2.6.1. pH of Gastric Content and Mucus Production
The effect of adiponectin on gastric acidity in the ethanol-induced gastric lesion model is reported in
Table 8. The acidity of gastric content in experimental animals pretreated with adiponectin or omeprazole was significantly decreased compared with that of the ulcer control group (p < 0.05). Also the gastric acidity was significantly decreased in the omeprazole treated group compared with the adenopectin groups. However, there were no significant differences between adenopection groups. The mucus production of gastric mucosa were significantly increased (p < 0.05) in animals pretreated with adiponectin or omeprazole compared with ulcer control group (
Table 7). However, there were no significant differences in mucus content between omeprazole and adenopectin groups.
Table 7.
Effect of adenopectin on pH of gastric content and mucus in rats.
Table 7.
Effect of adenopectin on pH of gastric content and mucus in rats.
| Animal Group | Pre-treatment(i.p.) injection | pH of gastric content (Mean ± S.E.M) | Mucus content |
|---|
| 1 | Distilled water (Ulcer control) | 3.34 ± 0.01 c | 0.36 + 0.01 b |
| 2 | Omeprazole (20 mg/kg) | 6.71 ± 0.33 a | 0.55 + 0.02 a |
| 3 | Adiponectin (2.5 mg/kg) | 4.79 ± 0.01 b | 0.52 + 0.01 a |
| 4 | Adiponectin (5 mg/kg) | 5.01 ± 0.01 b | 0.54 + 0.02 a |
2.6.2. Gross Evaluation of Gastric Lesions
The anti-ulcer activity of adiponectin in the ethanol-induced gastric lesion model is shown in
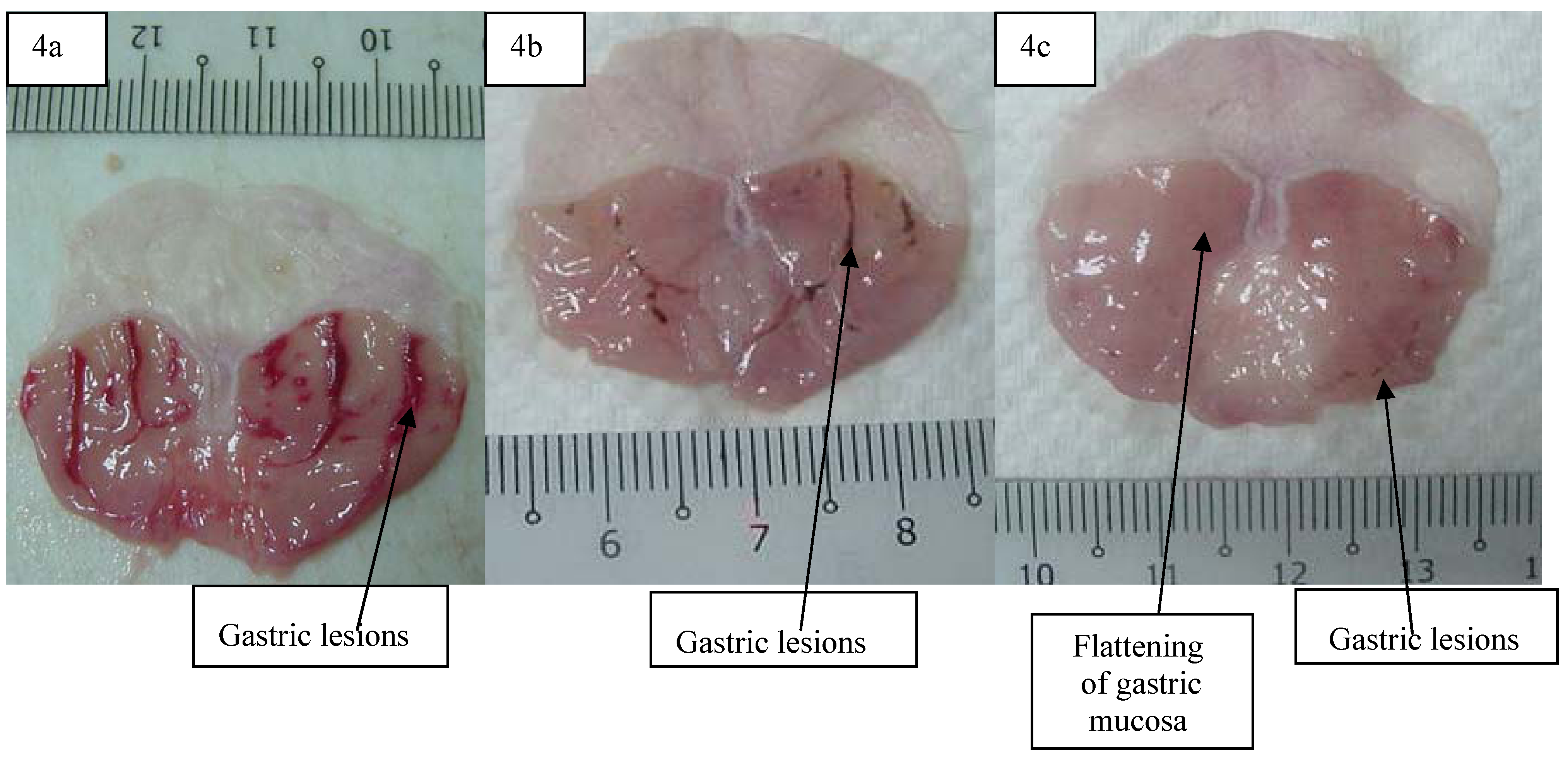
Table 8. Results showed that rats pre-treated with adiponectin before being given absolute ethanol had significantly reduced areas of gastric ulcer formation compared to rats pre-treated with only distilled water (ulcer control group) (
Figure 4 a, b and c) which means to say that the adiponectin significantly suppressed the formation of ulcers. Moreover it was interesting to note the flattening of gastric mucosal folds in rats pre-treated with adiponectin. It was also observed that protection of gastric mucosa was more prominent in rats pre-treated with 5 mg/kg adiponectin (
