Are Trauma Surgery Simulation Courses Beneficial in Low- and Middle-Income Countries—A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias
2.6. Statistical Analysis
3. Results
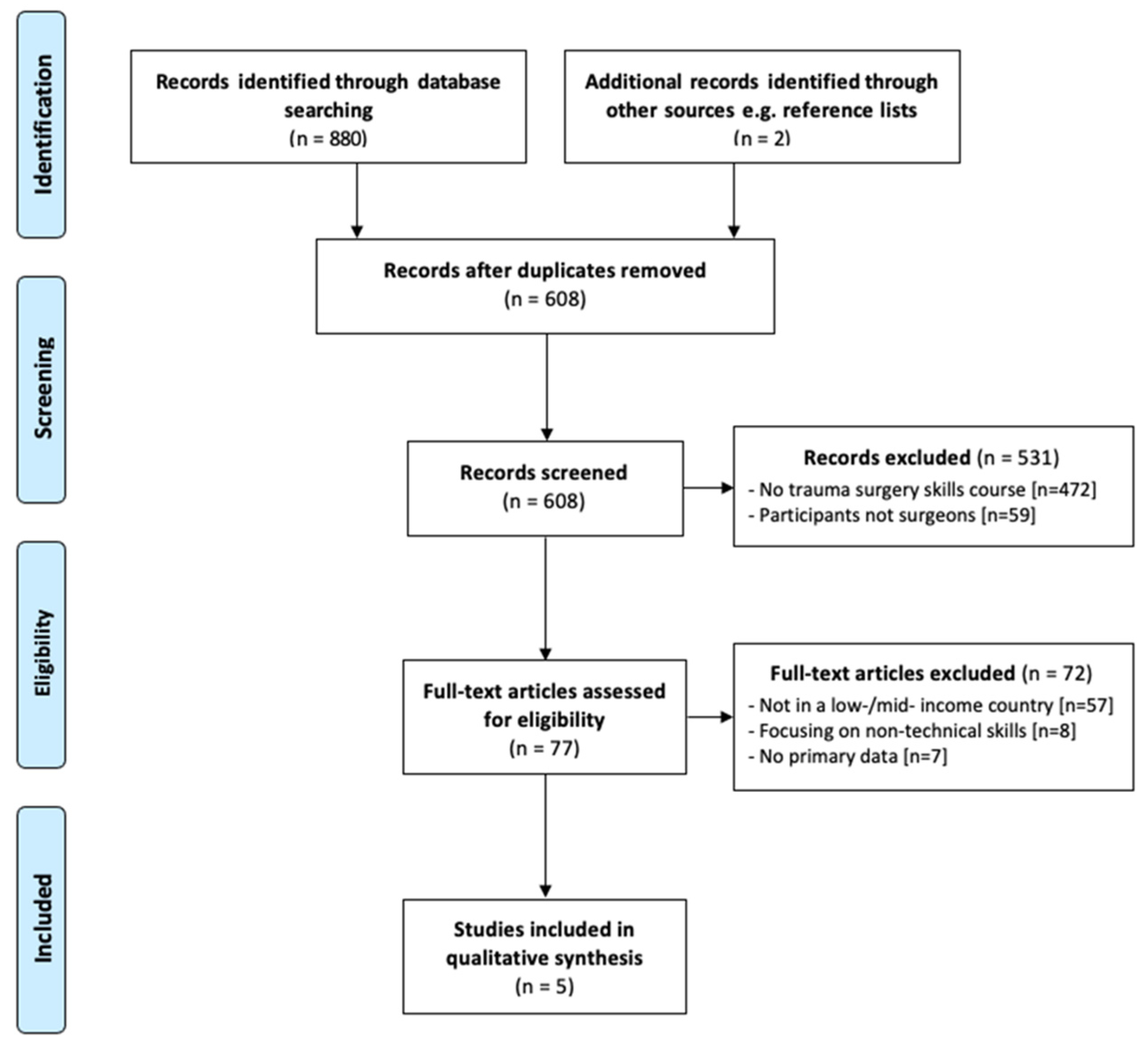
3.1. Study Selection
3.2. Study Characteristics
3.3. Results of Individual Studies—Primary Outcome
3.4. Results of Individual Studies—Secondary Outcomes
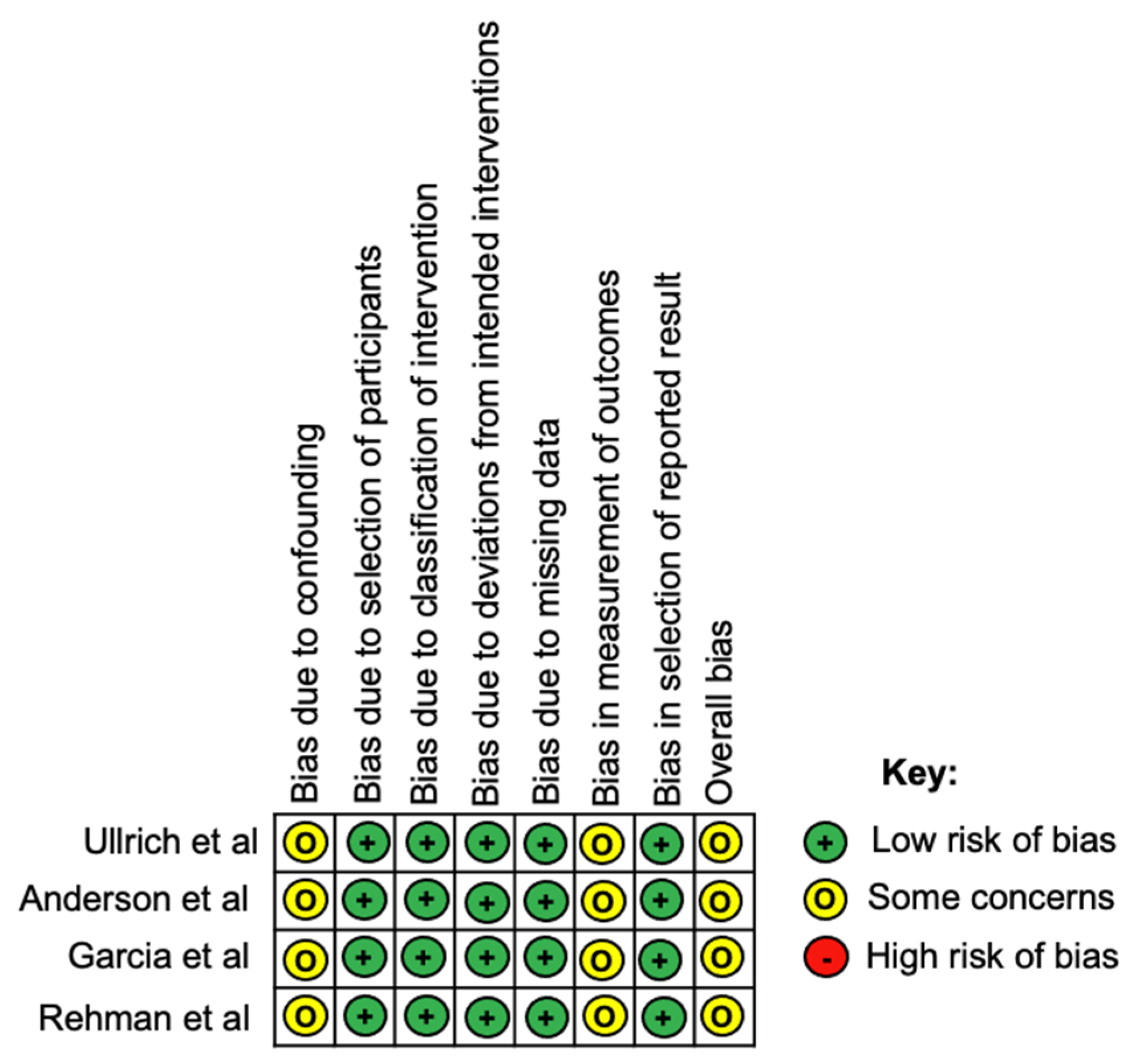
3.5. Risk of Bias in Studies
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gosselin, R.A.; Spiegel, D.A.; Coughlin, R.; Zirkle, L.G. Injuries: The neglected burden in developing countries. Bull. World Health Organ. 2009, 87, 246a. [Google Scholar] [CrossRef]
- Meara, J.G.; Leather, A.; Hagander, L.; Alkire, B.C.; Alonso, N.; Ameh, E.A.; Bickler, S.W.; Conteh, L.; Dare, A.J.; Davies, J.; et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet 2015, 386, 569–624. [Google Scholar] [CrossRef]
- Whitaker, J.; O’Donohoe, N.; Denning, M.; Poenaru, D.; Guadagno, E.; Leather, A.J.M.; Davies, J.I. Assessing trauma care systems in low-income and middle-income countries: A systematic review and evidence synthesis mapping the Three Delays framework to injury health system assessments. BMJ Glob. Health 2021, 6, e004324. