COVID-19 Vaccinated Individuals Can Be a Source of SARS-CoV-2 Transmission—A Systematic Review

Institute for Hygiene and Environmental Medicine, University Medicine Greifswald, Ferdinand-Sauerbruch-Strasse, 17475 Greifswald, Germany
Hygiene 2021, 1(1), 1-11; https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene1010001
Submission received: 7 April 2021
/
Revised: 7 May 2021
/
Accepted: 12 May 2021
/
Published: 20 May 2021
Abstract
:Fundamental rights are probably given back earlier to COVID-19 vaccinated individuals assuming that they cannot spread SARS-CoV-2 anymore. The objective of the study was to determine if COVID-19 vaccinated individuals can still be the source of SARS-CoV-2 transmission. PubMed was searched for studies on 4 April 2021. All studies with original data on COVID-19 cases among vaccinated individuals (phase III RCTs) and on viral load in the upper respiratory tract of vaccinated macaques after a SARS-CoV-2 challenge were included. Symptomatic COVID-19 cases were found in four trials among vaccinated participants although less frequently than among control subjects. One study revealed asymptomatic COVID-19 cases in a similar frequency among 2.168 AZD1222-vaccinated subjects (1.0%) compared to 2.223 control subjects (1.0%). In 15 studies with vaccinated macaques, it was found that the load of SARS-CoV-2 RNA, subgenomic RNA and infectious virus in the upper respiratory tract is variable. Sterilizing immunity was found in none of the animal studies. Major limitations of the animal studies are that the SARS-CoV-2 challenge took place within a few weeks of the final or only vaccine dose, that the viral challenge was often high and, in some studies, administered by up to four routes. Based on current knowledge it seems clear that COVID-19 vaccinated individuals can still be the source of SARS-CoV-2 transmission.
1. Introduction
COVID-19 is spreading worldwide. In addition to many non-pharmaceutical measures [1], the vaccination against COVID-19 is regarded as a another element to reduce the probability of severe disease [2]. Many countries aim to reach a high proportion of vaccinated citizens. The German Minster of Justice, Christine Lambrecht, recently indicated that the restriction of fundamental rights during the COVID-19 pandemic can be taken back for vaccinated citizens when there is solid evidence that they cannot transmit SARS-CoV-2 anymore [3]. A similar vision was communicated by Jens Spahn, the