
Targeted Non-Pharmacological Interventions for People Living with Frailty and Chronic Kidney Disease

 ,
,
Abstract
:1. Introduction
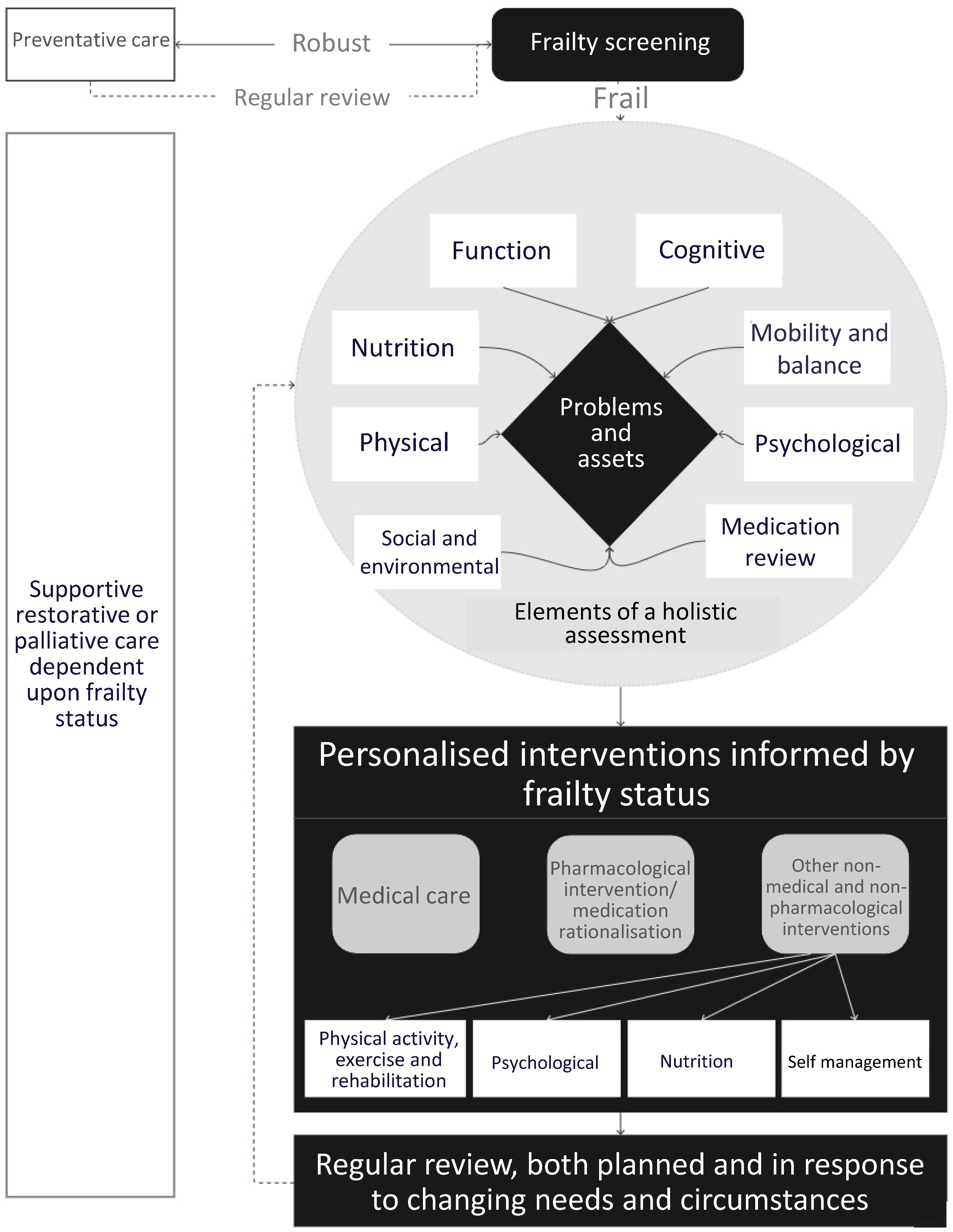
2. Frailty Identification and Assessment
3. Self-Management Interventions
4. Physical Activity and Exercise-Based Rehabilitation
5. Nutrition
6. Non-Pharmacological Interventions for Depression
7. Digital Health Interventions
8. Considerations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R. Cardiovascular Disease and Frailty: What Are the Mechanistic Links? Clin. Chem. 2019, 65, 80–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, K.; Vetrano, D.L.; Padua, L.; Romano, V.; Rivoiro, C.; Scelfo, B.; Marengoni, A.; Bernabei, R.; Onder, G. Frailty Syndromes in Persons With Cerebrovascular Disease: A Systematic Review and Meta-Analysis. Front. Neurol. 2019, 10, 1255. [Google Scholar] [CrossRef]
- El Haddad, K.; Rolland, Y.; Gérard, S.; Mourey, L.; Sourdet, S.; Vellas, B.; Stephan, E.; Abellan Van Kan, G.; de Souto Barreto, P.; Balardy, L. No Difference in the Phenotypic Expression of Frailty among Elderly Patients Recently Diagnosed with Cancer Vs Cancer Free Patients. J. Nutr. Health Aging 2020, 24, 147–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilgin, S.; Aktas, G.; Kurtkulagi, O.; Atak, B.M.; Duman, T.T. Edmonton frail score is associated with diabetic control in elderly type 2 diabetic subjects. J. Diabetes Metab. Disord. 2020, 19, 511–514. [Google Scholar] [CrossRef] [PubMed]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Lopez Samaniego, L.; Rodríguez-Mañas, L.; Bernabei, R.; Onder, G. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A 2018, 74, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-J.; Son, Y.-J. Prevalence and Associated Factors of Frailty and Mortality in Patients with End-Stage Renal Disease Undergoing Hemodialysis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Quint, E.E.; Zogaj, D.; Banning, L.B.D.; Benjamens, S.; Annema, C.; Bakker, S.J.L.; Nieuwenhuijs-Moeke, G.J.; Segev, D.L.; McAdams-DeMarco, M.A.; Pol, R.A. Frailty and Kidney Transplantation: A Systematic Review and Meta-analysis. Transpl. Direct 2021, 7, e701. [Google Scholar] [CrossRef]
- Brown, S.A.; Tyrer, F.C.; Clarke, A.L.; Lloyd-Davies, L.H.; Stein, A.G.; Tarrant, C.; Burton, J.O.; Smith, A.C. Symptom burden in patients with chronic kidney disease not requiring renal replacement therapy. Clin. Kidney J. 2017, 10, 788–796. [Google Scholar] [CrossRef]
- Gregg, L.P.; Jain, N.; Carmody, T.; Minhajuddin, A.T.; Rush, A.J.; Trivedi, M.H.; Hedayati, S.S. Fatigue in Nondialysis Chronic Kidney Disease: Correlates and Association with Kidney Outcomes. Am. J. Nephrol. 2019, 50, 37–47. [Google Scholar] [CrossRef]
- Goto, N.A.; van Loon, I.N.; Morpey, M.I.; Verhaar, M.C.; Willems, H.C.; Emmelot-Vonk, M.H.; Bots, M.L.; Boereboom, F.T.J.; Hamaker, M.E. Geriatric Assessment in Elderly Patients with End-Stage Kidney Disease. Nephron 2019, 141, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L.; Dalrymple, L.S.; Delgado, C.; Chertow, G.M.; Segal, M.R.; Chiang, J.; Grimes, B.; Kaysen, G.A. Factors Associated with Frailty and Its Trajectory among Patients on Hemodialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1100–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAdams-DeMarco, M.A.; Isaacs, K.; Darko, L.; Salter, M.L.; Gupta, N.; King, E.A.; Walston, J.; Segev, D.L. Changes in Frailty After Kidney Transplantation. J. Am. Geriatr. Soc. 2015, 63, 2152–2157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHS England. Supporting Routine Frailty Identification and Frailty through the GP Contract; NHS England: Leeds, UK, 2017. Available online: https://www.england.nhs.uk/publication/supporting-routine-frailty-identification-and-frailty-through-the-gp-contract-20172018/ (accessed on 16 May 2022).
