
Reliability of the Fluoroscopic Assessment of Load-Induced Glenohumeral Translation during a 30° Shoulder Abduction Test
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Image Acquisition
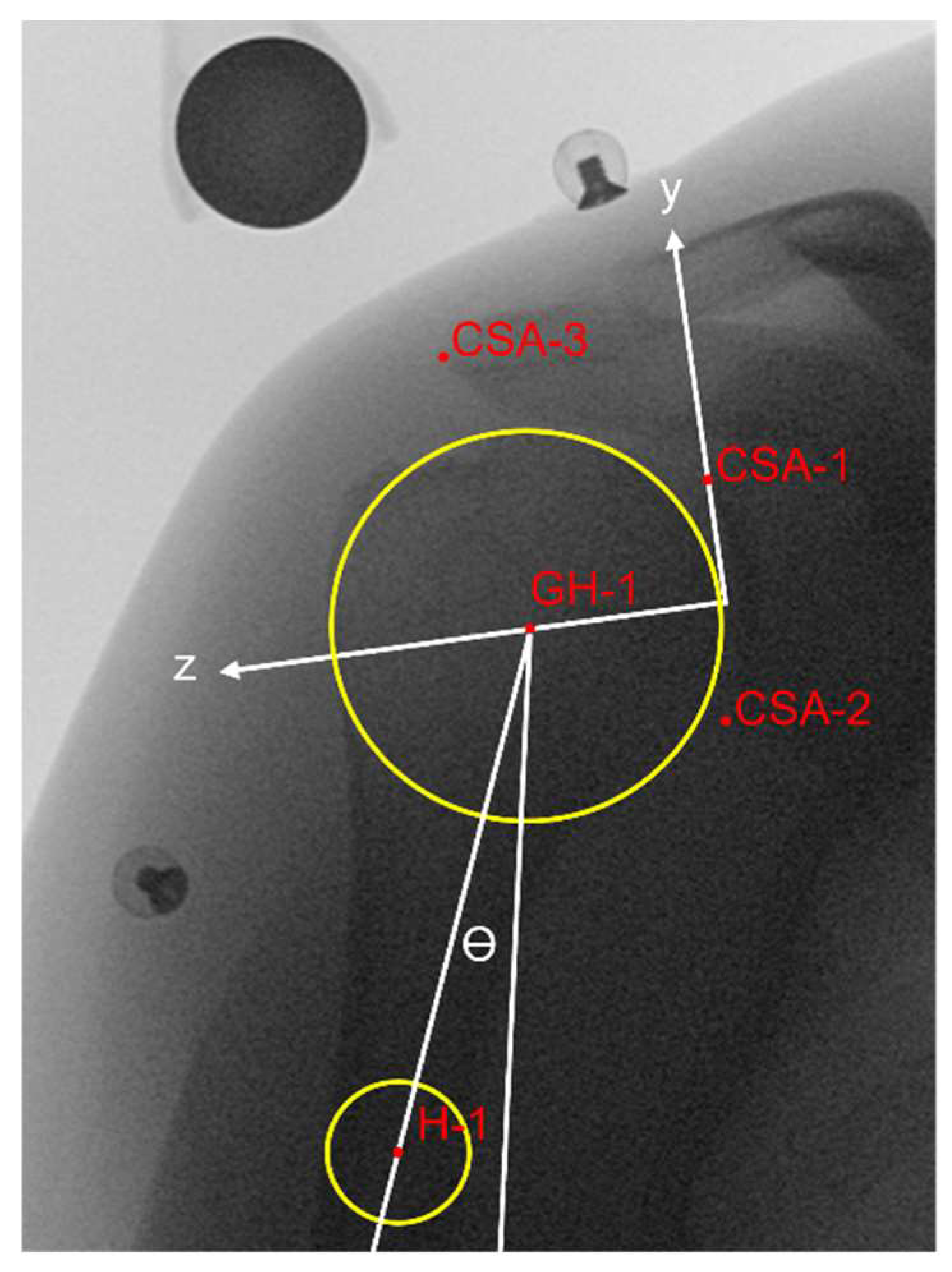
2.3. Assessment of Glenohumeral Translation
2.4. Statistical Analysis
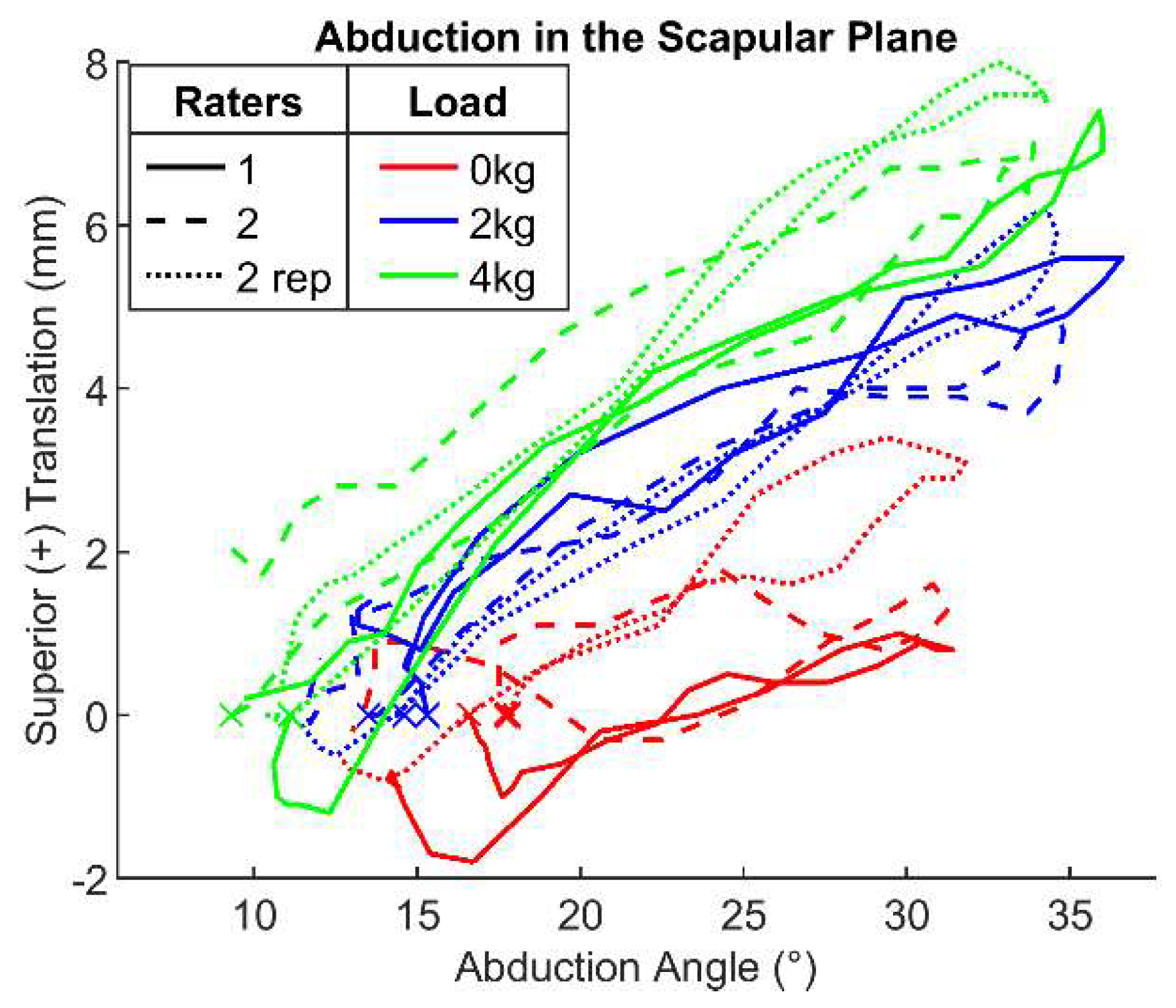
3. Results
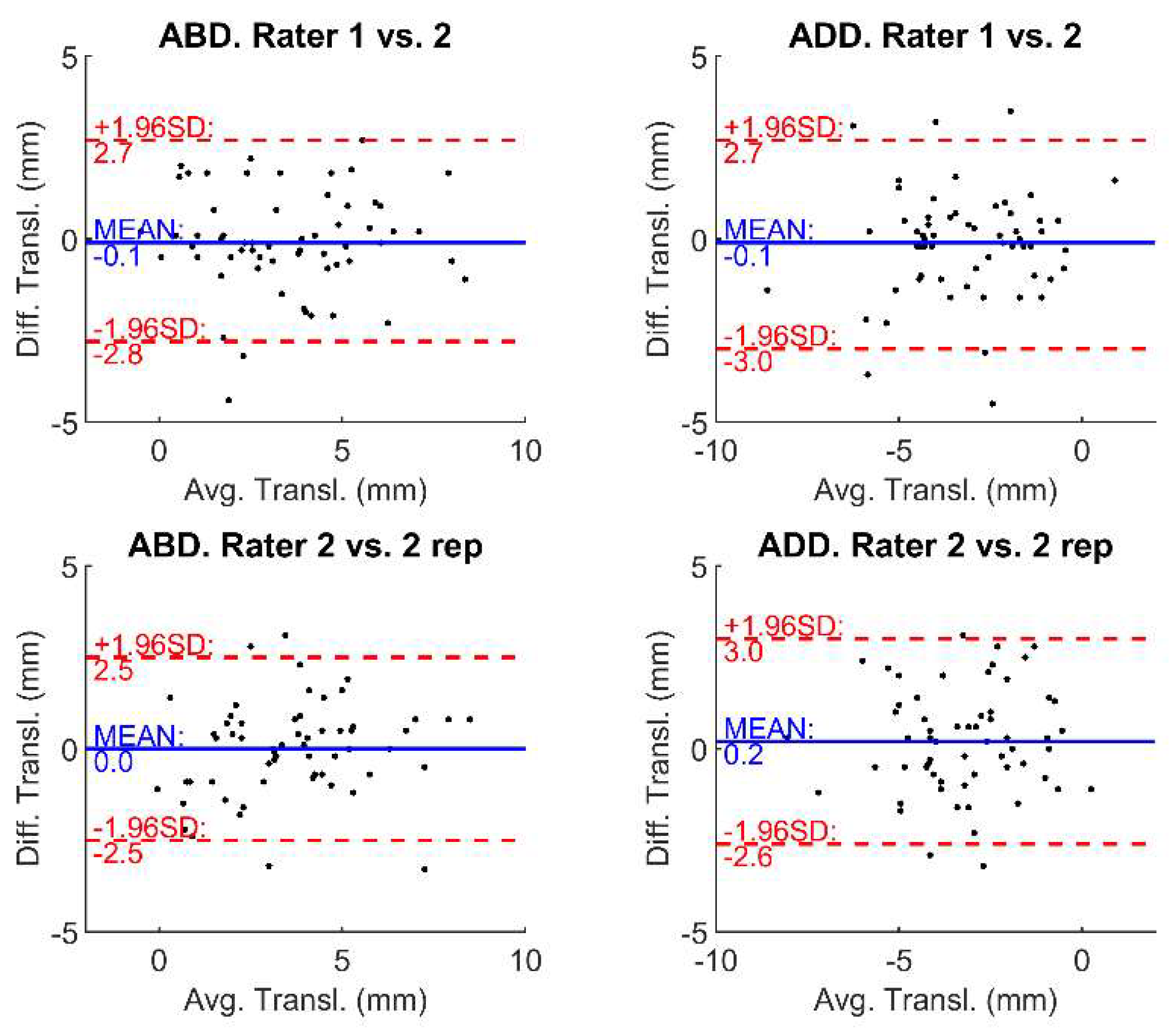
3.1. Interrater Reliability
3.2. Intrarater Reliability
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Konrad, G.G.; Markmiller, M.; Jolly, J.T.; Ruter, A.E.; Sudkamp, N.P.; McMahon, P.J.; Debski, R.E. Decreasing Glenoid Inclination Improves Function in Shoulders with Simulated Massive Rotator Cuff Tears. Clin. Biomech. 2006, 21, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Mura, N.; O’Driscoll, S.W.; Zobitz, M.E.; Heers, G.; Jenkyn, T.R.; Chou, S.M.; Halder, A.M.; An, K.N. The Effect of Infraspinatus Disruption on Glenohumeral Torque and Superior Migration of the Humeral Head: A Biomechanical Study. J. Shoulder Elb. Surg. 2003, 12, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Paletta, G.A.; Warner, J.J.P.; Warren, R.F.; Deutsch, A.; Altchek, D.W. Shoulder Kinematics with Two-Plane x-Ray Evaluation in Patients with Anterior Instability or Rotator Cuff Tearing. J. Shoulder Elb. Surg. 1997, 6, 516–527. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Sher, J.S.; Andersen, W.K.; Garretson, R.; Uribe, J.W.; Hechtman, K.; Neviaser, R.J. Glenohumeral Motion in Patients with Rotator Cuff Tears: A Comparison of Asymptomatic and Symptomatic Shoulders. J. Shoulder Elb. Surg. 2000, 9, 6–11. [Google Scholar] [CrossRef]
