
Painful Legs and Moving Toes


1
Department of Neurology, Charité University Hospital (CBS), Hindenburgdamm 30, 12203 Berlin, Germany
2
Outpatient Clinic for Neurology, Manfred-von-Richthofen-Straße 15, 12101 Berlin, Germany
3
Neurology and Psychosomatics at Wittenbergplatz, Outpatient-Clinic, Ansbacher Straße 17-19, 10787 Berlin, Germany
Encyclopedia 2022, 2(1), 325-335; https://doi.org/10.3390/encyclopedia2010020
Submission received: 19 December 2021
/
Revised: 24 January 2022
/
Accepted: 27 January 2022
/
Published: 28 January 2022
(This article belongs to the Section Medicine & Pharmacology)
Definition
:Painful Legs and Moving Toes syndrome (PLMT) is a rare neurological movement disorder characterized by involuntary and irregular movements of one or more toes, often together, with moderate to severe diffuse pain at the foot and leg. It can appear on one or both sides and in the upper limbs as well as lower limbs. The etiology of PLMT is still unclear; therefore, the main symptoms of PLMT, including pain in limbs as well as involuntary movements of toes, can be treated only symptomatically, and the outcomes are often unsatisfactory. Central or peripheral nerve injuries have been assumed to be the possible causes of irregular involuntary movements, often accompanied by chronic pain; however, its etiology is unknown in most cases. The management of PLMT is very difficult because of its rare prevalence and obscure pathogenesis, and there have been no clear guidelines for the treatment of PLMT. Oral medications (e.g., GABAergic agents, benzodiazepines, antiepileptics, antidepressants, atypical antipsychotics, beta-blockers, corticosteroids, cannabis, calcitonin, and analgesics) and several therapeutic interventions (e.g., local botulinum neurotoxin-A injection, spinal cord stimulation, anesthetic, and surgical interventions) have been recommended, based on individual experiences from several cases. Its etiology, pathogenesis, and effective treatments should be further discussed.
Keywords:
painful legs; moving toes; PLMT; pain; movement disorder; involuntary; botulinum; pregabalin; spinal stimulation1. History
Painful Legs and Moving Toes syndrome (PLMT), one of the spinal-generated movement disorders [1], is a rare movement disorder with involuntary irregular flexion/extension of one or more toes, which is often accompanied with pain felt deeply in the foot and leg. It therefore reduces the quality of life as well as activities in social community and the workplace [2,3]. PLMT was firstly reported as a pain syndrome in the feet or lower limbs with spontaneous movements of the toes by Spillane and colleagues in 1971 [2]; since then, PLMT has been described in case or cases series reports rarely [4,5,6,7,8,9,10,11,12,13]. Until now, about 130 cases with PLMT have been reported, according to our literature search on PubMed and other public open-access databases (screening on 31 October 2021) and patients’ ages ranged from 11 to 86 [13,14,15]. The definition of PLMT has expanded to the upper limbs (painful hands and moving fingers) [7,8,11,12,16]. It has been also called “painful limbs and moving extremities” involving more than toes or fingers, e.g., feet or hands and limbs [8,12,17]. The affected locations have extended from toes or fingers proximally to ipsilateral foot or hands and limbs, as well as contralateral limbs in some cases, and possibly from the lower limb to the upper [16]. Several atypical cases with painful movement disorder have been reported [9,10,18,19,20,21]. One case with PLMT extended to the tongue, called “painful moving tongue”, but detailed information was not available [22].
2. Etiology of PLMT
Until now, the etiology and pathogenesis of PLMT has been poorly known; however, it could come from neuropathic changes or traumatic injuries in the peripheral nervous system [3,6,10,11,13]. Sometimes, it is accompanied by injuries/lesions in the central nervous system [11,12,23,24,25]. (See Table 1.)
Its possible causes have been discussed in case/case series reports, including neuropathological conditions in peripheral and/or central nerves, e.g., post traumatic peripheral nerve injury [8,10,11,16,26,27], focal nerve injury (e.g., tarsal tunnel syndrome [27,28,29], polyneuropathy (large fiber and/or small fiber) [3,13,29,30,31,32,33, restless leg syndrome (RLS) [3,13], or injuries of the spinal cord [10,21,25], cauda equina [3,15,34,35], lumbar nerve root [3,5,6,17,23,30,35,36,37], or sympathetic nerve [2,6,7,10,38,39,40], as well as postoperative complications [34,36,41] and post traumatic injuries (e.g., bone [5,6,13,15] and conjunctive tissue of foot [5,6,10,13,15,23]). Additionally, stroke, Parkinson, Wilson’s disease, and Hashimoto’s encephalopathy were diagnosed long before PLMT in a few cases, in whom any possible cause was not found [15,23]. In one case Hashimoto’s encephalopathy [23], which was diagnosed over 30 years prior to the beginning of PLMT was assumed as a possible condition, with several small subcortical white matter fronto-parietal lesions on the brain MRI [23]. In several cases, increased protein concentration in cerebrospinal fluid (CSF) has been reported [42]. In other cases with stroke, Wilson’s disease, and Parkinson, their associations with the development of PLMT were not clear; however, no other pathologic conditions were found in these cases.
In a few cases, viral infection, such as human immunodeficiency virus [32] or herpetic virus [5,10,25], were found. The virus infection induced neuropathic changes in the peripheral as well as central nervous system where they invaded.
With the relief of or decrease in clinical symptoms after sympathetic ganglion block in some cases [2,4,6,10,25,31,39,41,43,44], it was assumed that that pathologically induced impulses from afferent fibers of an injured nerve into the sympathetic nervous system abnormally activated neurons in the anterior horn of spinal cord, resulting in involuntary movements of toes. The effectiveness of the sympathetic block varied, with mostly transient reductions in symptoms, and in just in a few cases, symptoms disappeared [2,10,41,44]. Two cases were reported, who had sympathectomy for the management of PLMT; however, it was not effective [2,17]. Later, two cases were additionally reported, which showed an improvement in symptoms, especially pain, after sympathectomy; so, the role of the sympathetic system was supported in the pathogenesis associated with pain development [45]. They concluded that sympathetic neuronal signals could provoke pain by activating “an impulse generator” (injured location) in the affected limbs.