- National Institute for Health and Care Excellence. Multimorbidity: Clinical Assessment and Management. 2017. Available online: https://www.nice.org.uk/guidance/qs153 (accessed on 19 January 2022).
- National Institute for Health and Care Excellence. Falls in Older People. 2015. Available online: https://www.nice.org.uk/guidance/cg161 (accessed on 19 January 2022).
- NHS England. Personalised Care. 2019. Available online: https://www.england.nhs.uk/personalisedcare/ (accessed on 19 January 2022).
- NHS England. The NHS Long Term Plan. 2019. Available online: https://www.england.nhs.uk/long-term-plan/ (accessed on 19 January 2022).
- Salter, M.L.; Gupta, N.; Massie, A.B.; McAdams-DeMarco, M.A.; Law, A.H.; Jacob, R.L.; Gimenez, L.F.; Jaar, B.G.; Walston, J.D.; Segev, D.L. Perceived frailty and measured frailty among adults undergoing hemodialysis: A cross-sectional analysis. BMC Geriatr 2015, 15, 52. [Google Scholar] [CrossRef] [Green Version]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Liu, Q.; Ji, J. The prevalence of frailty in patients on hemodialysis: A systematic review and meta-analysis. Int. Urol. Nephrol. 2020, 52, 115–120. [Google Scholar] [CrossRef]
- Zhang, Q.; Ma, Y.; Lin, F.; Zhao, J.; Xiong, J. Frailty and mortality among patients with chronic kidney disease and end-stage renal disease: A systematic review and meta-analysis. Int. Urol. Nephrol. 2020, 52, 363–370. [Google Scholar] [CrossRef]
- Mei, F.; Gao, Q.; Chen, F.; Zhao, L.; Shang, Y.; Hu, K.; Zhang, W.; Zhao, B.; Ma, B. Frailty as a Predictor of Negative Health Outcomes in Chronic Kidney Disease: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2021, 22, 535–543. [Google Scholar] [CrossRef]
- Vezza, C.; Vettoretti, S.; Caldiroli, L.; Bergamaschini, L.; Messa, P.; Cesari, M. Use of the Frailty Index in Older Persons With Chronic Kidney Disease. J. Am. Med. Dir. Assoc. 2019, 20, 1179–1180. [Google Scholar] [CrossRef]
- Clegg, A.; Bates, C.; Young, J.; Ryan, R.; Nichols, L.; Ann Teale, E.; Mohammed, M.A.; Parry, J.; Marshall, T. Development and validation of an electronic frailty index using routine primary care electronic health record data. Age Ageing 2016, 45, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sam, R.; Usha, A.; Kuldeep, S.; John, S.; John, B.; Andy, C.; Robert, W.; Jenny, H.; Mooney, A. The Electronic Frailty Index (EFI) Indicates Mortality Risk in End Stage Kidney Disease Patients on Dialysis. Nephrol. Dial. Transplant. 2019, 34, gfz096.FO032. [Google Scholar] [CrossRef]
- Worthen, G.; Tennankore, K. Frailty Screening in Chronic Kidney Disease: Current Perspectives. Int. J. Nephrol. Renov. Dis. 2019, 12, 229–239. [Google Scholar] [CrossRef] [Green Version]
- Nixon, A.C.; Bampouras, T.M.; Pendleton, N.; Mitra, S.; Dhaygude, A.P. Diagnostic Accuracy of Frailty Screening Methods in Advanced Chronic Kidney Disease. Nephron 2019, 141, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Loon, I.N.; Goto, N.A.; Boereboom, F.T.J.; Bots, M.L.; Verhaar, M.C.; Hamaker, M.E. Frailty Screening Tools for Elderly Patients Incident to Dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1480–1488. [Google Scholar] [CrossRef] [Green Version]
- Van Munster, B.C.; Drost, D.; Kalf, A.; Vogtlander, N.P. Discriminative value of frailty screening instruments in end-stage renal disease. Clin. Kidney J. 2016, 9, 606–610. [Google Scholar] [CrossRef] [Green Version]
- Farrington, K.; Covic, A.; Aucella, F.; Clyne, N.; de Vos, L.; Findlay, A.; Fouque, D.; Grodzicki, T.; Iyasere, O.; Jager, K.J.; et al. Clinical Practice Guideline on management of older patients with chronic kidney disease stage 3b or higher (eGFR <45 mL/min/1.73 m2). Nephrol. Dial. Transpl. 2016, 31, ii1–ii66. [Google Scholar] [CrossRef] [Green Version]
- Church, S.; Rogers, E.; Rockwood, K.; Theou, O. A scoping review of the Clinical Frailty Scale. BMC Geriatr. 2020, 20, 393. [Google Scholar] [CrossRef]
- Kumarasinghe, A.P.; Chakera, A.; Chan, K.; Dogra, S.; Broers, S.; Maher, S.; Inderjeeth, C.; Jacques, A. Incorporating the Clinical Frailty Scale into routine outpatient nephrology practice: An observational study of feasibility and associations. Intern. Med. J. 2021, 51, 1269–1277. [Google Scholar] [CrossRef]
- Alfaadhel, T.A.; Soroka, S.D.; Kiberd, B.A.; Landry, D.; Moorhouse, P.; Tennankore, K.K. Frailty and mortality in dialysis: Evaluation of a clinical frailty scale. Clin. J. Am. Soc. Nephrol. 2015, 10, 832–840. [Google Scholar] [CrossRef] [Green Version]
- Nixon, A.C.; Brown, J.; Brotherton, A.; Harrison, M.; Todd, J.; Brannigan, D.; Ashcroft, Q.; So, B.; Pendleton, N.; Ebah, L.; et al. Implementation of a frailty screening programme and Geriatric Assessment Service in a nephrology centre: A quality improvement project. J. Nephrol. 2020, 34, 1215–1224. [Google Scholar] [CrossRef] [PubMed]
