1. Introduction
Glioblastoma multiforme (GBM) affects males and females and knows no age barrier; it accounts for more than 50% of all human primary brain tumors. Despite advances in surgery, chemotherapy, and radiation therapy GBM remains a highly invasive cancer, and the average life span is only 12 to 15 months from time of diagnosis. Increasing incidence of GBM is one of the prime factors driving the development of new therapeutic strategies. GBM is considered the most aggressive form of brain cancer; it grows rapidly and spreads into the normal brain. The National Cancer Institute (NCI) estimates that 23,880 adults will be diagnosed with brain and other nervous system forms of cancer in 2018. The NCI also estimates that in 2018, 16,830 of these diagnoses will result in death [
1]. The mainstay of treatment for GBM is surgery, followed by radiation and chemotherapy. The main objective of surgery is to remove as much of the tumor as possible without injuring the surrounding normal brain tissue needed for neurological function [
2]. Surgical debulking can have multiple positive effects on patient survival including relieving the tumor mass effect, decreasing intracranial pressure, reducing associated brain edema, and lowering steroid dependence, all of which can lead to increased overall patient survival and a higher quality of life [
2]. However, GBM is surrounded by a zone of migrating, infiltrating tumor cells that invade surrounding tissues, which uniformly makes the complete removal of the tumor very challenging.
Temozolomide is a leading molecule for the treatment of newly diagnosed GBM [
3]. The gold standard of therapy for newly diagnosed patients with primary GBM was first introduced more than a decade ago and is called the Stupp protocol [
4]. This consists of a regimen of conformal radiotherapy (dosed fractionated at about 2 Gy/day for a total cumulative dose of 60 Gy) administered concurrently with temozolomide dosed at 75 mg/m
2 for 42 consecutive days, followed by multiple cycles of adjuvant temozolomide administered for 5 days on and 23 days off while dose is escalated up to 150 mg/m
2. Although it represented an important therapeutic advancement at the time of its implementation, the survival gains brought by the Stupp protocol are rather modest because resistance to temozolomide emerges rapidly in GBM and recurrence is typical for these patients. In addition to temozolomide there are only limited therapies available for the treatment of recurrent GBM with very limited survival gains. For recurrent GBM surgical management is a significantly more difficult problem and standard procedures are not fully developed at present. However, the current pipeline of experimental therapeutics for recurrent GBM is strong and includes biologics, small molecules, devices, innovative surgical strategies, and immunotherapy including several approaches in phase I and phase II clinical trials. A large group of immunotherapeutic approaches are currently undergoing clinical study for safety and efficacy in the treatment of newly diagnosed or recurrent high-grade gliomas. Further, combination therapies using immunotherapy and other forms of therapy are being explored [
5]. Some of these new forms of immunotherapy have shown promise, but a significant time delay will be involved for further testing and clinical trials before their incorporation into GBM standard therapy [
6]. Gaining better understanding of the disease will improve what can be achieved through an increase in understanding of molecular mechanisms and the development of clinical trials leading to more promising and effective therapeutic options. In aggregate, recurrent GBM poses a difficult challenge, as the desire to provide significant lesion removal needs to be balanced by the need to preserve neurological function and to retain a good quality of life [
7].
As indicated, due to its highly infiltrative nature, GBM is a complicated disease and thus its treatment is a challenge, forcing researchers into investigating novel diagnostic strategies and unique chemotherapeutic approaches. The tumor microenvironment plays a large role in cancer progression and its pharmacological manipulation can repress progression in the recurrence setting. Central to the ability of GBM cells to invade the surrounding brain distant from the tumor is a class of glycoproteins called integrins. Integrins are heterodimeric cell surface adhesion receptors (containing α and β chains) operating at the interface between the extracellular matrix and cytoskeletal apparatus [
8,
9,
10]. Integrins link cytoskeletal proteins to the extracellular matrix and are involved in bi-directional signaling to alter cellular functions. Among these interactions are the adhesion of both endothelial and glioma cells to extracellular matrix proteins and other interactions that are integral to tumor growth, metastasis and angiogenesis. Integrins allow cells to mechanically sense their environment [
11] by integrating multiple signaling pathways initiated by extracellular cues with the cellular locomotor apparatus. Integrins exhibit structural diversity and undergo conformational changes that are central to the regulation of their receptor function. They exist in three major conformational states: an inactive or low affinity state, a primed or activated high affinity state, and a ligand bound or occupied state [
8]. Activated integrins are not usually present in quiescent tissues, but some, such as the RGD-dependent ones which recognize the Arg-Gly-Asp (RGD) sequence present in key extracellular matrix proteins [
12], play an important role in neoplastic processes including glioma progression [
13], invasion (via invadosome formation) [
14,
15], angiogenesis [
16,
17] and dissemination. This subject was effectively reviewed in [
18].