Generally, the pain pathway consists of activating nociceptors or converting to neural signals or stimuli directly at the nerve injury site (transduction), transferring from peripheral neurons to central neurons in the dorsal horn of the spinal cord, brain stem, and thalamus (conduction and transmission), inhibition in the spinal cord and activation of descending inhibitory tracts (modulation), and projection to the somatosensory cortex, enabling the perception of pain (perception). [46] Interneurons may partially pass the transmitted abnormal neural signals to segmental or multisegmental efferent motor pathways in the spinal cord, which may reproduce abnormally involuntary movements. [2,3,5,6,15,40] (See Figure 1.)
Nerve plexus injury, radiculopathy, polyneuropathy (large fiber and/or small fiber), and posttraumatic peripheral nerve injuries were more common in cases, even though their exact participation in developing PLMT are not clear [13,15]. Nociplastic/ neuroplastic pain can join in the pathogenesis of chronic pain over time, by central pain modulating disturbances, e.g., increased excitability of ascending and descending facilitatory tracts, reduced inhibition of descending anti-nociceptive tracts, and psychogenic conditions due to the “learning and thinking pain” of the brain are also important in chronic pain management, so called as “psychogenic pain” [46]
PLMT could mostly begin with peripheral causes and be associated later with subsequent changes in CNS [6]. Frequent ectopic impulses to the posterior root, which are spontaneously produced at the injured peripheral nerve could lead to pain and involuntary movements via the abnormal re-networking of local spinal circuits [5,6,15,40]. This might be occasionally influenced by accompanied central diseases [12,23,41,47].
In several cases, central lesions, e.g., stroke [11], morbus Parkinson [41], encephalopathy [23], spinal cord injury [21,25], cervical myelitis [24] and Morbus Wilson [12] were identified and assumed to be associated with the development of PLMT, but the association with its development and these diseases was unclear. Involuntary movements did not appear or were reduced during sleep in some cases, which could be associated with the inhibition of the reticular activating system [6]. PLMT rarely appeared after long-term use of neuroleptics (perphenazine and ziprasidone) [9,48]. However, it remains unclear, how and to what extent a lesion or degenerative changes in the brain or spinal cord could contribute to the pathogenesis of PLMT.
In one recent report including eight cases with clinically identified PLMT [49], the brain single photon emission computed tomography (SPECT) showed the hypoperfusion to the frontal and occipital cortices, thalamus, and cerebellum, as well as hyperperfusion to the anterior cingulate gyrus and parietal cortices (primary and secondary sensory cortices) on both sides, which are related to pain, as compared to 34 controls [49].
The deficit of adenosine in blood might be also associated with the development of PLMT in individual cases. One case report showed the deficiency in circulating adenosine levels in patients with PLMT, compared with other chronic painful syndromes, e.g., sciatic pain [26].
In women, PLMT appeared more frequently than in men [13], and the influence of female hormone concentration on the symptoms of PLMT was reported in one case. In this case, leg pain and involuntary movements of toes nearly disappeared in the first as well as second pregnancy. These symptoms were worse during the menstrual cycle and when taking progesterone [50].
3. Diagnostics of PLMT
3.1. Medical History of Possible Pathological Conditions of PLMT
Although the etiology of PLMT is still unclear, there are possible pathological conditions, which were reported in many case/case series reports. (See Table 1) Therefore, a summary of the medical history including trauma history, pre-existing diseases, accompanied neurological diseases, or other chronic diseases, which influence the development of a neuropathologic condition, e.g., diabetes mellitus, Hashimoto’s diseases, virus infection, and post-operative conditions, is the first important step of the diagnosis and effective management of PLMT [3,14,15].
3.2. Clinical and Neurophysiological Diagnostics
As described in the clinical definition of PLMT, its main symptoms are involuntary and irregular movements of one or more toes/fingers and moderate to severe diffuse pain in the affected limbs [13,14,15].
Pain often appeared first; later, involuntary movements appeared, and pain mainly caused the reduced quality of life as well as limited activities at work and in social community, so that the treatment of PLMT has been often focused on pain [2,3,49]. Moderate to severe pain has been reported in most cases, felt deeply in the leg/arm. Pain in PLMT was assumed to be associated with neuropathic pain [51]. Pain was often characterized as bursting, tearing, tingling, numbness, cramp-like, aching, electric sensation, pulling, etc. The diverse descriptions of pain may be related to different conditions, which were considered as possible causes [3,34].
Later, several painless cases were reported, and most of them required the treatment of involuntary movements only when related to a cosmetic problem [9,10,18,19,20,21].
The involuntary movements are flexion and extension and/or side-to-side movements (adduction/abduction) of one or more toes/fingers on one or both sides [2,3,6,10,15,34,52]. Those movements were dystonic, myoclonic, or occasionally rhythmic [34]. Involuntary irregular movements began at one toe or finger and, later, could spread to more toes or fingers [5]. In some cases, the affected locations were further extended later, e.g., proximally to the foot or hand and limb or (from affected toes) to the ipsilateral hand as well as to the contralateral limb [5,16]. Toe movements were worsened by the aggravation of pain [15] and intensified often at rest and at night [3]. The involuntary movements disappeared during sleep, which might possibly be associated with the inhibition of the brainstem reticular system [6].
3.3. Neurophysiological Examination
Electroneurography (ENG) and Electromyography (EMG) are used to examine possible conditions of PLMT, e.g., peripheral nerve injuries and radiculopathy [15,47].
PLMT is not a homogenous disease, so the detailed characters of bursts in EMG varied diversely [28,40]. Two main patterns of bursts in the EMG were found [53]:
- -
- the first type with short duration (10–80 ms) and a higher frequency of 4–6 Hz
- -
- the second type with longer duration (160–500 ms) and lower frequency of 1.5–3 Hz.
Later, lower frequency of bursts of 0.5–1 Hz with irregular duration (50 ms to 1 s) were also reported [15,48].
