
Subcutaneous Craniofacial Emphysema Following Endodontic Treatment: Case Report with Literature Review



Department of Medical, Oral and Biotechnological Sciences, University G. d’Annunzio, 31, Via dei Vestini, 66100 Chieti, Italy
*
Author to whom correspondence should be addressed.
Oral 2021, 1(2), 153-158; https://0-doi-org.brum.beds.ac.uk/10.3390/oral1020015
Submission received: 15 April 2021
/
Revised: 29 May 2021
/
Accepted: 2 June 2021
/
Published: 4 June 2021
Abstract
:Subcutaneous emphysema is a well-known and recognized complication in oral surgery, due to high pressure rotating instrument use, mostly related to impacted tooth surgery. Although root canal treatment in endodontic therapy is considered as a safe and standard procedure, affected by a low incidence of complication, subcutaneous emphysema due to the choice of mechanical tools or as a consequence of the use of air stream to dry the operating field should be considered as a potential cause. The air can spread through soft tissue from the apex or from an iatrogenic root perforation, suddenly leading to this unusual complication. It is very important for a dental practitioner to promptly identify the adverse event and to know how to manage this situation. We report a case of a 57-year-old woman with immediate subcutaneous cervicofacial emphysema after root canal therapy of the right inferior second premolar and its management. A brief review of the literature is also displayed.
1. Introduction
Improper root canal therapy (RCT) can lead to subcutaneous emphysema as iatrogenic complication, along with periodontal treatment, tooth extraction and restorative dentistry [1]. The etymology of the term emphysema derives from the Greek “ἐμϕυσάω” translated as “to blow into” [2], and sure enough, the subcutaneous emphysema (SCE) is defined as an anomalous air or gas concentration in the tissue immediately under the skin layer.
The emphysema in dentistry can involve the facial area, up to the orbital region [3] and the neck region [4], but there are also a few cases of mediastinal emphysema [5]. However, all these complications may present at the same time [6], creating a challenge for their management by dentists. The major aspects of these conditions are the potential formation of air emboli and airway impairment, which can be life-threatening for patients [7]. The air expanding soft tissues can also spread into vessels and flow into the blood stream causing embolism. When an extensive SCE is present, it can elicit a huge pressure on the airways, reducing tracheal lumen and causing severe respiratory deficit. On the other hand, emphysema is a possible cause of infection in the deeper spaces occurring in communication environments with a microbial load, such as the oral cavity, and underlying sterile compartments. Literature on this topic also offers a case of loss of vision due to optic nerve damage [8]. Fortunately, SCE usually passes in a quiet and safe way without severe consequences [9]. The common presentation of SCE is a sudden swelling of variable extent that generates crepitus if pressed by the fingers.
The first reports of SCE after an endodontic treatment appeared in the 1950s [10,11,12], however nowadays we have different etiological hypotheses: strongly blowing air under pressure to dry the area [6,13], the use of dental handpieces that release air-water flow but also the extrusion of hydrogen peroxide through the apex [7]. In oral and dental procedures SCE is a rare phenomenon due to the combination of using a positive pressure handpiece and the interruption of the intraoral epithelium.
The aim of this study was to report on craniofacial SCE detected in a patient undergoing an RTC and diagnosed at the University Dental Clinic of Chieti in January 2021, focusing on the management and prevention of this adverse event, and to perform a brief literature review on this topic.
2. Materials and Methods
This study was carried out in accordance with the principles of the Declaration of Helsinki and the patient released detailed informed consent form for diagnostic and therapeutic procedures and for possible use of the radiological examinations and facial photos for research purposes.
A 57-year-old woman came to our attention via her dentist because of a vast puffiness of the right cheek and the right side of her neck, which appeared during root canal therapy of the inferior right second premolar performed without rubber dam isolation. The objective examination revealed a soft swelling of the right cheek extending to the homolateral neck side (Figure 1a,b) with pathognomonic crepitus on palpation. The WHO eight-step intraoral examination was performed and revealed bloating of the right oral floor and the ipsilateral fornix (Figure 1c,d).