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.G.; Lecky, F.; Bouamra, O.; Lawrence, T.; Edwards, A.; Woodford, M.; Willett, K.; Coats, T.J. Changing the System—Major Trauma Patients and Their Outcomes in the NHS (England) 2008–17. EClinicalMedicine 2018, 2–3, 13–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakran, J.V.; Greer, S.E.; Werlin, E.; McCunn, M. Care of the injured worldwide: Trauma still the neglected disease of modern society. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 64. [Google Scholar] [CrossRef] [Green Version]
- Hyder, A.; He, S.; Zafar, W.; Mir, M.; Razzak, J. One hundred injured patients a day: Multicenter emergency room surveillance of trauma in Pakistan. Public Health 2017, 148, 88–95. [Google Scholar] [CrossRef]
- Fernandez, G.L.; Page, D.W.; Coe, N.P.; Lee, P.C.; Patterson, L.A.; Skylizard, L.; Louis, M.S.; Amaral, M.H.; Wait, R.B.; Seymour, N.E. Boot Camp: Educational Outcomes after 4 Successive Years of Preparatory Simulation-Based Training at Onset of Internship. J. Surg. Educ. 2012, 69, 242–248. [Google Scholar] [CrossRef]
- Mohammad, A.; Branicki, F.; Abu-Zidan, F.M. Educational and Clinical Impact of Advanced Trauma Life Support (ATLS) Courses: A Systematic Review. World J. Surg. 2013, 38, 322–329. [Google Scholar] [CrossRef]
- Hanche-Olsen, T.P.; Alemu, L.; Viste, A.; Wisborg, T.; Hansen, K.S. Trauma care in Africa: A status report from Botswana, guided by the World Health Organization’s “Guidelines for Essential Trauma Care”. World J. Surg. 2012, 36, 2371–2383. [Google Scholar] [CrossRef] [Green Version]
