
Does the Current State of Evidence Justify the Broad Use of Cross-Links in Dorsal Instrumentation? A Systematic Review

 , , , ,
, , , ,
Abstract
:1. Introduction
- (1)
- Does the use of cross-links in dorsal instrumentation affects the radiological outcome, clinical outcome or rate of complication?
- (2)
- Are cross-links necessary in spinal fusion, if laminectomy is not performed?
- (3)
- Overall, does the current state of evidence justify the broad use of cross-links in spinal surgery? Alternatively, in which spinal disorders should cross-links be recommended?
2. Materials and Methods
2.1. Study Design
- (1)
- Cochrane library [Title Abstract Keyword]: “cross-link OR cross-links OR crosslink OR crosslinks OR <cross link> OR <cross links> OR <transverse connector> OR <transverse connectors>”.
- (2)
- Medline [All text]: “(crosslink OR crosslinks OR cross-link OR cross-links OR crosslinking OR <cross linking> OR cross-linking OR <transverse connector> OR <transverse connectors> OR connector OR connectors OR <rod connector> OR <rod connectors> OR transfixator OR transfixators OR <trans fixations>) AND (spine OR fusion OR stiffness OR fixation OR stability OR spondylodesis OR instrumentation) AND (randomized OR rct OR <clinical study> OR retrospective OR prospective OR <single center> OR single-center OR multi-center OR multicenter)”.
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Statistical Analysis
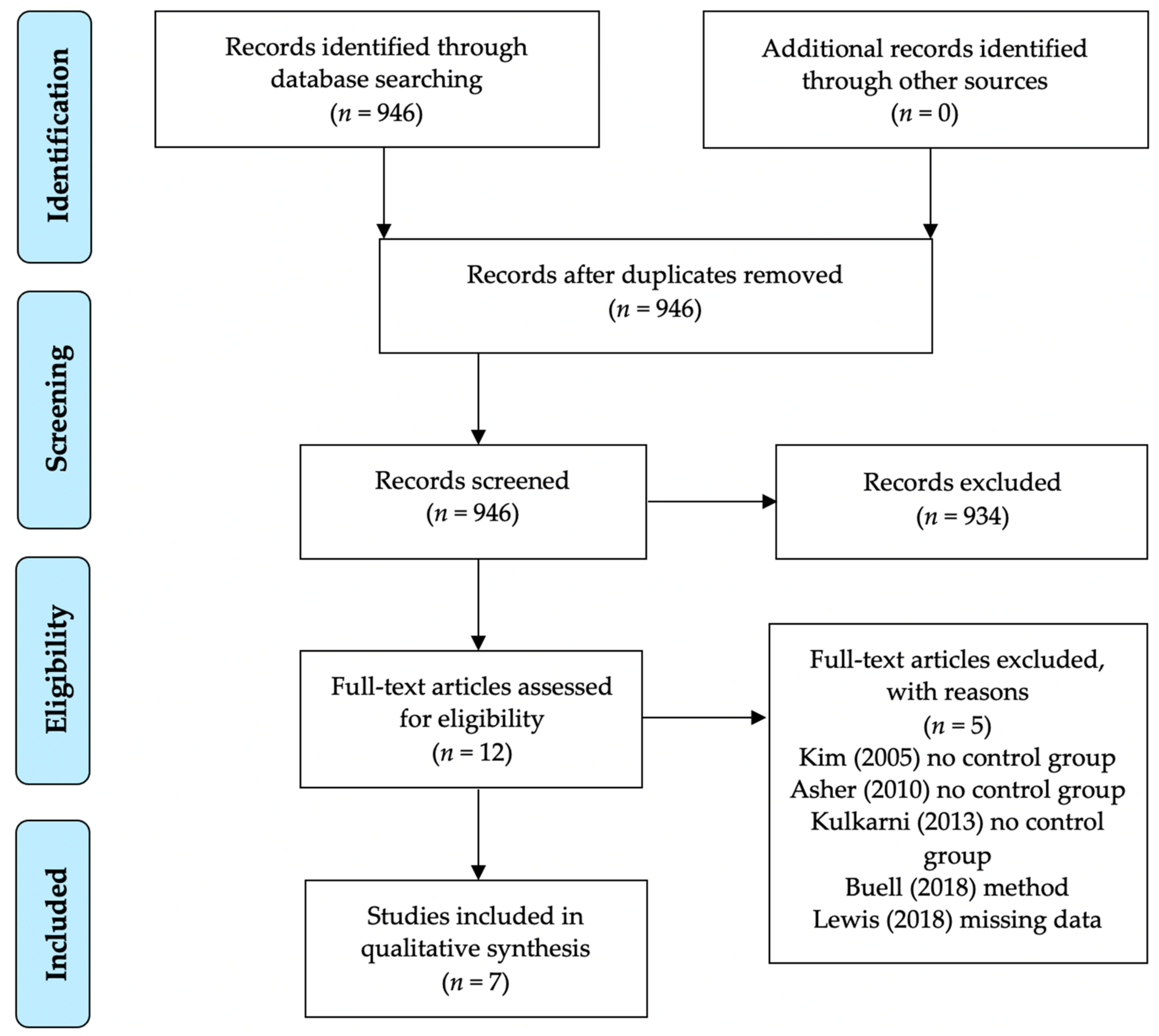
3. Results
3.1. Scoliosis
3.2. Atlantoaxial Fusion
3.3. Adult Short-Segment Fusion
3.4. Adult Long-Segment Fusion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hedlund, R.; Johansson, C.; Hagg, O.; Fritzell, P.; Tullberg, T.; Swedish Lumbar Spine Study Group. The long-term outcome of lumbar fusion in the Swedish lumbar spine study. Spine J. 2016, 16, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.; Hermsmeyer, J.T.; Sethi, R.K.; Norvell, D.C. Quality and Quantity of Published Studies Evaluating Lumbar Fusion during the Past 10 Years: A Systematic Review. Glob. Spine J. 2015, 5, 207–218. [Google Scholar] [CrossRef]
- El-Hawary, R.; Chukwunyerenwa, C. Update on evaluation and treatment of scoliosis. Pediatr. Clin. N. Am. 2014, 61, 1223–1241. [Google Scholar] [CrossRef]
- Rajaee, S.S.; Bae, H.W.; Kanim, L.E.; Delamarter, R.B. Spinal fusion in the United States: Analysis of trends from 1998 to 2008. Spine 2012, 37, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krag, M.H. Biomechanics of thoracolumbar spinal fixation. A review. Spine 1991, 16, S84–S99. [Google Scholar] [CrossRef] [PubMed]
- Koller, H.; Pfanz, C.; Meier, O.; Hitzl, W.; Mayer, M.; Bullmann, V.; Schulte, T.L. Factors influencing radiographic and clinical outcomes in adult scoliosis surgery: A study of 448 European patients. Eur. Spine J. 2016, 25, 532–548. [Google Scholar] [CrossRef] [PubMed]
