lutetium-177, for treatment.
Several studies have compared the detection rate between [68Ga]Ga-pentixafor and [18F]FDG, and the findings have been divergent. It has even been reported that in some cases [18F]FDG provided better detectability. Lapa et al. reported that in the 19 patients in whom a comparison to [18F]FDG was available, [68Ga]Ga-pentixafor PET detected more lesions in four (21%) patients while [18F]FDG was superior in seven (37%). In the remaining eight (42%) patients, both tracers detected an equal number of lesions. [18F]FDG PET positivity correlated with [68Ga]Ga-pentixafor PET positivity (p = 0.018) [51,52]. [68Ga]Ga-pentixafor PET/CT was in a later study reported to have a higher positive rate than [18F]FDG PET/CT [53], and a recently published article reported that 68Ga-[68Ga]Ga-pentixafor PET/CT was positive in 17 patients, of which 13 were also positive on [18F]FDG PET/CT, whereas seven patients were negative on both scans. A positive [68Ga]Ga-pentixafor scan was also associated with a poorer overall survival (p = 0.009) [54].
Treatment effect was obtained in a first-in-human study using CXCR4 labelled with a therapeutic radionuclide in three comprehensively pretreated MM patients with both intramedullary and extensive extramedullary disease [55]. The same research group made a follow-up study giving molecular radiotherapy with CXCR4 ([177Lu]pentixather) to eight patients with advanced stage MM and presence of extramedullary disease. The molecular radiotherapy was administered in combination with chemotherapy and ASCT. The radiotherapy was well-tolerated and exerted anti-myeloma activity [56]. Further assessment of this novel treatment option is therefore highly warranted.
Within the limitations of the small studies available, [68Ga]Ga-pentixafor PET/CT could be useful in prognostic stratification and in the selection of patients for radiotargeted therapy (as a theragnostic imaging agent), but primarily for diagnostic use the value is more questionable. Data for assessment of MRD are missing.
4.2. Immuno-PET Targeting Specific Antigens
Immuno-PET imaging is a novel method to assess targeting of specific antigens by therapeutic antibodies [57]. The increased use of therapeutics targeting clusters of differentiation (CD) antigens in clinical practice has helped drive the evolution of immuno-PET. Although [18F]FDG PET provides prognostic information and is valuable in monitoring therapy response, FDG is non-specific and is not necessarily optimal in assessing treatment response to particular immunotherapeutic agents. Imaging with targeted agents may more precisely assess the response to therapy based on the specific targeted mechanism.
Different integrins have been investigated for PET imaging of MM with various results [58,59,60]. The transmembrane integrin receptor very-late antigen 4 (VLA-4) is associated with angiogenesis, metastasis, and resistance to chemotherapy [61,62]. Currently, there is special interest in the integrins α4β1 (VLA-4) and α4β7 as they seem to have important functions in MM cells. Recently, it was reported that that integrin α4β7 constitutively adopts an active conformation in MM cells, and chimeric antigen receptor (CAR) T cell therapy that targets the activated conformation of integrin β7 may also be a promising new treatment for relapsed or refractory MM [63,64]. If so, PET imaging targeting α4β7 may play an important role in the future.
All multiple myeloma cells express the transmembrane glycoprotein CD38, which is the direct target of immunotherapy with Daratumumab. Daratumumab has been labelled with a positron emitter such as Zirconium-89 or Copper-64 and serves as an ideal PET tracer for MM imaging [57,65]. The most recently published study performed in xenograft animal models together with the first-in-human phase I study in six patients demonstrated a high ability to detect myeloma lesions with [89Zr]-DFO-daratumumab PET/CT [66]. One of the patients imaged with PET/CT from this study is shown in Figure 2. Using [89Zr]-DFO-daratumumab PET/CT may offer opportunities for future clinical trials with measurement of disease burden, evaluation of MRD, and prediction of daratumumab therapy response. Similar to CXCR4, there is also the opportunity for molecular radiotherapy by use of daratumumab as a targeting agent and substituting the position emitter by a therapeutic radionuclide. Preclinical investigations of different emitters have been initiated [67,68]. Although there are promising results from the first-in-human phase 1 study, further prospective studies are needed to define the role of this CD38 targeted PET/CT.
All things considered, specific tracers for plasma cell disorders appear to hold great potential for early diagnosis and in identifying patients who could benefit from different targeted therapies and immunotherapy. Such strategies open a new area in PET imaging and molecular radiotherapy for MM patients with the potential to target many other receptors and antigens highly expressed in MM cells.
