
Determinants of Fruits and Vegetables Consumption among In-School Adolescents in Ghana

 , , ,
, , ,  and
and
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Sampling Method and Sample Size
2.3. Study Variables
Outcome Variables
2.4. Explanatory Variables
2.5. Statistical Analyses
2.6. Ethical Consideration
3. Results
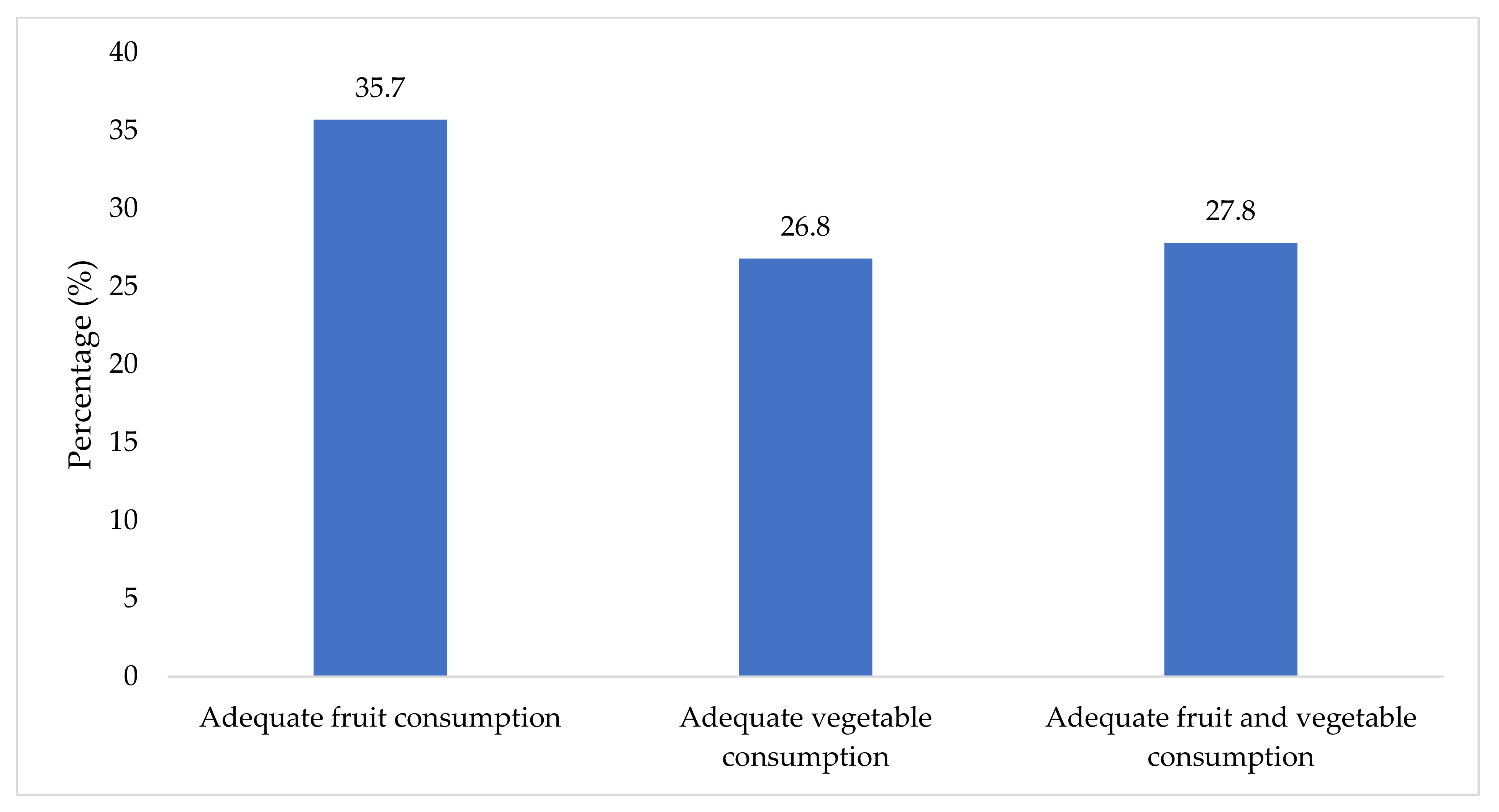
3.1. Prevalence of Fruit and Vegetable Consumption among In-School Adolescents
3.2. Bivariate Analysis of Fruit and Vegetable Consumption and Explanatory Variables
3.3. Multivariable Regression Analysis on Predictors of Adequate Fruit and Vegetable Consumption among In-School Adolescents
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stok, F.M.; Renner, B.; Clarys, P.; Lien, N.; Lakerveld, J.; Deliens, T. Understanding eating behavior during the transition from adolescence to young adulthood: A literature review and perspective on future research directions. Nutrients 2018, 10, 667. [Google Scholar] [CrossRef] [Green Version]
- Kpodo, F.M.; Mensah, C.; Dzah, C.S. Fruit and vegetable consumption patterns and preferences of students in a Ghanaian Polytechnic. World 2015, 3, 53–59. [Google Scholar]
- Blanchard, C.M.; Kupperman, J.; Sparling, P.B.; Nehl, E.; Rhodes, R.E.; Courneya, K.S.; Baker, F. Do ethnicity and gender matter when using the theory of planned behavior to understand fruit and vegetable consumption? Appetite 2009, 52, 15–20. [Google Scholar] [CrossRef]
- De Bruijn, G.J. Understanding college students’ fruit consumption. Integrating habit strength in the theory of planned behaviour. Appetite 2010, 54, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.M., Jr.; Cabang, A.B.; Wargovich, M.J. Future directions in the prevention of prostate cancer. Nat. Rev. Clin. Oncol. 2014, 11, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rekhy, R.; McConchie, R. Promoting consumption of fruit and vegetables for better health. Have campaigns delivered on the goals? Appetite 2014, 79, 113–123. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; Volume 916. [Google Scholar]