Table 8). Furthermore, ethanol-induced mucosal damage was significant and dose dependently reduced in the size and severity by pre-treatment of the animals with adiponectin. The significant inhibition of gastric ulcer after pre-treatment with adiponectin by dissolving it with distilled water and i.p. administration to rats in concentrations of 20 mg/kg body weight was comparable with omeprazole, which is a standard drug used for curing gastric ulcers [
11]. Omeprazole is a proton pump inhibitor which has been widely used as an acid inhibitor agents for the treatment of disorders related to gastric acid secretion for about 15 years [
12]. Omeprazole is a substituted benzimidazole that inhibits acid secretion by acting on the hydrogen-potassium exchanger (H+, K+-ATPase) for the apical plasma membrane of the gastric mucosa [
13].
Table 8.
Observed ulcer area and inhibition percentage in rats.
Table 8.
Observed ulcer area and inhibition percentage in rats.
| Animal Group | Pre-treatment (i.p.) injection | Ulcer area (mm)2 (mean ± S.E.M) | Inhibition (%) |
|---|
| 1 | Distilled water (Ulcer control) | 825.33 ± 11.86 a | - |
| 2 | Omeprazole (20 mg/kg) | 183.00 ± 8.47 b | 57.79% |
| 3 | Adiponectin (2.5 mg/kg) | 201.17 ± 9.00 c | 75.63% |
| 4 | Adiponectin (5 mg/kg) | 97.33 ± 8.02 d | 88.23% |
Figure 4.
Gross appearance of the gastric mucosa in (4a) a rat pre-treated with distilled water (negative control). Severe injuries are seen (4b) in the gastric mucosaof a rat pre-treated with omeprazole (20 mg/kg). Injuries to the gastric mucosa are milder compared to the injuries seen in the negative control rat(4c) a rat pre-treated with 5 mg/kg of adiponectin. Mild injuries to the gastric mucosa are seen, and flattening of gastric mucosa is shown.
Figure 4.
Gross appearance of the gastric mucosa in (4a) a rat pre-treated with distilled water (negative control). Severe injuries are seen (4b) in the gastric mucosaof a rat pre-treated with omeprazole (20 mg/kg). Injuries to the gastric mucosa are milder compared to the injuries seen in the negative control rat(4c) a rat pre-treated with 5 mg/kg of adiponectin. Mild injuries to the gastric mucosa are seen, and flattening of gastric mucosa is shown.