The findings of the Electroencephalography (EEG) were mostly normal. Polysomnography can show the disturbance of the sleep pattern, e.g., predominance in light sleep, in rapid eye movement, and reduction in slow wave sleep (SWS) and decreased total sleep time with frequent awakening [12,13,30]. During SWS, involuntary movements disappeared or rarely appeared, with only a few isolated jerks sporadically [2,30].
3.4. Differential Diagnoses
The clinical symptoms including pain and involuntary movements have been mainly used to diagnose PLMT. Therefore, PLMT should be differentiated from other neurologic diseases with involuntary movements and/or chronic pain in clinical practice.
- -
- Restless leg syndrome with pain and movement of feet and legs;
- -
- Painful radiculopathy or plexopathy;
- -
- Complex regional pain syndrome;
- -
- Akathisia with leg movements;
- -
- Cramps with unilateral involuntary muscle hardening, usually calf muscle;
- -
- Spinal segmental myoclonus with leg movement;
- -
- EPC with continuous toes/foot or leg movement;
- -
- Focal or polyneuropathy with feet numbness, tingling, and/or pain;
- -
- Dystonia with sustained involuntary movements of feet and legs;
- -
- Periodic-limb-movement disorder (PLMD);
- -
- Parkinson with tremor;
- -
- Chorea;
- -
- Pseudoathetosis;
- -
- Epilepsia partialis continua with toes/foot movements; and
- -
- Psychogenic movement disorder.
4. Management of PLMT
Until now, there have been no guidelines for the management of PLMT, due to the poor understanding of its etiology and pathogenesis as well as the lack of effective therapy against pain and/or involuntary irregular movements of toes [3,15]. It is a rare syndrome, managed only symptomatically, and the outcomes of different treatments were often unsatisfactory [10,12].
There are several symptomatic treatments including pharmacological as well as non-pharmacological therapies, which were reported to be effective for PLMT in individual cases (See Table 2). These therapies focused mostly on pain, because pain was the dominant symptom in most cases with PLMT [3,10,15,48].
4.1. Pharmacological Therapy
4.1.1. Oral Medication
Oral medications, the first line of PLMT treatment, included GABA (Gamma-AminoButyric Acid) ergic agents, benzodiazepines, antiepileptic agents, antidepressants, atypical antipsychotic agent, beta-blockers, corticosteroids, cannabis, calcitonin, and analgesics, which could be used as monotherapy or in combination. The effects of oral medications were often disappointing and mostly a temporary relief [1,3,13,15,33,40,62].
Pregabalin [3,48] and gabapentin [34,48,63,64,65], GABAergic agents, were reported as one of the favorable medications to improve PLMT-related pain, involuntary movements, and quality of life, including sleep disorders in some cases [63,64,65]. GABAergic agents also successfully improved the symptoms of PLMT in combination with baclofen or clonazepam [34].
However, their effects were often transient, [10,64] and in many cases, they were not effective in pain reduction and/or involuntary movements [10,20,66,67]. The long-term use of oral medications could lead to the downregulation of GABA receptors, and their side effects, e.g., worsening leg edema, led to reduced doses, even though not effective enough, or discontinuation in several cases [3].
Other suggested oral medications, e.g., baclofen [30,62], progabide (gamma-aminobutyric acid agonist) [68], amitriptyline [6,62], carbamazepine [30,37,64,69], clonazepam and other benzodiazepines [6,47,49,57,62], calcitonin (for PAMF) [11], quetiapine [33,48], propranolol [27], corticoids [6,23], and analgesics [6] also showed individually transient improvement of symptoms but, often, no satisfactory outcomes. These can be recommended as a monotherapy as well as in combination, depending on the assumed pathogens of PLMT.
The infusion of Adenosine triphosphate (ATP) was used and effective in two cases with traumatic peripheral nerve injuries, who had a deficiency of blood adenosine [26]; however, there has been no other report on ATP therapy.
Milacemide, the glycine precursor, was orally introduced to improve the symptoms of PLMT but showed no effect [70].
4.1.2. Interventions
Botulinum Neurotoxin
It has been known that Botulinum neurotoxin A (BoNT-A), a nerve blocker at the neuromuscular conjunction is also effective in the reduction in pain via blocking exocytosis of various inflammation-mediators, e.g., substance P, glutamate, calcitonin gene-related peptide, and blocking neurotransmission arising from sensory nerves in the peripheral nerve system [71,72,73,74]. Local injections of BoNT-A reduced neuropathic pain as well as muscle overactivity-associated pain, e.g., spastic, dystonic, or spasm-related pain [71,75].
Local intramuscular injections of BoNT-A have been strongly recommended as a monotherapy as well as in combination with other treatments in the cases with PLMT, in whom symptomatic treatments with oral medications or other therapeutic interventions failed or had insufficient effects [19,66,69,76].
In the management of PLMT, BoNT-A therapy focused on reducing involuntary movements [19,66,69,76,77] but also partially induced relief or reduction in pain [66,69,76,77,78]. However, in one case there was no improvement in pain intensity [19].
The effect duration of BoNT-A therapy is commonly 10–12 weeks, sometimes shorter as well as longer [71,79]. Local injection of BoNT-A is strongly recommended as a safe and effective symptomatic treatment in the management of moderate to severe symptoms of PLMT [13,15,78].
Epidural Block
A total of six cases with PLMT were treated by epidural block with local anesthetics. Four cases showed a temporary improvement of pain and involuntary movements with different effect times (transient, 3 h, 6 h, and longer) [25,39,41,43] Epidural block can be recommended in PLMT with severe pain.
Lumbar sympathetic blockade
In some cases, the block of sympathetic nerve system showed a reduction in pain intensity and involuntary movements, although its effect was mostly transient [2,4,6,10,31,38,39,41,43,44].
Only one of four cases showed the disappearance of both main symptoms after sympathetic block by Spillane, and three cases had mild transient improvement [2]. Of the other 18 cases, only in four cases was the blocking of the sympathetic nerve system effective with the disappearance of symptoms [10,31,41]. Dressler and his colleagues [10] reported that only one case had good effects after the blocking of the sympathetic nerve system among four cases with traumatic peripheral nerve injuries as a possible cause of PLMT; two cases showed no effect.