- Pugh, J.; Aggett, J.; Goodland, A.; Prichard, A.; Thomas, N.; Donovan, K.; Roberts, G. Frailty and comorbidity are independent predictors of outcome in patients referred for pre-dialysis education. Clin. Kidney J. 2016, 9, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Iyasere, O.U.; Brown, E.A.; Johansson, L.; Huson, L.; Smee, J.; Maxwell, A.P.; Farrington, K.; Davenport, A. Quality of Life and Physical Function in Older Patients on Dialysis: A Comparison of Assisted Peritoneal Dialysis with Hemodialysis. Clin. J. Am. Soc. Nephrol. 2016, 11, 423–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Loon, I.N.; Joosten, H.; Iyasere, O.; Johansson, L.; Hamaker, M.E.; Brown, E.A. The prevalence and impact of falls in elderly dialysis patients: Frail elderly Patient Outcomes on Dialysis (FEPOD) study. Arch. Gerontol. Geriatr. 2019, 83, 285–291. [Google Scholar] [CrossRef]
- Neradova, A.; Vajgel, G.; Hendra, H.; Antonelou, M.; Kostakis, I.D.; Wright, D.; Masson, P.; Milne, S.E.; Jones, G.; Salama, A.; et al. Frailty score before admission as risk factor for mortality of renal patients during the first wave of the COVID pandemic in London. G Ital. Nefrol. 2021, 38, 2021. [Google Scholar]
- Wu, H.H.L.; Van Mierlo, R.; McLauchlan, G.; Challen, K.; Mitra, S.; Dhaygude, A.P.; Nixon, A.C. Prognostic performance of clinical assessment tools following hip fracture in patients with chronic kidney disease. Int. Urol. Nephrol. 2021, 53, 2359–2367. [Google Scholar] [CrossRef]
- Kamijo, Y.; Kanda, E.; Ishibashi, Y.; Yoshida, M. Sarcopenia and Frailty in PD: Impact on Mortality, Malnutrition, and Inflammation. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2018, 38, 447–454. [Google Scholar] [CrossRef]
- Hwang, D.; Lee, E.; Park, S.; Yoo, B.C.; Park, S.; Choi, K.J.; Oh, S.; Kim, M.J.; Kim, H.; Jeon, J.S.; et al. Validation of risk prediction tools in elderly patients who initiate dialysis. Int. Urol. Nephrol. 2019, 51, 1231–1238. [Google Scholar] [CrossRef]
- Iyasere, O.; Brown, E.A.; Johansson, L.; Davenport, A.; Farrington, K.; Maxwell, A.P.; Collinson, H.; Fan, S.; Habib, A.-M.; Stoves, J.; et al. Quality of life with conservative care compared with assisted peritoneal dialysis and haemodialysis. Clin. Kidney J. 2018, 12, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Ellis, G.; Gardner, M.; Tsiachristas, A.; Langhorne, P.; Burke, O.; Harwood, R.H.; Conroy, S.P.; Kircher, T.; Somme, D.; Saltvedt, I.; et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst. Rev. 2017, 9, Cd006211. [Google Scholar] [CrossRef] [Green Version]
- Parker, S.G.; McCue, P.; Phelps, K.; McCleod, A.; Arora, S.; Nockels, K.; Kennedy, S.; Roberts, H.; Conroy, S. What is Comprehensive Geriatric Assessment (CGA)? An umbrella review. Age Ageing 2018, 47, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, R.K.; Haines, C.; Gorbatkin, S.M.; Schlanger, L.; Shaban, H.; Schell, J.O.; Gurley, S.B.; Colón-Emeric, C.S.; Bowling, C.B. Incorporating Geriatric Assessment into a Nephrology Clinic: Preliminary Data from Two Models of Care. J. Am. Geriatr. Soc. 2016, 64, 2154–2158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, G.; Taniguchi, Y.; Iliffe, S.; Jivraj, S.; Walters, K. Transitions between frailty states among community-dwelling older people: A systematic review and meta-analysis. Ageing Res. Rev. 2019, 50, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Voorend, C.G.N.; Joosten, H.; Berkhout-Byrne, N.C.; Diepenbroek, A.; Franssen, C.F.M.; Bos, W.J.W.; Van Buren, M.; Mooijaart, S.P. Design of a consensus-based geriatric assessment tailored for older chronic kidney disease patients: Results of a pragmatic approach. Eur. Geriatr. Med. 2021, 12, 931–942. [Google Scholar] [CrossRef]
- Van Oevelen, M.; Abrahams, A.C.; Bos, W.J.W.; Emmelot-Vonk, M.H.; Mooijaart, S.P.; van Diepen, M.; van Jaarsveld, B.C.; van Eck van der Sluijs, A.; Voorend, C.G.N.; van Buren, M.; et al. DIALysis or not: Outcomes in older kidney patients with GerIatriC Assessment (DIALOGICA): Rationale and design. BMC Nephrol. 2021, 22, 39. [Google Scholar] [CrossRef]
- Chang, J.; Gao, Y.; Fang, X.-Y.; Zhao, S.-M.; Hou, Y.-P.; Sun, Q.-M. Individualized intervention for frail non-dialysis elderly patients with chronic kidney disease: Protocol for a randomized controlled trial. BMC Geriatr. 2020, 20, 159. [Google Scholar] [CrossRef]
- Corbin, J.M.; Strauss, A. Unending Work and Care: Managing Chronic Illness at Home, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1988; ISBN 978-1555420826. [Google Scholar]
- Lorig, K.R.; Holman, H. Self-management education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef]
- Lightfoot, C.J.; Nair, D.; Bennett, P.N.; Smith, A.C.; Griffin, A.D.; Warren, M.; Wilkinson, T.J. Patient Activation: The Cornerstone of Effective Self-Management in Chronic Kidney Disease? Kidney Dial. 2022, 2, 91–105. [Google Scholar] [CrossRef]
- Steverink, N.; Lindenberg, S.; Slaets, J.P.J. How to understand and improve older people’s self-management of wellbeing. Eur. J. Ageing 2005, 2, 235–244. [Google Scholar] [CrossRef] [Green Version]
- Cramm, J.M.; Twisk, J.; Nieboer, A.P. Self-management abilities and frailty are important for healthy aging among community-dwelling older people; a cross-sectional study. BMC Geriatr. 2014, 14, 28. [Google Scholar] [CrossRef] [Green Version]