Minister for Health in Germany. He indicated that individuals should be able visit shops without a rapid antigen test once they have completed a COVID-19 vaccination scheme [4]. That is why many people consider a vaccination for themselves with the aim to get fundamental rights back earlier. In addition, Dodd et al. have recently described that the two main motivations for COVID-19 vaccination are for individuals to protect themselves and others and to help to stop the virus spread [5]. This is the reason why quite a few healthcare workers consider a vaccination for themselves—to reduce the probability of severe COVID-19 and to prevent an unnoticed transmission of SARS-CoV-2 to their patients while being asymptomatic or presymptomatic. A similar motivation to avoid spreading the influenza virus among the general population has been described among medical residents in Italy for the influenza vaccination [6]. The aim of the review is therefore to find out if COVID-19 vaccinated individuals can still be the source of SARS-CoV-2 transmission irrespective of the presence of symptoms.
2. Materials and Methods
A Medline search was done on 4 April 2021 using the following terms: “COVID-19”, “phase 3” and “vaccine” (63 hits), “COVID-19”, “phase III” and “vaccine” (108 hits), and “COVID-19”, “macaques” and “vaccine” (87 hits). All studies were screened by the author for original data for the frequency of symptomatic or asymptomatic COVID-19 cases among vaccinated individuals or macaques. In addition, the macaque studies were screened for original data on the viral load in the upper respiratory tract of vaccinated animals. Published peer-reviewed research articles and preprints were included. The effect of the vaccination on the incidence of COVID-19 cases (phase III RCTs) and on the viral load (genomic RNA, subgenomic RNA, infectious SARS-CoV-2) in the upper respiratory tract (nose or pharynx) of vaccinated macaques was extracted. This may allow the determination of whether SARS-CoV-2 transmission is still possible. The results are presented in tables and always compared to the control groups of non-vaccinated individuals or macaques.
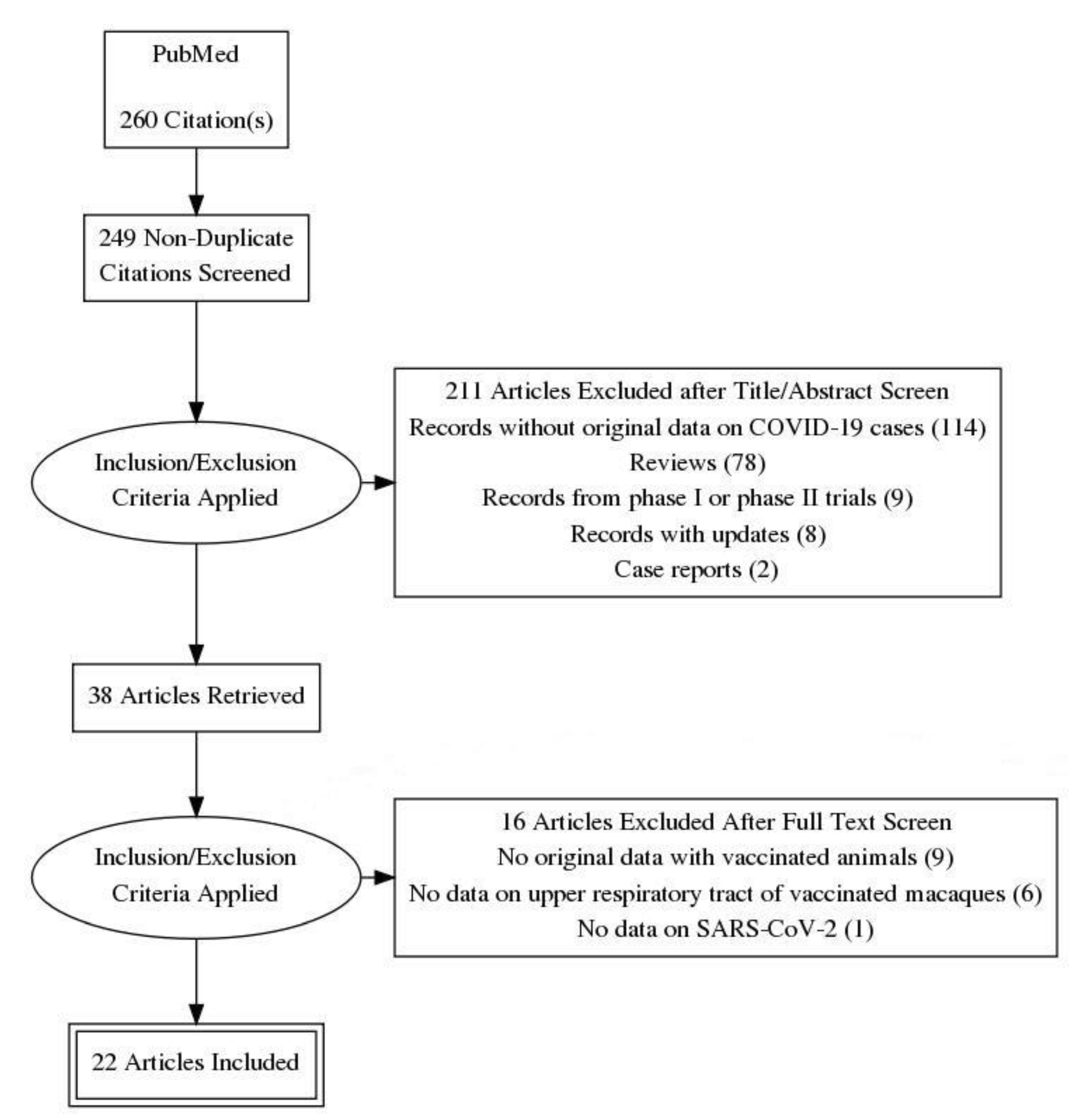
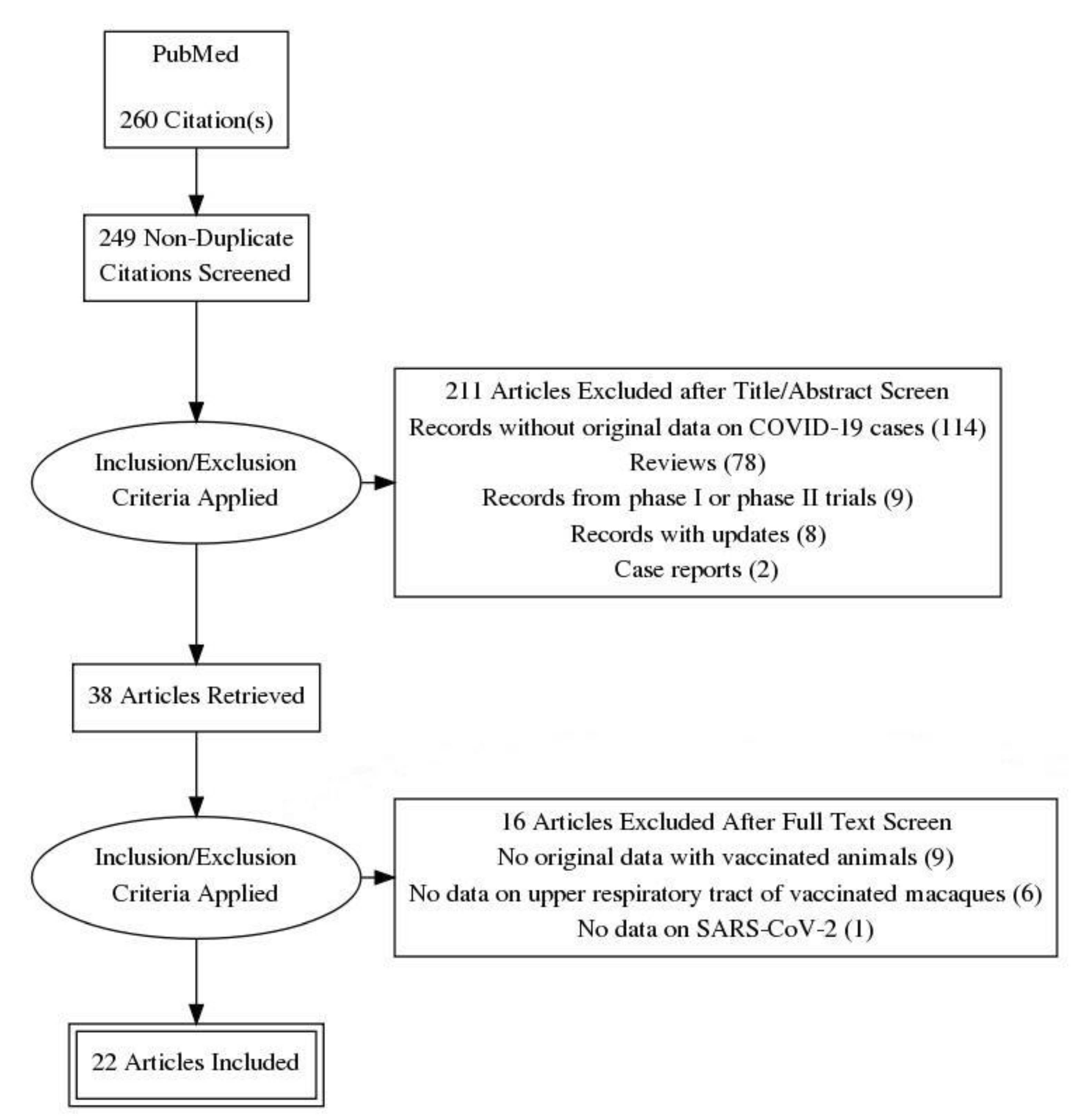
Data were extracted from studies that describe COVID-19 cases among vaccinated individuals or macaques. In addition, viral load data were extracted from studies with vaccinated and artificially infected macaques (Figure 1).