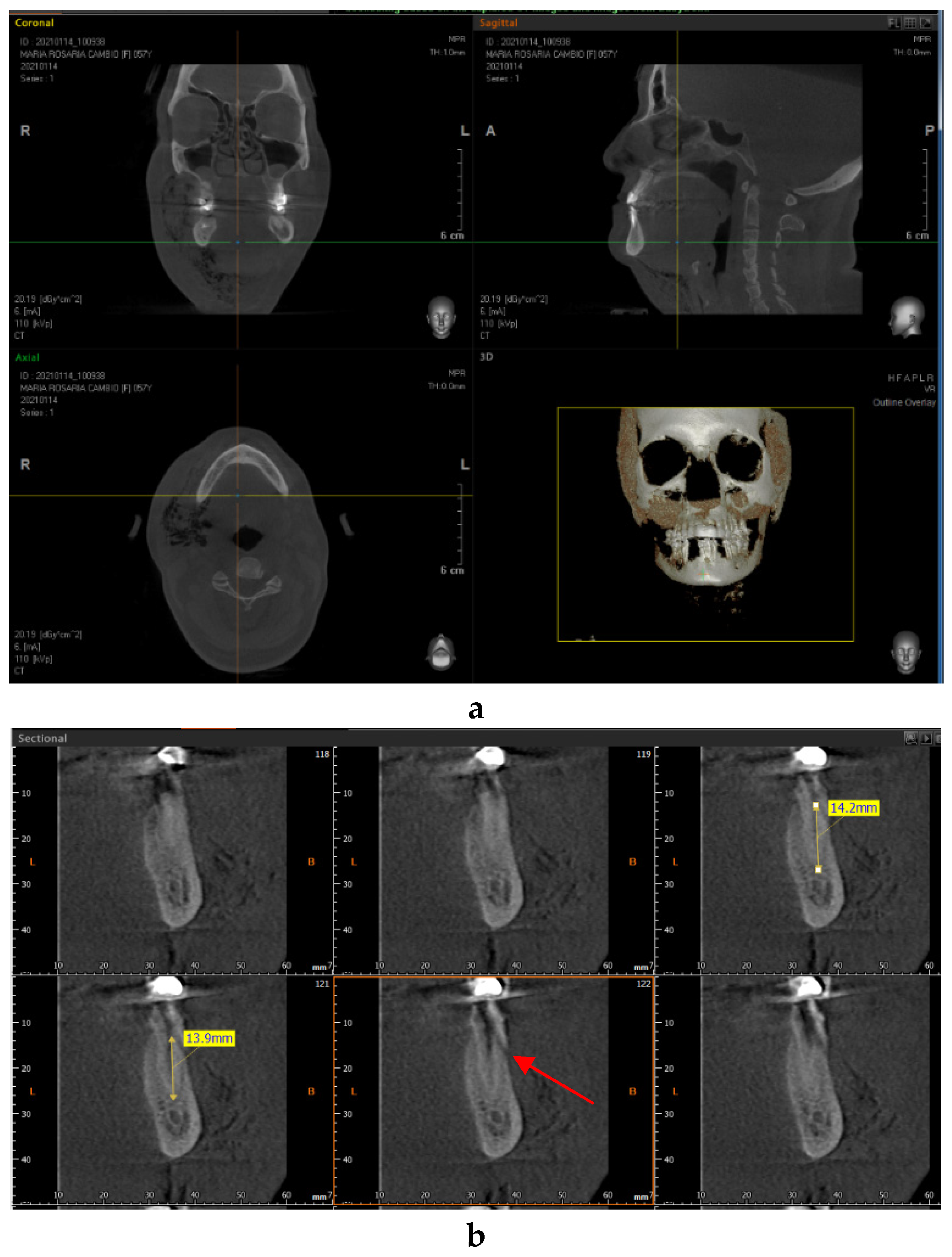
The lady underwent cone beam computed tomography (CBCT) with a PaX-Zenith3D (Vatech, 13, Samsung 1-ro 2-gil, Hwaseong-si, Gyeonggi-do, 445–170, Korea). Three dimensional images were acquired along sagittal, axial and coronal axes and confirmed the hypothesis of right cervicofacial SCE (Figure 2a). Particular attention was paid to the tooth treated, CT images revealed an iatrogenic perforation at 14 mm from the apical foramen, which could be the site of insufflation (Figure 2b). In addition to this, as clearly visible from the CT scans, the vestibular cortex ends approximately 1 mm below the site of perforation. This seems to explain how the air was able to reach the submucosal region and to expand soft tissues, creating a valve like mechanism.
