
Lung Diffusing Capacity in Dutch Special Operations Forces Divers Exposed to Oxygen Rebreathers over 18 Years

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
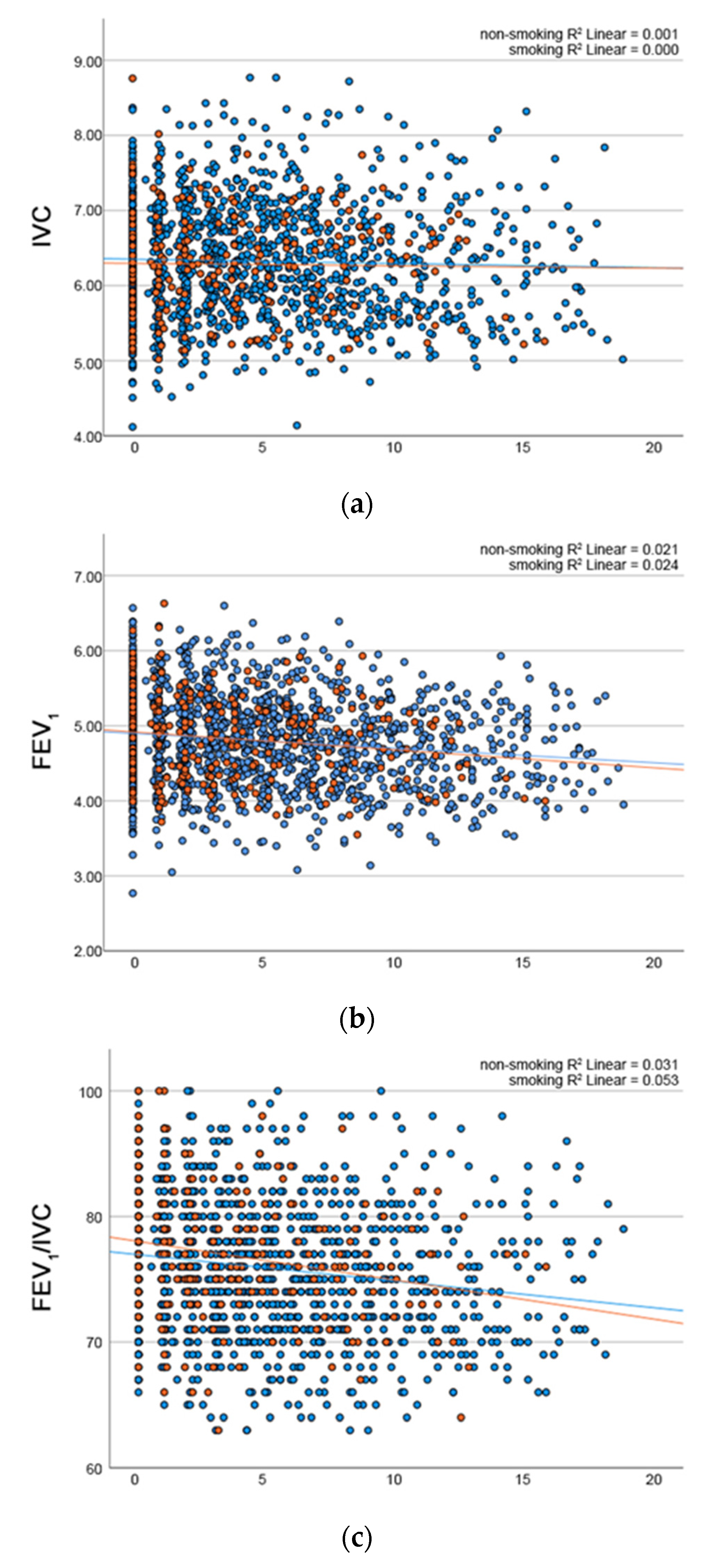
3.1. Pulmonary Function Tests
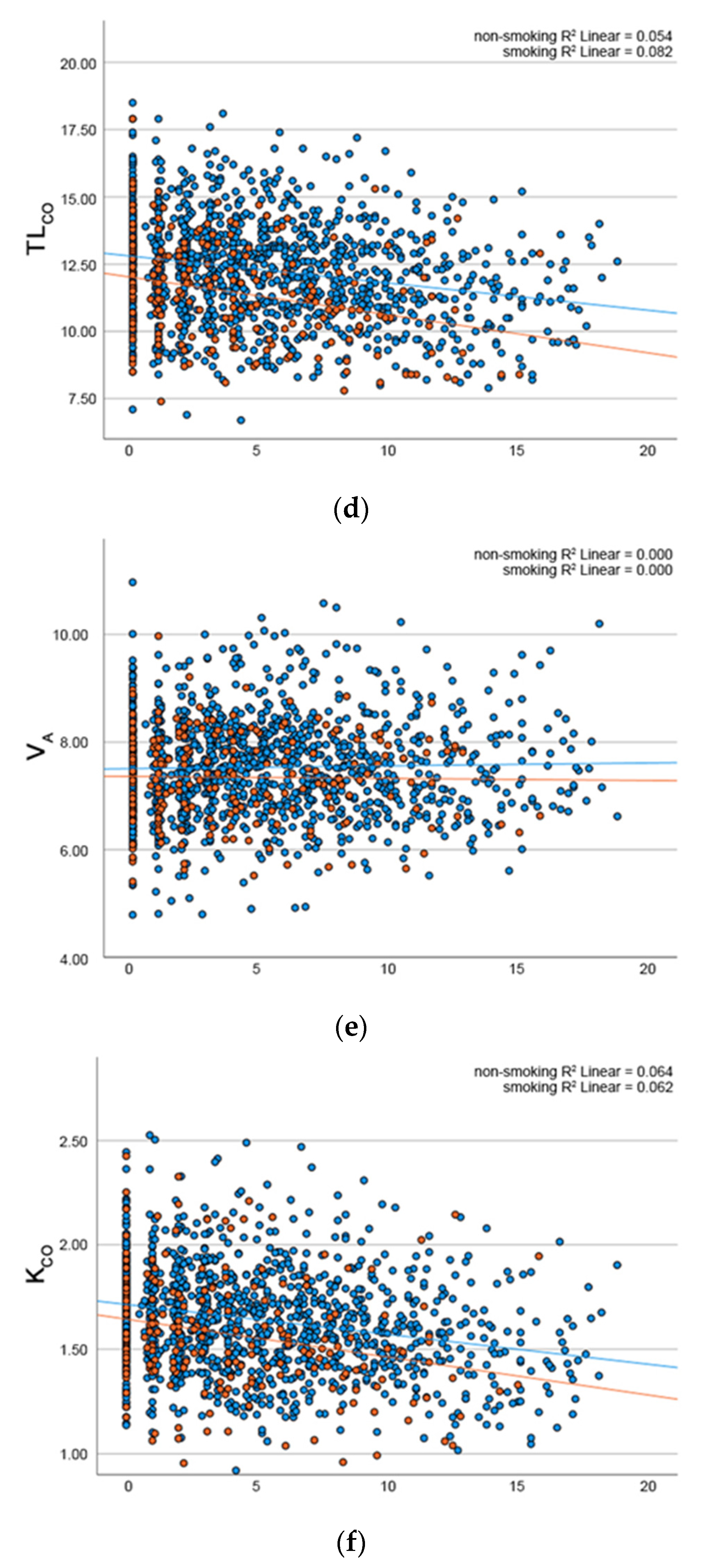
3.2. Diffusing Capacity
4. Discussion
Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bosco, G.; Rizzato, A.; Moon, R.E.; Camporesi, E.M. Environmental Physiology and Diving Medicine. Front. Psychol. 2018, 9, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wingelaar, T.T.; van Ooij, P.A.M.; van Hulst, R.A. Oxygen Toxicity and Special Operations Forces Diving: Hidden and Dangerous. Front. Psychol. 2017, 8, 1263. [Google Scholar] [CrossRef] [PubMed]
- Klein, J. Normobaric pulmonary oxygen toxicity. Anesth. Analg. 1990, 70, 195–207. [Google Scholar] [CrossRef]
- Van Ooij, P.A.; Sterk, P.J.; van Hulst, R.A. Oxygen, the lung and the diver: Friends and foes? Eur. Respir. Rev. 2016, 25, 496–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, J.M.; Lambertsen, C.J. Pulmonary Oxygen Tolerance in Man and Derivation of Pulmonary Oxygen Tolerance Curves; University of Pennsylvania Medical Center: Philadelphia, PA, USA, 1970. [Google Scholar]
- Wingelaar, T.T. Detecting Pulmonary Oxygen Toxicity Using Exhaled Breath Markers; University of Amsterdam: Amsterdam, The Netherlands, 2020; Available online: https://pure.uva.nl/ws/files/44848921/Thesis_complete_pdf (accessed on 28 February 2022).