Disintegrins represent evolution’s integrin targeting “invention”. Disintegrins are a class of disulfide-rich peptides, originally isolated from snake venom [
19,
20,
21]. These peptides hold a significant translational potential with desirable pharmacological attributes based on their high-affinity/high-specificity interaction with tumor integrins. The integrin-binding activity of disintegrins depends on the appropriate pairing of several cysteine residues responsible for the disintegrin fold, a mobile 11-amino acid loop protruding from the polypeptide core displaying a tripeptide motif, RGD in many disintegrins [
22,
23]. It is important to emphasize that disintegrins bind only to the activated conformations of integrins on motile cells such as cancer cells and angiogenic endothelial cells [
8,
21], making them attractive vehicles to specifically target cancerous tissues. We and others demonstrated that disintegrins are well tolerated and can be infused without toxicity or detrimental effect on blood pressure, body temperature, or other physiological parameters [
24,
25,
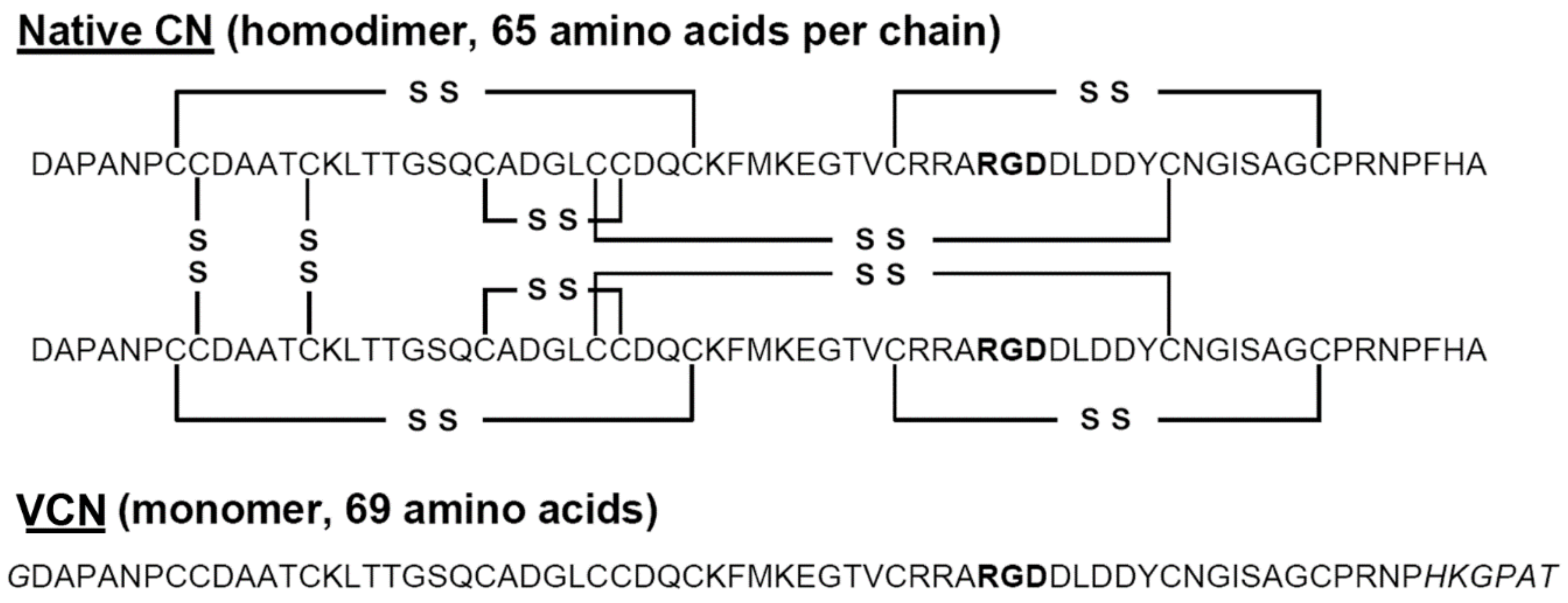
26]. Subsequently, our laboratory designed a sequence-engineered RGD-disintegrin, vicrostatin (VCN), that can be reliably produced in large quantity (~200 mg/L purified VCN from bacterial cell lysate) in a robust recombinant bacterial system [
27,
28]. Recombinant VCN retains the binding properties of the natural disintegrin from which it originated, the homodimer contortrostatin (CN) isolated from southern copperhead snake venom, while showing improved binding affinity, compared to native CN, for an important integrin in angiogenesis, integrin α5β1.