3. Results
3.1. Symptomatic Vaccinated COVID-19 Cases as a Possible Source
Four phase III trials were found with original data on symptomatic COVID-19 cases among vaccinated and control subjects (Table 1). Symptomatic COVID-19 cases were found in each trial among vaccinated individuals although at a significantly lower proportion compared to the groups of control subjects. In addition, of a subgroup of 373 study participants vaccinated with standard dose of AZD1222, two of them were identified as symptomatic COVID-19 cases (0.5%) [7]. Based on these data it is clear that a small proportion of vaccinated individuals may still get COVID-19 and thereby be a possible source for viral spread.
A recent analysis of COVID-19 infections among vaccinated and non-vaccinated healthcare workers revealed that 89.3% of COVID-19 infections were associated with symptoms with only 22.9% of them requiring medical attention whereas only 10.7% remained asymptomatic [11]. A total of 11 COVID-19 infections were noticed among the vaccinated healthcare workers, three of them were found more than 14 days after the second the second dose [11].
3.2. Asymptomatic Vaccinated COVID-19 Cases as a Possible Source
The same phase III trials were screened for information on the number of asymptomatic COVID-19 cases among vaccinated and control subjects. In the studies with BNT162b2 (BioNTech) and Sputnik V (Gamaleya), asymptomatic COVID-19 cases were not included in the analysis [9,10]. The results in the trial with mRNA 1273 (Moderna) on asymptomatic COVID-19 cases were described to be insufficient although some degree of prevention seemed to be possible [8]. The trial with AZD1222 (AstraZeneca) looked in addition at subjects with a positive SARS-CoV-2 RNA test result but without symptoms or with unknown symptoms. Among the 2.168 vaccinated seronegative subjects 22 were found as asymptomatic COVID-19 cases (1.0%), among the 2.223 seronegative control subjects 23 asymptomatic COVID-19 cases were detected (1.0%). In addition, of a subgroup of 373 seropositive study participants vaccinated with the standard dose of AZD1222, one of them was identified as an asymptomatic COVID-19 case (0.3%) [7].
3.3. Viral Clearance in Vaccinated and Artificially Infected Macaques
The efficacy of COVID-19 vaccines has also been studied in macaques because they develop an acute infection when challenged with SARS-CoV-2 [12,13,14,15]. The speed and extent of the viral clearance in the upper respiratory tract in vaccinated macaques may also indicate if they may spread SARS-CoV-2 despite vaccination.
3.3.1. Genomic RNA of SARS-CoV-2
The load of genomic SARS-CoV-2 RNA was not significantly reduced in vaccinated animals compared to the control group when AZD1222 was used (intramuscular or intranasal vaccination) [16,17]. A partial effect was seen with BNT162b2 [18], SARSCoV-2 S-I53-50NP [19], BBV152 [20], six different DNA vaccines [21], RBD [22], BBIBP-CorV [23], YF17D [24] and ChAd-SARS-CoV-2-S [25], but a statistical evaluation is lacking. In none of the studies the upper respiratory tract of vaccinated animals was clear of genomic SARS-CoV-2 RNA at the first time of sampling after the challenge (Table 2).
3.3.2. Subgenomic RNA of SARS-CoV-2
Subgenomic RNAs are generated after cell entry and are poorly incorporated into mature virions, and thus may provide a marker for actively replicating virus. It allows to distinguish actively replicating virus from input challenge virus [26]. The load of subgenomic SARS-CoV-2 RNA was not significantly lower in vaccinated animals compared to control animals when the animals were vaccinated with AZD1222 (intramuscular or intranasal vaccination) [16,17]. A partial effect was seen with six different DNA vaccines [21], Variant S.PP [27], mRNA-1273 [28], Vaccine Ad5-S-nb2 [29], most doses of Ad26.COV2.S [30], an MVA-based COVID-19 vaccine [31] and ChAd-SARS-CoV-2-S [25]. After vaccination with SARSCoV-2 S-I53-50NP [19], BBV152 [20], RBD [22], VX-CoV2327 vaccine [32] and the highest dose of Ad26.COV2.S [30], the upper respiratory tract of vaccinated animals was clear of subgenomic SARS-CoV-2 RNA at the first time of sampling suggesting a lack of relevant viral replication after the challenge (Table 3).
3.3.3. Infectious SARS-CoV-2
Infectious SARS-CoV-2 can remain in the upper respiratory tract for a few days after a viral challenge although the number of animals with infectious viruses and the number of infectious viruses per sample were much lower in all four studies (Table 4).
4. Discussion
Current evidence clearly shows that a small proportion of vaccinated individuals can still become a symptomatic COVID-19 case, even those individuals with a COVID-19 infection prior to vaccination (seropositive study participants) [16,17,25,27]. In addition, the phase III trial with AZD1222 provides evidence that the proportion of asymptomatic COVID-19 cases is equal in AZD1222-vaccinated and control subjects suggesting that viral clearance in the upper respiratory tract is more or less equal among vaccinated and control subjects. Vaccinated asymptomatic viral carriers may be more relevant for transmission because they do not even know or suspect that they may spread SARS-CoV-2.
All of the vaccines tested to date have conferred a substantial degree of protection to the immunized macaques although only a small number of animals was investigated in each study. That is why it is difficult to draw major conclusions without further study. In most macaques, there is no reasonable evidence for complete protection (i.e., “sterilizing immunity”) within a few weeks after vaccination completion. The majority of studies provide evidence for remaining SARS-CoV-2 RNA in the upper respiratory tract after a viral challenge. Most studies described viral replication in the upper respiratory tract of vaccinated animals measuring subgenomic RNA. Few studies demonstrated that infectious SARS-CoV-2 can also remain in the upper respiratory tract for a few days after a viral challenge although the number of animals with infectious viruses and the number of infectious viruses per sample were much lower in all of the vaccinated compared to the control groups. Similar findings have been described in macaques which were artificially infected with SARS-CoV-2 and rechallenged with the virus after viral clearance [33].