- Voortman, M.; Ooij, P.; Hulst, R.A.V.; Zanen, P. Pulmonary function changes in Navy divers during their professional careers. Undersea Hyperb. Med. 2016, 43, 649–657. [Google Scholar] [PubMed]
- Sames, C.; Gorman, D.F.; Mitchell, S.J.; Zhou, L. Long-term changes in spirometry in occupational divers: A 10–25 year audit. Diving Hyperb. Med. 2018, 48, 10–16. [Google Scholar] [CrossRef]
- Stanojevic, S.; Graham, B.L.; Cooper, B.G.; Thompson, B.R.; Carter, K.W.; Francis, R.W.; Hall, G. Official ERS technical standards: Global Lung Function Initiative reference values for the carbon monoxide transfer factor for Caucasians. Eur. Respir. J. 2017, 50, 1700010. [Google Scholar] [CrossRef]
- Van Ooij, P.J.; van Hulst, R.A.; Houtkooper, A.; Sterk, P.J. Differences in spirometry and diffusing capacity after a 3-h wet or dry oxygen dive with a PO(2) of 150 kPa. Clin. Physiol. Funct. Imaging 2011, 31, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Challenor, J. Medical Assessment of Working Divers. In Fitness to Dive Standards of European Diving Technology Committee; Wendling, J., Elliott, D., Nome, T., Eds.; European Diving Technology Committee: Kiel, France, 2004. ISBN 3-952284-2-7. Occup. Med. 2005, 55, 581. [Google Scholar] [CrossRef] [Green Version]
- Wingelaar, T.T.; Clarijs, P.; van Ooij, P.A.; Koch, D.A.; van Hulst, R.A. Modern assessment of pulmonary function in divers cannot rely on old reference values. Diving Hyperb. Med. 2018, 48, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49, 1600016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, D.T.; Conkin, J. Improved pulmonary function in working divers breathing nitrox at shallow depths. Aviat. Space Environ. Med. 2003, 74, 763–767. [Google Scholar] [PubMed]
- Clanton, T.L.; Dixon, G.F.; Drake, J.; Gadek, J.E. Effects of swim training on lung volumes and inspiratory muscle conditioning. J. Appl. Physiol. 1987, 62, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Eur. Respir. J. 1993, 6 (Suppl. S16), 5–40. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-Smoking (n = 208) | Smoking (n = 49) | p | |
|---|---|---|---|
| Age (years) | 27.0 (IQR 24.0–32.0) | 28.0 (IQR 23.0–30.0) | 0.575 |
| Height (cm) | 183 (SD 6.2) | 183 (SD 6.4) | 0.854 |
| IVC (L) | 6.31 (SD 0.79) Z 0.64 | 6.29 (SD 0.73) Z 0.18 | 0.868 |
| FEV1 (L) | 4.87 (SD 0.65) Z 0.09 | 4.92 (SD 0.58) Z 0.61 | 0.610 |
| FEV1/IVC | 0.77 (SD 0.53) Z −0.87 | 0.78 (SD 0.50) Z −0.71 | 0.117 |
| TLCO (mmol/min/kPa) | 12.88 (SD 2.19) Z 0.69 | 11.83 (SD 2.49) Z 0.05 | 0.004 * |
| VA (L) | 7.32 (SD 1.33) Z 0.28 | 6.70 (SD 1.90) Z −0.50 | 0.007 * |
| KCO (mmol/min/kPa/L) | 1.90 (SD 1.08) Z 1.11 | 2.21 (SD 1.74) Z 2.49 | 0.118 |
| Hb (mmol/L) | 9.29 (SD 0.78) | 9.56 (SD 0.66) | 0.025 * |
| IVC | p | FEV1 | p | FEV1/ IVC | p | TLCO | p | VA | p | KCO | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept | 6.337 | 0.000 * | 5.621 | 0.000 * | 81.286 | 0.000 * | 13.185 | 0.000 * | 7.273 | 0.000 * | 1.817 | 0.000 * |
| Dive years | 0.014 | 0.204 | 0.006 | 0.390 | −0.055 | 0.443 | −0.058 | 0.016 * | 0.002 | 0.890 | −0.008 | 0.010 * |
| Age | −0.024 | 0.002 * | −0.026 | 0.000 * | −0.138 | 0.006 * | −0.048 | 0.001 * | 0.002 | 0.815 | −0.007 | 0.001 * |
| Non-smoking | 0.070 | 0.446 | 0.027 | 0.708 | −0.388 | 0.539 | 1.019 | 0.000 * | 0.181 | 0.088 | 0.095 | 0.010 * |
| Value | Z-Score | |
|---|---|---|
| IVC (L) | 6.35 (SD 0.82) | 1.308 (baseline 0.64) |
| FEV1 (L) | 4.77 (SD 0.56) | 0.921 (baseline 0.09) |
| FEV1/IVC | 75.7 (SD 5.4) | −0.68 (baseline −0.87) |
| TLCO (mmol/min/kPa) | 11.57 (SD 0.72) | 0.610 (baseline 0.69) |
| VA (L) | 7.66 (SD 1.14) | 0.671 (baseline 0.28) |
| KCO (mmol/min/kPa/L) | 1.51 (SD 0.23) | −0.031 (baseline 1.11) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
den Ouden, T.H.B.; Wingelaar, T.T.; Endert, E.L.; van Ooij, P.-J.A.M. Lung Diffusing Capacity in Dutch Special Operations Forces Divers Exposed to Oxygen Rebreathers over 18 Years. Oxygen 2022, 2, 40-47. https://0-doi-org.brum.beds.ac.uk/10.3390/oxygen2020005
den Ouden THB, Wingelaar TT, Endert EL, van Ooij P-JAM. Lung Diffusing Capacity in Dutch Special Operations Forces Divers Exposed to Oxygen Rebreathers over 18 Years. Oxygen. 2022; 2(2):40-47. https://0-doi-org.brum.beds.ac.uk/10.3390/oxygen2020005
Chicago/Turabian Styleden Ouden, Tom H.B., Thijs T. Wingelaar, Edwin L. Endert, and Pieter-Jan A.M. van Ooij. 2022. "Lung Diffusing Capacity in Dutch Special Operations Forces Divers Exposed to Oxygen Rebreathers over 18 Years" Oxygen 2, no. 2: 40-47. https://0-doi-org.brum.beds.ac.uk/10.3390/oxygen2020005