Although lumbar sympathetic blockade was reported as an effective treatment in individual cases [31,41,44], the duration of relief by this intervention was not specified and mostly transient. Sympathetic blockade can be more recommended as a preoperative test after sympathectomy to evaluate the effect of surgical intervention.
4.2. Nonpharmacological Therapeutic Interventions
Epidural spinal cord stimulation
Epidural spinal cord stimulation (ESCS) has been applied in other pain conditions, such as complex regional pain syndrome, peripheral vascular diseases, and back pain, and has been used in the management of pain symptom in a few cases with PLMT [43,51,80].
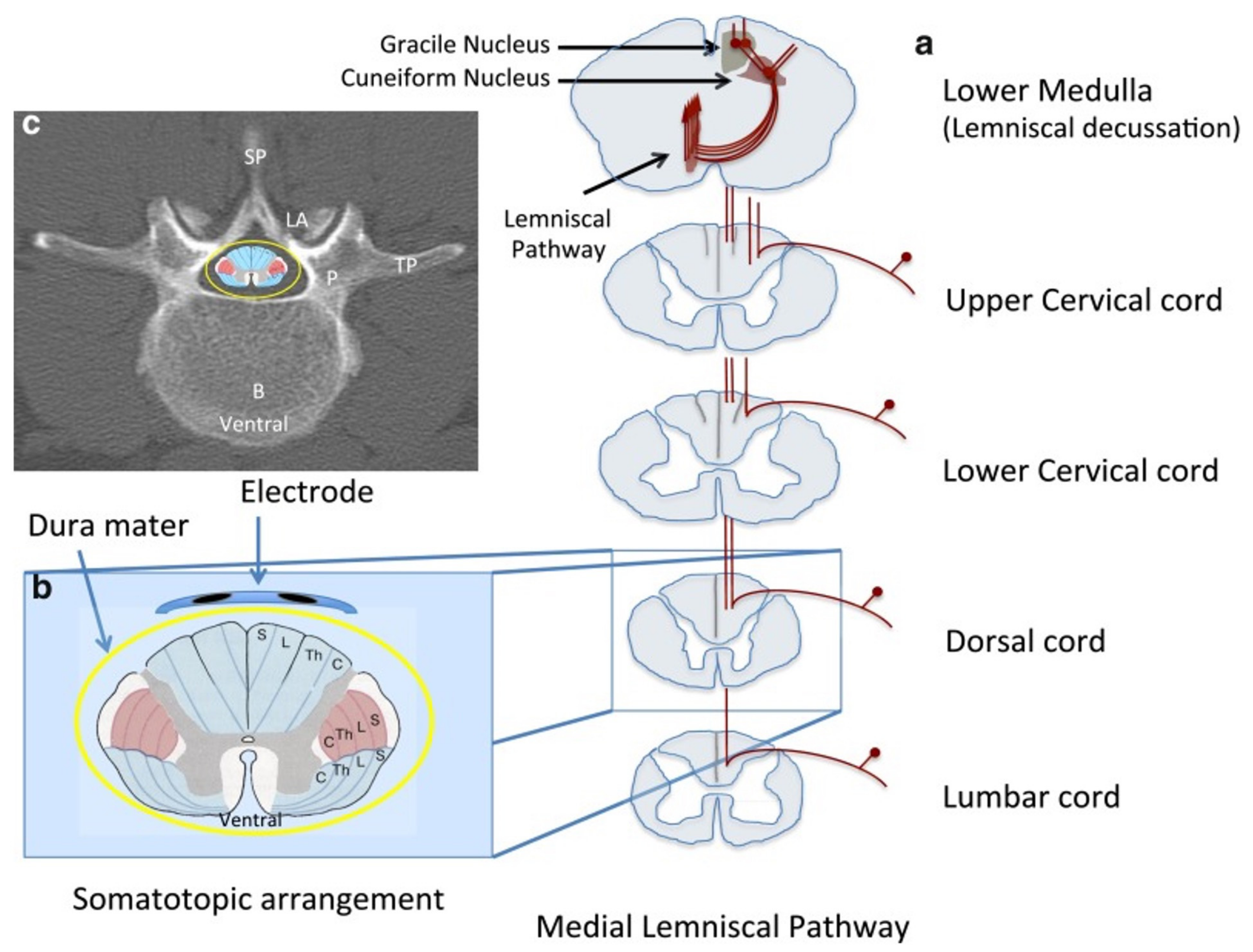
Long-term epidural spinal cord stimulation with a implanted permanent device (ITREL, Medtronic Inc, Minneapolis, MN, USA), placed at the dorsal aspect of the Th10–11 levels (See Figure 2) was applied for 20 min twice per day over six months (one case for six months and another case for 13 months), to improve pain and involuntary movements of PLMT [43,80] and had a beneficial effect with a significant reduction in pain and nearly complete resolution of the toe movements [43,80]. However, another case with PLMT, possibly due to herpes zoster myelitis, showed no effect with ESCS [25], and it could be assumed that the individually different effects of this intervention were due to the diverse pathogenesis of PLMT. Further studies are necessary to collect more data for this therapy.
General physical therapies
Different physical treatments such as transcutaneous electrical nerve stimulation (TENS), local vibration, local heat or cold therapy, and tactile stimulation can be applied to reduce pain symptoms [13,15,43,47,81].
Transcutaneous electrical nerve stimulation showed a temporary reduction in pain in individual cases and can be also used in combination with vibratory stimulation to increase its effect [43,47]. In one case the combination of TENS and vibratory stimulation showed a significant improvement of pain and movements [47]. This effect was assumed by the pain-modulating of vibration [26]. Local cold, heat, or tactile stimulation were considered as an additional therapy [13,15].
In two cases with painful arm/hand and moving fingers, the symptoms were improved temporarily after tactile stimulation [81].
4.3. Other Surgical Treatments
Surgical interventions have been strongly recommended to remove possible conditions of PLMT such as nerve root compression or local lesions at limbs, as well as in the spinal canal, when the symptoms were therapy-resistant [11,15,28,40]. Additionally, sympathectomy has also been considered in individual cases, due to the possible contribution of the sympathetic nerve system in the pathogenesis of PLMT [2,17,45].
