
Autologous Graft in the Anterior Maxilla—A Case Report †


Implantology Consultation, Egas Moniz Dental Clinic, 2829-511 Almada, Portugal
*
Author to whom correspondence should be addressed.
†
Presented at the 5th International Congress of CiiEM—Reducing Inequalities in Health and Society, Online, 16–18 June 2021.
Med. Sci. Forum 2021, 5(1), 36; https://0-doi-org.brum.beds.ac.uk/10.3390/msf2021005036
Published: 22 July 2021
(This article belongs to the Proceedings of The 5th International Congress of CiiEM (IC CiiEM))
{kind=link}
Abstract
:A 44-year-old male patient was referred to the Egas Moniz Dental Clinic, with a previous history of failed bone regeneration, resulting in a reduced buccal-palatal bone thickness and aesthetic compromise of the gingival margin of the anterior maxilla. Since the use of autologous bone is considered the “gold-standard” in guided bone regeneration, the treatment plan consisted of an autologous mental graft into the maxilla, with a simultaneous guided bone regeneration with a xenograft and absorbable membrane. This allowed a predictable volumetric bone regeneration with low patient morbidity and posterior fixed rehabilitation.
1. Introduction
Tooth extraction often leads to alveolar defects, which may present a difficult challenge to overcome, before the placement of implants, especially in the aesthetic zone. Depending on the size and location of the defect, different grafting materials can be used. Some materials, such as xenografts and allografts, and alloplastic materials of natural or synthetic origin, provide a scaffold, for new bone to grow. However, autogenous or autologous bone possesses osteoinductive, osteogenic, and osteoconductive properties, with a higher capacity of regeneration, when compared to other materials [1,2].
Various donor sites are available for autologous bone extraction. Regarding intraoral sites, the mandibular symphysis and the external oblique ridge of the mandible are the preferable donor sites, regarding both the quality and quantity of bone. Despite some potential complications described in the literature, as sensory alterations of the skin and mucosa, collection of bone from the symphysis provides thick and large grafts, suitable for vertical and horizontal augmentation [3,4].
Autologous bone is still considered the “gold standard” for bone augmentation, more importantly in cases of large and/or severe bone defects [2].
2. Materials and Methods
A 44-year-old male patient, without pathological and medicative references, and a regular smoker (about 10 cigarettes per day), was referred to the Egas Moniz Dental Clinic. Upon inspection, the patient presented a bone defect in the anterior maxilla on tooth #22, caused by a previous tooth extraction, and subsequent failed bone regeneration, which resulted in a reduced buccal-palatal bone thickness and aesthetic compromise of the gingival margin. Upon evaluation of the orthopantomography and CBCT scan, the treatment plan, which consisted of an autologous mental graft into the maxilla in conjunction with guided bone regeneration with a xenograft and absorbable membrane, was proposed to the patient and accepted.
3. Results and Discussion
After initial documentation, the first part of the surgery involved the exposure of the defect with a full thickness mucoperiosteal flap and measurement, facilitating the harvesting of bone.
Using the same method, the donor site was exposed, and an osteotomy was performed on the left mental region, to remove the bone block. Afterward, hemostasis was achieved, and the donor site was regenerated with collagen membrane and xenograft and sutured (Figure 1).
Lastly, the bone block was held in place in the recipient site with fixation screws. A xenograft material (NanoBone®) was used to fill the rest of the defect, and an absorbable collagen membrane (Evolution OsteoBiol®) was applied, covering the bone grafting materials. The recipient site was then sutured. A provisional crown was lastly adhered to the adjacent teeth.