- Sebaaly, A.; Lahoud, M.J.; Rizkallah, M.; Kreichati, G.; Kharrat, K. Etiology, evaluation, and treatment of failed back surgery syndrome. Asian Spine J. 2018, 12, 574–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- How, N.E.; Street, J.T.; Dvorak, M.F.; Fisher, C.G.; Kwon, B.K.; Paquette, S.; Smith, J.S.; Shaffrey, C.I.; Ailon, T. Pseudarthrosis in adult and pediatric spinal deformity surgery: A systematic review of the literature and meta-analysis of incidence, characteristics, and risk factors. Neurosurg. Rev. 2019, 42, 319–336. [Google Scholar] [CrossRef]
- Asher, M.; Carson, W.; Heinig, C.; Strippgen, W.; Arendt, M.; Lark, R.; Hartley, M. A modular spinal rod linkage system to provide rotational stability. Spine 1988, 13, 272–277. [Google Scholar] [CrossRef]
- Brodke, D.S.; Bachus, K.N.; Mohr, R.A.; Nguyen, B.K. Segmental pedicle screw fixation or cross-links in multilevel lumbar constructs. a biomechanical analysis. Spine J. 2001, 1, 373–379. [Google Scholar] [CrossRef]
- Chutkan, N.B.; Zhou, H.; Akins, J.P.; Wenger, K.H. Effects of facetectomy and crosslink augmentation on motion segment flexibility in posterior lumbar interbody fusion. Spine 2008, 33, E828–E835. [Google Scholar] [CrossRef]
- Dick, J.C.; Zdeblick, T.A.; Bartel, B.D.; Kunz, D.N. Mechanical evaluation of cross-link designs in rigid pedicle screw systems. Spine 1997, 22, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.; Hettwer, W.; Liu, Q.; Prem, S. Mechanical stiffness of segmental versus nonsegmental pedicle screw constructs: The effect of cross-links. Spine 2006, 31, E35–E38. [Google Scholar] [CrossRef] [PubMed]
- Kuklo, T.R.; Dmitriev, A.E.; Cardoso, M.J.; Lehman, R.A., Jr.; Erickson, M.; Gill, N.W. Biomechanical contribution of transverse connectors to segmental stability following long segment instrumentation with thoracic pedicle screws. Spine 2008, 33, E482–E487. [Google Scholar] [CrossRef]
- Lim, T.H.; Eck, J.C.; An, H.S.; Hong, J.H.; Ahn, J.Y.; You, J.W. Biomechanics of transfixation in pedicle screw instrumentation. Spine 1996, 21, 2224–2229. [Google Scholar] [CrossRef]
- Lynn, G.; Mukherjee, D.P.; Kruse, R.N.; Sadasivan, K.K.; Albright, J.A. Mechanical stability of thoracolumbar pedicle screw fixation. The effect of crosslinks. Spine 1997, 22, 1568–1572, discussion 1573. [Google Scholar] [CrossRef]
- Pintar, F.A.; Maiman, D.J.; Yoganandan, N.; Droese, K.W.; Hollowell, J.P.; Woodard, E. Rotational stability of a spinal pedicle screw/rod system. J. Spinal Disord. 1995, 8, 49–55. [Google Scholar] [CrossRef]
- Lim, T.H.; Kim, J.G.; Fujiwara, A.; Yoon, T.T.; Lee, S.C.; Ha, J.W.; An, H.S. Biomechanical evaluation of diagonal fixation in pedicle screw instrumentation. Spine 2001, 26, 2498–2503. [Google Scholar] [CrossRef]