Animal studies have major limitations. One of them is that the severity of COVID-19 disease is mostly mild in animals whereas severe disease can be seen in humans [34]. Nevertheless, SARS-CoV-2 can replicate rapidly in the upper airways of macaques and humans. That is why it can be assumed that the results on the nasal clearance of SARS-CoV-2 in macaques may indicate a similar reaction in the human upper airways. Another limitation is that the SARS-CoV-2 challenge was within a few weeks of the final or only vaccine dose. This is regarded as the time when the immune response is likely to be close to its peak. It is therefore unknown if the viral clearance in the upper respiratory tract would be as effective against challenges conducted many months after the immunization protocol has been completed [35]. It is likely that the immune response will gradually ease off so that the viral clearance in the upper respiratory tract might take longer or might be less effective. In this case vaccinated animals could possibly spread a higher viral load or could spread it for a longer period of time. The pattern may be similar in humans. A third limitation of the animal studies is that the viral challenge was often high and, in some studies, administered by up to four routes. As a general principle, it will be easier to protect against a low dose of a challenge virus than a higher one, all other things being equal.
The findings in the phase III trial with AZD1222 are supported by data obtained with macaques showing that the level of genomic and subgenomic RNA was similar in the upper respiratory tract of vaccinated and control animals. Only the load of infectious virus was partly reduced in AZD1222-vaccinated animals. Other vaccines reveal a faster and stronger clearance of SARS-CoV-2 RNA in the upper respiratory tract, some vaccines may even stop viral replication in the upper respiratory tract as suggested by a lack of subgenomic RNA. With this variety of results in mind it is clear that a sterilizing immunity cannot be achieved in all vaccinated individuals.
Vaccinated individuals can therefore not be ruled out as a possible source for SARS-CoV-2 transmission. In case of a COVID-19 infection in vaccinated individuals they will probably have a mild disease, maybe they remain asymptomatic. Based on these data it is possible that privileges for them may have an opposite effect because it seems to be more likely that they can be an asymptomatic viral spreader. Such a case has been reported recently in Halle, Germany [36]. Even when differentiating between the vaccinated and non-vaccinated is legal, it can still be unfair. Certifying those who are fit or vaccinated may stigmatize those who are not. There is ample historical evidence that tying advantage to fitness can amplify existing socioeconomic disparities. At the extreme, critics warn that excessive immunity advantages or vaccination certificates could create an Orwellian or dystopian social apartheid [37].
The assumption that vaccinated individuals cannot be a possible source of infection is not supported by current evidence. This finding may also have implications for healthcare workers and nursing staff in residential and nursing homes when the expectation towards a vaccination is to prevent them to be a possible source of transmission to patients or residents. If COVID-19 vaccines do not prevent transmission it also does not make sense to preferably return fundamental rights to vaccinated individuals. The focus of vaccination should be the individual protection against hospitalization, ICU, and death.
5. Conclusions
Based on current knowledge it seems clear that COVID-19 vaccinated individuals can still be the source of SARS-CoV-2 transmission. If COVID-19 vaccines do not prevent transmission it also does not make sense to preferably return fundamental rights to vaccinated individuals. The focus of vaccination should be the individual protection against hospitalization, ICU, and death.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
G.K. has received personal fees from Dr. Schumacher GmbH, Germany, for presentation and consultation.
References
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef] [PubMed]
- WHO. Covid-19 Advice for the Public: Getting Vaccinated (8 April 2021). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice (accessed on 7 May 2021).
- Anonymous. Lambrecht: Geimpften Grundrechte Zurückgeben (22 January 2021). Available online: https://www.zdf.de/nachrichten/politik/corona-lambrecht-einschraenkungen-geimpfte-aufheben-100.html (accessed on 23 January 2021).
- Anonymous. Spahn für Mehr Freiheiten für Geimpfte Beim Reisen und Einkaufen (4 April 2021). Available online: https://www.aerzteblatt.de/nachrichten/122648/Spahn-fuer-mehr-Freiheiten-fuer-Geimpfte-beim-Reisen-und-Einkaufen (accessed on 6 April 2021).