- Van het Bolscher-Niehuis, M.J.T.; den Ouden, M.E.M.; de Vocht, H.M.; Francke, A.L. Effects of self-management support programmes on activities of daily living of older adults: A systematic review. Int. J. Nurs. Stud. 2016, 61, 230–247. [Google Scholar] [CrossRef] [Green Version]
- Son, Y.-J.; Shim, D.K.; Seo, E.K.; Seo, E.J. Health Literacy but Not Frailty Predict Self-Care Behaviors in Patients with Heart Failure. Int. J. Environ. Res. Public Health 2018, 15, 2474. [Google Scholar] [CrossRef] [Green Version]
- Boersma, P.; Vaalburg, A.M.; Albers, M.; de Boer, C.J.M.; Gobbens, R.J.J. The Implications for Nursing Care of Frail Elderly with Limited Self-Management Abilities: A Cross-Sectional Study in the Netherlands. Lupine Online J. Nurs. Healthc. 2021, 3, 270–277. [Google Scholar]
- Walston, J.; Buta, B.; Xue, Q.L. Frailty Screening and Interventions: Considerations for Clinical Practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Liljas, A.E.M.; Iliffe, S. Frailty syndrome: Implications and challenges for health care policy. Risk Manag. Healthc. Policy 2019, 12, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.H.; Do, J.Y.; Lee, S.Y.; Kim, J.C. Effect of dialysis modality on frailty phenotype, disability, and health-related quality of life in maintenance dialysis patients. PLoS ONE 2017, 12, e0176814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Chronic Kidney Disease: Assessment and Management; NICE Guideline [NG203]; NICE: London, UK, 2014. Available online: https://www.nice.org.uk/guidance/ng203 (accessed on 16 May 2022).
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- Nixon, A.C.; Bampouras, T.M.; Gooch, H.J.; Young, H.M.L.; Finlayson, K.W.; Pendleton, N.; Mitra, S.; Brady, M.E.; Dhaygude, A.P. Home-based exercise for people living with frailty and chronic kidney disease: A mixed-methods pilot randomised controlled trial. PLoS ONE 2021, 16, e0251652. [Google Scholar] [CrossRef]
- Young, H.M.L.; March, D.S.; Highton, P.J.; Graham-Brown, M.P.M.; Churchward, D.C.; Grantham, C.; Goodliffe, S.; Jones, W.; Cheung, M.M.; Greenwood, S.A.; et al. Exercise for people living with frailty and receiving haemodialysis: A mixed-methods randomised controlled feasibility study. BMJ Open 2020, 10, e041227. [Google Scholar] [CrossRef]
- Sánchez-Tocino, M.L.; González-Parra, E.; Serrano, B.M.; Gracia-Iguacel, C.; de-Alba-Peñaranda, A.M.; López-González, A.; Olegario, M.G.; Ortíz, A.; Mas-Fontao, S. Evaluation of the impact of an intradialytic exercise program on sarcopenia in very elderly hemodialysis patients. Clin. Kidney J. 2022, sfac046. [Google Scholar] [CrossRef]
- Wilkinson, T.J.; Watson, E.L.; Xenophontos, S.; Gould, D.W.; Smith, A.C. The “Minimum Clinically Important Difference” in Frequently Reported Objective Physical Function Tests After a 12-Week Renal Rehabilitation Exercise Intervention in Nondialysis Chronic Kidney Disease. Am. J. Phys. Med. Rehabil. 2019, 98, 431–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, Y.; Kamiya, K.; Tanaka, S.; Hoshi, K.; Watanabe, T.; Harada, M.; Matsuzawa, R.; Shimoda, T.; Yamamoto, S.; Matsunaga, Y.; et al. Effects of electrical muscle stimulation in frail elderly patients during haemodialysis (DIAL): Rationale and protocol for a crossover randomised controlled trial. BMJ Open 2019, 9, e025389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidd, T.; Mold, F.; Jones, C.; Ream, E.; Grosvenor, W.; Sund-Levander, M.; Tingström, P.; Carey, N. What are the most effective interventions to improve physical performance in pre-frail and frail adults? A systematic review of randomised control trials. BMC Geriatr. 2019, 19, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [Green Version]
- Giné-Garriga, M.; Roqué-Fíguls, M.; Coll-Planas, L.; Sitjà-Rabert, M.; Salvà, A. Physical exercise interventions for improving performance-based measures of physical function in community-dwelling, frail older adults: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 753–769. [Google Scholar] [CrossRef]
- Puts, M.T.E.; Toubasi, S.; Andrew, M.K.; Ashe, M.C.; Ploeg, J.; Atkinson, E.; Ayala, A.P.; Roy, A.; Rodríguez Monforte, M.; Bergman, H.; et al. Interventions to prevent or reduce the level of frailty in community-dwelling older adults: A scoping review of the literature and international policies. Age Ageing 2017, 46, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef]
- Beckwée, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I. Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019, 1, Cd012424. [Google Scholar] [CrossRef]