- Millett, P.J.; Giphart, J.E.; Wilson, K.J.; Kagnes, K.; Greenspoon, J.A. Alterations in Glenohumeral Kinematics in Patients with Rotator Cuff Tears Measured with Biplane Fluoroscopy. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 446–451. [Google Scholar] [CrossRef]
- Chen, S.K.; Simonian, P.T.; Wickiewicz, T.L.; Otis, J.C.; Warren, R.F. Radiographic Evaluation of Glenohumeral Kinematics: A Muscle Fatigue Model. J. Shoulder Elb. Surg. 1999, 8, 49–52. [Google Scholar] [CrossRef]
- Chopp, J.N.; O’Neill, J.M.; Hurley, K.; Dickerson, C.R. Superior Humeral Head Migration Occurs after a Protocol Designed to Fatigue the Rotator Cuff: A Radiographic Analysis. J. Shoulder Elb. Surg. 2010, 19, 1137–1144. [Google Scholar] [CrossRef]
- Nishinaka, N.; Matsuhisa, T.; Takahashi, Y.; Tsutsui, H.; Sambe, T. Determination of In-Vivo Glenohumeral Translation during Loaded and Unloaded Arm Elevation. Showa Univ. J. Med. Sci. 2016, 28, 309–315. [Google Scholar] [CrossRef] [Green Version]
- Teyhen, D.S.; Christ, T.R.; Ballas, E.R.; Hoppes, C.W.; Walters, J.D.; Christie, D.S.; Dreitzler, G.; Kane, E.J. Digital Fluoroscopic Video Assessment of Glenohumeral Migration: Static vs. Dynamic Conditions. J. Biomech. 2010, 43, 1380–1385. [Google Scholar] [CrossRef]
- Moosmayer, S.; Lund, G.; Seljom, U.; Svege, I.; Hennig, T.; Tariq, R.; Smith, H.J. Comparison between Surgery and Physiotherapy in the Treatment of Small and Medium-Sized Tears of the Rotator Cuff: A Randomised Controlled Study of 103 Patients with One-Year Follow-Up. J. Bone Jt. Surg. Ser. B 2010, 92, 83–91. [Google Scholar] [CrossRef]