- Dodd, R.H.; Pickles, K.; Nickel, B.; Cvejic, E.; Ayre, J.; Batcup, C.; Bonner, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Concerns and motivations about COVID-19 vaccination. Lancet Infect. Dis. 2021, 21, 161–163. [Google Scholar] [CrossRef]
- Costantino, C.; Mazzucco, W.; Azzolini, E.; Baldini, C.; Bergomi, M.; Biafiore, A.D.; Bianco, M.; Borsari, L.; Cacciari, P.; Cadeddu, C.; et al. Influenza vaccination coverage among medical residents: An Italian multicenter survey. Hum. Vaccines Immunother. 2014, 10, 1204–1210. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.L.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.; Lutrick, K.; et al. Interim Estimates of Vaccine Effectiveness of BNT162b2 and mRNA-1273 COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Health Care Personnel, First Responders, and Other Essential and Frontline Workers—Eight U.S. Locations, December 2020-March 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 495–500. [Google Scholar] [CrossRef]
- Singh, D.K.; Singh, B.; Ganatra, S.R.; Gazi, M.; Cole, J.; Thippeshappa, R.; Alfson, K.J.; Clemmons, E.; Gonzalez, O.; Escobedo, R.; et al. Responses to acute infection with SARS-CoV-2 in the lungs of rhesus macaques, baboons and marmosets. Nat. Microbiol. 2021, 6, 73–86. [Google Scholar] [CrossRef]
- Yu, P.; Qi, F.; Xu, Y.; Li, F.; Liu, P.; Liu, J.; Bao, L.; Deng, W.; Gao, H.; Xiang, Z.; et al. Age-related rhesus macaque models of COVID-19. Anim. Models Exp. Med. 2020, 3, 93–97. [Google Scholar] [CrossRef] [Green Version]
- Shan, C.; Yao, Y.F.; Yang, X.L.; Zhou, Y.W.; Gao, G.; Peng, Y.; Yang, L.; Hu, X.; Xiong, J.; Jiang, R.D.; et al. Infection with novel coronavirus (SARS-CoV-2) causes pneumonia in Rhesus macaques. Cell Res. 2020, 30, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Li, H.; Guo, L.; Liang, Y.; Li, J.; Wang, X.; Hu, Y.; Wang, L.; Liao, Y.; Yang, F.; et al. Virulence and pathogenesis of SARS-CoV-2 infection in rhesus macaques: A nonhuman primate model of COVID-19 progression. PLoS Pathog. 2020, 16, e1008949. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Lambe, T.; Spencer, A.; Belij-Rammerstorfer, S.; Purushotham, J.N.; Port, J.R.; Avanzato, V.A.; Bushmaker, T.; Flaxman, A.; Ulaszewska, M.; et al. ChAdOx1 nCoV-19 vaccine prevents SARS-CoV-2 pneumonia in rhesus macaques. Nature 2020, 586, 578–582. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Purushotham, J.; Schulz, J.; Holbrook, M.; Bushmaker, T.; Carmody, A.; Port, J.; Yinda, K.C.; Okumura, A.; Saturday, G.; et al. Intranasal ChAdOx1 nCoV-19/AZD1222 vaccination reduces shedding of SARS-CoV-2 D614G in rhesus macaques. bioRxiv 2021. [Google Scholar] [CrossRef]
- Vogel, A.B.; Kanevsky, I.; Che, Y.; Swanson, K.A.; Muik, A.; Vormehr, M.; Kranz, L.M.; Walzer, K.C.; Hein, S.; Güler, A.; et al. BNT162b vaccines protect rhesus macaques from SARS-CoV-2. Nature 2021. [Google Scholar] [CrossRef]
- Brouwer, P.J.M.; Brinkkemper, M.; Maisonnasse, P.; Dereuddre-Bosquet, N.; Grobben, M.; Claireaux, M.; de Gast, M.; Marlin, R.; Chesnais, V.; Diry, S.; et al. Two-component spike nanoparticle vaccine protects macaques from SARS-CoV-2 infection. Cell 2021, 184, 1188–1200. [Google Scholar] [CrossRef]
- Yadav, P.D.; Ella, R.; Kumar, S.; Patil, D.R.; Mohandas, S.; Shete, A.M.; Vadrevu, K.M.; Bhati, G.; Sapkal, G.; Kaushal, H.; et al. Immunogenicity and protective efficacy of inactivated SARS-CoV-2 vaccine candidate, BBV152 in rhesus macaques. Nat. Commun. 2021, 12, 1386. [Google Scholar] [CrossRef]
- Yu, J.; Tostanoski, L.H.; Peter, L.; Mercado, N.B.; McMahan, K.; Mahrokhian, S.H.; Nkolola, J.P.; Liu, J.; Li, Z.; Chandrashekar, A.; et al. DNA vaccine protection against SARS-CoV-2 in rhesus macaques. Science 2020, 369, 806–811. [Google Scholar] [CrossRef]
- Yang, J.; Wang, W.; Chen, Z.; Lu, S.; Yang, F.; Bi, Z.; Bao, L.; Mo, F.; Li, X.; Huang, Y.; et al. A vaccine targeting the RBD of the S protein of SARS-CoV-2 induces protective immunity. Nature 2020, 586, 572–577. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, Y.; Huang, B.; Deng, W.; Quan, Y.; Wang, W.; Xu, W.; Zhao, Y.; Li, N.; Zhang, J.; et al. Development of an Inactivated Vaccine Candidate, BBIBP-CorV, with Potent Protection against SARS-CoV-2. Cell 2020, 182, 713–721. [Google Scholar] [CrossRef]
- Sanchez-Felipe, L.; Vercruysse, T.; Sharma, S.; Ma, J.; Lemmens, V.; Van Looveren, D.; Arkalagud Javarappa, M.P.; Boudewijns, R.; Malengier-Devlies, B.; Liesenborghs, L.; et al. A single-dose live-attenuated YF17D-vectored SARS-CoV-2 vaccine candidate. Nature 2021, 590, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.O.; Feldmann, F.; Zhao, H.; Curiel, D.T.; Okumura, A.; Tang-Huau, T.L.; Case, J.B.; Meade-White, K.; Callison, J.; Chen, R.E.; et al. A single intranasal dose of chimpanzee adenovirus-vectored vaccine protects against SARS-CoV-2 infection in rhesus macaques. Cell Rep. Med. 2021, 100230. [Google Scholar] [CrossRef] [PubMed]