After collecting the case history about any drug-related allergic event, antibiotic therapy based on amoxicillin and clavulanic acid 3 g/die for 7 days was provided. The patient was asked to come for a daily check in the first week and then after 2 weeks until the swelling totally resolved.
For the review part, an electronic search was performed in PubMed and ResearchGate considering the period from 2004 to 2021 and the following MeSH was used: “emphysema endodontic”. The study’s eligibility criteria are the description of SCE in children and adults caused by endodontic therapy, including case reports, clinical studies and case series presentation. Aspects pointed out are also the onset of the adverse event, its resolution and the pharmacological treatment when reported.
3. Results
The digital investigation provided 30 articles, 12 were positive for inclusion criteria (Table 1), while others were excluded due to involving sodium hypochlorite accidents and discussion without case presentation.
The articles describe SCE in 75% women (9/12 cases), with mean age of 55.5 years (±15.7) and in 25% men (3/12 cases) with mean age of 34.3 years (±30.4). The total adverse swelling during/post RCT is 13 cases and 53.8% (7/13 cases) occurred in the mandible, 38.5% (5/13 cases) affected the maxilla and 7.7% (1/13 case) is unknown.
The onset of this adverse event from our search is variable: 30.8% (4/13) of cases were immediate, 38.5% (5/13) by 1–2 h, 23% (3/13) by 5–10 min and 7.7% (1/13) required a few days to develop. Pharmacological treatment was referred in 11 works examined, but it was explained in just 10 articles and it differs from penicillin in association with cortisone or not, to cephalosporin, clindamycin plus ciprofloxacin. The antibiotic most often prescribed was amoxicillin in 45.5% (5/11) of articles. Oral administration was the most common adopted solution, while in 18.1% (2/11) of articles intravenous administration was reported because of massive and severe SCE. Often, non-steroidal anti-inflammatory drugs (NSAIDs) were given in 27.3% (3/11) of articles.
4. Discussion
As stated by the valuable paper by Fasoulas et al. [21], SCE is more frequent in females than in males, with a ratio of 2:1, this was also confirmed in our database. In most of the articles cited in this review, the endodontic procedure which leads to soft tissue swelling is initial RCT (78%), while 14% happens during non-surgical RCT and 5% is linked to endodontic surgery [22] Lastly, 3% arises throughout the surgical management of acute apical abscesses [15]. In this paper, 71% of involved teeth are maxillary, while in our report 6 authors in 11 (54.54%) referred to mandibular teeth and one author does not mention the tooth type. It is paramount to point out that in the cases analyzed in Table 1, the major cause of SCE during dental procedures seems to be root canal drying with air syringe under pressure, in line with Fasoulas et al.’s work.
SCE evidently spreads near the site where a valve mechanism occurs, hence when upper teeth are involved, periorbital swelling is more frequent, on the other hand when lower teeth are implicated, cheek and neck bulges are the most common areas. Antibiotic therapy is chosen in order to reduce the possible introduction of bacteria into deeper subcutaneous spaces. In accordance with our database, among various antibiotic molecules, amoxicillin and clavulanic acid remain the preferred drugs to manage SCE and most episodes resolve in 7–10 days without any consequences. Alternatives to amoxicillin are represented by: clindamycin, ceftriaxone, ampicillin, ciprofloxacin and cefuroxime as stated in Table 1.