5. Conclusions
The therapeutic advances have fundamentally changed the management of MM over recent years, and imaging techniques able to match them are essential. Many patients now achieve traditionally defined complete response after first-line treatment, but relapse is frequent. It is therefore of special importance to improve the initial prognostic stratification and to detect MRD after treatment. Even though new targets for PET/CT imaging in the assessment of MM appear to have potential, there is no conclusive data for the superiority over [18F]FDG in evaluation of treatment response, especially for MRD assessment in clinical practice. However, considering the small patient populations included in studies testing novel targets, their results must be interpreted with caution. Future prospective studies with a larger number of subjects are needed to assess their clinical utility. Other factors of importance are tumor heterogeneity and inter-patient variations, with the result that one tracer may not be suitable for all patients.
Future developments for PET imaging in MM depend on convergence of understanding of the disease and tracer properties that can be achieved through closer collaboration between hematologists and nuclear medicine physicians and well constructed clinical trials.
Author Contributions
M.-E.R. conceived the idea and co-wrote the manuscript. All authors (C.S., J.N.N., F.S., H.F.P., A.G.S., J.P.C.) contributed to the writing and editing of the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Revheim: South-Eastern Norway Regional Health Authority: Research Funding, 2019005. Nørgaard: Bayer: Honoraria; AstraZeneca: Honoraria. Schjesvold: Amgen, Celgene, Janssen, MSD, Novartis, Oncopeptides, Sanofi, Takeda: Consultancy; Celgene, Amgen, Janssen, Oncopeptides: Research Funding; Amgen, Celgene, Janssen, MSD, Novartis, Oncopeptides, Sanofi, SkyliteDX, Takeda: Honoraria.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interests.
References
- Albagoush, S.A.; Azevedo, A.M. Multiple Myeloma. In StatPearls; StatPearls Publishing Copyright © 2021; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Kumar, S.; Paiva, B.; Anderson, K.C.; Durie, B.; Landgren, O.; Moreau, P.; Munshi, N.; Lonial, S.; Blade, J.; Mateos, M.V.; et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet. Oncol. 2016, 17, e328–e346. [Google Scholar] [CrossRef]
- Munshi, N.C.; Avet-Loiseau, H.; Rawstron, A.C.; Owen, R.G.; Child, J.A.; Thakurta, A.; Sherrington, P.; Samur, M.K.; Georgieva, A.; Anderson, K.C.; et al. Association of Minimal Residual Disease With Superior Survival Outcomes in Patients With Multiple Myeloma: A Meta-analysis. JAMA Oncol. 2017, 3, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Hillengass, J.; Usmani, S.; Rajkumar, S.V.; Durie, B.G.M.; Mateos, M.V.; Lonial, S.; Joao, C.; Anderson, K.C.; García-Sanz, R.; Riva, E.; et al. International myeloma working group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet. Oncol. 2019, 20, e302–e312. [Google Scholar] [CrossRef]
- Paiva, B.; van Dongen, J.J.; Orfao, A. New criteria for response assessment: Role of minimal residual disease in multiple myeloma. Blood 2015, 125, 3059–3068. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.C.; Auclair, D.; Adam, S.J.; Agarwal, A.; Anderson, M.; Avet-Loiseau, H.; Bustoros, M.; Chapman, J.; Connors, D.E.; Dash, A.; et al. Minimal Residual Disease in Myeloma: Application for Clinical Care and New Drug Registration. Clin. Cancer Res. 2021, 27, 5195–5212. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.; Barlogie, B.; Haessler, J.; Tricot, G.; Anaissie, E.; Shaughnessy, J.D., Jr.; Epstein, J.; van Hemert, R.; Erdem, E.; Hoering, A.; et al. Magnetic resonance imaging in multiple myeloma: Diagnostic and clinical implications. J. Clin. Oncol. 2007, 25, 1121–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bladé, J.; de Larrea, C.F.; Rosiñol, L. Extramedullary involvement in multiple myeloma. Haematologica 2012, 97, 1618–1619. [Google Scholar] [CrossRef]
