Comparative Study of Validity and Reliability of Two Handgrip Dynamometers: K-Force Grip and Jamar

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
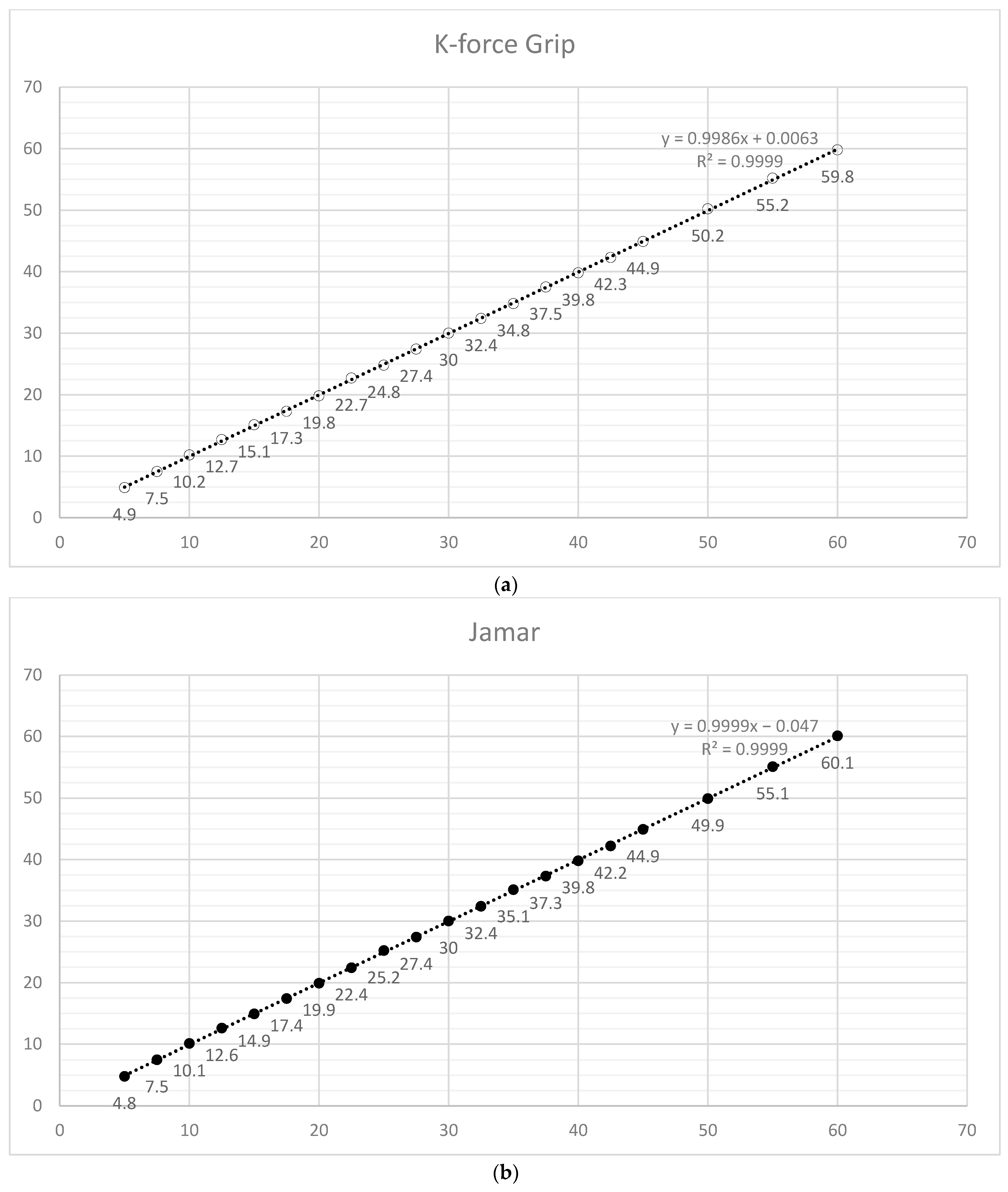
2.1. Concurrent Validity
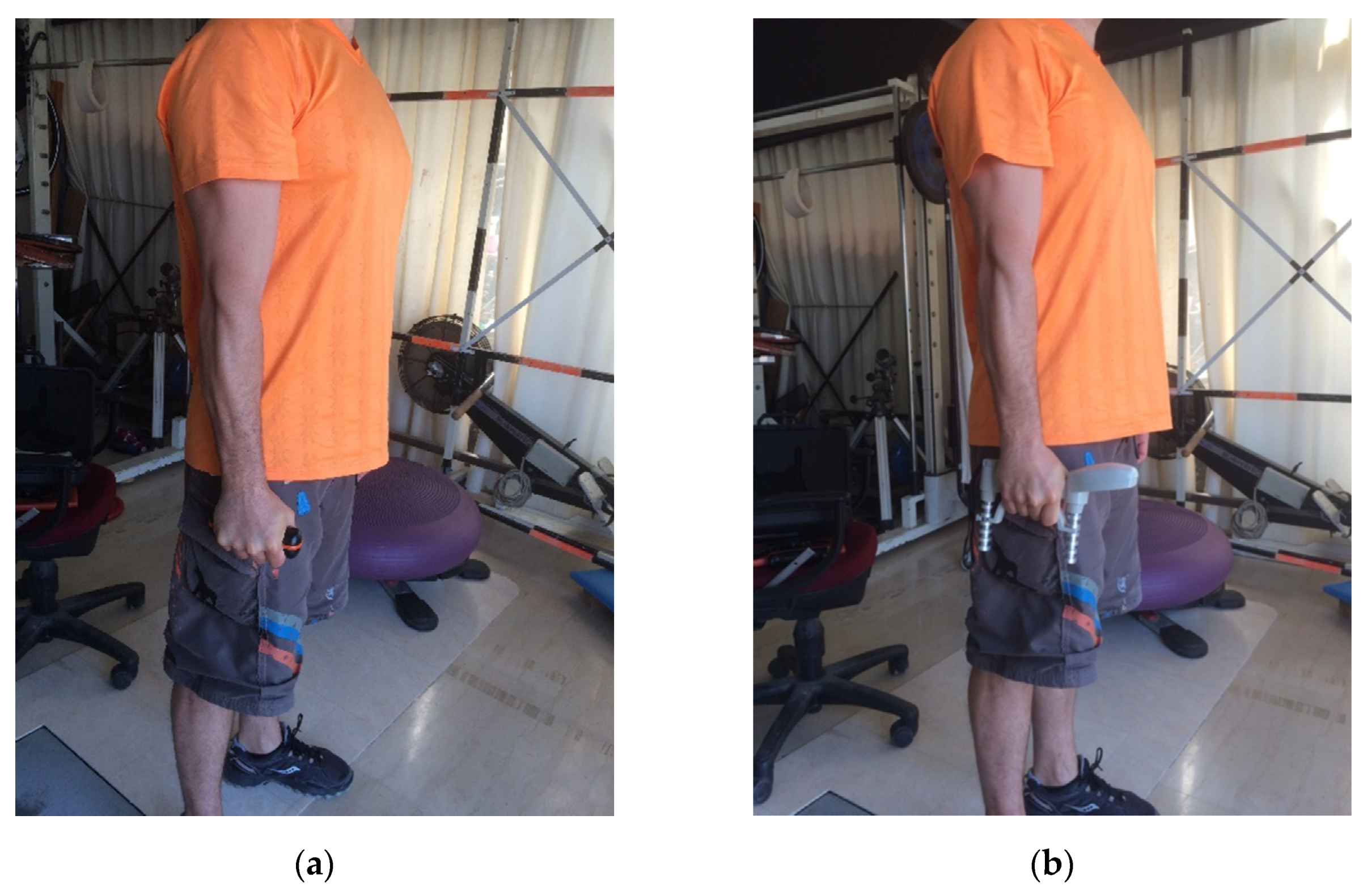
2.2. Strength Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sousa-Santos, A.R.; Amaral, T.F. Differences in handgrip strength protocols to identify sarcopenia and frailty—A systematic review. BMC Geriatr. 2017, 17, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Muscle strength. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- Horsley, I.; Herrington, L.; Hoyle, R.; Prescott, E.; Bellamy, N. Do changes in hand grip strength correlate with shoulder rotator cuff function? Shoulder Elb. 2016, 8, 124–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzato, T.M.; Baptista, C.R.J.A.; Souza, M.A.; Benedicto, M.M.B.; Martinez, E.Z.; Mattiello-Sverzut, A.C. Longitudinal assessment of grip strength using bulb dynamometer in Duchenne Muscular Dystrophy. Braz. J. Phys. Ther. 2014, 18, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kachanathu, S.J.; Zedan, A.M.E.; Hafez, A.R.; Alodaibi, F.A.; Alenazi, A.M.; Nuhmani, S. Effect of shoulder stability exercises on hand grip strength in patients with shoulder impingement syndrome. Somatosens. Mot. Res. 2019, 36, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Ramlagan, S.; Peltzer, K.; Phaswana-Mafuya, N. Hand grip strength and associated factors in non-institutionalised men and women 50 years and older in South Africa. BMC Res. Notes 2014, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Yorke, A.M.; Curtis, A.B.; Shoemaker, M.; Vangsnes, E. The impact of multimorbidity on grip strength in adults age 50 and older: Data from the health and retirement survey (HRS). Arch. Gerontol. Geriatr. 2017, 72, 164–168. [Google Scholar] [CrossRef]
- Aguilar-Lazcano, C.A.; Rechy-Ramirez, E.J. Performance analysis of leap motion controller for finger rehabilitation using serious games in two lighting environments. Measurement 2020, 157, 107677. [Google Scholar] [CrossRef]
- Friedman, N.; Chan, V.; Reinkensmeyer, A.N.; Beroukhim, A.; Zambrano, G.J.; Bachman, M.; Reinkensmeyer, D.J. Retraining and assessing hand movement after stroke using the MusicGlove: Comparison with conventional hand therapy and isometric grip training. J. Neuroeng. Rehabil. 2014, 11, 76. [Google Scholar] [CrossRef] [Green Version]