- Dagotto, G.; Mercado, N.B.; Martinez, D.R.; Hou, Y.J.; Nkolola, J.P.; Carnahan, R.H.; Crowe, J.E., Jr.; Baric, R.S.; Barouch, D.H. Comparison of Subgenomic and Total RNA in SARS-CoV-2 Challenged Rhesus Macaques. J. Virol. 2021, 95, 8. [Google Scholar] [CrossRef]
- Mercado, N.B.; Zahn, R.; Wegmann, F.; Loos, C.; Chandrashekar, A.; Yu, J.; Liu, J.; Peter, L.; McMahan, K.; Tostanoski, L.H.; et al. Single-shot Ad26 vaccine protects against SARS-CoV-2 in rhesus macaques. Nature 2020, 586, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Corbett, K.S.; Flynn, B.; Foulds, K.E.; Francica, J.R.; Boyoglu-Barnum, S.; Werner, A.P.; Flach, B.; O’Connell, S.; Bock, K.W.; Minai, M.; et al. Evaluation of the mRNA-1273 Vaccine against SARS-CoV-2 in Nonhuman Primates. N. Engl. J. Med. 2020, 383, 1544–1555. [Google Scholar] [CrossRef]
- Feng, L.; Wang, Q.; Shan, C.; Yang, C.; Feng, Y.; Wu, J.; Liu, X.; Zhou, Y.; Jiang, R.; Hu, P.; et al. An adenovirus-vectored COVID-19 vaccine confers protection from SARS-COV-2 challenge in rhesus macaques. Nat. Commun. 2020, 11, 4207. [Google Scholar] [CrossRef]
- He, X.; Chandrashekar, A.; Zahn, R.; Wegmann, F.; Yu, J.; Mercado, N.B.; McMahan, K.; Martinot, A.J.; Piedra-Mora, C.; Beecy, S.; et al. Low-Dose Ad26.COV2.S Protection Against SARS-CoV-2 Challenge in Rhesus Macaques. bioRxiv 2021. [Google Scholar] [CrossRef]
- Routhu, N.K.; Cheedarla, N.; Gangadhara, S.; Bollimpelli, V.S.; Boddapati, A.K.; Shiferaw, A.; Rahman, S.A.; Sahoo, A.; Edara, V.V.; Lai, L.; et al. A modified vaccinia Ankara vector-based vaccine protects macaques from SARS-CoV-2 infection, immune pathology, and dysfunction in the lungs. Immunity 2021, 54, 542–556. [Google Scholar] [CrossRef]
- Guebre-Xabier, M.; Patel, N.; Tian, J.H.; Zhou, B.; Maciejewski, S.; Lam, K.; Portnoff, A.D.; Massare, M.J.; Frieman, M.B.; Piedra, P.A.; et al. NVX-CoV2373 vaccine protects cynomolgus macaque upper and lower airways against SARS-CoV-2 challenge. Vaccine 2020, 38, 7892–7896. [Google Scholar] [CrossRef]
- Chandrashekar, A.; Liu, J.; Martinot, A.J.; McMahan, K.; Mercado, N.B.; Peter, L.; Tostanoski, L.H.; Yu, J.; Maliga, Z.; Nekorchuk, M.; et al. SARS-CoV-2 infection protects against rechallenge in rhesus macaques. Science 2020, 369, 812–817. [Google Scholar] [CrossRef]
- Ehaideb, S.N.; Abdullah, M.L.; Abuyassin, B.; Bouchama, A. Evidence of a wide gap between COVID-19 in humans and animal models: A systematic review. Crit. Care 2020, 24, 594. [Google Scholar] [CrossRef] [PubMed]
- Klasse, P.J.; Nixon, D.F.; Moore, J.P. Immunogenicity of clinically relevant SARS-CoV-2 vaccines in nonhuman primates and humans. Sci. Adv. 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. Geimpfter Soll Mehrere Personen in Klinik Angesteckt Haben (2 April 2021). Available online: https://www.rtl.de/cms/corona-alarm-in-halle-geimpfter-soll-unwissentlich-mehrere-personen-angesteckt-haben-4732838.html (accessed on 6 April 2021).
- Hall, M.A.; Studdert, D.M. Privileges and Immunity Certification during the COVID-19 Pandemic. JAMA 2020, 323, 2243–2244. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram on study selection, exclusion and inclusion.

{kind=link}
Table 1.
Number of symptomatic COVID-19 cases (subjects with at least one symptom indicative of COVID-19 and a positive PCR test for detection of SARS-CoV-2 RNA) in phase 3 vaccination trials.
Table 1.
Number of symptomatic COVID-19 cases (subjects with at least one symptom indicative of COVID-19 and a positive PCR test for detection of SARS-CoV-2 RNA) in phase 3 vaccination trials.
| Vaccine (Manufacturer) | Symptomatic COVID-19 Cases * Among | Reference | |
|---|---|---|---|
| Vaccinated Subjects | Control Subjects | ||
| AZD1222 (AstraZeneca) | 74 of 7.201 (1.0%) | 197 of 7.178 (2.7%) | [7] |
| mRNA 1273 (Moderna) | 11 of 15.210 (0.07%) | 185 of 15.210 (1.2%) | [8] |
| BNT162b2 (BioNTech) | 8 of 18.198 (0.04%) | 162 of 18.325 (0.9%) | [9] |
| Sputnik V (Gamaleya) | 16 of 14.964 (0.1%) | 62 of 4.902 (1.3%) | [10] |
* The symptoms depend on the study: at least one of the following symptoms: fever ≥ 37.8 °C, cough, shortness of breath, anosmia or ageusia [7]; at least two of the following symptoms: fever (temperature ≥ 38 °C), chills, myalgia, headache, sore throat, or new olfactory or taste disorder, or as occurring in those who had at least one respiratory sign or symptom (including cough, shortness of breath, or clinical or radiographic evidence of pneumonia) [8]; at least one of the following symptoms: fever, new or increased cough, new or increased shortness of breath, chills, new or increased muscle pain, new loss of taste or smell, sore throat, diarrhea, or vomiting [9]; any clinical signs of a respiratory tract infection [10].
Table 2.
Effect of COVID-19 vaccines and vaccine candidates on genomic RNA load (nose or throat) after a SARS-CoV-2 challenge in vaccinated and non-vaccinated macaques.
Table 2.
Effect of COVID-19 vaccines and vaccine candidates on genomic RNA load (nose or throat) after a SARS-CoV-2 challenge in vaccinated and non-vaccinated macaques.