- Young, H.M.L.; March, D.S.; Graham-Brown, M.P.M.; Jones, A.W.; Curtis, F.; Grantham, C.S.; Churchward, D.R.; Highton, P.; Smith, A.C.; Singh, S.J.; et al. Effects of intradialytic cycling exercise on exercise capacity, quality of life, physical function and cardiovascular measures in adult haemodialysis patients: A systematic review and meta-analysis. Nephrol. Dial. Transpl. 2018, 33, 1436–1445. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, S.A.; Koufaki, P.; Macdonald, J.H.; Bulley, C.; Bhandari, S.; Burton, J.O.; Dasgupta, I.; Farrington, K.; Ford, I.; Kalra, P.A.; et al. Exercise programme to improve quality of life for patients with end-stage kidney disease receiving haemodialysis: The PEDAL RCT. Health Technol. Assess. 2021, 25, 1–52. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.N.; Fraser, S.; Barnard, R.; Haines, T.; Ockerby, C.; Street, M.; Wang, W.C.; Daly, R. Effects of an intradialytic resistance training programme on physical function: A prospective stepped-wedge randomized controlled trial. Nephrol. Dial. Transpl. 2016, 31, 1302–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hristea, D.; Deschamps, T.; Paris, A.; Lefrançois, G.; Collet, V.; Savoiu, C.; Ozenne, S.; Coupel, S.; Testa, A.; Magnard, J. Combining intra-dialytic exercise and nutritional supplementation in malnourished older haemodialysis patients: Towards better quality of life and autonomy. Nephrology 2016, 21, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Dogra, S.; Copeland, J.L.; Altenburg, T.M.; Heyland, D.K.; Owen, N.; Dunstan, D.W. Start with reducing sedentary behavior: A stepwise approach to physical activity counseling in clinical practice. Patient Educ. Couns. 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- Lerma, N.L.; Cho, C.C.; Swartz, A.M.; Miller, N.E.; Keenan, K.G.; Strath, S.J. Isotemporal Substitution of Sedentary Behavior and Physical Activity on Function. Med. Sci. Sports Exerc. 2018, 50, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Biddle, S.J.H.; Buman, M.P.; Chastin, S.; Ekelund, U.; Friedenreich, C.M.; Katzmarzyk, P.T.; Leitzmann, M.F.; Stamatakis, E.; van der Ploeg, H.P.; et al. New global guidelines on sedentary behaviour and health for adults: Broadening the behavioural targets. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 151. [Google Scholar] [CrossRef]
- Da Silva Coqueiro, R.; de Queiroz, B.M.; Oliveira, D.S.; das Merces, M.C.; Oliveira Carneiro, J.A.; Pereira, R.; Fernandes, M.H. Cross-sectional relationships between sedentary behavior and frailty in older adults. J Sports Med. Phys. Fit. 2017, 57, 825–830. [Google Scholar] [CrossRef]
- Wilkinson, T.J.; Clarke, A.L.; Nixon, D.G.D.; Hull, K.L.; Song, Y.; Burton, J.O.; Yates, T.; Smith, A.C. Prevalence and correlates of physical activity across kidney disease stages: An observational multicentre study. Nephrol. Dial. Transpl. 2021, 36, 641–649. [Google Scholar] [CrossRef]
- Glavinovic, T.; Ferguson, T.; Komenda, P.; Rigatto, C.; Duhamel, T.A.; Tangri, N.; Bohm, C. CKD and Sedentary Time: Results From the Canadian Health Measures Survey. Am. J. Kidney Dis. 2018, 72, 529–537. [Google Scholar] [CrossRef]
- Sheshadri, A.; Kittiskulnam, P.; Lai, J.C.; Johansen, K.L. Effect of a pedometer-based walking intervention on body composition in patients with ESRD: A randomized controlled trial. BMC Nephrol. 2020, 21, 100. [Google Scholar] [CrossRef] [Green Version]
- Baggetta, R.; D’Arrigo, G.; Torino, C.; ElHafeez, S.A.; Manfredini, F.; Mallamaci, F.; Zoccali, C.; Tripepi, G.; Bolignano, D.; Lamberti, N.; et al. Effect of a home based, low intensity, physical exercise program in older adults dialysis patients: A secondary analysis of the EXCITE trial. BMC Geriatr. 2018, 18, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawney, K.W.; Tawney, P.J.; Hladik, G.; Hogan, S.L.; Falk, R.J.; Weaver, C.; Moore, D.T.; Lee, M.Y. The life readiness program: A physical rehabilitation program for patients on hemodialysis. Am. J. Kidney Dis. 2000, 36, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Lyden, K.; Boucher, R.; Wei, G.; Zhou, N.; Christensen, J.; Chertow, G.M.; Greene, T.; Beddhu, S. Targeting Sedentary Behavior in CKD: A Pilot and Feasibility Randomized Controlled Trial. Clin. J. Am. Soc. Nephrol. 2021, 16, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Van Loon, I.N.; Goto, N.A.; Boereboom, F.T.J.; Bots, M.L.; Hoogeveen, E.K.; Gamadia, L.; van Bommel, E.F.H.; van de Ven, P.J.G.; Douma, C.E.; Vincent, H.H.; et al. Geriatric Assessment and the Relation with Mortality and Hospitalizations in Older Patients Starting Dialysis. Nephron 2019, 143, 108–119. [Google Scholar] [CrossRef]
- Chou, H.-Y.; Chen, S.-C.; Yen, T.-H.; Han, H.-M. Effect of a Virtual Reality-Based Exercise Program on Fatigue in Hospitalized Taiwanese End-Stage Renal Disease Patients Undergoing Hemodialysis. Clin. Nurs. Res. 2020, 29, 368–374. [Google Scholar] [CrossRef]
- Wytsma-Fisher, K.; Mustata, S.; Cowan, T.; Ester, M.; Culos-Reed, S.N. A Physical Activity Intervention Feasibility Study for Kidney Inpatients: A Basic Research Protocol. Can. J. Kidney Health Dis. 2021, 8, 2054358120987052. [Google Scholar] [CrossRef]
- Wynter-Blyth, V.; Moorthy, K. Prehabilitation: Preparing patients for surgery. BMJ 2017, 358, j3702. [Google Scholar] [CrossRef]
- Willingham, F.C.; Speelman, I.; Hamilton, J.; von Fragstein, G.; Shaw, S.; Taal, M.W. Feasibility and effectiveness of pre-emptive rehabilitation in persons approaching dialysis (PREHAB). J. Ren. Care 2019, 45, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, E.C.; Hickson, L.J.; Weatherly, R.M.; Thompson, K.L.; Walker, H.A.; Rasmussen, J.M.; Stewart, T.L.; Garrett, J.K.; Amer, H.; Kennedy, C.C. Protocolized exercise improves frailty parameters and lower extremity impairment: A promising prehabilitation strategy for kidney transplant candidates. Clin. Transpl. 2020, 34, e14017. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Ying, H.; Van Pilsum Rasmussen, S.; Schrack, J.; Haugen, C.E.; Chu, N.M.; González Fernández, M.; Desai, N.; Walston, J.D.; Segev, D.L. Prehabilitation prior to kidney transplantation: Results from a pilot study. Clin. Transpl. 2019, 33, e13450. [Google Scholar] [CrossRef]