- Wahba, G.M.; Bhatia, N.; Bui, C.N.; Lee, K.H.; Lee, T.Q. Biomechanical evaluation of short-segment posterior instrumentation with and without crosslinks in a human cadaveric unstable thoracolumbar burst fracture model. Spine 2010, 35, 278–285. [Google Scholar] [CrossRef]
- Lehman, R.A., Jr.; Dmitriev, A.E.; Wilson, K.W. Biomechanical analysis of the C2 intralaminar fixation technique using a cross-link and offset connector for an unstable atlantoaxial joint. Spine J. 2012, 12, 151–156. [Google Scholar] [CrossRef]
- Johnston, C.E., 2nd; Ashman, R.B.; Baird, A.M.; Allard, R.N. Effect of spinal construct stiffness on early fusion mass incorporation. Experimental study. Spine 1990, 15, 908–912. [Google Scholar] [CrossRef]
- Zeng, Z.L.; Zhu, R.; Wu, Y.C.; Zuo, W.; Yu, Y.; Wang, J.J.; Cheng, L.M. Effect of Graded Facetectomy on Lumbar Biomechanics. J. Healthc Eng. 2017, 2017, 7981513. [Google Scholar] [CrossRef]
- Zander, T.; Rohlmann, A.; Klockner, C.; Bergmann, G. Influence of graded facetectomy and laminectomy on spinal biomechanics. Eur. Spine J. 2003, 12, 427–434. [Google Scholar] [CrossRef] [Green Version]
- Overdevest, G.; Vleggeert-Lankamp, C.; Jacobs, W.; Thome, C.; Gunzburg, R.; Peul, W. Effectiveness of posterior decompression techniques compared with conventional laminectomy for lumbar stenosis. Eur. Spine J. 2015, 24, 2244–2263. [Google Scholar] [CrossRef] [Green Version]
- Burney, M.U.; Mukherjee, D.P.; Ogden, A.L.; Robinson, E.; McCall, R.E. A biomechanical study of posterior spinal instrumentation using pedicle screws with and without cross-links. J. Spinal Disord. Tech. 2005, 18, 364–368. [Google Scholar] [CrossRef]
- Valdevit, A.; Kambic, H.E.; McLain, R.F. Torsional stability of cross-link configurations: A biomechanical analysis. Spine J. 2005, 5, 441–445. [Google Scholar] [CrossRef]
- Kulkarni, A.G.; Dhruv, A.N.; Bassi, A.J. Should we cross the cross-links? Spine 2013, 38, E1128–E1134. [Google Scholar] [CrossRef]
- Garg, S.; Niswander, C.; Pan, Z.; Erickson, M. Cross-links do not improve clinical or radiographic outcomes of posterior spinal fusion with pedicle screws in adolescent idiopathic scoliosis: A multicenter cohort study. Spine Deform. 2015, 3, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, O.; et al. The Oxford Levels of Evidence 2. Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/index.aspx?o=5653 (accessed on 13 November 2020).
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.H.; Chen, X.; Zhu, Z.Z.; Wang, B.; Qian, B.P.; Zhu, F.; Sun, X.; Qiu, Y. Does addition of crosslink to pedicle-screw-based instrumentation impact the development of the spinal canal in children younger than 5 years of age? Eur. Spine J. 2015, 24, 1391–1398. [Google Scholar] [CrossRef]