In agreement with Van Tubergen et al. [23], the differential diagnosis has to be established with allergic events and hematoma after anesthesia injection. Allergic evidences include cutaneous erythema often with warmth and itching, while trismus and intraoral swelling at the injection site tend to point to a blood effusion. When an air iatrogenic emphysema happens, it is mandatory to identify a possible airway restriction risk. It is desirable to refer the patient in order to perform a second level exam such as a CBCT, that allows recognizing of the damage extent.
5. Conclusions
Among the rare consequences of RCT, SCE can emerge and be potentially life-threatening. During endodontic therapy, the major cause seems to be the pressurized air stream, which should not be directed towards a site where a valve mechanism is suspected. SCE remains empirically handled by the administration of antibiotics, corticosteroids and NSAIDs as well as analgesic if necessary. Awareness among dentists and oral and maxillofacial surgeons is crucial, guidelines may be necessary to choose the right management and allow the safest treatment of this rare iatrogenic condition.
Author Contributions
Conceptualization, S.D.; methodology, S.D.; investigation, S.D. and M.D.; resources, S.D.; data curation, S.D.; writing—original draft preparation, S.D.; writing—review and editing, S.D.; visualization, S.D.; supervision, M.D.; project administration, S.D. and M.D. Both authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient to publish this paper.
Acknowledgments
We would like to thank Vincenzo Ginefra for his professionalism and valuable clinical contribution.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, K.C.; Chiu, W.C.; Lo, W.L.; Huang, T.T. Iatrogenic orbital, cervicofacial, and mediastinal emphysema through endodontic crestal perforation. J. Dent. Sci. 2021, 16, 549–551. [Google Scholar] [CrossRef] [PubMed]
- Treccani. Available online: https://www.treccani.it/vocabolario/ricerca/enfisema/ (accessed on 15 January 2021).
- Chang, C.H.; Lien, W.C. Palpebral emphysema following a dental procedure. Am. J. Emerg. Med. 2018, 36, 908.e1–908.e2. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Ganti, L.; Haupt, J.D.; Marshall, B. Iatrogenic post-pulpectomy cervicofacial subcutaneous emphysema in a paediatric patient. BMJ Case Rep. 2020, 13, e234074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawlinson, R.D.; Negmadjanov, U.; Rubay, D.; Ohanisian, L.; Waxman, J. Pneumomediastinum after dental filling: A rare case presentation. Cureus 2019, 11, e5593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, G.K.; Zats, B.; Kunin, M. Orbital, mediastinal, and cervicofacial subcutaneous emphysema after endodontic retreatment of a mandibular premolar: A case report. J. Endod. 2014, 40, 880–883. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, W.S.; Rosenberg, M. Iatrogenic subcutaneous emphysema of dental and surgical origin: A literature review. J. Oral Maxillofac. Surg. 2009, 67, 1265–1268. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, A.; Riddell, C.E.; Akram, I.; Ahmado, A.; Benjamin, L. Orbital emphysema leading to blindness following routine functional endoscopic sinus surgery. Arch. Ophthalmol. 2005, 123, 1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Groot, A.J. Emphyseem via het pulpakanaal [Facial emphysema via the root canal]. Tijdschr Tandheelkd. 1950, 57, 573–574. [Google Scholar]
- Langegger, P.A. Emphysem bei zahnbehandlung [Emphysema in dentistry]. Osterr. Z Stomatol. 1950, 47, 133–137. [Google Scholar]