Sympathetomy
A few cases received sympathectomy after failed treatments such as oral medication, physical therapies, and other nonsurgical interventions [2,17,45]. Two cases showed good effects with significant decreased pain intensity and reduced involuntary movements [45]. However, other two other cases showed no change in symptoms after sympathectomy [2,17].
Surgical decompression
When nerve root compression existed, surgical decompression has been strongly recommended, because radiculopathy has been possibly associated with the development of PLMT. Most of these cases with nerve compression showed an improvement of symptoms, including the disappearance of or reduction in pain and involuntary movements after surgical decompression [17,21,28,36,40].
Surgical decompression is strongly recommended in cases of PLMT with the compression of the lumbar nerve root.
5. Conclusions and Prospects
The etiology and pathogenesis of Painful Leg and Moving Toes syndrome (PLMT) is still unclear; however, traumatic or neuropathic peripheral nerve injuries, as well as radiculopathy, are common, and central factors can be later joined additionally. Individually introduced oral medications (monotherapy as well as in combination) are the first line of PLMT management, and physical therapies, e.g., TENS, local vibration can be adjunct. Several therapeutic interventions, e.g., BoNT-A injections, spinal blockade, and epidural spinal cord stimulation are also recommended due to the significant effects including pain relief/reduction and the improvement of involuntary movements in individual cases, although further discussion with more cases are necessary. Surgical decompressions are strongly recommended when a case has the compression of a nerve root or spinal cord as a possible condition of PLMT. Sympathectomy can be considered after a few pre-operative tests, e.g., the blockade of sympathetic nerve system.
Funding
This research received no external funding.
Acknowledgments
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
Entry Link on the Encyclopedia Platform
References
- Termsarasab, P.; Thammongkolchai, T.; Frucht, S.J. Spinal-generated movement disorders: A clinical review. J. Clin. Mov. Disord. 2015, 2, 18. [Google Scholar] [CrossRef] [PubMed]
- Spillane, J.D.; Nathan, P.W.; Kelly, R.E.; Marsden, C.D. Painful legs and moving toes. Brain 1971, 94, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.H.; Liu, W.; Geigel, E.; Castaneda, S.; Rossi, E.M.; Schnacky, K. Painful legs and moving toes syndrome responsive to pregabalin. J. Postgrad. Med. 2015, 61, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, S.; Takegami, T.; Mano, T. Peculiar involuntary movement of the toes associated with discomfort of the foot, a case of so-called “painful legs and moving toes”. Rinsho Shinkeigaku 1974, 14, 829–834. (In Japanese) [Google Scholar] [PubMed]
- Nathan, P.W. Painful legs and moving toes: Evidence on the site of the lesion. J. Neurol. Neurosurg. Psychiatry 1978, 41, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Schott, G.D. Painful legs and moving toes: The role of trauma. J. Neurol. Neurosurg. Psychiatry 1981, 44, 344–346. [Google Scholar] [CrossRef]
- Verhagen, W.I.; Horstink, M.W.; Notermans, S.L. Painful arm and moving fingers. J. Neurol. Neurosurg. Psychiatry 1985, 48, 384–385. [Google Scholar] [CrossRef]
- Funakawa, I.; Mano, Y.; Takayanagi, T. Painful hand and moving fingers. A case report. J. Neurol. 1987, 234, 342–343. [Google Scholar] [CrossRef]
- Walters, A.S.; Hening, W.A.; Shah, S.K.; Chokroverty, S. Painless legs and moving toes: A syndrome related to painful legs and moving toes? Mov. Disord. 1993, 8, 377–379. [Google Scholar] [CrossRef]
- Dressler, D.; Thompson, P.D.; Gledhill, R.F.; Marsden, C.D. The syndrome of painful legs and moving toes. Mov. Disord. 1994, 9, 13–21. [Google Scholar] [CrossRef]
- Supiot, F.; Gazagnes, M.D.; Blecic, S.A.; Zegers de Beyl, D. Painful arm and moving fingers: Clinical features of four new cases. Mov. Disord. 2002, 17, 616–618. [Google Scholar] [CrossRef] [PubMed]
- Papapetropoulos, S.; Singer, C. Painless legs moving toes in a patient with Wilson’s disease. Mov. Disord. 2006, 21, 579–580. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.; Mateen, F.J.; Coon, E.A.; Ahlskog, J.E. Painful legs and moving toes syndrome: A 76-patient case series. Arch. Neurol. 2012, 69, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.Y.; Xu, Y.; Gao, X.G. Spontaneous aching pain and peculiar involuntary movements: A case report of painful legs and moving toes and review of the literature. Case Rep. Med. 2014, 2014, 581402. [Google Scholar] [CrossRef] [PubMed]
- Reich, S.G. Painful legs and moving toes. Handb. Clin. Neurol. 2011, 100, 375–383. [Google Scholar] [CrossRef]
- Ebersbach, G.; Schelosky, L.; Schenkel, A.; Scholz, U.; Poewe, W. Unilateral painful legs and moving toes syndrome with moving fingers--evidence for distinct oscillators. Mov. Disord. 1998, 13, 965–968. [Google Scholar] [CrossRef]
- Mosek, A.; Rabey, J.M.; Kushnir, M.; Korczyn, A.D. Painful calf, moving foot. Mov. Disord. 1996, 11, 339–340. [Google Scholar] [CrossRef]
- Dziewas, R.; Kuhlenbäumer, G.; Okegwo, A.; Lüdemann, P. Painless legs and moving toes in a mother and her daughter. Mov. Disord. 2003, 18, 718–722. [Google Scholar] [CrossRef]