- Pérez-Sáez, M.J.; Morgado-Pérez, A.; Faura, A.; Muñoz-Redondo, E.; Gárriz, M.; Muns, M.D.; Nogués, X.; Marco, E.; Pascual, J. The FRAILMar Study Protocol: Frailty in Patients With Advanced Chronic Kidney Disease Awaiting Kidney Transplantation. A Randomized Clinical Trial of Multimodal Prehabilitation. Front. Med. 2021, 8, 647. [Google Scholar] [CrossRef] [PubMed]
- Barawid, E.; Covarrubias, N.; Tribuzio, B.; Liao, S. The benefits of rehabilitation for palliative care patients. Am. J. Hosp. Palliat. Care 2015, 32, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Ramanjulu, R. Palliative Rehabilitation: The Essence of Personalized Care. Indian J. Palliat. Care 2020, 26, 399–400. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-López, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [Green Version]
- Ni Lochlainn, M.; Cox, N.J.; Wilson, T.; Hayhoe, R.P.G.; Ramsay, S.E.; Granic, A.; Isanejad, M.; Roberts, H.C.; Wilson, D.; Welch, C.; et al. Nutrition and Frailty: Opportunities for Prevention and Treatment. Nutrients 2021, 13, 2349. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Kalantar-Zadeh, K.; Kopple, J.D. Frailty and protein-energy wasting in elderly patients with end stage kidney disease. J. Am. Soc. Nephrol. 2013, 24, 337–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrero, J.J.; Stenvinkel, P.; Cuppari, L.; Ikizler, T.A.; Kalantar-Zadeh, K.; Kaysen, G.; Mitch, W.E.; Price, S.R.; Wanner, C.; Wang, A.Y.; et al. Etiology of the protein-energy wasting syndrome in chronic kidney disease: A consensus statement from the International Society of Renal Nutrition and Metabolism (ISRNM). J. Ren. Nutr. 2013, 23, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Byham-Gray, L.; Burrowes, J.D.; Chertow, G.M. Nutrition in Kidney Disease, 3rd ed.; Springer International Publishing: Cham, Switzerland, 2020. [Google Scholar]
- NHS RightCare. NHS RightCare: Frailty Toolkit; National Institute for Health and Care Excellence: London, UK, 2019. Available online: https://www.england.nhs.uk/rightcare/wp-content/uploads/sites/40/2019/07/frailty-toolkit-june-2019-v1.pdf (accessed on 16 May 2022).
- Wright, M.; Southcott, E.; MacLaughlin, H.; Wineberg, S. Clinical practice guideline on undernutrition in chronic kidney disease. BMC Nephrol. 2019, 20, 370. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Woodhouse, L.; Rodríguez-Mañas, L.; Fried, L.P.; Woo, J.; Aprahamian, I.; Sanford, A.; Lundy, J.; et al. Physical Frailty: ICFSR International Clinical Practice Guidelines for Identification and Management. J. Nutr. Health Aging 2019, 23, 771–787. [Google Scholar] [CrossRef] [Green Version]
- Moraes, M.B.; Avgerinou, C.; Fukushima, F.B.; Vidal, E.I.O. Nutritional interventions for the management of frailty in older adults: Systematic review and meta-analysis of randomized clinical trials. Nutr. Rev. 2021, 79, 889–913. [Google Scholar] [CrossRef] [PubMed]
- Dedeyne, L.; Deschodt, M.; Verschueren, S.; Tournoy, J.; Gielen, E. Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: A systematic review. Clin. Interv. Aging 2017, 12, 873–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, B.M.; Dutton, M.; Day, E.; Jackson, T.A.; Ferro, C.J.; Sharif, A. Frailty Intervention Trial iN End-Stage patientS on haemodialysis (FITNESS): Study protocol for a randomised controlled trial. Trials 2018, 19, 457. [Google Scholar] [CrossRef] [PubMed]
- Chilcot, J.; Guirguis, A.; Friedli, K.; Almond, M.; Day, C.; Da Silva-Gane, M.; Davenport, A.; Fineberg, N.A.; Spencer, B.; Wellsted, D.; et al. Depression Symptoms in Haemodialysis Patients Predict All-Cause Mortality but Not Kidney Transplantation: A Cause-Specific Outcome Analysis. Ann. Behav. Med. 2018, 52, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.C.; Chiu, Y.W.; Hung, C.C.; Hwang, S.J.; Tsai, J.C.; Wang, S.L.; Lin, M.Y.; Chen, H.C. Association of symptoms of depression with progression of CKD. Am. J. Kidney Dis. 2012, 60, 54–61. [Google Scholar] [CrossRef]
- Farrokhi, F.; Abedi, N.; Beyene, J.; Kurdyak, P.; Jassal, S.V. Association between depression and mortality in patients receiving long-term dialysis: A systematic review and meta-analysis. Am. J. Kidney Dis. 2014, 63, 623–635. [Google Scholar] [CrossRef]
- Palmer, S.; Vecchio, M.; Craig, J.C.; Tonelli, M.; Johnson, D.W.; Nicolucci, A.; Pellegrini, F.; Saglimbene, V.; Logroscino, G.; Fishbane, S.; et al. Prevalence of depression in chronic kidney disease: Systematic review and meta-analysis of observational studies. Kidney Int. 2013, 84, 179–191. [Google Scholar] [CrossRef] [Green Version]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.T.; et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Gregg, L.P.; Carmody, T.; Le, D.; Martins, G.; Trivedi, M.; Hedayati, S.S. A Systematic Review and Meta-Analysis of Depression and Protein-Energy Wasting in Kidney Disease. Kidney Int. Rep. 2019, 5, 318–330. [Google Scholar] [CrossRef] [Green Version]