- Aboutanos, M.B.; Mora, F.; Rodas, E.; Salamea, J.; Parra, M.O.; Salgado, E.; Mock, C.; Ivatury, R. Ratification of IATSIC/WHO’s Guidelines for Essential Trauma Care Assessment in the South American Region. World J. Surg. 2010, 34, 2735–2744. [Google Scholar] [CrossRef]
- Mock, C.; Nguyen, S.; Quansah, R.; Arreola-Risa, C.; Viradia, R.; Joshipura, M.; Nguyen, T.S. Evaluation of Trauma Care Capabilities in Four Countries Using the WHO-IATSIC Guidelines for Essential Trauma Care. World J. Surg. 2006, 30, 946–956. [Google Scholar] [CrossRef]
- Kesinger, M.R.; Puyana, J.C.; Rubiano, A.M. Improving Trauma Care in Low- and Middle-Income Countries by Implementing a Standardized Trauma Protocol. World J. Surg. 2014, 38, 1869–1874. [Google Scholar] [CrossRef] [PubMed]
- Kadhum, M.; Sinclair, P.; Lavy, C. Are Primary Trauma Care (PTC) courses beneficial in low- and middle-income countries—A systematic review. Injury 2020, 51, 136–141. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, C.F.; Tisherman, S.A.; Shackelford, S.; Sevdalis, N.; Elster, E.; Bowyer, M.W. Efficacy of Trauma Surgery Technical Skills Training Courses. J. Surg. Educ. 2019, 76, 832–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- The World Bank. Data on Countries and Economies 2021. Available online: https://data.worldbank.org/country (accessed on 1 September 2021).