- Confalonieri, M.; Guandalini, G.; Da Lio, M.; De Cecco, M. Force and touch make video games serious for dexterity rehabilita-tion. pHealth 2012, 177, 139–144. [Google Scholar] [CrossRef]
- Guerra, R.S.; Amaral, T.F.; Sousa, A.S.; Fonseca, I.; Pichel, F.; Restivo, M.T. Comparison of Jamar and bodygrip dynamometers for handgrip strength measurement. J. Strength Cond. Res. 2017, 31, 1931–1940. [Google Scholar] [CrossRef]
- Bellace, J.V.; Healy, D.; Besser, M.P.; Byron, T.; Hohman, L. Validity of the Dexter evaluation system’s Jamar dynamometer attachment for assessment of hand grip strength in a normal population. J. Hand Ther. 2000, 13, 46–51. [Google Scholar] [CrossRef]
- Amaral, J.F.; Mancini, M.; Júnior, J.M.N. Comparison of three hand dynamometers in relation to the accuracy and precision of the measurements. Braz. J. Phys. Ther. 2012, 16, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Hogrel, J.-Y. Grip strength measured by high precision dynamometry in healthy subjects from 5 to 80 years. BMC Musculoskelet. Disord. 2015, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Eckman, M.; Gigliotti, C.; Sutermaster, S.; Mehta, K. Get a grip! Handgrip strength as a health screening tool. In Proceedings of the IEEE Global Humanitarian Technology Conference (GHTC 2014), San Jose, CA, USA, 10–13 October 2014; pp. 242–248. [Google Scholar]
- Agnew, P.; Maas, F. Jamar dynamometer and adapted sphygmomanometer for measuring grip strength in patients with rheumatoid arthritis. Occup. Ther. J. Res. 1991, 11, 259–270. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Vizenor, L.; Melander, D. Comparison of baseline instruments to the Jamar dynamometer and the B&L engineering pinch gauge. Occup. Ther. J. Res. 2000, 20, 147–162. [Google Scholar] [CrossRef]
- Shechtman, O.; Gestewitz, L.; Kimble, C. Reliability and validity of the DynEx dynamometer. J. Hand Ther. 2005, 18, 339–347. [Google Scholar] [CrossRef]
- Farfaras, S.; Ejerhed, L.E.; Hallström, E.K.; Hultenby, K.; Meknas, K.; Movin, T.; Papadogiannakis, N.; Kartus, J.-T. More histologic and ultrastructural degenerative signs in the subscapularis tendon and the joint capsule in male patients with shoulder impingement. Knee Surgery, Sports Traumatol. Arthrosc. 2017, 26, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckup, K. Clinical Tests for the Musculoskeletal System Examinations, Signs, Phenomena, 2nd ed.; Thieme: Stuttgart, Germany, 2008. [Google Scholar]