- Ngome, P.I.T.; Shackleton, C.; Degrande, A.; Tieguhong, J.C. Addressing constraints in promoting wild edible plants’ utilization in household nutrition: Case of the Congo Basin forest area. Agric. Food Secur. 2017, 6, 20. [Google Scholar] [CrossRef] [Green Version]
- Ungar, N.; Sieverding, M.; Stadnitski, T. Increasing fruit and vegetable intake.“Five a day” versus “just one more”. Appetite 2013, 65, 200–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, S.M.; Pollock, E.D.; Braun, B. Family influence: Key to fruit and vegetable consumption among fourth-and fifth-grade students. J. Nutr. Educ. Behav. 2010, 42, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Kalmpourtzidou, A.; Eilander, A.; Talsma, E.F. Global vegetable intake and supply compared to recommendations: A systematic review. Nutrients 2020, 12, 1558. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Promoting fruit and vegetable consumption around the world. Global Strategy on Diet, Physical Activity and Health. Food Nutr. Bull. 2004, 25. [Google Scholar] [CrossRef]
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef]
- Wu, F.; Guo, Y.; Chatterji, S.; Zheng, Y.; Naidoo, N.; Jiang, Y.; Biritwum, R.; Yawson, A.; Minicuci, N.; Salinas-Rodriguez, A.; et al. Common risk factors for chronic non- communicable diseases among older adults in China, Ghana, Mexico, India, Russia and South Africa: The study on global ageing and adult health (SAGE) wave 1. BMC Public Health 2015, 15, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghose, B.; Yaya, S. Fruit and vegetable consumption and anemia among adult non- pregnant women: Ghana demographic and health survey. PeerJ 2018, 6, e4414. [Google Scholar] [CrossRef] [Green Version]
- Ruel, M.T.; Minot, N.; Smith, L. Patterns and Determinants of Fruit and Vegetable Consumption in Sub- Saharan Africa: A Multicountry Comparison; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Ghana Statistical Service, (GSS); Ghana Health Service, (GHS); Inner City Fund International. Ghana Demographic and Health Survey 2014; GSS; GHS; ICF International: Rockville, MD, USA, 2015.