- Cavo, M.; Terpos, E.; Nanni, C.; Moreau, P.; Lentzsch, S.; Zweegman, S.; Hillengass, J.; Engelhardt, M.; Usmani, S.Z.; Vesole, D.H.; et al. Role of 18F-FDG PET/CT in the diagnosis and management of multiple myeloma and other plasma cell disorders: A consensus statement by the International Myeloma Working Group. Lancet. Oncol. 2017, 18, e206–e217. [Google Scholar] [CrossRef]
- Lu, Y.Y.; Chen, J.H.; Lin, W.Y.; Liang, J.A.; Wang, H.Y.; Tsai, S.C.; Kao, C.H. FDG PET or PET/CT for detecting intramedullary and extramedullary lesions in multiple Myeloma: A systematic review and meta-analysis. Clin. Nucl. Med. 2012, 37, 833–837. [Google Scholar] [CrossRef] [PubMed]
- Michaud-Robert, A.V.; Zamagni, E.; Carlier, T.; Bailly, C.; Jamet, B.; Touzeau, C.; Moreau, P.; Kraeber-Bodere, F.; Nanni, C.; Bodet-Milin, C. Glucose Metabolism Quantified by SUVmax on Baseline FDG-PET/CT Predicts Survival in Newly Diagnosed Multiple Myeloma Patients: Combined Harmonized Analysis of Two Prospective Phase III Trials. Cancers 2020, 12, 2532. [Google Scholar] [CrossRef] [PubMed]
- Zamagni, E.; Nanni, C.; Dozza, L.; Carlier, T.; Bailly, C.; Tacchetti, P.; Versari, A.; Chauvie, S.; Gallamini, A.; Gamberi, B.; et al. Standardization of 18F-FDG-PET/CT According to Deauville Criteria for Metabolic Complete Response Definition in Newly Diagnosed Multiple Myeloma. J. Clin. Oncol. 2021, 39, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Zamagni, E.; Patriarca, F.; Nanni, C.; Zannetti, B.; Englaro, E.; Pezzi, A.; Tacchetti, P.; Buttignol, S.; Perrone, G.; Brioli, A.; et al. Prognostic relevance of 18F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation. Blood 2011, 118, 5989–5995. [Google Scholar] [CrossRef] [Green Version]
- Moreau, P.; Attal, M.; Karlin, L.; Garderet, L.; Facon, T.; Macro, M.; Benboubker, L.; Caillot, D.; Escoffre, M.; Stoppa, A.M.; et al. Prospective Evaluation of MRI and PET-CT at Diagnosis and before Maintenance Therapy in Symptomatic Patients with Multiple Myeloma Included in the IFM/DFCI 2009 Trial. Blood 2015, 126, 395. [Google Scholar] [CrossRef]
- Moreau, P.; Attal, M.; Caillot, D.; Macro, M.; Karlin, L.; Garderet, L.; Facon, T.; Benboubker, L.; Escoffre-Barbe, M.; Stoppa, A.M.; et al. Prospective Evaluation of Magnetic Resonance Imaging and [18F]Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography at Diagnosis and Before Maintenance Therapy in Symptomatic Patients With Multiple Myeloma Included in the IFM/DFCI 2009 Trial: Results of the IMAJEM Study. J. Clin. Oncol. 2017, 35, 2911–2918. [Google Scholar] [CrossRef] [PubMed]
- Weng, W.W.; Dong, M.J.; Zhang, J.; Yang, J.; Xu, Q.; Zhu, Y.J.; Liu, N.H. A systematic review of MRI, scintigraphy, FDG-PET and PET/CT for diagnosis of multiple myeloma related bone disease—Which is best? Asian Pac. J. Cancer Prev. 2014, 15, 9879–9884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamagni, E.; Nanni, C.; Patriarca, F.; Englaro, E.; Castellucci, P.; Geatti, O.; Tosi, P.; Tacchetti, P.; Cangini, D.; Perrone, G.; et al. A prospective comparison of 18F-fluorodeoxyglucose positron emission tomography-computed tomography, magnetic resonance imaging and whole-body planar radiographs in the assessment of bone disease in newly diagnosed multiple myeloma. Haematologica 2007, 92, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Rasche, L.; Angtuaco, E.; McDonald, J.E.; Buros, A.; Stein, C.; Pawlyn, C.; Thanendrarajan, S.; Schinke, C.; Samant, R.; Yaccoby, S.; et al. Low expression of hexokinase-2 is associated with false-negative FDG-positron emission tomography in multiple myeloma. Blood 2017, 130, 30–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abe, Y.; Ikeda, S.; Kitadate, A.; Narita, K.; Kobayashi, H.; Miura, D.; Takeuchi, M.; O’Uchi, E.; O’Uchi, T.; Matsue, K. Low hexokinase-2 expression-associated false-negative 18F-FDG PET/CT as a potential prognostic predictor in patients with multiple myeloma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1345–1350. [Google Scholar] [CrossRef]