Omeprazole is highly selective for the proton pump and undergoes a catalyzed conversion into active form within the acid forming space. The active inhibitors react with SH (thiol) groups of the proton pump, resulting in inhibition of acid formation. Omeprazole blocks the enzymes in the wall of the stomach from producing acid. A decrease in production of stomach acid would thus allow the stomach to heal [
14].
2.6.3. Histological Evaluation of Gastric Lesions
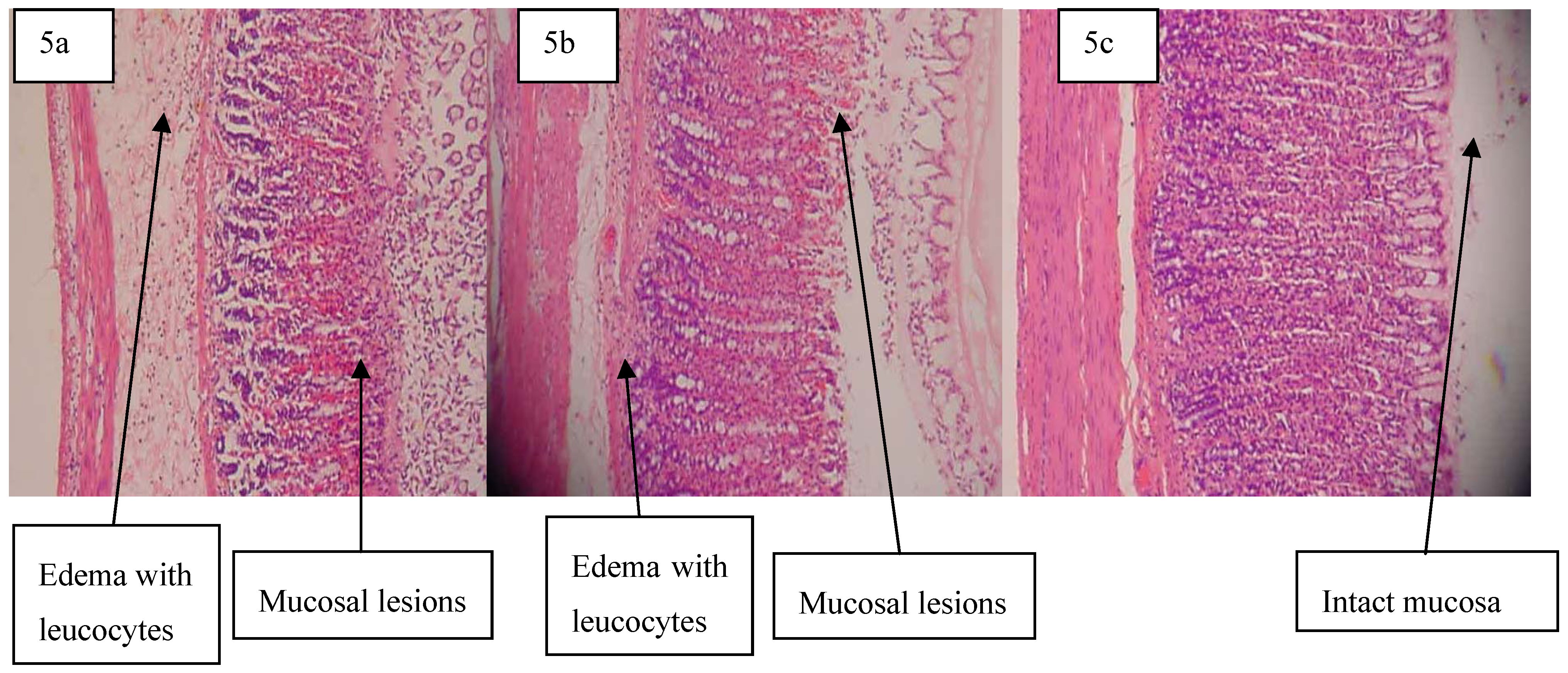
Histological observation of ethanol-induced gastric lesions in the ulcer control group pre-treated with distilled water only showed comparatively extensive damage to the gastric mucosa, edema and leukocyte infiltration of the submucosal layer (
Figure 5a). Rats that received pre-treatment with adiponectin had comparatively better protection of gastric mucosa as seen by the reduction in ulcer area, reduced or absent of sub mucosal edema and leukocyte infiltration. (
Figure 5b and
Figure 5c). Adiponectin has thus been shown to exert its cytoprotective effects in a dose-dependent manner.