- Doku, D.; Koivusilta, L.; Raisamo, S.; Rimpelä, A. Socio-economic differences in adolescents’ breakfast eating, fruit and vegetable consumption and physical activity in Ghana. Public Health Nutr. 2013, 16, 864–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health (MoH) Regenerative Health and Nutrition: A New Paradigm for Health Promotion. Source Manual for the Training of Trainers. Ministry of Health, Ghana. 2008. Available online: http://www.rhnp.gov.gh/admindox/RHN%20SOURCE-%20MANUAL.pdf (accessed on 7 April 2015).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Strobe, I. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atorkey, P.; Asante, K.O. Clustering of multiple health risk factors among a sample of adolescents in Liberia: A latent class analysis. J. Public Health 2021, 1–9. [Google Scholar] [CrossRef]
- Darfour-Oduro, S.A.; Buchner, D.M.; Andrade, J.E.; Grigsby-Toussaint, D.S. A comparative study of fruit and vegetable consumption and physical activity among adolescents in 49 Low-and-Middle-Income Countries. Sci. Rep. 2018, 8, 1623. [Google Scholar] [CrossRef] [Green Version]
- Pengpid, S.; Peltzer, K. Prevalence and correlates of fruit and vegetable consumption among adolescents in Laos. Int. J. Adolesc. Med. Health 2020, 1. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Fruits and vegetables consumption and associated factors among in-school adolescents in five Southeast Asian countries. Int. J. Environ. Res. Public Health 2012, 9, 3575–3587. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Fruits and vegetables consumption and associated factors among in-school adolescents in seven African countries. Int. J. Public Health 2010, 55, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Tachi, K.; Tetteh, J.; Yawson, A.E.; Agyei-Nkansah, A.; Archampong, T. Alcohol consumption and fruits and vegetable intake among older adults in Ghana: A cross-sectional survey based on WHO-SAGE Wave 2 data. BMJ Nutr. Prev. Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Kabwama, S.N.; Bahendeka, S.K.; Wesonga, R.; Mutungi, G.; Guwatudde, D. Low consumption of fruits and vegetables among adults in Uganda: Findings from a countrywide cross- sectional survey. Arch. Public Health 2019, 77, 4. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K. The prevalence and social determinants of fruit and vegetable consumption among adults in Kenya: A cross- sectional national population- based survey, 2015. Pan. Afr. Med. J. 2018, 31, 137. [Google Scholar] [CrossRef] [PubMed]
- Olatona, F.A.; Sosanya, A.; Sholeye, O.O.; Obrutu, O.E.; Nnoaham, K.E. Knowledge of fruits and vegetables, consumption pattern and associated factors among adults in Lagos state, Nigeria. Res. J. Health Sci. 2018, 6, 50–62. [Google Scholar] [CrossRef]
- Nago, E.S.; Verstraeten, R.; Lachat, C.K.; Dossa, R.A.; Kolsteren, P.W. Food safety is a key determinant of fruit and vegetable consumption in urban Beninese adolescents. J. Nutr. Educ. Behav. 2012, 44, 548–555. [Google Scholar] [CrossRef] [Green Version]
- Pengpid, S.; Vonglokham, M.; Kounnavong, S.; Sychareun, V.; Peltzer, K. The prevalence and social determinants of fruit and vegetable consumption and its associations with noncommunicable diseases risk factors among adults in Laos. Asia Pac. J. Public Health 2019, 31, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Azagba, S.; Sharaf, M.F. Disparities in the frequency of fruit and vegetable consumption by socio-demographic and lifestyle characteristics in Canada. Nutr. J. 2011, 10, 118. [Google Scholar] [CrossRef] [Green Version]