- Jüni, P.; Loke, Y.; Pigott, T.; Ramsay, C.; Regidor, D.; Rothstein, H.; Sandhu, L.; Santaguida, P.L.; Schünemann, H.J.; Shea, B.; et al. Risk of bias in non-randomized studies of interventions (ROBINS-I): Detailed guidance. Br. Med. J. 2016, 355, i4919. [Google Scholar]
- Ullrich, S.J.; DeWane, M.P.; Cheung, M.; Fleming, M.; Namugga, M.M.; Fu, W.; Kurigamba, G.; Kabuye, R.; Mabweijano, J.; Galukande, M.; et al. Development of an Operative Trauma Course in Uganda—A Report of a Three-Year Experience. J. Surg. Res. 2020, 256, 520–527. [Google Scholar] [CrossRef]
- Anderson, G.A.; Kayima, P.; Ilcisin, L.; Benitez, N.P.; Albutt, K.H.; Briggs, S.M.; Nehra, D. Development of a Comprehensive Trauma Training Curriculum for the Resource-Limited Environment. J. Surg. Educ. 2018, 75, 1317–1324. [Google Scholar] [CrossRef]
- Rehman, Z.U.; Moosa, M.A.; Riaz, Q. Knowledge gain of the non-vascular surgeons after attending a course on traumatic vascular emergencies. J. Pak. Med. Assoc. 2020, 70, S6–S9. [Google Scholar]
- Garcia, D.F.; Domingues, C.A.; Silva, F.S.; Mori, N.D.; Brasel, K.J.; Kortbeek, J.; Ali, J.; Poggetti, R.S. Efficacy of a novel surgical manikin for simulating emergency surgical procedures. Am. Surg. 2019, 85, 1318–1324. [Google Scholar] [CrossRef]
- Jacobs, L.M.; Burns, K.J.; Luk, S.S.; Cornwell, E.E., 3rd; Adebonojo, S.A. Advanced trauma operative management course introduced to surgeons in West Africa. Bull. Am. Coll. Surg. 2005, 90, 8–14. [Google Scholar]
- Carley, S.; Driscoll, P. Trauma education. Resuscitation 2001, 48, 47–56. [Google Scholar] [CrossRef]
- Flint, L. Achievements, present-day problems, and some solutions for trauma care, surgical critical care, and surgical education. Am. J. Surg. 1991, 161, 207–212. [Google Scholar] [CrossRef]
- Hogan, M.P.; Boone, D.C. Trauma education and assessment. Injury 2008, 39, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Mock, C.; Joshipura, M.; Goosen, J.; Lormand, J.D.; Maier, R. Strengthening Trauma Systems Globally: The Essential Trauma Care Project. J. Trauma Inj. Infect. Crit. Care 2005, 59, 1243–1246. [Google Scholar] [CrossRef] [PubMed]
- Higashi, H.; Barendregt, J.J.; Kassebaum, N.J.; Weiser, T.G.; Bickler, S.W.; Vos, T. Burden of Injuries Avertable by a Basic Surgical Package in Low- and Middle-Income Regions: A Systematic Analysis from the Global Burden of Disease 2010 Study. World J. Surg. 2014, 39, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bohl, M.A.; McBryan, S.; Spear, C.; Pais, D.; Preul, M.C.; Wilhelmi, B.; Yeskel, A.; Turner, J.D.; Kakarla, U.K.; Nakaji, P. Evaluation of a novel surgical skills training course: Are cadavers still the gold standard for surgical skills training? World Neurosurg. 2019, 127, 63–71. [Google Scholar] [CrossRef]
- Buzink, S.; Soltes, M.; Radoňak, J.; Fingerhut, A.; Hanna, G.; Jakimowicz, J. Laparoscopic Surgical Skills programme: Preliminary evaluation of Grade I Level 1 courses by trainees. Videosurg. Other Miniinvasive Tech. 2012, 3, 188–192. [Google Scholar] [CrossRef]
- Moore, L.; Champion, H.; Tardif, P.-A.; Kuimi, B.-L.; O’Reilly, G.; Leppaniemi, A.; Cameron, P.; Palmer, C.S.; Abu-Zidan, F.M.; Gaarder, C.; et al. Impact of Trauma System Structure on Injury Outcomes: A Systematic Review and Meta-Analysis. World J. Surg. 2017, 42, 1327–1339. [Google Scholar] [CrossRef] [Green Version]
- Van Hove, P.; Tuijthof, G.; Verdaasdonk, E.; Stassen, L.; Dankelman, J. Objective assessment of technical surgical skills. J. Br. Surg. 2010, 97, 972–987. [Google Scholar] [CrossRef]
- Mitchell, E.L.; Arora, S.; Moneta, G.L.; Kret, M.R.; Dargon, P.T.; Landry, G.J.; Eidt, J.F.; Sevdalis, N. A systematic review of assessment of skill acquisition and operative competency in vascular surgical training. J. Vasc. Surg. 2014, 59, 1440–1455. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, L.; Burns, K.; Luk, S.; Hull, S. Advanced Trauma Operative Management Course: Participant Survey. World J. Surg. 2009, 34, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Catchpole, K.; Dale, T.; McCulloch, P. The influence of non-technical performance on technical outcome in laparoscopic cholecystectomy. Surg. Endosc. 2007, 22, 68–73. [Google Scholar] [CrossRef]