- Singer, C.; Papapetropoulos, S. A case of painless arms/moving fingers responsive to botulinum toxin a injections. Parkinsonism Relat. Disord. 2007, 13, 55–56. [Google Scholar] [CrossRef]
- Alrawashdeh, O. Painless legs and moving toes syndrome associated with a sacral Tarlov cyst: A case report. J. Med. Case Rep. 2016, 10, 52. [Google Scholar] [CrossRef]
- Bermejo, P.E.; Zabala, J.A. Painless legs and moving toes” syndrome due to spinal cord compression. Eur. Spine J. 2008, 17 (Suppl. S2), S294–S295. [Google Scholar] [CrossRef] [PubMed]
- Schwingenschuh, P.; Bhatia, K.P. Painful moving tongue in a patient with the painful legs moving toes syndrome. Mov. Disord. 2008, 23, 1324–1325. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, J.; Santos, L.; Bugalho, P. Painful legs and moving toes syndrome associated with Hashimoto’s disease. Eur. J. Neurol. 2007, 14, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Renard, D.; Taieb, G.; Castelnovo, G.; Labauge, P. Teaching Video NeuroImages: Painful legs, moving toes associated with partial transverse myelitis. Neurology 2010, 75, e74. [Google Scholar] [CrossRef]
- Ikeda, K.; Deguchi, K.; Touge, T.; Sasaki, I.; Tsukaguchi, M.; Shimamura, M.; Komatsu, E.; Takeuchi, H.; Kuriyama, S. Painful legs and moving toes syndrome associated with herpes zoster myelitis. J. Neurol. Sci. 2004, 219, 147–150. [Google Scholar] [CrossRef]
- Guieu, R.; Sampiéri, F.; Pouget, J.; Guy, B.; Rochat, H. Adenosine in painful legs and moving toes syndrome. Clin. Neuropharmacol. 1994, 17, 460–469. [Google Scholar] [CrossRef]
- Zinnuroglu, M.; Ozkayran, T. Painful legs and moving toes following a traumatic medial plantar nerve injury. Mov. Disord. 2010, 25, 133–135. [Google Scholar] [CrossRef]
- Mitsumoto, H.; Levin, K.H.; Wilbourn, A.J.; Chou, S.M. Hypertrophic mononeuritis clinically presenting with painful legs and moving toes. Muscle Nerve 1990, 13, 215–221. [Google Scholar] [CrossRef]
- Pla, M.E.; Dillingham, T.R.; Spellman, N.T.; Colon, E.; Jabbari, B. Painful legs and moving toes associates with tarsal tunnel syndrome and accessory soleus muscle. Mov. Disord. 1996, 11, 82–86. [Google Scholar] [CrossRef]
- Montagna, P.; Cirignotta, F.; Sacquegna, T.; Martinelli, P.; Ambrosetto, G.; Lugaresi, E. “Painful legs and moving toes” associated with polyneuropathy. J. Neurol. Neurosurg. Psychiatry 1983, 46, 399–403. [Google Scholar] [CrossRef]
- Touge, T.; Ishibashi, T.; Kamoda, M.; Tsukaguchi, M.; Takeuchi, H. Painful legs and moving toes” and muscle cramps spreading to the bilateral legs in a patient with alcoholic polyneuropathy. Rinsho Shinkeigaku 1998, 38, 762–766. (In Japanese) [Google Scholar] [PubMed]
- Pitágoras de Mattos, J.; Oliveira, M.; André, C. Painful legs and moving toes associated with neuropathy in HIV-infected patients. Mov. Disord. 1999, 14, 1053–1054. [Google Scholar] [CrossRef]
- Di Fabio, R.; Casali, C.; Pierelli, F. Quetiapine: An alternative treatment in painless legs and moving toes. Mov. Disord. 2008, 23, 1326–1328. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.; Soni, G. Painful leg and moving toes syndrome in secondary tethered cord syndrome. J. Spinal Cord Med. 2016, 39, 363–365. [Google Scholar] [CrossRef]
- Kwon, S.J.; Kim, J.M.; Jeon, B.S. A case report of painless moving toes syndrome. J. Clin. Neurol. 2008, 4, 33–35. [Google Scholar] [CrossRef]
- Wulff, C.H. Painful legs and moving toes. A report of 3 cases with neurophysiological studies. Acta Neurol. Scand. 1982, 66, 283–287. [Google Scholar] [CrossRef]
- El Otmani, H.; Moutaouakil, F.; Fadel, H.; Slassi, I. Syndrome de jambe douloureuse et orteils instables associé à une radiculopathie lombaire [Painful legs and moving toes syndrome associated with lumbar radiculopathy]. Rev. Neurol. 2009, 165, 980–983. [Google Scholar] [CrossRef]
- Sahashi, K.; Tsuchiya, I.; Iwase, S.; Ibi, T.; Mano, T. Clinical analyses on moving toes in “painful legs and moving toes”. Rinsho Shinkeigaku 1989, 29, 849–853. (In Japanese) [Google Scholar]
- Okuda, Y.; Suzuki, K.; Kitajima, T.; Masuda, R.; Asai, T. Lumbar epidural block for ‘painful legs and moving toes’ syndrome: A report of three cases. Pain 1998, 78, 145–147. [Google Scholar] [CrossRef]
- Miyakawa, T.; Yoshimoto, M.; Takebayashi, T.; Yamashita, T. Case reports: Painful limbs/moving extremities: Report of two cases. Clin. Orthop. Relat. Res. 2010, 468, 3419–3425. [Google Scholar] [CrossRef]
- Uchihara, T.; Ichikawa, T.; Furukawa, T.; Tsukagoshi, H. Myoclonus with burning sensation in legs that remits with sympathetic blockade. J. Neurol. Sci. 1990, 100, 161–164. [Google Scholar] [CrossRef]
- Seipelt, M.; Zerr, I.; Nau, R.; Mollenhauer, B.; Kropp, S.; Steinhoff, B.J.; Wilhelm-Gössling, C.; Bamberg, C.; Janzen, R.W.; Berlit, P.; et al. Hashimoto’s encephalitis as a differential diagnosis of Creutzfeldt-Jakob disease. J. Neurol. Neurosurg. Psychiatry 1999, 66, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Saitoh, C.; Iwata, O.; Nanbu, T.; Takada, S.; Morita, S. Epidural spinal cord stimulation for the treatment of painful legs and moving toes syndrome. Pain 2002, 96, 343–345. [Google Scholar] [CrossRef]
- Shime, N.; Sugimoto, E. Lumbar sympathetic ganglion block in a patient with painful legs and moving toes syndrome. Anesth. Analg. 1998, 86, 1056–1057. [Google Scholar] [CrossRef] [PubMed]
