



Cancers 2023, 15(7), 1955; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15071955 - 24 Mar 2023
Cited by 1 | Viewed by 1811
Abstract
►
Show Figures
Background: This study aimed to summarize the surgical and therapeutic activities of non-functional pancreatic neuroendocrine tumors (NF-PanNETs) and perform survival analyses of a 15-year single-institutional cohort of NF-PanNETs. Methods: In total, 1001 patients with neuroendocrine neoplasms treated at Fudan University Shanghai Cancer Center
[...] Read more.
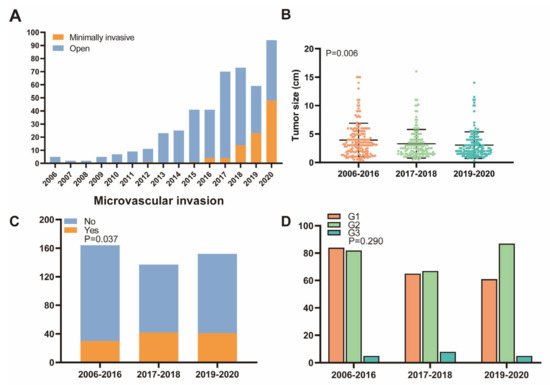
Background: This study aimed to summarize the surgical and therapeutic activities of non-functional pancreatic neuroendocrine tumors (NF-PanNETs) and perform survival analyses of a 15-year single-institutional cohort of NF-PanNETs. Methods: In total, 1001 patients with neuroendocrine neoplasms treated at Fudan University Shanghai Cancer Center were screened for inclusion, and 509 patients with NF-PanNETs from 2006 to 2020 were included. For time trend analyses, the 15-year study period was randomly divided into three periods. Survival analyses used the Kaplan–Meier method and Cox regression models. Results: The total number of resected NF-PanNETs increased over the 15-year study period, from 5 resections in 2006 to 94 resections in 2020. A significant decrease in the tumor size was observed, from a mean of 4.0 cm to 3.3 cm, and to 3.0 cm in the most recent period (p = 0.006). Minimally invasive techniques gradually increased from 3.5% to 12.9%, and finally to 46.4% in the most recent period (p < 0.001). In non-metastatic and resected tumors, the tumor size (p < 0.001), positive lymph node (p < 0.001), adjuvant treatment (p = 0.048), and tumor grade (p < 0.001) were independent prognostic factors for recurrence-free survival (RFS). The microvascular invasion (p = 0.024) and tumor grade (p = 0.013) were independent prognostic factors for overall survival (OS). A malignant transformation from NET into neuroendocrine carcinoma was observed. Conclusions: An increasing number of NF-PanNETs resection and minimally invasive surgery was shown. In non-metastatic and resected tumors NF-PanNETs, tumor size, positive lymph node, adjuvant treatment, and tumor grade were independent predictors of RFS. Microvascular invasion and tumor grade were independent prognostic factors for OS.
Full article
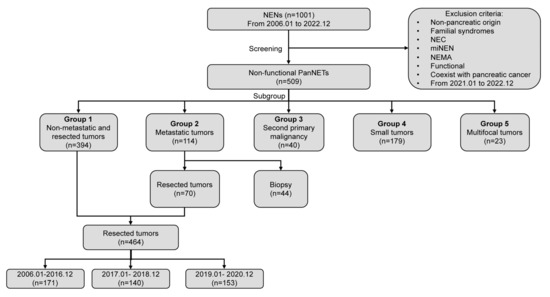
Figure 1

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}