- Herve, M. Emphysème souscutané au cours de traitement de canàux [Subcutaneous emphysema during root canal therapy]. Rev. Odontol. Parana. 1952, 74, 40–45. [Google Scholar]
- Mishra, L.; Patnaik, S.; Patro, S.; Debnath, N.; Mishra, S. Iatrogenic subcutaneous emphysema of endodontic origin—Case report with literature review. J. Clin. Diagn. Res. 2014, 8, 279–281. [Google Scholar] [CrossRef]
- Schneider, L.A.; Weber, L.; Maetzke, J.; Scharffetter-Kochanek, K. A swollen face after dental surgery. J. Dtsch Dermatol. Ges. 2005, 3, 987–989. [Google Scholar] [CrossRef]
- Smatt, Y.; Browaeys, H.; Genay, A.; Raoul, G.; Ferri, J. Iatrogenic pneumomediastinum and facial emphysema after endodontic treatment. Br. J. Oral Maxillofac. Surg. 2004, 42, 160–162. [Google Scholar] [CrossRef]
- Frühauf, J.; Weinke, R.; Pilger, U.; Kerl, H.; Müllegger, R.R. Soft tissue cervicofacial emphysema after dental treatment: Report of 2 cases with emphasis on the differential diagnosis of angioedema. Arch. Dermatol. 2005, 141, 1437–1440. [Google Scholar] [CrossRef] [Green Version]
- Farfel, M.J.; Filho, R.S.O.; Cade, J.R.; Santos, A.R.C.; Iervolino, M.; Faulhaber, M.H.V. Pneumomediastinum after dental treatment. Einstein 2008, 6, 209–211. [Google Scholar]
- Buchbender, M.; Musazada, S.; Kreißel, S.; Schmitt, C.M. Extensive cervicofacial and mediastinal subcutaneous emphysema after endodontic retreatment of a maxillary canine: A case report. J. Oral Maxillofac. Radiol. 2017, 5, 14–18. [Google Scholar] [CrossRef]
- Rodríguez-Calzadilla, M.; García-Vázquez, M.; Contreras-Espuny, M.; Soto-Guerrero, A.; Rodríguez-Suárez, A.H.; Benítez-del-Castillo-Sánchez, F.J.; García-Íñiguez, M. Enfisema periorbitario secundario a procedimiento dental: Reportede un caso y revisión de la literatura. Rev. Mex Oftalmol. 2017. [Google Scholar] [CrossRef] [Green Version]
- Tenore, G.; Palaia, G.; Ciolfi, C.; Mohsen, M.; Battisti, A.; Romeo, U. Subcutaneous emphysema during root canal therapy: Endodontic accident by sodium hypoclorite. Ann. Stomatol. 2018, 8, 117–122. [Google Scholar] [CrossRef]
- Gouda, H.S.; Shashidhar; Mestri, C. Mediastinal emphysema due to an isolated facial trauma: A case report. Med. Sci. Law. 2008, 48, 178–180. [Google Scholar] [CrossRef]
- Fasoulas, A.; Boutsioukis, C.; Lambrianidis, T. Subcutaneous emphysema in patients undergoing root canal treatment: A systematic review of the factors affecting its development and management. Int. Endod. J. 2019, 52, 1586–1604. [Google Scholar] [CrossRef] [Green Version]
- Imai, T.; Michizawa, M.; Arimoto, E.; Kimoto, M.; Yura, Y. Cervicofacial subcutaneous emphysema and pneumomediastinum after intraoral laser irradiation. J. Oral Maxillofac. Surg. 2009, 67, 428–430. [Google Scholar] [CrossRef] [PubMed]
- Van Tubergen, E.; Tindle, D.; Fox, G. Sudden onset of subcutaneous air emphysema after the application of air to a maxillary premolar located in a nonsurgical field. Oper. Dent. 2017, 42, E134–E138. [Google Scholar] [CrossRef]
Figure 1.
(a,b) Extraoral examination. An area of swelling on the right side of the cervicofacial region is clearly visible. (c,d) Intraoral examination. The right fornix and oral floor appear inflated.
Figure 1.
(a,b) Extraoral examination. An area of swelling on the right side of the cervicofacial region is clearly visible. (c,d) Intraoral examination. The right fornix and oral floor appear inflated.

Figure 2.
Cone beam computed tomography (CBCT) images. (a) Air infiltration is recognizable in the right side of cheek and neck. (b) The right inferior second premolar. It presents an iatrogenic communication (red arrow) at 14 mm from the apex.
Figure 2.