- Dankerl, A.; Liebisch, P.; Glatting, G.; Friesen, C.; Blumstein, N.M.; Kocot, D.; Wendl, C.; Bunjes, D.; Reske, S.N. Multiple Myeloma: Molecular Imaging with 11C-Methionine PET/CT—Initial Experience. Radiology 2007, 242, 498–508. [Google Scholar] [CrossRef] [PubMed]
- Luckerath, K.; Lapa, C.; Spahmann, A.; Jorg, G.; Samnick, S.; Rosenwald, A.; Einsele, H.; Knop, S.; Buck, A.K. Targeting paraprotein biosynthesis for non-invasive characterization of myeloma biology. PLoS ONE 2013, 8, e84840. [Google Scholar] [CrossRef]
- Nakamoto, Y.; Kurihara, K.; Nishizawa, M.; Yamashita, K.; Nakatani, K.; Kondo, T.; Takaori-Kondo, A.; Togashi, K. Clinical value of 11C-methionine PET/CT in patients with plasma cell malignancy: Comparison with 18F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Lapa, C.; Garcia-Velloso, M.J.; Luckerath, K.; Samnick, S.; Schreder, M.; Otero, P.R.; Schmid, J.S.; Herrmann, K.; Knop, S.; Buck, A.K.; et al. 11C-Methionine-PET in Multiple Myeloma: A Combined Study from Two Different Institutions. Theranostics 2017, 7, 2956–2964. [Google Scholar] [CrossRef]
- McDonald, J.E.; Kessler, M.M.; Gardner, M.W.; Buros, A.F.; Ntambi, J.A.; Waheed, S.; van Rhee, F.; Zangari, M.; Heuck, C.J.; Petty, N.; et al. Assessment of Total Lesion Glycolysis by 18F FDG PET/CT Significantly Improves Prognostic Value of GEP and ISS in Myeloma. Clin. Cancer Res. 2017, 23, 1981–1987. [Google Scholar] [CrossRef] [Green Version]
- Fonti, R.; Pellegrino, S.; Catalano, L.; Pane, F.; Del Vecchio, S.; Pace, L. Visual and volumetric parameters by 18F-FDG-PET/CT: A head to head comparison for the prediction of outcome in patients with multiple myeloma. Ann. Hematol. 2020, 99, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Morales-Lozano, M.I.; Viering, O.; Samnick, S.; Rodriguez-Otero, P.; Buck, A.K.; Marcos-Jubilar, M.; Rasche, L.; Prieto, E.; Kortum, K.M.; San-Miguel, J.; et al. 18F-FDG and 11C-Methionine PET/CT in Newly Diagnosed Multiple Myeloma Patients: Comparison of Volume-Based PET Biomarkers. Cancers 2020, 12, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapa, C.; Kircher, M.; Da Via, M.; Schreder, M.; Rasche, L.; Kortum, K.M.; Einsele, H.; Buck, A.K.; Hanscheid, H.; Samnick, S. Comparison of 11C-Choline and 11C-Methionine PET/CT in Multiple Myeloma. Clin. Nucl. Med. 2019, 44, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Floeth, F.W.; Sabel, M.; Stoffels, G.; Pauleit, D.; Hamacher, K.; Steiger, H.J.; Langen, K.J. Prognostic value of 18F-fluoroethyl-L-tyrosine PET and MRI in small nonspecific incidental brain lesions. J. Nucl. Med. 2008, 49, 730–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czyz, J.; Malkowski, B.; Jurczyszyn, A.; Grzasko, N.; Lopatto, R.; Olejniczak, M.; Czyz, A.; Jachalska, A. 18F-fluoro-ethyl-tyrosine (18F-FET) PET/CT as a potential new diagnostic tool in multiple myeloma: A preliminary study. Contemp. Oncol. 2019, 23, 23–31. [Google Scholar] [CrossRef]
- Shoup, T.M.; Olson, J.; Hoffman, J.M.; Votaw, J.; Eshima, D.; Eshima, L.; Camp, V.M.; Stabin, M.; Votaw, D.; Goodman, M.M. Synthesis and evaluation of [18F]1-amino-3-fluorocyclobutane-1-carboxylic acid to image brain tumors. J. Nucl. Med. 1999, 40, 331–338. [Google Scholar] [PubMed]