Due to the multi-dimensional defect present, the use of an autologous bone block was crucial, both to stabilize the grafting materials, as well as to ensure the maximum regenerative ability both vertically and in buccal-palatal thickness, thus confirming, that the use of autologous bone in large bone defects remains one of the best options for bone augmentation procedures.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Danesh-Sani, S.; Engebretson, S.; Janal, M. Histomorphometric results of different grafting materials and effect of healing time on bone maturation after sinus floor augmentation: A systematic review and meta-analysis. J. Periodont Res. 2016, 52, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F.; Hanser, T. Mandibular Bone Block Harvesting from the Retromolar Region: A 10-Year Prospective Clinical Study. Int. J. Oral Maxillofac. Implants 2015, 30, 688–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reininger, D.; Cobo-Vazquez, C.; Monteserin-Matesanz, M.; Lopez-Quiles, J. Complications in the use of the mandibular body, ramus and symphysis as donor sites in bone graft surgery. A systematic review. Medicina Oral Patologia Oral y Cirugia Bucal. 2016, 21, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Pourabbas, R.; Nezafati, S. Clinical results of localized alveolar ridge augmentation with bone grafts harvested from symphysis in comparison with ramus. J. Dent. Res. Dent. Clin. Dent. Prospect. 2007, 1, 7–12. [Google Scholar] [CrossRef]
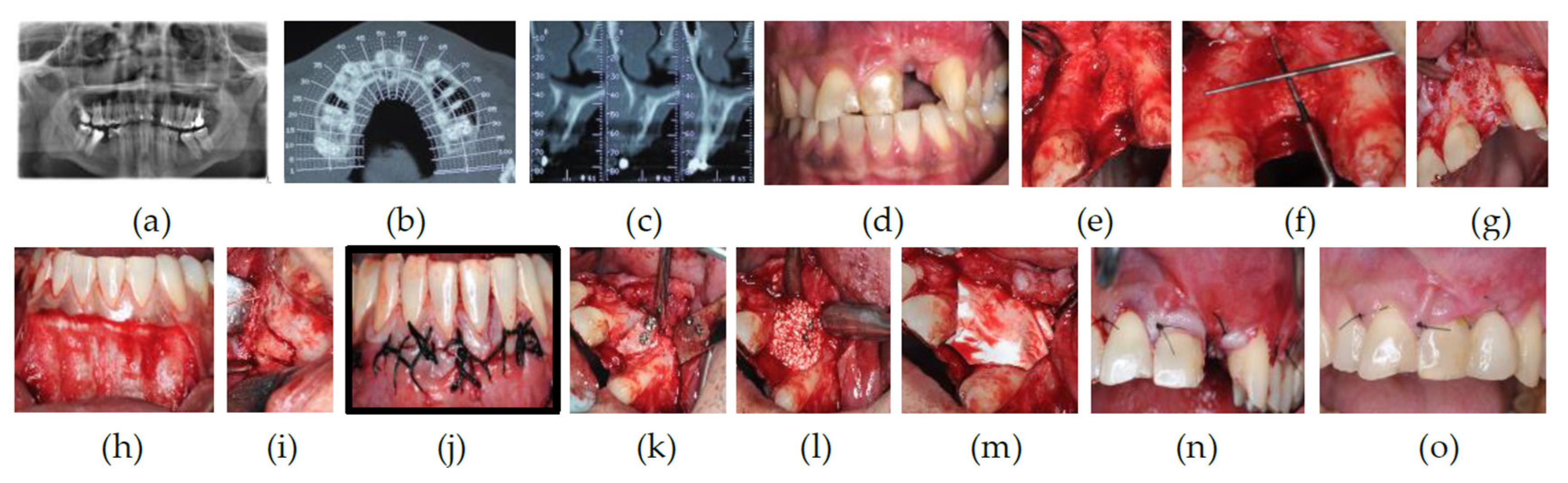
Figure 1.
Surgical stages: (a) Orthopantomography; (b) CBCT scan (axial plane); (c) CBCT scan (sagittal plane); (d) initial photograph; (e) exposure of the defect; (f) measurements; (g) cortical perforations; (h) exposure of the donor site; (i) osteotomy; (j) suture of the donor site; (k) fixation of the bone block; (l) xenograft application; (m) collagen membrane placement; (n) suture of the recipient site; (o) provisional crown (1-week post-op).
Figure 1.
Surgical stages: (a) Orthopantomography; (b) CBCT scan (axial plane); (c) CBCT scan (sagittal plane); (d) initial photograph; (e) exposure of the defect; (f) measurements; (g) cortical perforations; (h) exposure of the donor site; (i) osteotomy; (j) suture of the donor site; (k) fixation of the bone block; (l) xenograft application; (m) collagen membrane placement; (n) suture of the recipient site; (o) provisional crown (1-week post-op).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Vaz, R.; Gameiro, P.; Sottomayor, P.; Saldanha, B.; Rodrigues, P. Autologous Graft in the Anterior Maxilla—A Case Report. Med. Sci. Forum 2021, 5, 36. https://0-doi-org.brum.beds.ac.uk/10.3390/msf2021005036
AMA Style
Vaz R, Gameiro P, Sottomayor P, Saldanha B, Rodrigues P. Autologous Graft in the Anterior Maxilla—A Case Report. Medical Sciences Forum. 2021; 5(1):36. https://0-doi-org.brum.beds.ac.uk/10.3390/msf2021005036
Chicago/Turabian StyleVaz, Rodolfo, Pedro Gameiro, Pedro Sottomayor, Bernardo Saldanha, and Pedro Rodrigues. 2021. "Autologous Graft in the Anterior Maxilla—A Case Report" Medical Sciences Forum 5, no. 1: 36. https://0-doi-org.brum.beds.ac.uk/10.3390/msf2021005036