The characteristic expression of very high densities of active RGD-dependent integrins by GBM (expressed both by its florid neovasculature and by the tumor cells themselves) creates a unique opportunity for precision delivery of minute doses of beta-emitting radionuclides (such as 131I) into the tumor microenvironment via highly targeted polypeptides such as VCN. In the present report we describe our findings with the use of radioiodinated-VCN as a form of integrin-targeted radionuclide therapy (brachytherapy) in combination with temozolomide in murine models of human GBM.
3. Discussion
Intratumor implantation of radioactive materials has been historically used to deliver a strong dose of radiation to a small, defined area of glioma tissue, while limiting the amount of radiation damage to nearby normal tissue. For instance,
125I seeds have been used for glioma and there is recent interest in the use of new forms of brachytherapy for glioma [
31]. Two recent reviews detail findings [
32,
33] of brachytherapy in glioma patients. It was noted that there was clear survival advantage with postoperative radiation therapy at doses of 50 to 60 Gy, but dose escalation at doses higher than this resulted in increased toxicity without any survival benefit. For relapsed glioma, brachytherapy is also effective, but is associated with significant toxicity [
32]. Here, we tested the systemic administration of small amounts (dosed at 100 µCi) of beta-emitting radionuclides delivered into the tumor microenvironment of GBM via a novel recombinant disintegrin called vicrostatin (VCN).
VCN was purposely designed with a carboxy-terminal extension, which was expected to enhance affinity for integrin α5β1, and this was confirmed as binding affinity of VCN for α5β1 was found to be ~13-fold higher than that of the native snake venom disintegrin, contortrostatin, VCN was modelled after. Mass spectrometry shows that VCN is predominantly a monomer with a MW of 7146 Da, a size which makes this molecule an ideal candidate for efficient penetration of the tumor microenvironment for payload delivery. Moreover, the high density of integrin targets expressed by the glioma neovasculature obviates the need for VCN to penetrate the blood-brain-barrier in order to deliver its
131I payload. According to the brachytherapy principle and provided that VCN sticks to the neovasculature, the beta particles emitted by
131I will have an effective energy release radius of about 2 mm into the tumor tissue. Regarding the ability of VCN to effectively ligate integrins, unlike cyclic RGD peptides and peptidomimetics, additional structural elements of VCN enable the disintegrin to engage the receptor in an efficient and unique manner which leads to rapid integrin internalization. Unlike cilengitide, cyclo(
l-Arg-Gly-
l-Asp-
d-Phe-
N-methyl-
l-Val), a cyclic RGD peptide that was extensively tested in the clinic in GBM [
34], the additional residues flanking the RGD-loop in VCN enable more extensive contacts with the integrin receptor. Also, NMR and crystallographic studies have revealed that the C-terminal tail in disintegrins folds in close proximity to the RGD-containing disintegrin loop, linking these two structural elements together in an extended conformational epitope, suggesting that these two functional regions are engaged in extensive interactions with the target integrin receptor [
35,
36,
37]. This finding was further supported by our work on the rational design of VCN, accounting for a 13-fold improved affinity for α5β1, by incorporating changes to the amino acid sequence at the COOH-terminus of VCN [
28]. By using structural and functional regions in addition to the RGD motif, a sequence that serves as the sole basis for the design of cyclic RGD peptides and RGD mimetics, disintegrins exhibit novel antitumor activities [
27,
28] compared to small cyclic RGD peptides and peptidomimetics. Due to its robustness and reproducibility, we believe that our recombinant production method will be easily translatable for scale up and cGMP production of VCN. Furthermore, toxicity studies in rodents using dose escalation of VCN (250 mg/kg to 500 mg/kg), a dose many times higher than that used in animal model studies of glioma, demonstrated complete lack of toxicity.