One of the adipocyte-specific plasma proteins which are secreted by adipose tissue like other adipocytokines, is adiponectin. Adiponectin modulates a variety of metabolic processes, including glucose regulation and fatty acid catabolism [
15]. Adiponectin displays a multiplicity of functions, such as antiatherogenic and antidiabetic properties [
16], and also acts as an endogenous regulator of endothelial cells in response to inflammatory stimuli and regulates the metabolism of lipids and proteins [
16,
17]. Although adiponectin is secreted from adipose tissue, it is well known that low levels of this protein are present in obese people, which means the levels of this hormone are inversely correlated with body fat percentage in adults [
2,
10,
18]. Adiponectin is secreted into the bloodstream and it accounts for 0.01% of total plasma protein. Plasma concentrations of adiponectin reveal a sexual dimorphism with males having lower levels than females [
16,
19]. A number of oligomeric forms of adiponectin have been described in blood [
20]. Initially three adiponectin molecules bind together to form a homotrimer. Like the plasma concentration, the relative levels of the higher-order structures are sexually dimorphic, where females have increased proportions of the high-molecular weight forms [
21].
Figure 5.
Histology and pathology snapshots of gastric mucosa (5a) in a rat pre-treated with distilled water only. There is severe disruption to the surface epithelium, and edema of the submucosa layer with leucocyte infiltration,(5b)in a rat pre-treated with omeprazole (20 mg/kg). There is mild disruption to the surface epithelium with mild edema and leucocyte infiltration of the submucosal layer, (5c) in a rat pre-treated with 5 mg/kg of adiponectin. There is mild disruption to the surface epithelium with no edema and no leucocyte infiltration of the submucosal layer.
Figure 5.
Histology and pathology snapshots of gastric mucosa (5a) in a rat pre-treated with distilled water only. There is severe disruption to the surface epithelium, and edema of the submucosa layer with leucocyte infiltration,(5b)in a rat pre-treated with omeprazole (20 mg/kg). There is mild disruption to the surface epithelium with mild edema and leucocyte infiltration of the submucosal layer, (5c) in a rat pre-treated with 5 mg/kg of adiponectin. There is mild disruption to the surface epithelium with no edema and no leucocyte infiltration of the submucosal layer.
Production of adiponectin thus is very important for basic research and clinical applications. According to preparation for the operation and production systems compared to recent studies, one of the increasingly popular cellular hosts for expressing the adiponectin is the methylotrophic yeast,
P. pastoris [
22]. The
P. pastoris expression systems have been successfully developed for the production of a variety of heterologous recombinant proteins [
23,
24].
High triglyceride levels and decreased HDL cholesterol levels, but relatively small differences in LDL are the most common patterns of dyslipidemia in type 2 diabetics [
25]. The mean triglyceride level in type 2 diabetes is <200 mg/dL and 85-95% of patients have triglyceride levels below 400 mg/dL. In diabetics, optimal LDL cholesterol levels are <100 mg/dL, optimal HDL cholesterol levels are >45 mg/dL and optimal triglyceride levels are <200 mg/dL. The study of [
26] indicates that metformin is one of the anti-diabetic drugs which has opposing effects on adiponectin protein expression and releases in differentiated adipocytes.
Since metformin is a potent insulin-sensitizing agent that acts primarily on hepatic glucose production and has additional effects on peripheral insulin sensitivity, results from the present study indicate that the effects of a combination of metformin and adiponectin on blood glucose are more effective than the effects of adiponectin itself. The study of adiponectin by [
27] showed that the values of fasting and random blood glucose, serum triglycerides and LDL cholesterol were significantly increased in diabetic patients as compared with normal control subjects, except for serum adiponectin and HDL cholesterol concentrations which were significantly decreased in diabetic patients [
27]. On the other hand, regarding to [
21] the pharmacological effect of adiponectin on dropping insulin resistance is correlated to a decline in triglyceride content and in plasma fatty acid levels in liver and muscle.