| Vaccine (Manufacturer) | Animals | Timing of SARS-CoV-2 Challenge | Nasal SARS-CoV-2 Challenge | SARS-CoV-2 Challenge in Other Organs | Effect in Control Animals | Effect in Vaccinated Animals | Reference |
|---|---|---|---|---|---|---|---|
| AZD1222 (AstraZeneca) | 6 per group | 2 weeks after the second intramuscular vaccination with 2.5 × 1010 ChAdOx1 nCoV-19 on days 0 and 28 *** | 4 × 105 * | Intratracheal: 1.6 × 106 * Oral: 4 × 105 * Ocular: 2 × 105 * | Approx. 106 cpm on day 1, between 102 and 104 cpm on day 7 | Approx. 105 to 107 cpm on day 1, between 102 and 105 cpm on day 7; no significant difference to control group | [16] |
| AZD1222 (AstraZeneca) | 4 per group | 56 days after the intranasal vaccination with 2.5 × 1010 ChAdOx1 nCoV-19 on day 0 | 2 × 105 * | Intratracheal: 8 × 105 * | Between 103 and 108 cpm on day 3, between 103 and 104 cpm on day 7 | Between 103 and 106 cpm on day 3, below limit of detection (103) on day 7; no significant difference to control group | [17] |
| BNT162b2 (BioNTech Pfizer) | 9 (control group) and 6 (vaccine group) | 55 days after the second intramuscular vaccination with 100 µg on days 0 and 21 **** | 6.3 × 105 ** | Intratracheal: 6.3 × 105 ** | Between 103 and 105 viral RNA copies on days 1, 3 and 6 | Between 103 and 106 viral RNA copies on day 1, below limit of detection (103) on days 3 and 6 (no comparative statistics) | [18] |
| SARSCoV-2 S-I53-50NP (not described) | 4 or 6 per group | 2 weeks after the third vaccination with 50 µg on days 0, 28 and 70 | 105 ** | Intratracheal: 5.9 × 105 ** | Approx. 108 cpm on day 2, mostly none detected after day 8 | Approx. 105 cpm on day 2, none detected after day 3 | [19] |
| BBV152 (Bharat Biotech) | 5 per group | 4 weeks after the second intramuscular vaccination with 3 µg vaccine and adjuvant-B on days 0 and 14 | 106 * | Intratracheal: 106.5 * | Approx. 107 cpm on days 1 and 3, between 104 and 105 cpm on days 5 and 7 | Approx. 105 cpm on day 1, no RNA detected on days 3, 5 and 7 | [20] |
| Six different DNA vaccines (Janssen) | 4 or 5 per group | 3 weeks after the second intramuscular vaccination with a vaccine on days 0 and 21 | 1.1 × 104 ** | Intratracheal: 1.1 × 104 ** | Approx. 107 cps on day 2, slowly going down to 102 cps on day 14 | Between 103 and 108 cps on day 2, mostly going down to less than 102 cps on day 10 | [21] |
| RBD ***** (not described) | 3 or 4 per group | 3 weeks after the second intramuscular vaccination with 20 or 40 µg on days 0 and 7 | 5 × 105 ** | None | Between 104 and 106 cpm on days 2–6 | Between 1 and 106 cpm on days 2–6 | [22] |
| BBIBP-CorV *** (not described) | 2 or 4 per group | 10 days after the second intramuscular vaccination with 2 or 8 µg on days 0 and 14 | None | Intratracheal: 106 * | Between 105 and 106 cpm on days 3, 5 and 7 | Approx. 103 cpm on day 3, between 102 and 105 on day 5, between 0 and 102 on day 7 | [23] |
| YF17D ****** (not described) | 6 per group | 21 days after the second subcutaneously vaccination with 105 PFU on days 0 and 7 | 7.5 × 103 * | Intratracheal: 7.5 × 103 * | Between 102 and 106 cpm on days 1–4 | Mostly < 102 cpm on days 1–4 | [24] |
| ChAd-SARS-CoV-2-S (not described) | 6 per group | 4 weeks after the intranasal vaccination with 1011 viral particles | 5.7 × 105 * | Intratracheal: 5.7 × 105 * | Between 103 and 104 cpm on day 1, slowly going down to 0 to 103 on day 7 | Between 102 and 103 cpm on day 1, slowly going down to 0 to 10 on day 7 | [25] |
* TCID50; ** PFU; *** the vaccine with temporary authorization (UK) contains 5 × 1010 viral particles; **** the vaccine with conditional marketing authorization (European Union), temporary authorization (UK) and emergency use authorization (USA) contains 30 µg BNT162b2; ***** receptor-binding protein; ****** live-attenuated yellow fever vaccine; cpm = copies per mL; cps = copies per swab.
Table 3.
Effect of COVID-19 vaccines and vaccine candidates on subgenomic RNA load (nose or throat) after a SARS-CoV-2 challenge in vaccinated and non-vaccinated macaques.
Table 3.
Effect of COVID-19 vaccines and vaccine candidates on subgenomic RNA load (nose or throat) after a SARS-CoV-2 challenge in vaccinated and non-vaccinated macaques.
| Vaccine (Manufacturer) | Animals | Timing of SARS-CoV-2 Challenge | Nasal SARS-CoV-2 Challenge (PFU) | SARS-CoV-2 Challenge in Other Organs (PFU) | Effect in Control Animals | Effect in Vaccinated Animals | Reference |
|---|---|---|---|---|---|---|---|
| AZD1222 (AstraZeneca) | 6 per group | 2 weeks after the second intramuscular vaccination with 2.5 × 1010 ChAdOx1 nCoV-19 on days 0 and 28 *** | 4 × 105 * | Intratracheal: 1.6 × 106 * Oral: 4 × 105 * Ocular: 2 × 105 * | Between 102 and 105 cpm on day 1, below limit of detection (102) on day 7 | Between 102 and 105 cpm on day 1, below limit of detection (102) on day 7; no significant difference to control group | [16] |
| AZD1222 (AstraZeneca) | 4 per group | 56 days after the intranasal vaccination with 2.5 × 1010 ChAdOx1 nCoV-19 on day 0 | 2 × 105 * | Intratracheal: 8 × 105 * | Between 102.5 and 104.5 cpm on day 1, between 102.5 and 103.5 cpm on day 5, below limit of detection (102.5) on day 7 | Between 102.5 and 103.5 cpm on day 5, below limit of detection (102.5) on days 1, 3 and 7; no significant difference to control group | [17] |
| SARSCoV-2 S-I53-50NP (not described) | 4 or 6 per group | 2 weeks after the third vaccination with on days 0, 28 and 70 | 105 ** | Intratracheal: 5.9 × 105 ** | Between 105 and 107 cpm on day 2, between 102 and 104 cpm on days 5 and 6 | No sgRNA detected on days 2, 5 and 6 | [19] |
| BBV152 (Bharat Biotech) | 5 per group | 4 weeks after the second intramuscular vaccination with 3 µg vaccine and adjuvant-B on days 0 and 14 | 106 * | Intratracheal: 106.5 * | Approx. 107 cpm on days 1, 3 and 7 | No sgRNA detected on days 1, 3, 5 and 7 | [20] |