- Dhawale, A.A.; Shah, S.A.; Yorgova, P.; Neiss, G.; Layer, D.J., Jr.; Rogers, K.J.; Gabos, P.G.; Holmes, L., Jr. Effectiveness of cross-linking posterior segmental instrumentation in adolescent idiopathic scoliosis: A 2-year follow-up comparative study. Spine J. 2013, 13, 1485–1492. [Google Scholar] [CrossRef]
- Garg, S.; Holland, C.; LaGreca, J.; McNair, B.; Erickson, M. Predicting failure of iliac fixation in neuromuscular spine deformity. Spine Deform. 2014, 2, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Mizutani, J.; Inada, A.; Kato, K.; Kondo, A.; Kainuma, S.; Fujita, K.; Yagi, K.; Shimamura, Y.; Fukuoka, M.; Shibamoto, Y.; et al. Advantages of an on-the-screwhead crosslink connector for atlantoaxial fixation using the Goel/Harms technique. J. Clin. Neurosci. 2018, 50, 183–189. [Google Scholar] [CrossRef]
- Usmani, M.F.; Shah, S.A.; Yaszay, B.; Samdani, A.F.; Cahill, P.J.; Newton, P.O.; Marks, M.C.; Sponseller, P.D. The role of cross-links in posterior spinal fusion for cerebral palsy-related scoliosis. Spine 2019, 44, E1256–E1263. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.W.; Yin, Y.H.; Li, T.; Yu, X.G.; Qiao, G.Y. Effects of transverse connector on reduction and fixation of atlantoaxial dislocation and basilar invagination using posterior C1-C2 screw-rod technique. Spine J. 2019, 19, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.A.; Lai, S.M.; Burton, D.C. Analysis of instrumentation/fusion survivorship without reoperation after primary posterior multiple anchor instrumentation and arthrodesis for idiopathic scoliosis. Spine J. 2010, 10, 5–15. [Google Scholar] [CrossRef]
- Wipplinger, C.; Melcher, C.; Hernandez, R.N.; Lener, S.; Navarro-Ramirez, R.; Kirnaz, S.; Schmidt, F.A.; Kim, E.; Hartl, R. “One and a half” minimally invasive transforaminal lumbar interbody fusion: Single level transforaminal lumbar interbody fusion with adjacent segment unilateral laminotomy for bilateral decompression for spondylolisthesis with bisegmental stenosis. J. Spine Surg. 2018, 4, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Grunert, P.; Reyes, P.M.; Newcomb, A.G.; Towne, S.B.; Kelly, B.P.; Theodore, N.; Hartl, R. Biomechanical Evaluation of Lumbar Decompression Adjacent to Instrumented Segments. Neurosurgery 2016, 79, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.C.; Pell, J.P. Parachute use to prevent death and major trauma related to gravitational challenge: Systematic review of randomised controlled trials. BMJ 2003, 327, 1459–1461. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author (Year) | Study Design | N | Minimum Follow-up (Months) | Level of Evidence | Risk of Bias |
|---|---|---|---|---|---|
| Scoliosis | |||||