- Phillips, N. Tests for Diagnosing Subacromial Impingement Syndrome and Rotator Cuff Disease. Shoulder Elb. 2014, 6, 215–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deutsch, A.; Altchek, D.W.; Schwartz, E.; Otis, J.C.; Warren, R.F. Radiologic Measurement of Superior Displacement of the Humeral Head in the Impingement Syndrome. J. Shoulder Elb. Surg. 1996, 5, 186–193. [Google Scholar] [CrossRef]
- Lagacé, P.Y.; Billuart, F.; Ohl, X.; Skalli, W.; Tétreault, P.; de Guise, J.; Hagemeister, N. Analysis of Humeral Head Displacements from Sequences of Biplanar X-Rays: Repeatability Study and Preliminary Results in Healthy Subjects. Comput. Methods Biomech. Biomed. Engin. 2012, 15, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Poppen, N.; Walker, P. Normal and Abnormal Motion of the Shoulder. J. Bone Jt. Surg. 1976, 58, 195–201. [Google Scholar] [CrossRef]
- Bey, M.J.; Kline, S.K.; Zauel, R.; Lock, T.R.; Kolowich, P.A. Measuring Dynamic In-Vivo Glenohumeral Joint Kinematics: Technique and Preliminary Results. J. Biomech. 2008, 41, 711–714. [Google Scholar] [CrossRef] [Green Version]
- Giphart, J.E.; Brunkhorst, J.P.; Horn, N.H.; Shelburne, K.B.; Torry, M.R.; Millett, P.J. Effect of Plane of Arm Elevation on Glenohumeral Kinematics: A Normative Biplane Fluoroscopy Study. J. Bone Jt. Surg. Ser. A 2013, 95, 238–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kijima, T.; Matsuki, K.; Ochiai, N.; Yamaguchi, T.; Sasaki, Y.; Hashimoto, E.; Sasaki, Y.; Yamazaki, H.; Kenmoku, T.; Yamaguchi, S.; et al. In Vivo 3-Dimensional Analysis of Scapular and Glenohumeral Kinematics: Comparison of Symptomatic or Asymptomatic Shoulders with Rotator Cuff Tears and Healthy Shoulders. J. Shoulder Elb. Surg. 2015, 24, 1817–1826. [Google Scholar] [CrossRef] [Green Version]