- Drummond, P.D.; Finch, P.M. Sympathetic nervous system involvement in the syndrome of painful legs and moving toes. Clin. J. Pain 2004, 20, 370–374. [Google Scholar] [CrossRef]
- Tanaka, M.; Török, N.; Tóth, F.; Szabó, Á.; Vécsei, L. Co-Players in Chronic Pain: Neuroinflammation and the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines 2021, 9, 897. [Google Scholar] [CrossRef]
- Guieu, R.; Tardy-Gervet, M.F.; Blin, O.; Pouget, J. Pain relief achieved by transcutaneous electrical nerve stimulation and/or vibratory stimulation in a case of painful legs and moving toes. Pain 1990, 42, 43–48. [Google Scholar] [CrossRef]
- Alvarez, M.V.; Driver-Dunckley, E.E.; Caviness, J.N.; Adler, C.H.; Evidente, V.G. Case series of painful legs and moving toes: Clinical and electrophysiologic observations. Mov. Disord. 2008, 23, 2062–2066. [Google Scholar] [CrossRef]
- Nishioka, K.; Suzuki, M.; Nakajima, M.; Hara, T.; Iseki, M.; Hattori, N. Painful legs and moving toes syndrome evaluated through brain single photon emission computed tomography: A case series. J. Neurol. 2019, 266, 717–725. [Google Scholar] [CrossRef]
- Diaz, N.L.; Hanspal, E.K.; Mazzoni, P. Painless legs and moving toes: Symptom reduction during pregnancy. Mov. Disord. 2012, 27, 328–329. [Google Scholar] [CrossRef]
- Thiriez, C.; Gurruchaga, J.M.; Goujon, C.; Fénelon, G.; Palfi, S. Spinal stimulation for movement disorders. Neurotherapeutics 2014, 11, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Sanders, P.; Waddy, H.M.; Thompson, P.D. An ‘annoying’ foot: Unilateral painful legs and moving toes syndrome. Pain 1999, 82, 103–104. [Google Scholar] [CrossRef]
- Schoenen, J.; Gonce, M.; Delwaide, P.J. Painful legs and moving toes: A syndrome with different physiopathologic mechanisms. Neurology 1984, 34, 1108–1112. [Google Scholar] [CrossRef] [PubMed]
- Lugaresi, E.; Cirignotta, F.; Coccagna, G.; Montagna, P. Nocturnal myoclonus and restless legs syndrome. Adv. Neurol. 1986, 43, 295–307. [Google Scholar] [PubMed]
- Jankovic, J.; Pardo, R. Segmental myoclonus. Clinical and pharmacologic study. Arch. Neurol. 1986, 43, 1025–1031. [Google Scholar] [CrossRef]
- Liu, R.; Moizuddin, M.; Hung, S. Painful legs and moving toes: Case report and review of literature. Br. J. Med. Pract. 2011, 4, a431. [Google Scholar]
- Tan, A.K.; Tan, C.B. The syndrome of painful legs and moving toes—A case report. Singap. Med. J. 1996, 37, 446–447. [Google Scholar]
- Gastaut, J.L. Jambes douloureuses et orteils instables. Un cas d’origine médicamenteuse [Painful legs and moving toes. A drug-induced case]. Rev. Neurol. 1986, 142, 641–642. (In French) [Google Scholar]
- Malapert, D.; Degos, J.D. Jambes douloureuses et orteils instables. Neuropathie induite par la cytarabine [Painful legs and moving toes. Neuropathy caused by cytarabine]. Rev. Neurol. 1989, 145, 869–871. (In French) [Google Scholar]
- Schwartzman, R.J.; Kerrigan, J. The movement disorder of reflex sympathetic dystrophy. Neurology 1990, 40, 57–61. [Google Scholar] [CrossRef]
- Bhatia, K.P.; Bhatt, M.H.; Marsden, C.D. The causalgia-dystonia syndrome. Brain 1993, 116, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Sandyk, R. Neuroleptic-induced “painful legs and moving toes” syndrome: Successful treatment with clonazepam and baclofen. Ital. J. Neurol. Sci. 1990, 11, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Villarejo, A.; Porta-Etessam, J.; Camacho, A.; De La Aleja, J.G.; Martínez-Salio, A.; Penas, M. Gabapentin for painful legs and moving toes syndrome. Eur. Neurol. 2004, 51, 180–181. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, H. Gabapentin for painful legs and moving toes syndrome. Intern. Med. 2007, 46, 1937. [Google Scholar] [CrossRef]
- Bhargava, P.; Pandav, V.; Peche, S. A pediatric case of painful legs and moving toes syndrome. Pediatr. Neurol. 2013, 49, 298–299. [Google Scholar] [CrossRef]
- Eisa, M.; Singer, C.; Sengun, C.; Russel, A.; Jabbari, B.; Papapetropoulos, S. Treatment of painful limbs/moving extremities with botulinum toxin type A injections. Eur. Neurol. 2008, 60, 104–106. [Google Scholar] [CrossRef]
- Peña, E.; Llanero, M. Painful legs and moving toes syndrome associated with a sacral Tarlov cyst. Parkinsonism Relat. Disord. 2011, 17, 645–646. [Google Scholar] [CrossRef]
- Bovier, P.; Hilleret, H.; Tissot, R. Traitement par le progabide d’un cas de syndrome des jambes douloureuses et orteils instables [Progabide treatment of a case of the syndrome of painful legs and moving toes]. Rev. Neurol. 1985, 141, 422–424. (In French) [Google Scholar]
- Azzi, J.; Atweh, S.; Saade, N.; Jabbour, R. Neuroleptics as a cause of painful legs and moving toes syndrome. BMJ Case Rep. 2014, 2014, bcr2014205117. [Google Scholar] [CrossRef]
- Gordon, M.F.; Diaz-Olivo, R.; Hunt, A.L.; Fahn, S. Therapeutic trial of milacemide in patients with myoclonus and other intractable movement disorders. Mov. Disord. 1993, 8, 484–488. [Google Scholar] [CrossRef]