- Ledoux, T.A.; Hingle, M.D.; Baranowski, T. Relationship of fruit and vegetable intake with adiposity: A systematic review. Obes. Rev. 2010, 12, e143–e150. [Google Scholar] [CrossRef]
- Nepal, V.P.; Mgbere, O.; Banerjee, D.; Arafat, R.R. Disparities in fruits and vegetables consumption in Houston, Texas: Implications for health promotion. J. Prim. Care Community Health 2011, 2, 142–147. [Google Scholar] [CrossRef] [Green Version]
- Amo-Adjei, J.; Kumi-Kyereme, A. Fruit and vegetable consumption by ecological zone and socioeconomic status in Ghana. J. Biosoc. Sci. 2015, 47, 613. [Google Scholar] [CrossRef] [PubMed]
- Darvin, M.E.; Patzelt, A.; Knorr, F.; Blume-Peytavi, U.; Sterry, W.; Lademann, J. One-year study on the variation of carotenoid antioxidant substances in living human skin: Influence of dietary supplementation and stress factors. J. Biomed. Opt. 2008, 13, 44028. [Google Scholar] [CrossRef] [Green Version]
- Lademann, J.; Meinke, M.C.; Sterry, W.; Darvin, M.E. Carotenoids in human skin. Exp. Dermatol. 2011, 20, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, R.D.; Re, D.; Xiao, D.; Ozakinci, G.; Perrett, D.I. You are what you eat: Within-subject increases in fruit and vegetable consumption confer beneficial skin-color changes. PLoS ONE 2012, 7, e32988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephen, I.D.; Coetzee, V.; Perrett, D.I. Carotenoid and melanin pigment coloration affect perceived human health. Evol. Hum. Behav. 2011, 32, 216–227. [Google Scholar] [CrossRef]
- Abizari, A.R.; Ali, Z.; Abdulai, S.A.; Issah, F.; Frimpomaa, N.A. Free Senior High School Lunch Contributes to Dietary Quality of Nonresidential Students in Ghana. Food Nutr. Bull. 2020, 15, 0379572120970828. [Google Scholar] [CrossRef]
- Majabadi, H.A.; Solhi, M.; Montazeri, A.; Shojaeizadeh, D.; Nejat, S.; Farahani, F.K.; Djazayeri, A. Factors influencing fast-food consumption among adolescents in Tehran: A qualitative study. Iran. Red Crescent Med. J. 2016, 18, e23890. [Google Scholar] [CrossRef] [Green Version]
- Riediger, N.D.; Shooshtari, S.; Moghadasian, M.H. The influence of sociodemographic factors on patterns of fruit and vegetable consumption in Canadian adolescents. J. Am. Diet. Assoc. 2007, 107, 1511–1518. [Google Scholar] [CrossRef]
- Flores, O.C.; Orellana, Y.Z.; Leyton, B.D.; Valenzuela, R.B.; Barrera, C.R.; Almagià, A.F.; Martínez, V.C.; Ivanovic, D. Overnutrition and Scholastic Achievement: Is There a Relationship An 8-Year Follow-Up Study. Obes. Facts 2018, 11, 344–359. [Google Scholar] [CrossRef]
- Karim, M.N.; Zaman, M.M.; Rahman, M.M.; Chowdhury, M.A.J.; Ahsan, H.A.M.N.; Hassan, M.M.; Karim, S.R.; Hossain, M.Z.; Billah, B. Sociodemographic determinants of low fruit and vegetable consumption among Bangladeshi adults: Results from WHO-STEPS Survey 2010. Asia Pac. J. Public Health 2017, 29, 189–198. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Correlates of healthy fruit and vegetable diet in students in low-, middle- and high-income countries. Int. J. Public Health 2015, 60, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Ivanovic, D.M.; Valenzuela, R.B.; Almagia, A.F.; Barrera, C.R.; Arancibia, V.C.; Larraín, C.G.; Silva, C.F.; Billeke, P.B.; Zamorano, F.M.; Villagrán, F.S.; et al. Impact of anthropometric nutritional parameters on the university selection test in Chile: A multifactorial approach. Nutrition 2019, 57, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Ivanovic, D.M.; Almagià, A.F.; Arancibia, V.C.; Ibaceta, C.V.; Arias, V.F.; Rojas, T.R.; Flores, O.C.; Villagrán, F.S.; Tapia, L.U.; Acevedo, J.A.; et al. A multifactorial approach of nutritional, intellectual, brain development, cardiovascular risk, socio-economic, demographic and educational variables affecting the scholastic achievement in Chilean students: An eight-year follow-up study. PLoS ONE 2019, 14, e0212279. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Weighted N (%) | Adequate Fruit Consumption | Adequate Vegetable Consumption | Adequate Fruit and Vegetable Consumption | |||
|---|---|---|---|---|---|---|---|
| Yes | p-Value | Yes | p-Value | Yes | p-Value | ||
| Age | <0.001 | 0.088 | 0.002 | ||||
| 14 years or younger | 820 (29.4) | 45.4 | 30.3 | 35.2 | |||
| 15 years or older | 1966 (70.6) | 31.7 | 25.4 | 24.7 | |||
| Sex | 0.097 | 0.002 | 0.002 | ||||
| Female | 1362 (48.9) | 38.2 | 30.4 | 32.2 | |||
| Male | 1424 (51.1) | 33.4 | 23.5 | 23.7 | |||
| Grade | <0.001 | 0.009 | 0.001 | ||||
| JHS | 1610 (57.8) | 46.1 | 32.7 | 36.1 | |||
| SHS | 1176 (42.2) | 21.6 | 18.9 | 16.5 | |||
| Felt hungry | 0.332 | 0.930 | 0.707 | ||||
| No | 2403 (86.2) | 36.1 | 26.9 | 27.7 | |||
| Yes | 383 (13.8) | 33.2 | 26.6 | 28.9 | |||
| Soft drinks | <0.001 | <0.001 | <0.001 | ||||
| No | 1540 (55.3) | 20.1 | 16.6 | 15.9 | |||
| Yes | 1246 (44.7) | 55.1 | 39.5 | 42.6 | |||
| Fast food | <0.001 | 0.002 | <0.001 | ||||
| No | 2041 (73.3) | 31.6 | 24.2 | 24.6 | |||
| Yes | 745 (26.7) | 47.0 | 34.0 | 36.8 | |||
| Physical activity | 0.508 | 0.470 | 0.527 | ||||
| No | 2215 (79.5) | 36.1 | 26.4 | 27.4 | |||
| Yes | 571 (20.5) | 34.2 | 28.6 | 29.5 | |||
| Sedentary behaviour | 0.026 | 0.361 | 0.040 | ||||
| No | 2261 (81.2) | 34.2 | 26.3 | 26.6 | |||
| Yes | 525 (18.8) | 42.4 | 29.1 | 33.1 | |||
| Overweight | 0.545 | 0.547 | 0.547 | ||||
| No | 2561 (91.9) | 36.0 | 26.7 | 26.7 | |||
| Yes | 225 (8.1) | 33.0 | 28.7 | 28.7 | |||
| Obesity | 0.348 | 0.489 | 0.848 | ||||
| No | 2745 (98.5) | 35.9 | 26.7 | 27.9 | |||
| Yes | 41 (1.5) | 26.4 | 33.1 | 25.9 | |||
| Underweight | 0.606 | 0.829 | 0.289 | ||||
| No | 2664 (95.6) | 35.6 | 26.9 | 27.5 | |||
| Yes | 122 (4.4) | 38.1 | 25.7 | 35.4 | |||
| Current alcohol use | 0.016 | 0.863 | 0.392 | ||||
| No | 2422 (86.9) | 34.9 | 26.9 | 27.5 | |||
| Yes | 364 (13.1) | 41.3 | 26.3 | 30.1 | |||
| Current cigarette smoking | 0.069 | 0.301 | 0.999 | ||||
| No | 2643 (94.9) | 35.3 | 27.1 | 27.8 | |||
| Yes | 143 (5.1) | 43.6 | 21.7 | 27.8 | |||
| Current marijuana use | 0.016 | 0.408 | 0.169 | ||||
| No | 2666 (95.7) | 35.0 | 27.0 | 27.4 | |||
| Yes | 120 (4.3) | 51.9 | 23.0 | 36.5 | |||
| Current tobacco use | 0.276 | 0.451 | 0.659 | ||||
| No | 2547 (91.4) | 35.3 | 27.1 | 27.6 | |||
| Yes | 239 (8.6) | 40.4 | 24.1 | 29.8 | |||
| Psychological distress | 0.944 | 0.323 | 0.161 | ||||
| Low | 197 (7.1) | 34.5 | 31.3 | 35.6 | |||
| Medium | 1745 (62.6) | 35.6 | 27.0 | 26.4 | |||