- Kozono, N.; Okada, T.; Takeuchi, N.; Hamai, S.; Higaki, H.; Shimoto, T.; Ikebe, S.; Gondo, H.; Nakanishi, Y.; Senju, T.; et al. Dynamic Kinematics of the Glenohumeral Joint in Shoulders with Rotator Cuff Tears. J. Orthop. Surg. Res. 2018, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.J.; Min, Y.K.; Chung, I.K.; Kang, S.W.; Banks, S.A. Comparison of Dynamic In Vivo Shoulder Kinematics Before and After Superior Capsular Reconstruction for Irreparable Rotator Cuff Tears. Orthop. J. Sport. Med. 2021, 9, 2325967120970502. [Google Scholar] [CrossRef]
- Matsuki, K.; Kenmoku, T.; Ochiai, N.; Sugaya, H.; Banks, S.A. Differences in Glenohumeral Translations Calculated with Three Methods: Comparison of Relative Positions and Contact Point. J. Biomech. 2016, 49, 1944–1947. [Google Scholar] [CrossRef]
- Nishinaka, N.; Tsutsui, H.; Mihara, K.; Suzuki, K.; Makiuchi, D.; Kon, Y.; Wright, T.W.; Moser, M.W.; Gamada, K.; Sugimoto, H.; et al. Determination of in Vivo Glenohumeral Translation Using Fluoroscopy and Shape-Matching Techniques. J. Shoulder Elb. Surg. 2008, 17, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Iordache, S.D.; Goldberg, N.; Paz, L.; Peylan, J.; Hur, R.B.; Steinmetz, A. Radiation Exposure from Computed Tomography of the Upper Limbs. Acta Orthop. Belg. 2017, 83, 581–588. [Google Scholar] [PubMed]