- Ono, M.; Oka, S.; Okudaira, H.; Schuster, D.M.; Goodman, M.M.; Kawai, K.; Shirakami, Y. Comparative evaluation of transport mechanisms of trans-1-amino-3-[18F]fluorocyclobutanecarboxylic acid and L-[methyl-(1)(1)C]methionine in human glioma cell lines. Brain Res. 2013, 1535, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Seierstad, T.; Hole, K.H.; Tulipan, A.J.; Stromme, H.; Lilleby, W.; Revheim, M.E.; Hernes, E. 18F-Fluciclovine PET for Assessment of Prostate Cancer with Histopathology as Reference Standard: A Systematic Review. PET Clin. 2021, 16, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Parihar, A.S.; Schmidt, L.R.; Dehdashti, F.; Wahl, R.L. Detection of additional primary neoplasms on 18F-Fluciclovine PET/CT in patients with primary prostate cancer. J. Nucl. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Revheim, M.E.; Nørgaard, J.N.; Phillips, H.F.; Sherwani, A.; Nuruddin, S.; Connelly, J.P.; Schjesvold, F.; Stokke, C. Amino Acid-Based Fluciclovine PET/CT Detection of Multiple Myeloma. In Proceedings of the 62nd ASH Annual Meeting and Exposition, abstract number 3177. Virtual, USA, 5–8 December 2020. [Google Scholar]
- Nanni, C.; Zamagni, E.; Cavo, M.; Rubello, D.; Tacchetti, P.; Pettinato, C.; Farsad, M.; Castellucci, P.; Ambrosini, V.; Montini, G.C.; et al. 11C-choline vs. 18F-FDG PET/CT in assessing bone involvement in patients with multiple myeloma. World J. Surg. Oncol. 2007, 5, 68. [Google Scholar] [CrossRef] [Green Version]
- Cassou-Mounat, T.; Balogova, S.; Nataf, V.; Calzada, M.; Huchet, V.; Kerrou, K.; Devaux, J.Y.; Mohty, M.; Talbot, J.N.; Garderet, L. 18F-fluorocholine versus 18F-fluorodeoxyglucose for PET/CT imaging in patients with suspected relapsing or progressive multiple myeloma: A pilot study. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1995–2004. [Google Scholar] [CrossRef]
- Ho, C.L.; Chen, S.; Leung, Y.L.; Cheng, T.; Wong, K.N.; Cheung, S.K.; Liang, R.; Chim, C.S. 11C-acetate PET/CT for metabolic characterization of multiple myeloma: A comparative study with 18F-FDG PET/CT. J. Nucl. Med. 2014, 55, 749–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.; Ho, C.L.; Ng, S.H.; Wang, P.N.; Huang, Y.; Lin, Y.C.; Tang, T.C.; Tsai, S.F.; Rahmouni, A.; Yen, T.C. 11C-acetate as a new biomarker for PET/CT in patients with multiple myeloma: Initial staging and postinduction response assessment. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Agool, A.; Schot, B.W.; Jager, P.L.; Vellenga, E. 18F-FLT PET in hematologic disorders: A novel technique to analyze the bone marrow compartment. J. Nucl. Med. 2006, 47, 1592–1598. [Google Scholar] [PubMed]
- Hovhannisyan, N.; Dhilly, M.; Fidalgo, M.; Fillesoye, F.; Guillouet, S.; Sola, B.; Barré, L. [18F]Fludarabine-PET in a murine model of multiple myeloma. PLoS ONE 2017, 12, e0177125. [Google Scholar] [CrossRef] [Green Version]
- Okasaki, M.; Kubota, K.; Minamimoto, R.; Miyata, Y.; Morooka, M.; Ito, K.; Ishiwata, K.; Toyohara, J.; Inoue, T.; Hirai, R.; et al. Comparison of 11C-4’-thiothymidine, 11C-methionine, and 18F-FDG PET/CT for the detection of active lesions of multiple myeloma. Ann. Nucl. Med. 2015, 29, 224–232. [Google Scholar] [CrossRef] [Green Version]
- Czernin, J.; Satyamurthy, N.; Schiepers, C. Molecular mechanisms of bone 18F-NaF deposition. J. Nucl. Med. 2010, 51, 1826–1829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zadeh, M.Z.; Seraj, S.M.; Østergaard, B.; Mimms, S.; Raynor, W.Y.; Aly, M.; Borja, A.J.; Arani, L.S.; Gerke, O.; Werner, T.J.; et al. Prognostic significance of 18F-sodium fluoride in newly diagnosed multiple myeloma patients. Am. J. Nucl. Med. Mol. Imaging 2020, 10, 151–160. [Google Scholar] [PubMed]