| High | 844 (30.3) | 36.3 | 25.5 | 29.0 | |||
| Peer support | 0.035 | 0.184 | 0.182 | ||||
| No | 1897 (68.1) | 34.0 | 25.8 | 26.7 | |||
| Yes | 889 (31.9) | 39.5 | 29.0 | 30.3 | |||
| Parent or guardian supervision | 0.003 | 0.160 | 0.160 | ||||
| No | 1606 (57.6) | 31.2 | 25.2 | 25.2 | |||
| Yes | 1180 (42.4) | 42.0 | 29.0 | 29.0 | |||
| Parent or guardian connectedness | 0.292 | 0.307 | 0.307 | ||||
| No | 1746 (62.7) | 34.6 | 25.8 | 25.8 | |||
| Yes | 1040 (37.3) | 37.7 | 28.5 | 28.5 | |||
| Parent or guardian bonding | 0.051 | 0.287 | 0.039 | ||||
| No | 1737 (62.3) | 34.0 | 26.2 | 26.7 | |||
| Yes | 1049 (37.7) | 38.6 | 27.9 | 29.8 | |||
| Variable | Adequate Fruits Consumption | Adequate Vegetable Consumption | Adequate Fruit and Vegetable Consumption |
|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |
| aOR [95% CI] | aOR [95% CI] | aOR [95% CI] | |
| Age | |||
| 14 years or younger | 1.0 | 1.0 | 1.0 |
| 15 years or older | 1.11 [0.91, 1.35] | 1.31 [0.99, 1.73] | 1.13 [0.88, 1.46] |
| Sex | |||
| Female | 1.0 | 1.0 | 1.0 |
| Male | 0.82 [0.65, 1.04] | 0.71 ** [0.57, 0.87] | 0.64 ** [0.51, 0.82] |
| Grade | |||
| JHS | 1.0 | 1.0 | 1.0 |
| SHS | 0.34 *** [0.21, 0.55] | 0.48 ** [0.28, 0.80] | 0.36 ** [0.22, 0.61] |
| Soft drinks | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 4.06 *** [3.23, 5.09] | 2.90 *** [2.22, 3.79] | 3.29 *** [2.42, 4.46] |
| Fast food | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 1.45 ** [1.15, 1.83] | 1.34 * [1.07, 1.67] | 1.42 ** [1.13, 1.77] |
| Sedentary behaviour | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 1.42 ** [1.12, 1.80] | 1.15 [0.89, 1.49] | 1.38 * [1.07, 1.77] |
| Current alcohol use | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 1.12 [0.86, 1.46] | 0.97 [0.64, 1.47] | 1.01 [0.74, 1.39] |
| Current marijuana use | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 1.27 [0.58, 2.78] | 0.57 [0.32, 1.03] | 0.99 [0.45, 2.20] |
| Peer support | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 1.06 [0.90, 1.25] | 1.06 [0.84, 1.34] | 1.05 [0.87, 1.28] |
| Parent or guardian supervision | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 1.35 [0.96, 1.92] | 1.03 [0.76, 1.40] | 1.13 [0.85, 1.51] |
| Parent or guardian bonding | |||
| No | 1.0 | 1.0 | 1.0 |
| Yes | 1.10 [0.88, 1.37] | 1.02 [0.86, 1.24] | 1.09 [0.92, 1.30] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidu, A.-A.; Aboagye, R.G.; Frimpong, J.B.; Iddrisu, H.; Agbaglo, E.; Budu, E.; Hagan, J.E., Jr.; Ahinkorah, B.O. Determinants of Fruits and Vegetables Consumption among In-School Adolescents in Ghana. Adolescents 2021, 1, 199-211. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents1020016
Seidu A-A, Aboagye RG, Frimpong JB, Iddrisu H, Agbaglo E, Budu E, Hagan JE Jr., Ahinkorah BO. Determinants of Fruits and Vegetables Consumption among In-School Adolescents in Ghana. Adolescents. 2021; 1(2):199-211. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents1020016
Chicago/Turabian StyleSeidu, Abdul-Aziz, Richard Gyan Aboagye, James Boadu Frimpong, Hawa Iddrisu, Ebenezer Agbaglo, Eugene Budu, John Elvis Hagan, Jr., and Bright Opoku Ahinkorah. 2021. "Determinants of Fruits and Vegetables Consumption among In-School Adolescents in Ghana" Adolescents 1, no. 2: 199-211. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents1020016