| Usmani et al. (2019) | Retrospective | 256 | 24 | III | High |
| Garg et al. (2015) | Retrospective | 500 | 24 | III | High |
| Chen et al. (2015) | Retrospective | 34 | 24 | III | High |
| Garg et al. (2014) | Retrospective | 100 | 24 | IV | High |
| Dhawale et al. (2013) | Retrospective | 75 | 24 | III | High |
| Atlantoaxial Fusion | |||||
| Wang et al. (2019) | Retrospective | 317 | 12 | III | High |
| Mizutani et al. (2018) | Retrospective | 35 | 36 | IV | High |
| Author (Year) | Number of Patients | Sex | Age (Years) |
|---|---|---|---|
| N (XL/NXL) | Female/Male | Mean (±1 SD/Range) | |
| Scoliosis | |||
| Usmani et al. (2019) | 256 (94/162) | 123/33 | 14.0 (±2.7) |
| Garg et al. (2015) | 500 (377/123) | 413/83 (4 unknown) | 14.9 |
| Chen et al. (2015) | 34 (24/19) | 14/20 | 3.1 (1.8–4.8) |
| Garg et al. (2014) | 100 | 38/62 | 13.8 (7–21) |
| Dhawale et al. (2013) | 75 (25/50) | 61/14 | 14.0 (±2.3) |
| Atlantoaxial Fusion | |||
| Wang et al. (2019) | 317 (149/168) | 206/111 | 38.6 (13–74) |
| Mizutani et al. (2018) | 35 (18/17) | 27/8 | 56.1 (32–77) |
| Author (Year) | N | Treated Disease | Radiological Parameters Assesed | Results |
|---|---|---|---|---|
| Scoliosis | ||||
| Usmani et al. (2019) | 256 | Neuromuscular scoliosis | Major Cobb angle, pelvic obliquitiy, thoracal kyphosis, lumbar lordosis | No sign. difference at 24 months follow-up |
| Garg et al. (2015) | 500 | AIS | Coronal and saggital balance, shoulder high difference, trunk shift, coronal plane deformity measurements (Cobb angle) | Sign. less improvement in sagittal balance and sign. greater improvement in thoracolumbar Cobb angle in XL-group |
| Chen et al. (2015) | 34 | Congenital scoliosis | Spinal canal parameters (a.p./transverse), area of the spinal canal, screw-angle, distance between bilateral screws | No sign. negative effect on the develeopement of the spinal canal |
| Garg et al. (2014) | 100 | Neuromuscular scoliosis | Levels fused, coronal plane deformity, pelvic obliquity, distal fixation point, presence of implant failure/screw lucency > 2 mm | No predictor for pelvic fixation failure |
| Dhawale et al. (2013) | 75 | AIS | Thoracic/lumbar/lateral Cobb angle, correction rate, apical vertebral translation/rotation, Risser grade, Lenke classification | No sign. difference at 24 months follow-up |
| Atlantoaxial fusion | ||||
| Wang et al. (2019) | 317 | Atlantoaxial dislocation and basilar invagination | Ant./post. atlantodental interval, Chamberlain line, cervicomedullary angle, fusion rate | Sign. higher fusion rate in XL-group at 3/6/12 months follow-up |
| Mizutani et al. (2018) | 35 | Atlantoaxial subluxation | Fusion rate—bony union C1 posterior arch and C2 lamina, ankyosis lateral C1/2 joint | Sign. higher fusion rate in XL-group at 6/12/24 months follow-up without sign. difference 3 years after surgery |