- Sachpekidis, C.; Kopp-Schneider, A.; Merz, M.; Jauch, A.; Raab, M.S.; Goldschmidt, H.; Dimitrakopoulou-Strauss, A. Can 18F-NaF PET/CT before Autologous Stem Cell Transplantation Predict Survival in Multiple Myeloma? Cancers 2020, 12, 1335. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Witzig, T.E.; Timm, M.; Haug, J.; Wellik, L.; Fonseca, R.; Greipp, P.R.; Rajkumar, S.V. Expression of VEGF and its receptors by myeloma cells. Leukemia 2003, 17, 2025–2031. [Google Scholar] [CrossRef] [Green Version]
- Oosting, S.F.; Brouwers, A.H.; van Es, S.C.; Nagengast, W.B.; Oude Munnink, T.H.; Lub-de Hooge, M.N.; Hollema, H.; de Jong, J.R.; de Jong, I.J.; de Haas, S.; et al. 89Zr-bevacizumab PET visualizes heterogeneous tracer accumulation in tumor lesions of renal cell carcinoma patients and differential effects of antiangiogenic treatment. J. Nucl. Med. 2015, 56, 63–69. [Google Scholar] [CrossRef] [Green Version]
- van Es, S.C.; Brouwers, A.H.; Mahesh, S.V.K.; Leliveld-Kors, A.M.; de Jong, I.J.; Lub-de Hooge, M.N.; de Vries, E.G.E.; Gietema, J.A.; Oosting, S.F. 89Zr-Bevacizumab PET: Potential Early Indicator of Everolimus Efficacy in Patients with Metastatic Renal Cell Carcinoma. J. Nucl. Med. 2017, 58, 905–910. [Google Scholar] [CrossRef] [Green Version]
- Sasikumar, A.; Joy, A.; Pillai, M.R.; Nanabala, R.; Thomas, B. 68Ga-PSMA PET/CT Imaging in Multiple Myeloma. Clin. Nucl. Med. 2017, 42, e126–e127. [Google Scholar] [CrossRef] [PubMed]
- Vande Broek, I.; Leleu, X.; Schots, R.; Facon, T.; Vanderkerken, K.; Van Camp, B.; Van Riet, I. Clinical significance of chemokine receptor (CCR1, CCR2 and CXCR4) expression in human myeloma cells: The association with disease activity and survival. Haematologica 2006, 91, 200–206. [Google Scholar] [PubMed]
- Philipp-Abbrederis, K.; Herrmann, K.; Knop, S.; Schottelius, M.; Eiber, M.; Luckerath, K.; Pietschmann, E.; Habringer, S.; Gerngross, C.; Franke, K.; et al. In vivo molecular imaging of chemokine receptor CXCR4 expression in patients with advanced multiple myeloma. EMBO Mol. Med. 2015, 7, 477–487. [Google Scholar] [CrossRef]
- Lapa, C.; Luckerath, K.; Kircher, S.; Hanscheid, H.; Grigoleit, G.U.; Rosenwald, A.; Stolzenburg, A.; Kropf, S.; Einsele, H.; Wester, H.J.; et al. Potential influence of concomitant chemotherapy on CXCR4 expression in receptor directed endoradiotherapy. Br. J. Haematol. 2019, 184, 440–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapa, C.; Schreder, M.; Schirbel, A.; Samnick, S.; Kortum, K.M.; Herrmann, K.; Kropf, S.; Einsele, H.; Buck, A.K.; Wester, H.J.; et al. [68Ga]Pentixafor-PET/CT for imaging of chemokine receptor CXCR4 expression in multiple myeloma—Comparison to [18F]FDG and laboratory values. Theranostics 2017, 7, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Cao, X.; Luo, Y.; Li, J.; Feng, J.; Li, F. Chemokine receptor-4 targeted PET/CT with 68Ga-Pentixafor in assessment of newly diagnosed multiple myeloma: Comparison to 18F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Kuyumcu, S.; Isik, E.G.; Tiryaki, T.O.; Has-Simsek, D.; Sanli, Y.; Buyukkaya, F.; Ozkan, Z.G.; Kalayoglu-Besisik, S.; Unal, S.N. Prognostic significance of 68Ga-Pentixafor PET/CT in multiple myeloma recurrence: A comparison to 18F-FDG PET/CT and laboratory results. Ann. Nucl. Med. 2021, 35, 1147–1156. [Google Scholar] [CrossRef]
- Herrmann, K.; Schottelius, M.; Lapa, C.; Osl, T.; Poschenrieder, A.; Hanscheid, H.; Luckerath, K.; Schreder, M.; Bluemel, C.; Knott, M.; et al. First-in-Human Experience of CXCR4-Directed Endoradiotherapy with 177Lu- and 90Y-Labeled Pentixather in Advanced-Stage Multiple Myeloma with Extensive Intra- and Extramedullary Disease. J. Nucl. Med. 2016, 57, 248–251. [Google Scholar] [CrossRef] [Green Version]