- Soni, R.K.; Weisbord, S.D.; Unruh, M.L. Health-related quality of life outcomes in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2010, 19, 153–159. [Google Scholar] [CrossRef]
- Sy, J.; McCulloch, C.E.; Johansen, K.L. Depressive symptoms, frailty, and mortality among dialysis patients. Hemodial. Int. 2019, 23, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Konel, J.M.; Warsame, F.; Ying, H.; Haugen, C.E.; Mountford, A.; Chu, N.M.; Crews, D.C.; Desai, N.M.; Garonzik-Wang, J.M.; Walston, J.D.; et al. Depressive symptoms, frailty, and adverse outcomes among kidney transplant recipients. Clin. Transplant. 2018, 32, e13391. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.C.; Chan, G.C.; Ng, J.K.; Chow, K.M.; Kwan, B.C.; Cheng, P.M.; Kwong, V.W.; Law, M.C.; Leung, C.B.; Li, P.K. Depression and Physical Frailty Have Additive Effect on the Nutritional Status and Clinical Outcome of Chinese Peritoneal Dialysis. Kidney Blood Press. Res. 2018, 43, 914–923. [Google Scholar] [CrossRef]
- Chan, G.C.-K.; Ng, J.K.-C.; Chow, K.-M.; Kwan, B.C.-H.; Kwong, V.W.-K.; Pang, W.-F.; Cheng, P.M.-S.; Law, M.-C.; Leung, C.-B.; Li, P.K.-T.; et al. Depression does not predict clinical outcome of Chinese peritoneal Dialysis patients after adjusting for the degree of frailty. BMC Nephrol. 2020, 21, 329. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Zhao, P.; Wang, H.; Wang, S.; Wei, C.; Gao, F.; Liu, H. Factors associated with frailty in kidney transplant recipients: A cross-sectional study. J. Ren. Care 2021. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; van Hout, H.P.; van der Horst, H.E.; Frijters, D.H.; Dent, E.; Deeg, D.J.; Huisman, M. Do psychosocial resources modify the effects of frailty on functional decline and mortality? J. Psychosom. Res. 2014, 77, 547–551. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Maruthappu, M.; Sood, H.S.; Keogh, B. The NHS Five Year Forward View: Transforming care. Br. J. Gen. Pract. 2014, 64, 635. [Google Scholar] [CrossRef] [Green Version]
- Soobiah, C.; Cooper, M.; Kishimoto, V.; Bhatia, R.; Scott, T.; Maloney, S.; Larsen, D.; Wijeysundera, H.; Zelmer, J.; Steele Gray, C.; et al. Identifying optimal frameworks to implement or evaluate digital health interventions: A scoping review protocol. BMJ Open 2020, 10, e037643. [Google Scholar] [CrossRef]
- WHO. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/publications/i/item/9789241550505 (accessed on 16 May 2022).
- Linn, N.; Goetzinger, C.; Regnaux, J.-P.; Schmitz, S.; Dessenne, C.; Fagherazzi, G.; Aguayo, G.A. Digital Health Interventions among People Living with Frailty: A Scoping Review. J. Am. Med. Dir. Assoc. 2021, 22, 1802–1812. [Google Scholar] [CrossRef]
- Romeo, A.; Edney, S.; Plotnikoff, R.; Curtis, R.; Ryan, J.; Sanders, I.; Crozier, A.; Maher, C. Can Smartphone Apps Increase Physical Activity? Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e12053. [Google Scholar] [CrossRef] [PubMed]
- Brickwood, K.-J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-Based Wearable Activity Trackers Increase Physical Activity Participation: Systematic Review and Meta-Analysis. JMIR mHealth uHealth 2019, 7, e11819. [Google Scholar] [CrossRef] [PubMed]
- Lobelo, F.; Kelli, H.M.; Tejedor, S.C.; Pratt, M.; McConnell, M.V.; Martin, S.S.; Welk, G.J. The Wild Wild West: A Framework to Integrate mHealth Software Applications and Wearables to Support Physical Activity Assessment, Counseling and Interventions for Cardiovascular Disease Risk Reduction. Prog. Cardiovasc. Dis. 2016, 58, 584–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muellmann, S.; Forberger, S.; Möllers, T.; Bröring, E.; Zeeb, H.; Pischke, C.R. Effectiveness of eHealth interventions for the promotion of physical activity in older adults: A systematic review. Prev. Med. 2018, 108, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Yerrakalva, D.; Yerrakalva, D.; Hajna, S.; Griffin, S. Effects of Mobile Health App Interventions on Sedentary Time, Physical Activity, and Fitness in Older Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e14343. [Google Scholar] [CrossRef]
- McGarrigle, L.; Boulton, E.; Todd, C. Map the apps: A rapid review of digital approaches to support the engagement of older adults in strength and balance exercises. BMC Geriatr. 2020, 20, 483. [Google Scholar] [CrossRef]
- Antoun, J.; Brown, D.J.; Jones, D.J.W.; Sangala, N.C.; Lewis, R.J.; Shepherd, A.I.; McNarry, M.A.; Mackintosh, K.A.; Mason, L.; Corbett, J.; et al. Understanding the Impact of Initial COVID-19 Restrictions on Physical Activity, Wellbeing and Quality of Life in Shielding Adults with End-Stage Renal Disease in the United Kingdom Dialysing at Home versus In-Centre and Their Experiences with Telemedicine. Int. J. Environ. Res. Public Health 2021, 18, 3144. [Google Scholar] [CrossRef]
- Kidney Beam. Available online: https://beamfeelgood.com/kidney%20disease2020 (accessed on 19 January 2022).