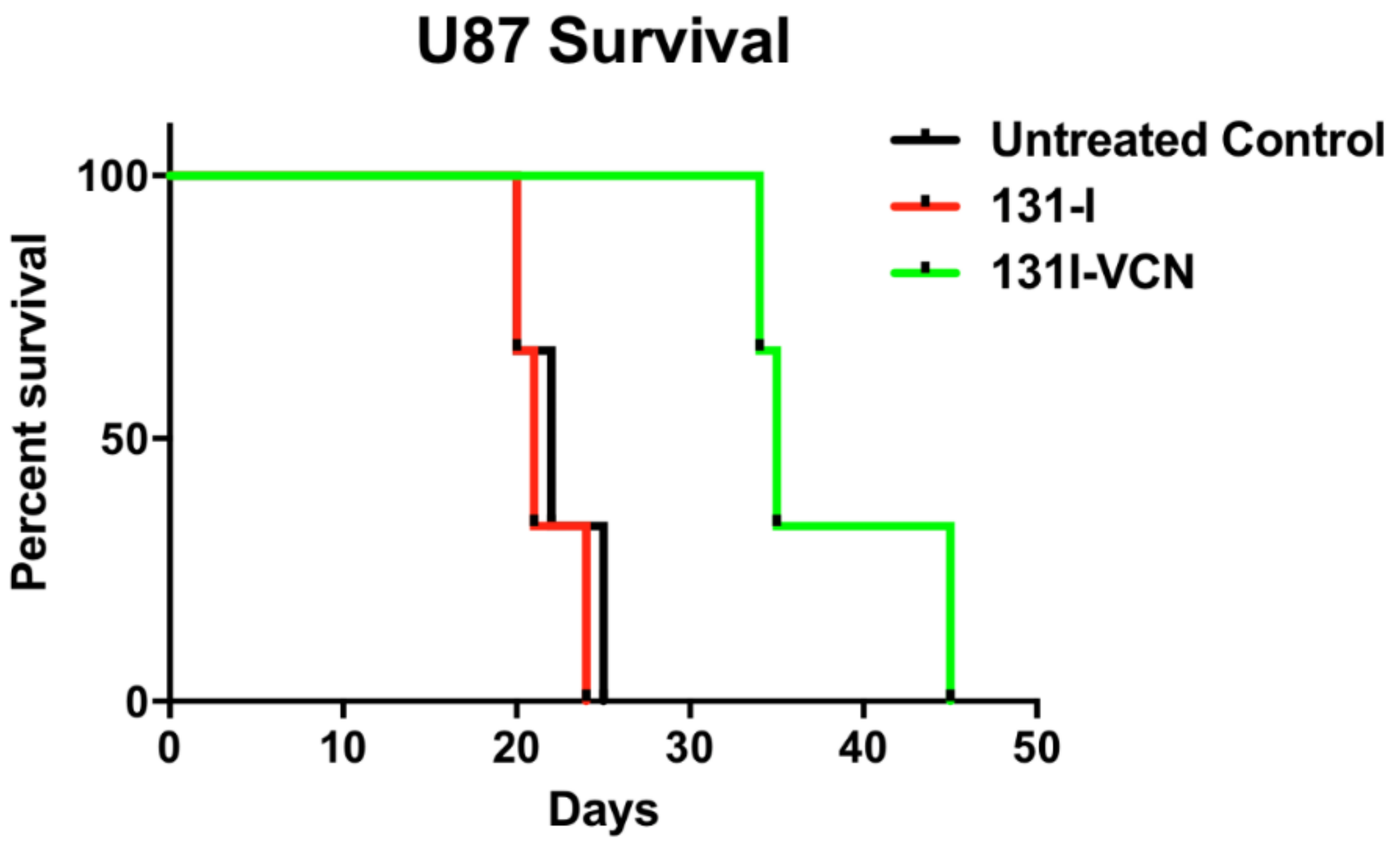
In the present study, we show that radioiodinated VCN can be used for precision delivery of therapeutic doses of
131I into the microenvironment of glioma. In an earlier biodistribution study, we demonstrated that radioiodinated VCN specifically binds to tumor tissue but not to the normal brain after intravenous administration [
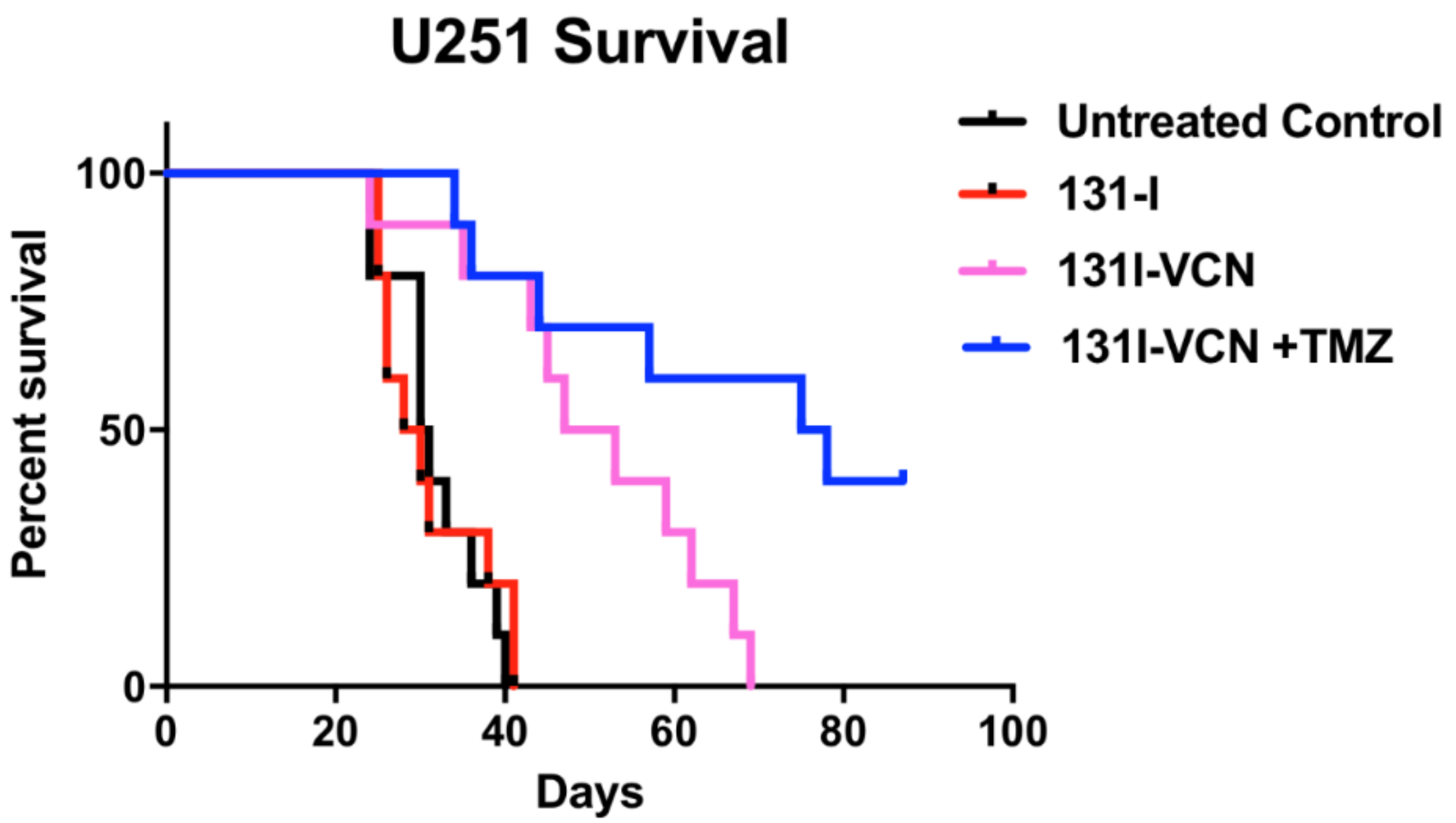
13]. Moreover, in two distinct animal models of glioma we show that radioiodinated VCN can significantly prolong the survival of treated animals. Specifically, in the TMZ-sensitive U251 xenograft model we show that
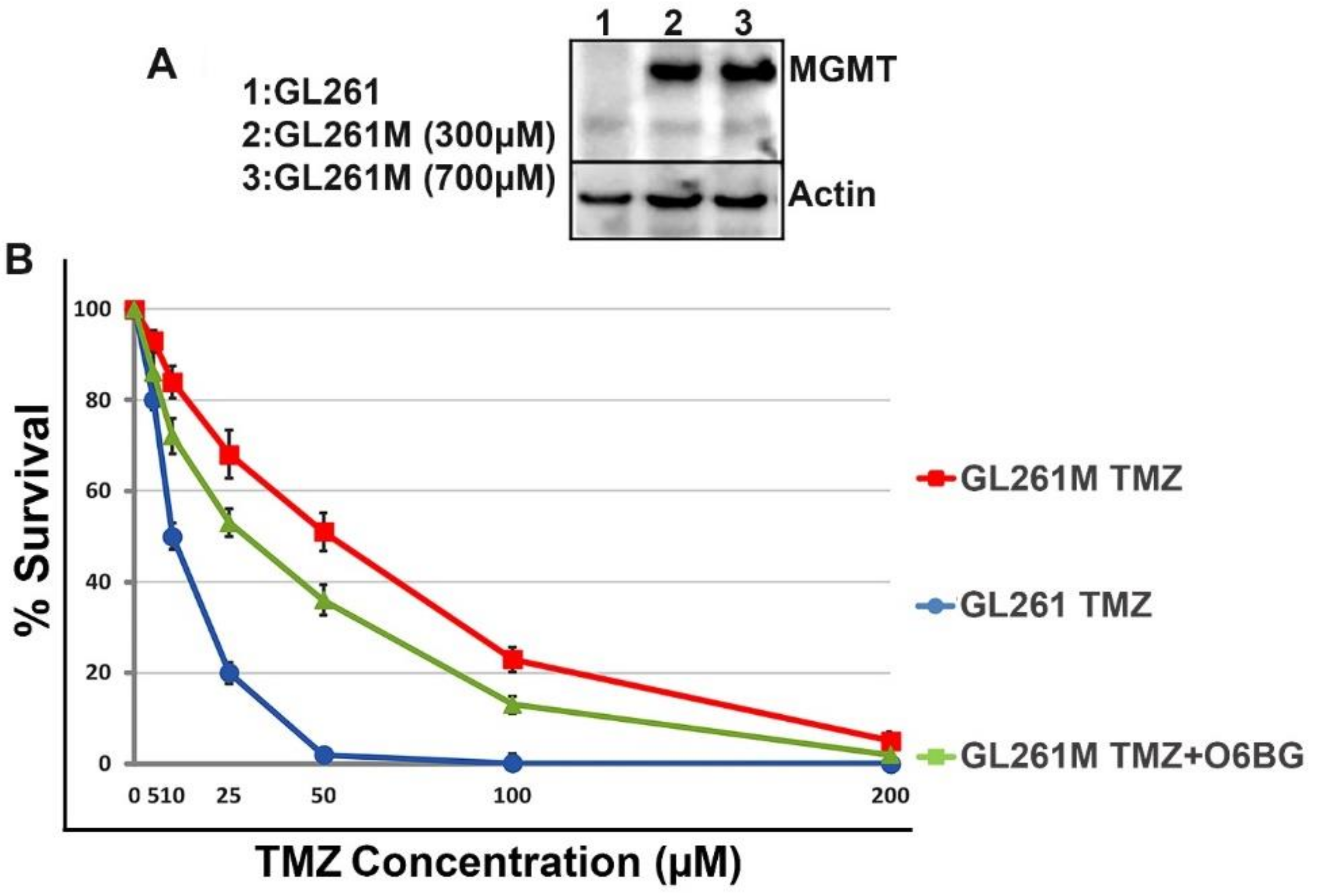
131I-VCN (100 μCi, intravenous) administered in combination with TMZ (25 mg/kg, oral gavage) more than doubles the survival of treated animals compared to the untreated controls. This result