- Lapa, C.; Herrmann, K.; Schirbel, A.; Hanscheid, H.; Luckerath, K.; Schottelius, M.; Kircher, M.; Werner, R.A.; Schreder, M.; Samnick, S.; et al. CXCR4-directed endoradiotherapy induces high response rates in extramedullary relapsed Multiple Myeloma. Theranostics 2017, 7, 1589–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandit-Taskar, N. Functional Imaging Methods for Assessment of Minimal Residual Disease in Multiple Myeloma: Current Status and Novel ImmunoPET Based Methods. Semin. Hematol. 2018, 55, 22–32. [Google Scholar] [CrossRef]
- Withofs, N.; Cousin, F.; De Prijck, B.; Bonnet, C.; Hustinx, R.; Gambhir, S.S.; Beguin, Y.; Caers, J. A First Report on [18F]FPRGD2 PET/CT Imaging in Multiple Myeloma. Contrast Media Mol. Imaging 2017, 2017, 6162845. [Google Scholar] [CrossRef] [Green Version]
- Roxin, Á.; Zhang, C.; Huh, S.; Lepage, M.L.; Zhang, Z.; Lin, K.S.; Bénard, F.; Perrin, D.M. Preliminary evaluation of 18F-labeled LLP2A-trifluoroborate conjugates as VLA-4 (α(4)β(1) integrin) specific radiotracers for PET imaging of melanoma. Nucl. Med. Biol. 2018, 61, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Soodgupta, D.; Zhou, H.; Beaino, W.; Lu, L.; Rettig, M.; Snee, M.; Skeath, J.; DiPersio, J.F.; Akers, W.J.; Laforest, R.; et al. Ex Vivo and In Vivo Evaluation of Overexpressed VLA-4 in Multiple Myeloma Using LLP2A Imaging Agents. J. Nucl. Med. 2016, 57, 640–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noborio-Hatano, K.; Kikuchi, J.; Takatoku, M.; Shimizu, R.; Wada, T.; Ueda, M.; Nobuyoshi, M.; Oh, I.; Sato, K.; Suzuki, T.; et al. Bortezomib overcomes cell-adhesion-mediated drug resistance through downregulation of VLA-4 expression in multiple myeloma. Oncogene 2009, 28, 231–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, H.; Su, J.; Garmy-Susini, B.; Kleeman, J.; Varner, J. Integrin alpha4beta1 promotes monocyte trafficking and angiogenesis in tumors. Cancer Res. 2006, 66, 2146–2152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosen, N.; Matsunaga, Y.; Hasegawa, K.; Matsuno, H.; Nakamura, Y.; Makita, M.; Watanabe, K.; Yoshida, M.; Satoh, K.; Morimoto, S.; et al. The activated conformation of integrin β(7) is a novel multiple myeloma-specific target for CAR T cell therapy. Nat. Med. 2017, 23, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Hosen, N.; Yoshihara, S.; Takamatsu, H.; Ri, M.; Nagata, Y.; Kosugi, H.; Shimomura, Y.; Hanamura, I.; Fuji, S.; Minauchi, K.; et al. Expression of activated integrin β7 in multiple myeloma patients. Int. J. Hematol. 2021, 114, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Caserta, E.; Chea, J.; Minnix, M.; Poku, E.K.; Viola, D.; Vonderfecht, S.; Yazaki, P.; Crow, D.; Khalife, J.; Sanchez, J.F.; et al. Copper 64-labeled daratumumab as a PET/CT imaging tracer for multiple myeloma. Blood 2018, 131, 741–745. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Sobol, N.B.; O’Donoghue, J.A.; Kirov, A.S.; Riedl, C.C.; Min, R.; Smith, E.; Carter, L.M.; Lyashchenko, S.K.; Lewis, J.S.; et al. CD38-targeted Immuno-PET of Multiple Myeloma: From Xenograft Models to First-in-Human Imaging. Radiology 2020, 295, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Quelven, I.; Monteil, J.; Sage, M.; Saidi, A.; Mounier, J.; Bayout, A.; Garrier, J.; Cogne, M.; Durand-Panteix, S. (212)Pb α-Radioimmunotherapy Targeting CD38 in Multiple Myeloma: A Preclinical Study. J. Nucl. Med. 2020, 61, 1058–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minnix, M.; Adhikarla, V.; Caserta, E.; Poku, E.; Rockne, R.; Shively, J.E.; Pichiorri, F. Comparison of CD38-Targeted α- Versus β-Radionuclide Therapy of Disseminated Multiple Myeloma in an Animal Model. J. Nucl. Med. 2021, 62, 795–801. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Male, 48 years old, with newly diagnosed multiple myeloma imaged with both [18F]fluciclovine and [18F]FDG PET (A) before treatment and (B) 3 months after first-line treatment with standard induction therapy and autologous stem cell transplantation (ASCT).