- Su, C.Y.; Lin, J.H.; Chien, T.H.; Cheng, K.F.; Sung, Y.T. Grip strength in different positions of elbow and shoulder. Arch. Phys. Med. Rehabil. 1994, 75, 812–815. [Google Scholar] [CrossRef]
- Savva, C.; Karagiannis, C.; Rushton, A. Test-retest reliability of grip strength measurement in full elbow extension to evaluate maximum grip strength. J. Hand Surg. Eur. Vol. 2012, 38, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Ludbrook, J. Special article comparing methods of measurement. Clin. Exp. Pharmacol. Physiol. 1997, 24, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V. Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occup. Ther. Int. 2002, 9, 201–209. [Google Scholar] [CrossRef]
- Hamilton, A.; Balnave, R.; Adams, R. Grip strength testing reliability. J. Hand Ther. 1994, 7, 163–170. [Google Scholar] [CrossRef]
- Fess, E.E. A method for checking Jamar dynamometer calibration. J. Hand Ther. 1987, 1, 28–32. [Google Scholar] [CrossRef]
- Hamilton, G.F.; McDonald, C.; Chenier, T.C. Measurement of grip strength: Validity and reliability of the sphygmomanometer and Jamar grip dynamometer. J. Orthop. Sports Phys. Ther. 1992, 16, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Svens, B.; Lee, H. Intra- and inter-instrument reliability of Grip-Strength Measurements: GripTrack™ and Jamar® hand dynamometers. Br. J. Hand Ther. 2005, 10, 47–55. [Google Scholar] [CrossRef]
- Savva, C.; Mougiaris, P.; Xadjimichael, C.; Karagiannis, C.; Efstathiou, M. Test-retest reliability of handgrip strength as an outcome measure in patients with symptoms of shoulder impingement syndrome. J. Manip. Physiol. Ther. 2018, 41, 252–257. [Google Scholar] [CrossRef]
- Crosby, C.A.; Wehbé, M.A. Hand strength: Normative values. J. Hand Surg. 1994, 19, 665–670. [Google Scholar] [CrossRef]
- Trampisch, U.S.; Franke, J.; Jedamzik, N.; Hinrichs, T.; Platen, P. Optimal Jamar dynamometer handle position to assess maximal isometric hand grip strength in epidemiological studies. J. Hand Surg. 2012, 37, 2368–2373. [Google Scholar] [CrossRef]