encouraged us to test the same therapeutic strategy in a syngeneic model of TMZ-resistant glioma. To establish this model, we transfected GL261 murine glioma cells with a plasmid that carries the murine
MGMT gene under a mouse medium-strength promoter (i.e., the murine phosphoglycerate kinase 1 promoter). The transfected cells were further incubated in increased concentrations of TMZ (up to 700 μM) to select for highly TMZ-resistant clones which were further implanted in syngeneic hosts. In this model, we compared head-to-head the efficacy of
131I-VCN in combination with TMZ versus external beam radiotherapy in combination with TMZ. Although we expected all O6-methylguanine lesions to be directly reversed in the presence of murine MGMT, we reasoned that TMZ could still synergize with radiotherapy in this model via non-O6-methylguanine lesions, which in fact represent more than 90% of the DNA lesions inflicted by TMZ. Indeed, the combination of
131I-VCN plus TMZ proved superior to
131I-VCN alone which clearly suggest the possibility of a synergistic effect between TMZ and
131I-VCN in this setting. Moreover, two doses of
131I-VCN (100 μCi given twice) proved to be superior to five consecutive doses of whole-brain external beam radiotherapy (2 Gy given five times). These preliminary data suggest that, if dosed according to rigorous dosimetry studies,
131I-VCN may have the potential to significantly synergize with TMZ in the clinical setting of TMZ resistance (i.e., typically newly diagnosed patients with GBM tumors with unmethylated
MGMT promoters). This could represent a therapeutic alternative to the current Stupp protocol [
4] which only provides very limited benefit to this subset of patients.