- Ri, S.; Kivi, A.; Wissel, J. The Safety and Effect of Local Botulinumtoxin a Injections for Long-Term Management of Chronic Pain in Post-Herpetic Neuralgia: Literature Review and Cases Report Treated with Incobotulinumtoxin A. J. Pers. Med. 2021, 11, 758. [Google Scholar] [CrossRef] [PubMed]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Lucioni, A.; Bales, G.T.; Lotan, T.L.; McGehee, D.S.; Cook, S.P.; Rapp, D.E. Botulinum toxin type A inhibits sensory neuropeptide release in rat bladder models of acute injury and chronic inflammation. BJU Int. 2008, 101, 366–370. [Google Scholar] [CrossRef] [PubMed]
- McMahon, H.T.; Foran, P.; Dolly, J.O.; Verhage, M.; Wiegant, V.M.; Nicholls, D.G. Tetanus toxin and botulinum toxins type A and B inhibit glutamate, gamma-aminobutyric acid, aspartate, and met-enkephalin release from synaptosomes. Clues to the locus of action. J. Biol. Chem. 1992, 267, 21338–21343. [Google Scholar] [CrossRef]
- Wissel, J.; Ri, S. Assessment, goal setting, and botulinum neurotoxin a therapy in the management of post-stroke spastic movement disorder: Updated perspectives on best practice. Expert Rev. Neurother. 2021, 30, 1–16. [Google Scholar] [CrossRef]
- Rodriguez, R.L.; Fernandez, H.H. Sustained benefit of painful legs moving toes syndrome with botulinum toxin type A. J. Clin. Neurosci. 2013, 20, 1031–1032. [Google Scholar] [CrossRef]
- Argyriou, A.A.; Papapetropoulos, S. Botulinum toxin type A for painful limbs moving extremities. Mov. Disord. 2010, 25, 125. [Google Scholar] [CrossRef]
- Schoffer, K. Painful leg moving toes treated with botulinum toxin type A: A video report. Mov. Disord. 2010, 25, 784–785. [Google Scholar] [CrossRef]
- Kivi, A.; Ri, S.; Wissel, J. What clinicians and patients want: The past, the presence, and the future of the botulinum toxins. Toxicon 2020, 177, 46–51. [Google Scholar] [CrossRef]
- Raina, G.B.; Piedimonte, F.; Micheli, F. Posterior spinal cord stimulation in a case of painful legs and moving toes. Stereotact Funct. Neurosurg. 2007, 85, 307–309. [Google Scholar] [CrossRef]
- Wider, C.; Kuntzer, T.; Olivier, P.; Debatisse, D.; Nancoz, R.; Maeder, P.; Bogousslavsky, J.; Vingerhoets, F. Painful hand and moving finger treated by wearing a glove. Neurology 2006, 67, 491–493. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Theory of the interneuron role in the development of pain and involuntary movement of PLMT (reproduced from [40] under the © The Association of Bone and Joint Surgeons® 2010 license).
Figure 1.
Theory of the interneuron role in the development of pain and involuntary movement of PLMT (reproduced from [40] under the © The Association of Bone and Joint Surgeons® 2010 license).

Figure 2.
Medial lemniscal pathway and placing of epidural electrode. (a) lemniscal track at different levels of the spinal cord; (b) medial lemniscal track (in light blue, dorsal) and spinothalamic track (in light blue, ventral), lateral pyramidal track (in red). Epidural electrode along the dorsal aspect of the spinal cord; (c) Computed tomography of thoracic spine. S = sacral; L = lumbar; Th = thoracic; C = cervical; P = pedicle; TP = transverse process; LA = lamina, SP = spinous process; B = vertebral body. (reproduced from [50] under the © The American Society for Experimental NeuroTherapeutics, Inc. 2014).
Figure 2.
Medial lemniscal pathway and placing of epidural electrode. (a) lemniscal track at different levels of the spinal cord; (b) medial lemniscal track (in light blue, dorsal) and spinothalamic track (in light blue, ventral), lateral pyramidal track (in red). Epidural electrode along the dorsal aspect of the spinal cord; (c) Computed tomography of thoracic spine. S = sacral; L = lumbar; Th = thoracic; C = cervical; P = pedicle; TP = transverse process; LA = lamina, SP = spinous process; B = vertebral body. (reproduced from [50] under the © The American Society for Experimental NeuroTherapeutics, Inc. 2014).


{kind=link}
{kind=link}
Table 1.
Potential Conditions Associated with the Development of PLMT.
| Cauda equina trauma Radiculopathy Plexus injury Focal neuropathy (e.g., tarsal tunnel syndrome) Polyneuropathy (large fiber, small fiber) Herpes zoster myelitis Spinal cord compression Traumatic spinal cord injury Postsurgical complication Hashimoto’s Encephalopathy Morbus Wilson Morbus Parkinson Stroke Neuroleptics Endocrinologic condition, e.g., Hashimoto thyroiditis and Hypophysenadenome Local trauma without neurologic injury (at least not found) Dupuytren’s contracture |
Table 2.
Recommended Treatments.
| Oral medications, e.g., gabapentin, pregabalin, baclofen, clonazepam, carbamazepine, amitriptyline, citalopram, duloxetine, Levodopa, Tramadol, Fentanyl citrate, quetiapine, progabide, beta-blockers, corticosteroids, cannabis, calcitonin, adenosine, etc. Spinal cord stimulation Botulinum neurotoxin injection Local vibration Sympathetic blockade Epidural blockade Transcutaneous electrical nerve stimulation Massage Local cold, warm, or tactile stimulation Sympathectomy Surgical decompression Other surgical treatments according to possible causes of PLMT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ri, S. Painful Legs and Moving Toes. Encyclopedia 2022, 2, 325-335. https://0-doi-org.brum.beds.ac.uk/10.3390/encyclopedia2010020
AMA Style
Ri S. Painful Legs and Moving Toes. Encyclopedia. 2022; 2(1):325-335. https://0-doi-org.brum.beds.ac.uk/10.3390/encyclopedia2010020
Chicago/Turabian StyleRi, Songjin. 2022. "Painful Legs and Moving Toes" Encyclopedia 2, no. 1: 325-335. https://0-doi-org.brum.beds.ac.uk/10.3390/encyclopedia2010020