| Author (Year) | N | Treated Disease | Clinical Parameters Assessed | Results |
|---|---|---|---|---|
| Scoliosis | ||||
| Usmani et al. (2019) | 256 | Neuromuscular scoliosis | NA | NA |
| Garg et al. (2015) | 500 | AIS | SRS-22r score (SRS-score), SAQ | Sign. improvement in health domain of SRS-score in XL-group. No sign. difference in SRS- or SAQ-score at 24 months follow-up |
| Chen et al. (2015) | 34 | Congenital scoliosis | NA | NA |
| Garg et al. (2014) | 100 | Neuromuscular scoliosis | NA | NA |
| Dhawale et al. (2013) | 75 | AIS | SRS 22r-score | No sign. difference in SRS-score at 24 months follow-up |
| Atlantoaxial fusion | ||||
| Wang et al. (2019) | 317 | Atlantoaxial dislocation and basilar invagination | Japanese Orthopaedic Association Score (JOA) | Sign. higher JOA-score in XL-group at 12 months follow-up |
| Mizutani et al. (2018) | 35 | Atlantoaxial subluxation | NA | NA |
| Author (Year) | N | Treated Disease | N Complication XL- vs. NXL-Group (%) | ||
|---|---|---|---|---|---|
| All | Surgical Side Infection | Reoperation | |||
| Scoliosis | |||||
| Usmani et al. (2019) | 256 | Neurom. Scoliosis | 14 (16)/23 (14) | 11 (12)/13 (8) | 3 (3.2)/4 (2.5) |
| Garg et al. (2015) | 500 | AIS | 21 (6)/9 (7) | 2 (0.5)/0 (0) | 4 (1.1)/(0) |
| Chen et al. (2015) | 34 | Congenital scoliosis | NA | NA | NA |
| Garg et al. (2014) | 100 | Neurom. Scoliosis | NA | NA | NA |
| Dhawale et al. (2013) | 75 | AIS | 1 (4)/1 (2) | 1 (4)/0 (0) | 1 (4)/1 (2) |
| Atlantoaxial Fusion | |||||
| Wang et al. (2019) | 317 | Atlantoaxial dislocation and basilar invagination | 7 (4.7)/9 (5.4) | NA | NA |
| Mizutani et al. (2018) | 35 | Atlantoaxial subluxation | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heck, V.J.; Oikonomidis, S.; Prasse, T.; Meyer, C.; Scheyerer, M.J.; Wetsch, W.A.; Eysel, P.; Bredow, J. Does the Current State of Evidence Justify the Broad Use of Cross-Links in Dorsal Instrumentation? A Systematic Review. BioMed 2021, 1, 1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed1010001
Heck VJ, Oikonomidis S, Prasse T, Meyer C, Scheyerer MJ, Wetsch WA, Eysel P, Bredow J. Does the Current State of Evidence Justify the Broad Use of Cross-Links in Dorsal Instrumentation? A Systematic Review. BioMed. 2021; 1(1):1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed1010001
Chicago/Turabian StyleHeck, Vincent J., Stavros Oikonomidis, Tobias Prasse, Carolin Meyer, Max J. Scheyerer, Wolfgang A. Wetsch, Peer Eysel, and Jan Bredow. 2021. "Does the Current State of Evidence Justify the Broad Use of Cross-Links in Dorsal Instrumentation? A Systematic Review" BioMed 1, no. 1: 1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed1010001