- Cherchi, L.; Ciornohac, J.F.; Godet, J.; Clavert, P.; Kempf, J.F. Critical Shoulder Angle: Measurement Reproducibility and Correlation with Rotator Cuff Tendon Tears. Orthop. Traumatol. Surg. Res. 2016, 102, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Chopp-Hurley, J.N.; O’Neill, J.M.; McDonald, A.C.; Maciukiewicz, J.M.; Dickerson, C.R. Fatigue-Induced Glenohumeral and Scapulothoracic Kinematic Variability: Implications for Subacromial Space Reduction. J. Electromyogr. Kinesiol. 2016, 29, 55–63. [Google Scholar] [CrossRef]
- Jacxsens, M.; Van Tongel, A.; Willemot, L.B.; Mueller, A.M.; Valderrabano, V.; De Wilde, L. Accuracy of the Glenohumeral Subluxation Index in Nonpathologic Shoulders. J. Shoulder Elb. Surg. 2015, 24, 541–546. [Google Scholar] [CrossRef]
- Schröter, S.; Krämer, M.; Welke, B.; Hurschler, C.; Russo, R.; Herbst, M.; Stöckle, U.; Ateschrang, A.; Maiotti, M. The Effect of the Arthroscopic Augmentation of the Subscapularis Tendon on Shoulder Instability and Range of Motion: A Biomechanical Study. Clin. Biomech. 2016, 38, 75–83. [Google Scholar] [CrossRef]
- Verstraeten, T.R.G.M.; Deschepper, E.; Jacxsens, M.; Walravens, S.; De Coninck, B.; Pouliart, N.; De Wilde, L.F. Determination of a Reference System for the Three-Dimensional Study of the Glenohumeral Relationship. Skelet. Radiol. 2013, 42, 1061–1071. [Google Scholar] [CrossRef]
- Martin Bland, J.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, R.L.; Moutzouros, V.; Bey, M.J. Asymptomatic Rotator Cuff Tears. JBJS Rev. 2019, 7, e9. [Google Scholar] [CrossRef]