- Kong, Y.-K.; Kim, D.-M. The relationship between hand anthropometrics, total grip strength and individual finger force for various handle shapes. Int. J. Occup. Saf. Ergon. 2015, 21, 187–192. [Google Scholar] [CrossRef]
- El-Sais, W.M.; Mohammad, W.S. Biomechanical effect of testing positions on hand grip strength. J. Mech. Med. Biol. 2016, 16, 1650026. [Google Scholar] [CrossRef]
- LaStayo, P.; Hartzel, J. Dynamic versus static grip strength: How grip strength changes when the wrist is moved, and why dynamic grip strength may be a more functional measurement. J. Hand Ther. 1999, 12, 212–218. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age | Body Weight | Height | Body Mass Index (BMI) | |
|---|---|---|---|---|
| Pain group (male) | 51.6 ± 13 years | 79.5 ± 12.1 kg | 174.2 ± 8 cm | 27.1 ± 7 kg/cm2 |
| Pain group (female) | 58 ± 15.7 years | 63.2 ± 11.5 kg | 159.2 ± 11 cm | 25.2 ± 6.3 kg/cm2 |
| Healthy group (male) | 19.9 ± 1.6 years | 74.52 ± 9.1 kg | 177.8 ± 6 cm | 23.6 ± 2.2 kg/cm2 |
| Healthy group (female) | 19.4 ± 0.5 years | 56.62 ± 6.6 kg | 163.8 ± 5 cm | 22 ± 2.3 kg/cm2 |
| Concurrent Validity (Against Fixed Mass) | ||||
|---|---|---|---|---|
| Variable | Fixed Bias | Proportional Bias | ||
| Intercept | 95% CI | Slope | 95% CI | |
| Grip | 0.004 | −0.142–0.151 | 0.998 | 0.993–1.003 |
| Jamar | −0.048 | −0.168–0.071 | 0.999 | 0.995–1.004 |
| Within instruments reliability | ||||
| Variable | Fixed bias | Proportional bias | ||
| Intercept | 95% CI | Slope | 95% CI | |
| Grip Left 1–2 | −1.04 | −4.42–2.03 | 1.06 | 0.96–1.16 |
| Grip Left 2–3 | 0.6 | −2.81–3.68 | 1.01 | 0.91–1.12 |
| Grip Left 1–3 | −0.53 | −6.65–4.61 | 1.07 | 0.91–1.26 |
| Grip Right 1–2 | −2.62 | −5.73–0.23 | 1.07 | 0.99–1.17 |
| Grip Right 2–3 | 0.79 | −2.45–3.75 | 0.96 | 0.87–1.06 |
| Grip Right 1–3 | 1.8 | −5.87–1.84 | 1.03 | 0.93–1.15 |
| Jamar Left 1–2 | −1.54 | −9.43–4.99 | 1.03 | 0.85–1.23 |
| Jamar Left 2–3 | 1.51 | −1.61–4.4 | 0.96 | 0.88–1.04 |
| Jamar Left 1–3 | 0.12 | −5.94–5.34 | 0.98 | 0.84–1.14 |
| Jamar Right 1–2 | 2.67 | −1.15–6.17 | 0.93 | 0.84–1.02 |
| Jamar Right 2–3 | 1.57 | −2.06–4.92 | 0.95 | 0.87–1.05 |
| Jamar Right 1–3 | 4.21 | −0.27–8.24 | 0.91 | 0.82–1.01 |
| Between instruments reliability | ||||
| Variable | Fixed bias | Proportional bias | ||
| Intercept | 95% CI | Slope | 95% CI | |