Cone beam computed tomography (CBCT) images. (a) Air infiltration is recognizable in the right side of cheek and neck. (b) The right inferior second premolar. It presents an iatrogenic communication (red arrow) at 14 mm from the apex.


{kind=link}
{kind=link}
Table 1.
Distribution of subcutaneous emphysema (SCE) during endodontic treatment in literature. IV: intravenous; h: hours; min: minutes.
Table 1.
Distribution of subcutaneous emphysema (SCE) during endodontic treatment in literature. IV: intravenous; h: hours; min: minutes.
| Author | Gender/Age | Tooth | SCE Distribution | Onset | Resolution (Days) | Pharmacological Therapy |
|---|---|---|---|---|---|---|
| Smatt et al., 2004 [14] | F 25 | 19 | Head, neck and presternal regions | 10 min later | 7 | Antibiotics; Analgesics |
| Frühauf et al., 2005 [15] | M 68 | 31 32 | Laterocervical and presternal areas, orbita, submaxillary area, perimandibular and retromandibular spaces | 2 h later | 7 | Amoxicillin sodium plus clavulanic acid 2 g/12 h |
| Farfel et al., 2008 [16] | F 55 | 18 | Submandibular, parapharyngeal, retropharyngeal, carotid, anterior and posterior left spaces, superior mediastinum | 2 h later | 3 | Clindamycin 600 mg/8 h; Ciprofloxacin 400 mg/12 h |
| An et al., 2014 [6] | F 33 | 21 | Facial, periorbital, buccal, submandibular | Immediate | 14 | Clindamycin and dexamethasone IV for 24 h |
| Mishra et al., 2014 [13] | F 53 | 9 | Lower eyelid, lower mandibular margin | 10 min later | 7 | Amoxicillin/Potassium Clavulanate 625 mg/12 h for 5 d |
| Buchbender et al., 2017 [17] | F 79 | 6 | Submandibular cervicofacial and mediastinal emphysema | Immediate | 14 | Cefuroxime 1.5 g IV/8 h, Ibuprofen 600 mg |
| Calzadilla et al., 2017 [18] | F 57 | 15 | Periorbital | Immediate | 7 | Amoxicillin and clavulanic acid 875/125 mg/8 h; Ibuprofen 600 mg/8 h |
| Chang et al., 2018 [3] | F 48 | 5 | Facial/eyelid | Progressive (3 d later) | 10 | Antibiotic prophylaxis |
| Tenore et al., 2018 [19] | F 60 | 23 | Left eye, upper labial region, mandibular region, the contralateral infraorbital region, left cheek | Immediate | 30 | Ceftriaxone; Betamethasone |
| Chen et al., 2021 [1] | M 26 | 20 | Left facial, periorbital, buccal, submental, submandibular | After few hours | 20 | Ampicillin 1 g; Sulbactam 0.5 g; Amoxicillin/clavulanic acid |
| Singh et al., 2020 [4] | M 9 | - | Periorbital and maxillary regions | 1 h later | 7 | - |
| Gouda et al., 2020 [20] | F 45 | 15 | Suborbital region, from upper eyelid to 3 cm from lower mandible margin | 5 min later | 14 | Amoxicillin 500 mg for 5 d; Betamethasone 0.5 mg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
D’Agostino, S.; Dolci, M. Subcutaneous Craniofacial Emphysema Following Endodontic Treatment: Case Report with Literature Review. Oral 2021, 1, 153-158. https://0-doi-org.brum.beds.ac.uk/10.3390/oral1020015
AMA Style
D’Agostino S, Dolci M. Subcutaneous Craniofacial Emphysema Following Endodontic Treatment: Case Report with Literature Review. Oral. 2021; 1(2):153-158. https://0-doi-org.brum.beds.ac.uk/10.3390/oral1020015
Chicago/Turabian StyleD’Agostino, Silvia, and Marco Dolci. 2021. "Subcutaneous Craniofacial Emphysema Following Endodontic Treatment: Case Report with Literature Review" Oral 1, no. 2: 153-158. https://0-doi-org.brum.beds.ac.uk/10.3390/oral1020015