- Cioe-Pena, E.; Granados, J.; Wrightsmith, L.; Henriquez-Vigil, A.; Moresky, R. Development and implementation of a hospital-based trauma response system in an urban hospital in San Salvador, El Salvador. Trauma 2016, 19, 118–126. [Google Scholar] [CrossRef]
- Dickason, R.M.; Cioe-Pena, E.; Chisolm-Straker, M. Primary trauma care curriculum: A qualitative analysis of impediments to improvement. Trauma 2016, 19, 127–132. [Google Scholar] [CrossRef]
- James, H.K.; Chapman, A.W.; Pattison, G.; Griffin, D.R.; Fisher, J.D. Systematic review of the current status of cadaveric simulation for surgical training. BJS 2019, 106, 1726–1734. [Google Scholar] [CrossRef] [Green Version]
- Bowyer, M.W.; Kuhls, D.A.; Haskin, D.; Sallee, R.A.; Henry, S.M.; Garcia, G.D.; Luchette, F. Advanced surgical skills for exposure in trauma (ASSET): The first 25 courses. J. Surg. Res. 2013, 183, 553–558. [Google Scholar] [CrossRef]
- Sheikh, A.H.; Barry, D.S.; Gutierrez, H.; Cryan, J.F.; O’Keeffe, G.W. Cadaveric anatomy in the future of medical education: What is the surgeons view? Anat. Sci. Educ. 2016, 9, 203–208. [Google Scholar] [CrossRef]
- Stefanidis, D.; Yonce, T.C.; Green, J.M.; Coker, A.P. Cadavers versus pigs: Which are better for procedural training of surgery residents outside the OR? Surgery 2013, 154, 34–37. [Google Scholar] [CrossRef]
- Hall, A.B. Randomized objective comparison of live tissue training versus simulators for emergency procedures. Am. Surg. 2011, 77, 561–565. [Google Scholar] [CrossRef]
- Bellanova, G.; Buccelletti, F.; Berletti, R.; Cavana, M.; Folgheraiter, G.; Groppo, F.; Marchetti, C.; Marzano, A.; Masse’, A.; Musetti, A.; et al. How formative courses about damage control surgery and non-operative management improved outcome and survival in unstable politrauma patients in a Mountain Trauma Center. Ann. Ital. Di Chir. 2016, 87, 68–74. [Google Scholar]
- Ng-Kamstra, J.S.; Arya, S.; Greenberg, S.L.M.; Kotagal, M.; Arsenault, C.; Ljungman, D.; Yorlets, R.R.; Agarwal, A.; Frankfurter, C.; Nikouline, A.; et al. Perioperative mortality rates in low-income and middle-income countries: A systematic review and meta-analysis. BMJ Glob. Health 2018, 3, e000810. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Surgeons Surgical trainees | Medical students, non-surgical doctors, and other allied health specialties such as nurses, midwives, and physiotherapists. |
| Intervention | Trauma surgery simulation courses conducted in low- or middle-income countries as defined by The World Bank Classification [16] | Non-trauma related surgical courses (e.g., elective orthopaedic surgery courses, general surgery courses etc.) Courses with no operative tasks. |
| Comparison | N/A | N/A |
| Outcome | Primary outcome: clinical/operative knowledge improvement Secondary outcomes: general course feedback scores, immediate and long-term self-rated confidence scores | N/A |
| Study design | Primary data studies including randomised controlled trials and observational studies | Reviews, abstracts, case reports or quality improvement projects |
| Study | Course | Course Format | Course Length | Course Content | Cost Description |
|---|---|---|---|---|---|
| Ullrich et al., 2020 [18] | M-OTR | Didactic lectures. Practical sessions, daily cadaver lab sessions. | 3 days | Team management dynamics. Primary and secondary survey. Airway management. Ultrasound uses in trauma. Trauma radiology. Penetrating + blunt injuries to the neck, chest, abdomen, and pelvis. | $5000 initial investment and $1500 per course. $186 charged per student. |