- Mayes, J.; Billany, R.E.; Vadaszy, N.; Young, H.M.L.; Castle, E.M.; Bishop, N.C.; Bramham, K.; Nixon, A.C.; Wilkinson, T.J.; Hamilton, A.; et al. The rapid development of a novel kidney-specific digital intervention for self-management of physical activity and emotional wellbeing during the COVID-19 pandemic and beyond: Kidney Beam. Clin. Kidney J. 2021, 15, 571–573. [Google Scholar] [CrossRef]
- Weber, M.B.; Ziolkowski, S.; Bootwala, A.; Bienvenida, A.; Anand, S.; Lobelo, F. Perceptions of physical activity and technology enabled exercise interventions among people with advanced chronic kidney disease: A qualitative study. BMC Nephrol. 2021, 22, 373. [Google Scholar] [CrossRef]
- Rampersad, C.; Darcel, J.; Harasemiw, O.; Brar, R.S.; Komenda, P.; Rigatto, C.; Prasad, B.; Bohm, C.; Tangri, N. Change in Physical Activity and Function in Patients with Baseline Advanced Nondialysis CKD. Clin. J. Am. Soc. Nephrol. 2021, 16, 1805. [Google Scholar] [CrossRef]
- Gobeil-Lavoie, A.P.; Chouinard, M.C.; Danish, A.; Hudon, C. Characteristics of self-management among patients with complex health needs: A thematic analysis review. BMJ Open 2019, 9, e028344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, e323. [Google Scholar] [CrossRef]
- Lindsay, S. The influence of childhood poverty on the self-management of heart disease in later life. Res. Sociol. Health Care 2009, 27, 161–183. [Google Scholar] [CrossRef]
- Anand, S.; Johansen, K.L.; Kurella Tamura, M. Aging and chronic kidney disease: The impact on physical function and cognition. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Mallappallil, M.; Friedman, E.A.; Delano, B.G.; McFarlane, S.I.; Salifu, M.O. Chronic kidney disease in the elderly: Evaluation and management. Clin. Pract. 2014, 11, 525–535. [Google Scholar] [CrossRef] [Green Version]
- Beetham, K.S.; Krishnasamy, R.; Stanton, T.; Sacre, J.W.; Douglas, B.; Isbel, N.M.; Coombes, J.S.; Howden, E.J. Effect of a 3-Year Lifestyle Intervention in Patients with Chronic Kidney Disease: A Randomized Clinical Trial. J. Am. Soc. Nephrol. 2022, 33, 431. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author and Country | Study Type | Sample Size | Population | Frailty Measure(s) Used | Aims | Intervention | Results |
|---|---|---|---|---|---|---|---|
| Suzuki et al., 2019 Japan | RCT protocol | 20 | Maintenance haemodialysis. Aged 65 years or more. SPPB Score 4–9 | Short Physical Performance Battery (SPPB) | To evaluate whether electrical muscle stimulation (EMS) during dialysis may be beneficial to reduce physical function impairment in frail elderly haemodialysis patients. | EMS performed on each leg using belt electrode skeletal muscle electrical stimulation. | To be determined—this is a protocol paper. |
| Nixon et al., 2021 United Kingdom | Pilot RCT | 35 | Age >65 years old CKD G3b-5 (not receiving dialysis or received a kidney transplant); Clinical Frailty Scale score > 4 | Clinical Frailty Scale | To inform the design of a definitive RCT that evaluates the effectiveness of a home-based exercise intervention in pre-frail and frail older adults with CKD. | Multi-component Home Based Exercise Intervention | Feasibility Outcomes:
|
| Wytsma-fisher et al., 2021 Canada | Pilot RCT Protocol | 24–36 | Maintenance dialysis Current inpatients with discharge date > 7 days | Frailty Phenotype | To assess the feasibility and preliminary efficacy of an early physical activity intervention in the care of kidney failure inpatients. | Early physical activity/mobility intervention | To be determined—this is a protocol paper. |
| Perez-Saez et al., 2021 Spain | RCT Protocol | 38 frail and 76 non-frail participants | Waitlist for deceased donor kidney transplant (KT). | Frailty Phenotype | To study the potential effects of multi-modal prehabilitation as a prognostic variable to predict the 90-day primary endpoint based on clinical and functional outcomes achieved in frail and non-frail KT candidates. | Multi-modal exercise intervention with nutritional supplementation. | To be determined—this is a protocol paper. |
| Anderson et al., 2018 United Kingdom | Pilot RCT | 50 | Haemodialysis | Frailty Phenotype | To explore a multi-disciplinary clinical intervention to improve frailty status among patients receiving haemodialysis | Dietetic advice Cognitive Behavioural Therapy Goal Setting | To be determined—this is a protocol paper. |
| Young et al., 2020 United Kingdom | Feasibility RCT | 64 | Haemodialysis | Clinical Frailty Scale | To determine the feasibility of conducting a randomised controlled trial (RCT) investigating the effects of Intra- Dialytic Cycling (IDC) for HD patients living with frailty. | Intra-dialytic cycling |
|
| Chang et al., 2020 China | RCT Protocol | 242 | CKD stage 3–5 without dialysis Aged > 65 years | Frailty Phenotype | To explore the risk factors related to frailty in elderly CKD patients without dialysis. To investigate the effect of individualised interventions of frailty on the prognosis of elderly patients with CKD who did not undergo dialysis. | Nutrition, psychology, and exercise intervention. | To be determined—this is a protocol paper. |
| Areas of Focus | Practical Applications |
|---|---|
| Frailty identification and assessment |
|
| Self-management support |
|
| Exercise/physical activity |
|
| Nutrition |
|
| Psychological management |
|
| Digital health interventions (DHIs) |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayes, J.; Young, H.M.L.; Blacklock, R.M.; Lightfoot, C.J.; Chilcot, J.; Nixon, A.C. Targeted Non-Pharmacological Interventions for People Living with Frailty and Chronic Kidney Disease. Kidney Dial. 2022, 2, 245-261. https://0-doi-org.brum.beds.ac.uk/10.3390/kidneydial2020025
Mayes J, Young HML, Blacklock RM, Lightfoot CJ, Chilcot J, Nixon AC. Targeted Non-Pharmacological Interventions for People Living with Frailty and Chronic Kidney Disease. Kidney and Dialysis. 2022; 2(2):245-261. https://0-doi-org.brum.beds.ac.uk/10.3390/kidneydial2020025
Chicago/Turabian StyleMayes, Juliet, Hannah M. L. Young, Rochelle M. Blacklock, Courtney J. Lightfoot, Joseph Chilcot, and Andrew C. Nixon. 2022. "Targeted Non-Pharmacological Interventions for People Living with Frailty and Chronic Kidney Disease" Kidney and Dialysis 2, no. 2: 245-261. https://0-doi-org.brum.beds.ac.uk/10.3390/kidneydial2020025