Although metformin increases lipolysis and reduces triglyceride stores in adipocytes [
26], and triglyceride accumulation is significantly reduced by supporting the oxidation of lipid treatment of diabetic animals with adiponectin, our study shows that there is no significant difference in the combination of adiponectin and metformin on triglycerides, compared with metformin alone [
28]. This may be because of suppression of adiponectin production through metformin action in different adipocytes [
26].
Since cholesterol levels are closely associated with LDL levels, when total cholesterol levels increased, LDL would do so too. Schmitt
et al. suggested that LDL uptake by fibroblasts may be impaired in type 2 diabetes. This leads to an increase in LDL: HDL ratio in type 2 diabetics. In our study, the LDL ratio did not differ significantly between the control and metformin-adiponectin groups (
p value >0.05). No significant difference was found in the total cholesterol levels in the metformin- adiponectin group compared to other groups of mice [
29].
Adiponectin has also been proven by recent studies to be a remarkable protective factor against development of atherosclerosis due to its anti-inflammatory effects. Now by this theory it is believed that the use of recombinant adiponectin is helpful to avoid cardiovascular disease [
21]. It is known that gastric lesions produced by ethanol administration appear as multiple-hemorrhagic red bands of different size along the glandular stomach. Absolute ethanol is commonly used for inducing ulcers in experimental rats and leads to intense gastric mucosal damage. In the present study, flattening of the mucosal folds was observed, which suggests that gastro-protective effect of adiponectin might be due to a decrease in gastric motility. It is reported that the changes in the gastric motility may play a role in the development and prevention of experimental gastric lesions [
30]. Relaxation of circular muscles may protect the gastric mucosa through flattening of the folds. This will increase the mucosal area exposed to necrotizing agents and reduce the volume of the gastric irritants on the rugal crest [
30,
31]. Ethanol produces a marked contraction of the circular muscles of rat fundic strip. Such a contraction can lead to mucosal compression at the site of the greatest mechanical stress, at the crests of mucosal folds leading to necrosis and ulceration [
30].
The result of the present study also revealed protection of gastric mucosa and inhibition of leucocyte infiltration of gastric wall in rats pre-treated with adiponectin. Similarly, [
30] demonstrated that the reduction of neutrophil infiltration into ulcerated gastric tissue promotes the prevention of gastric ulcers in rats. This study evaluated the activity of adiponectin on gastric ulcer compared to omeprazole for the first time. In the current study, the rats pre-treated with adiponectin have significantly reduced areas of gastric ulcer formation before being given absolute alcohol compared to rats pre-treated with only distilled water. This proves that the adiponectin significantly suppressed the creation of ulcers. Moreover, the present study indicated that the protection of gastric mucosa is more prevalent in rats pre-treated with adiponectin. Besides, ethanol-induced mucosal damage is significant and does dependently reduce in size and severity by pre-treatment of the animals with adiponectin. The significant inhibition of gastric ulcer in pre-treatment with adiponectin was compared with omeprazole which is a standard drug used for curing gastric ulcer. In histological observation, the rats that received pre-treatment with adiponectin had comparatively better protection of the gastric mucosa. Subsequently, adiponectin has been shown to exert cytoprotective effects in a dose-dependent manner.
To determine the safety of adiponectin for human use, toxicological evaluation is carried out in various experimental animals to predict toxicity and to provide guidelines for selecting a ‘safe’ dose in humans. Liver and kidney of the treated rats showed no significant change as compared to the control group. Clinical biochemistry values were within the range of the control animals tested and similar to some of the control reference values published elsewhere [
30,
32]. The highest dose of adiponectinwhich did not cause any toxicity was 5 mg/kg body weight, suggesting that adiponectin is relatively non-toxic since in acute toxicity studies, the product is considered non-toxic if no deaths are registered after 14 days of observation and no clinical signs of toxicity are observed at doses at or below 5 g/kg [
30,
33].



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