- Yamamoto, A.; Takagishi, K.; Osawa, T.; Yanagawa, T.; Nakajima, D.; Shitara, H.; Kobayashi, T. Prevalence and Risk Factors of a Rotator Cuff Tear in the General Population. J. Shoulder Elb. Surg. 2010, 19, 116–120. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Load | Abduction Translation (mm) | Adduction Translation (mm) | ||
|---|---|---|---|---|
| Asymptomatic Mean (SD) | Symptomatic Mean (SD) | Asymptomatic Mean (SD) | Symptomatic Mean (SD) | |
| 0 kg | 3.3 (2.2) | 2.3 (1.5) | −3.4 (1.9) | −1.9 (1.2) |
| 2 kg | 3.8 (2.1) | 3.9 (2.6) | −3.5 (1.4) | −3.1 (1.9) |
| 4 kg | 4.1 (1.8) | 3.8 (2.2) | −3.9 (1.3) | −3.4 (2.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Croci, E.; Künzler, M.; Börlin, S.; Eckers, F.; Nüesch, C.; Baumgartner, D.; Müller, A.M.; Mündermann, A. Reliability of the Fluoroscopic Assessment of Load-Induced Glenohumeral Translation during a 30° Shoulder Abduction Test. Biomechanics 2022, 2, 255-263. https://0-doi-org.brum.beds.ac.uk/10.3390/biomechanics2020020
Croci E, Künzler M, Börlin S, Eckers F, Nüesch C, Baumgartner D, Müller AM, Mündermann A. Reliability of the Fluoroscopic Assessment of Load-Induced Glenohumeral Translation during a 30° Shoulder Abduction Test. Biomechanics. 2022; 2(2):255-263. https://0-doi-org.brum.beds.ac.uk/10.3390/biomechanics2020020
Chicago/Turabian StyleCroci, Eleonora, Marina Künzler, Sean Börlin, Franziska Eckers, Corina Nüesch, Daniel Baumgartner, Andreas Marc Müller, and Annegret Mündermann. 2022. "Reliability of the Fluoroscopic Assessment of Load-Induced Glenohumeral Translation during a 30° Shoulder Abduction Test" Biomechanics 2, no. 2: 255-263. https://0-doi-org.brum.beds.ac.uk/10.3390/biomechanics2020020