| Six different DNA vaccines (Janssen) | 4 or 5 per group | 3 weeks after the second intramuscular vaccination with a vaccine on days 0 and 21 | 1.1 × 104 ** | Intratracheal: 1.1 × 104 ** | Between 105 and 107 cps on days 1 to 4, slowly going down to 102 cps on day 14 | Between 102 and 105 cps on day 2, mostly going down to less than 102 cps on day 7 | [21] |
| Variant S.PP (Janssen) | 20 (control group) and 6 (vaccine group) | 6 weeks after the intramuscular vaccination with 1011 viral particles on day 0 | 5.5 × 103 ** | Intratracheal: 5.5 × 103 ** | Between 104 and 108 viral copies on day 2, between 101.5 and 105 on day 10 | Between 101.5 and 103.5 viral copies on day 1, below limit of detection on days 4 to 10 | [27] |
| mRNA-1273 (Moderna) | 8 per group | 4 weeks after the second intramuscular vaccination with 100 µg on days 0 and 28 **** | 1.9 × 105 ** | Intratracheal: 5.7 × 105 ** | Between 101.5 and 105.5 cpm on days 1 and 2, between 101.5 and 104.5 cpm on day 4, below limit of detection (101.5) on day 7 | Between 101.5 and 104.5 cpm on day 1, below limit of detection (101.5) on days 2, 4 and 7 (one animal with 102.5 cpm on day 4); peak levels on days 2–7: p = 0.009 | [28] |
| RBD (not described) | 3 or 4 per group | 3 weeks after the second intramuscular vaccination with 20 or 40 µg on days 0 and 7 | 5 × 105 ** | None | Between 103 and 105 cpm on days 2–6 | No sgRNA detected on days 2–6 | [22] |
| Vaccine Ad5-S-nb2 (Guangzhou nBiomed) | 2 or 4 per group | 30 days after an intramuscular vaccination (high dose or low dose) or an intranasal and oral application of the vaccine | None | Intratracheal: 2 × 104 or 400 * | Between 102 and 106 cpm on days 1–10 | Mostly less than 102 cpm on days 1–10, one peak of 104 cpm on day 6 (intranasal and oral application) | [29] |
| VX-CoV2327 vaccine (Novavax) | 4 per group | After the second intramuscular vaccination with 2.5, 5 or 25 µg on days 0 and 21 | 5.5 × 103 ** | Intratracheal: 5.5 × 103 ** | Between 10 and 104 cpm on days 2 and 4 | None detected | [32] |
| Ad26.COV2.S (Janssen) | 5 or 10 per group | 6 weeks after an intramuscular vaccination with 1 × 1011, 5 × 1010, 1.125 × 1010 or 2 × 109 viral particles on day 0 | 1.1 × 104 ** | Intratracheal: 1.1 × 104 ** | Peak values between 104 and 107 cps | Highest dose: none detected Middle doses: mostly none detected Lowest dose: mostly between 105 and 107 cps | [30] |
| MVA-based COVID-19 vaccine (not described) | 5 per group | 4 weeks after the second intramuscular vaccination with 108 PFU on weeks 0 and 4 | 2.5 × 104 ** | Intratracheal: 2.5 × 104 ** | Between 10 and 107 cpm on days 2, 4 and 7, none on day 10 | Between 10 and 105 cpm on days 2, 4 and 7, none on day 10 | [31] |
| ChAd-SARS-CoV-2-S (not described) | 6 per group | 4 weeks after the intranasal vaccination with 1011 viral particles | 5.7 × 105 * | Intratracheal: 5.7 × 105 * | Between 105 and 107 cpm on days 1–7 | Between 103 and 108 cpm on days 1–7 | [25] |
* TCID50; ** PFU; *** the vaccine with temporary authorization (UK) contains 5 × 1010 viral particles; **** equivalent to conditional marketing authorization (European Union), temporary authorization (UK) and emergency use authorization (USA); cpm = copies per mL; cps = copies per swab.
Table 4.
Effect of COVID-19 vaccines and vaccine candidates on the load of infectious SARS-CoV-2 (nose or throat) after a SARS-CoV-2 challenge in vaccinated and non-vaccinated macaques.
Table 4.
Effect of COVID-19 vaccines and vaccine candidates on the load of infectious SARS-CoV-2 (nose or throat) after a SARS-CoV-2 challenge in vaccinated and non-vaccinated macaques.
| Vaccine (Manufacturer) | Animals | Timing of SARS-CoV-2 Challenge | Nasal SARS-CoV-2 Challenge (PFU) | SARS-CoV-2 Challenge in Other Organs (PFU) | Effect in Control Animals | Effect in Vaccinated Animals | Reference |
|---|---|---|---|---|---|---|---|
| AZD1222 (AstraZeneca) | 6 per group | 2 weeks after the second intramuscular vaccination with 2.5 × 1010 ChAdOx1 nCoV-19 on days 0 and 28 * | 4 × 105 | Intratracheal: 1.6 × 106 Oral: 4 × 105 Ocular: 2 × 105 | Detected in 4 animals on day 1, in 1 animal on day 3, and in 0 animals on days 5 and 7 | Detected in 2 animals on day 1 and in 0 animals on days 3, 5 and 7 (no comparative statistics) | [16] |
| AZD1222 (AstraZeneca) | 4 per group | 56 days after the intranasal vaccination with 2.5 × 1010 ChAdOx1 nCoV-19 on day 0 | 2 × 105 | Intratracheal: 8 × 105 | 10 and 106 on day 1 | 10–150 on day 1 (p < 0.05) | [17] |
| Variant S.PP (Janssen) | 20 (control group) and 6 (vaccine group) | 6 weeks after the intramuscular vaccination with 1011 viral particles on day 0 | 5.5 × 103 | Intratracheal: 5.5 × 103 | Infectious virus on day 2 between 10 and 1000 PFU per swab | No infectious virus on day 2 | [27] |
| ChAd-SARS-CoV-2-S (not described) | 6 per group | 4 weeks after the intranasal vaccination with 1011 viral particles | 5.7 × 105 | Intratracheal: 5.7 × 105 | 4 animals with infectious virus on day 1 | 1 animal with infectious virus on day 1 | [25] |
* the vaccine with temporary authorization (UK) contains 5 × 1010 viral particles.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kampf, G. COVID-19 Vaccinated Individuals Can Be a Source of SARS-CoV-2 Transmission—A Systematic Review. Hygiene 2021, 1, 1-11. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene1010001
AMA Style
Kampf G. COVID-19 Vaccinated Individuals Can Be a Source of SARS-CoV-2 Transmission—A Systematic Review. Hygiene. 2021; 1(1):1-11. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene1010001
Chicago/Turabian StyleKampf, Günter. 2021. "COVID-19 Vaccinated Individuals Can Be a Source of SARS-CoV-2 Transmission—A Systematic Review" Hygiene 1, no. 1: 1-11. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene1010001