Figure 1.
Male, 48 years old, with newly diagnosed multiple myeloma imaged with both [18F]fluciclovine and [18F]FDG PET (A) before treatment and (B) 3 months after first-line treatment with standard induction therapy and autologous stem cell transplantation (ASCT).

Figure 2.
A 41-year-old patient with multiple myeloma and CD38 expression within normal range was imaged with [89Zr]-DFO-daratumumab PET/CT. (A) Maximum intensity projection images 1, 2, 5, and 7 days after injection showing biodistribution of daratumumab. Dashed red lines represent level of trans-axial images in B. (B) Transaxial CT and fused PET/CT of the distal right femur showing increasing [89Zr]-DFO-daratumab uptake with time and decreasing blood pool activity (level of dashed red line). (C) Time activity curve of [89Zr]-DFO-daratumumab in index regions with standardized uptake value (SUV). Blood pool activity was measured in cardiac left ventricle [66].
Figure 2.
A 41-year-old patient with multiple myeloma and CD38 expression within normal range was imaged with [89Zr]-DFO-daratumumab PET/CT. (A) Maximum intensity projection images 1, 2, 5, and 7 days after injection showing biodistribution of daratumumab. Dashed red lines represent level of trans-axial images in B. (B) Transaxial CT and fused PET/CT of the distal right femur showing increasing [89Zr]-DFO-daratumab uptake with time and decreasing blood pool activity (level of dashed red line). (C) Time activity curve of [89Zr]-DFO-daratumumab in index regions with standardized uptake value (SUV). Blood pool activity was measured in cardiac left ventricle [66].


{kind=link}
{kind=link}
Table 1.
Radiotracers for targeted imaging: a selection of tracers explored for imaging of multiple myeloma.
Table 1.
Radiotracers for targeted imaging: a selection of tracers explored for imaging of multiple myeloma.
| Radiolabeled Tracer | Target/Mechanism |
|---|---|
| [18F]FDG | Glucose metabolism |
| [11C]acetate | Fatty acid metabolism |
| [11C]/[18F]choline | Cell membrane synthesis |
| [18F]fluoroethyldimethyl-2-hydroxy-ethylammonium (FECH) | Choline analog and cell membrane |
| [11C]methionine | Amino acid metabolism |
| [18F]fluciclovine | Amino acid metabolism |
| Sodium [18F]fluoride | Bone matrix |
| [18F]fluorothymidine | Thymidine kinase activity |
| [11C]4-thiothymidine | Thymidine kinase activity |
| [68Ga]Ga-pentixafor | Chemokine receptor—CXCR-4 |
| [64Cu]-CB-TE1A1P-LLP2 | VLA-4 receptor targeting |
| [89Zr]bevacizumab | VEGF receptor targeting and angiogenesis |
| [111In]pentetreotide | Somatostatin receptor targeting |
| [68Ga]Ga-PSMA | Tumor vasculature |
| [89Zr]-DFO-daratumomab | Anti CD-38 antibody |
| [64Cu]-DOTA-Dara | Daratumomab-anti CD-38 antibody |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Revheim, M.-E.; Stokke, C.; Nørgaard, J.N.; Phillips, H.F.; Sherwani, A.G.; Schjesvold, F.; Connelly, J.P. New Targets for PET Imaging of Myeloma. Hemato 2021, 2, 727-738. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040049
AMA Style
Revheim M-E, Stokke C, Nørgaard JN, Phillips HF, Sherwani AG, Schjesvold F, Connelly JP. New Targets for PET Imaging of Myeloma. Hemato. 2021; 2(4):727-738. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040049
Chicago/Turabian StyleRevheim, Mona-Elisabeth, Caroline Stokke, Jakob Nordberg Nørgaard, Hilde Feiring Phillips, Alexander Gul Sherwani, Fredrik Schjesvold, and James P. Connelly. 2021. "New Targets for PET Imaging of Myeloma" Hemato 2, no. 4: 727-738. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040049