| Pain group (mean values Jamar-Grip) | 0.35 | −3.77–4.00 | 0.93 | 0.84–1.02 |
| Healthy group (mean values Jamar-Grip) | 1.52 | −2.33–4.97 | 0.79 | 0.68–0.91 * |
| Healthy group (mean values Jamar-Grip) outliers removed | −5.13 | (−8.45)–(−2.07) * | 0.89 | 0.83–1.01 |
| ICC 95% CI | Pain Group | Healthy Group | ||||||
|---|---|---|---|---|---|---|---|---|
| Intra-instrument reliability | Jamar affected | Jamar healthy | K-Force Grip (affected) | K-Force Grip (healthy) | Jamar left | Jamar right | K-Force Grip (left) | K-Force Grip (right) |
| 0.977 (0.956–0.989) | 0.983 (0.962–0.993) | 0.972 (0.946–0.987) | 0.96 (0.923–0.981) | 0.929 (0.895–0.954) | 0.946 (0.919–0.965) | 0.941 (0.911–0.963) | 0.949 (0.923–0.967) | |
| Inter-instrument reliability | Jamar—K-Force Grip affected | Jamar—K-Force Grip (healthy) | Jamar—K-Force Grip (left) | Jamar—K-Force Grip (right) | ||||
| 0.979 (0.911–0.993) | 0.911 (0.706–0.959) | 0.91 (0.69–0.918) | 0.907 (0.728–0.9134) | |||||
| Pain Group | Healthy Group | ||||||
|---|---|---|---|---|---|---|---|
| Jamar affected | K-Force Grip affected | Jamar healthy | K-Force Grip healthy | Jamar left | K-Force Grip left | Jamar right | K-Force Grip right |
| 32.1 ± 17 kg | 27.3 ± 13.8 kg | 32.6 ± 15.3 kg | 28.1 ± 13.8 kg | 36.7 ± 17 kg | 30 ± 10.4 kg | 38.6 ± 11.8 kg | 30.7 ± 11.3 kg |
| Cohen’s D effect size | Cohen’s D effect size | Cohen’s D effect size | Cohen’s D effect size | ||||
| 0.35 | 0.33 | 0.58 | 0.61 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikodelis, T.; Savvoulidis, S.; Athanasakis, P.; Chalitsios, C.; Loizidis, T. Comparative Study of Validity and Reliability of Two Handgrip Dynamometers: K-Force Grip and Jamar. Biomechanics 2021, 1, 73-82. https://0-doi-org.brum.beds.ac.uk/10.3390/biomechanics1010006
Nikodelis T, Savvoulidis S, Athanasakis P, Chalitsios C, Loizidis T. Comparative Study of Validity and Reliability of Two Handgrip Dynamometers: K-Force Grip and Jamar. Biomechanics. 2021; 1(1):73-82. https://0-doi-org.brum.beds.ac.uk/10.3390/biomechanics1010006
Chicago/Turabian StyleNikodelis, Thomas, Stratos Savvoulidis, Petros Athanasakis, Christos Chalitsios, and Theodoros Loizidis. 2021. "Comparative Study of Validity and Reliability of Two Handgrip Dynamometers: K-Force Grip and Jamar" Biomechanics 1, no. 1: 73-82. https://0-doi-org.brum.beds.ac.uk/10.3390/biomechanics1010006