| Anderson et al., 2018 [19] | STaRTLE | Didactic lectures. Practical sessions, cadaver-based surgical technique education. | 2 days | Operative techniques in the chest, abdomen, neck and extremities. | Unspecified (low). |
| Rehman et al., 2020 [20] | EVSC | Interactive lectures. Video demonstrations. Practical vascular skills training on animal models. | 1 day | Common vascular emergencies. Vessel exposure. Arteriotomy and primary closure. End-to end anastomosis. Shunt placement. Performing embolectomy. Performing fasciotomy. | Unspecified. |
| Garcia et al., 2019 [21] | ATLS (surgical skills stations) | 60 min per station (n = 3). Procedures simulated on TraumaMan, SurgeMan and live animals. | 1 day | Cricothyroidotomy Tube thoracostomy Pericardiocentesis Diagnostic peritoneal lavage | TraumaMan simulator; $30,000 initial investment + $6000 per course. SurgMan simulator; $2500 initial investment + $650 per course. |
| Jacobs et al., 2005 [22] | ATOM | Didactic lectures (n = 6). Practical operative skills sessions on 50 kg swine with 12 pre-created standardised injuries. | 1 day | Injuries to various organ systems including trauma to the bowel, bladder, ureter, kidney, duodenum, pancreas, liver, stomach, spleen, diaphragm, inferior vena cava, and heart. | Unspecified (high). |
| Study | Course | Location | Study Design | Participants | Outcome Measures |
|---|---|---|---|---|---|
| Ullrich et al., 2020 [18] | M-OTR | Kampala, Uganda | Non-randomised cross-sectional study | 52 surgical trainees | Knowledge improvement via pre- and post-course test (n = 48). General course review survey. General trauma education needs assessment survey (n = 28). Resource utilisation survey (n = 18). |
| Anderson et al., 2018 [19] | STaRTLE | Mbarara, Uganda | Non-randomised cross-sectional study | 8 surgical trainees | Knowledge improvement via pre- and post-course test (n = 8). Participant operative skill confidence via pre- and post-course survey (n = 8). Long-term operative skill confidence via 1–2 month (n = 8) and 1-year survey (n = 4). |
| Rehman et al., 2020 [20] | EVSC | Karachi, Pakistan | Non-randomised cross-sectional study | 21 total participants, 18 surgical trainees and 3 consultant surgeons | Knowledge improvement via pre- and post-course test (n = 21). General course review survey (n = 21). |
| Garcia et al., 2019 [21] | ATLS (surgical skills stations) | Sao Paulo, Brazil | Randomised prospective crossover study | 36 surgical trainees | User satisfaction of SurgeMan, TraumaMan and animal models for use in surgical skills station via survey (n = 36). |
| Jacobs et al., 2005 [21] | ATOM | Accra, Ghana | n/a | 55 surgeons | n/a |
| Study | Course Assessment | Participants | Mean Pre-Test Score (% ± SD) | Mean Post-Test Score (% ± SD) | p-Value |
|---|---|---|---|---|---|
| Ullrich et al., 2020 [18] | Written exam | n = 48/52 | 56.0 ± 10.0 | 79.0 ± 9.0 | <0.05 |
| Anderson et al., 2018 [19] | 20-item MCQ | n = 8/8 | 50.7 ± 10.5 | 73.6 ± 9.1 | 0.002 |
| Rehman et al., 2020 [20] | 20-item MCQ | n = 21/21 | 59.5 ± 21.3 | 81.6 ± 16.6 | <0.001 |
| Combined | Written exam/MCQ | n = 77/81 | 55.4 ± 13.9 | 78.1 ± 11.6 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashmi, Y.; Ayyaz, N.; Umar, H.; Jawaid, A.; Ahmed, Z. Are Trauma Surgery Simulation Courses Beneficial in Low- and Middle-Income Countries—A Systematic Review and Meta-Analysis. Trauma Care 2021, 1, 130-142. https://0-doi-org.brum.beds.ac.uk/10.3390/traumacare1030012
Hashmi Y, Ayyaz N, Umar H, Jawaid A, Ahmed Z. Are Trauma Surgery Simulation Courses Beneficial in Low- and Middle-Income Countries—A Systematic Review and Meta-Analysis. Trauma Care. 2021; 1(3):130-142. https://0-doi-org.brum.beds.ac.uk/10.3390/traumacare1030012
Chicago/Turabian StyleHashmi, Yousuf, Nashmeeya Ayyaz, Hamza Umar, Anam Jawaid, and Zubair Ahmed. 2021. "Are Trauma Surgery Simulation Courses Beneficial in Low- and Middle-Income Countries—A Systematic Review and Meta-Analysis" Trauma Care 1, no. 3: 130-142. https://0-doi-org.brum.beds.ac.uk/10.3390/traumacare1030012