We would like to make one additional point regarding the potential off-target effects of 131I-VCN in a clinical scenario. When compared to 131I sodium iodide which, even though it cannot discriminate between normal and cancerous thyroid tissue, is used in clinical practice for radioablation of cancerous thyroid cells, radioiodinated VCN is a much bigger molecule (i.e., a polypeptide of ~7 KDa). Due to its size, it is highly unlikely that VCN will fit into the Na-I symporter expressed by thyroid cells. For this reason, we predict that 131I-VCN will not accumulate in the thyroid glands of GBM patients treated with this form of intravenous brachytherapy. Moreover, the normal thyroid tissue is not known to express the integrin receptors expressed by the GBM tissue, which are ligated by VCN. However, because a potential off-target/off-tumor accumulation of radioactive material remains a concern with any form of radioiodine brachytherapy in clinical practice, we believe that any therapeutic protocol for 131I-VCN in glioma patients should include a pre-brachytherapy dosing step with potassium iodide. This preparatory step is intended to temporarily shut down the thyroid glands of GBM patients while 131I-VCN is present in the circulation.
In aggregate, our animal studies demonstrate that VCN can be successfully used as a novel delivery mechanism for targeting radioactivity to glioma cells. Although results are still preliminary, they serve as a proof-of-principle demonstration that radioiodinated VCN, which we tested in several animal models of GBM, can serve as an effective therapeutic approach for this deadly form of cancer. Further, the complexity of the cancer microenvironment dictates that for optimal efficacy an anti-integrin therapeutic must target at least two members of the RGD-binding integrin class and preferably more [
38] given the ability of cancer cells to change their integrin repertoire in response to drug treatment. Our experience with VCN, which binds to multiple RGD-dependent integrins, suggests that it admirably meets this criterion while also showing minimal binding to normal tissue. Therefore, its excellent stability and high affinity for tumor integrins uniquely positions VCN for precision delivery of targeted radioactivity in GBM, a type of solid tumor where radiotherapy is an integral part of standard of care. In future investigations we will conduct dosimetry studies with VCN labeled with
124I (a positron emitter), which will allow us to precisely calculate by quantitative PET (positron emission tomography) imaging the therapeutic dose of
131I-VCN for each animal based on its tumor burden and integrin biology.
4. Materials and Methods
4.1. Cells and Reagents
The U87 and U251 human glioma cell lines were obtained from ATCC (Manassas, VA, USA) and maintained according to the manufacturer’s protocol. The GL261 murine glioma cell line was a gift from Dr. Alan Epstein (Keck School of Medicine, University of Southern California, Los Angeles, CA, USA). The TMZ-resistant variant of GL261 cell (i.e., GL261M) were generated by transfecting the wildtype cells with a plasmid construct carrying the mouse O6-methylguanine-DNA-methyltransferase (
MGMT) gene under a mouse phosphoglycerate kinase 1 (mPGK) promoter. The transfected GL261 cells were further cultured in increasing concentrations of TMZ (up to 700 μM) to select the GL261M variant. VCN was produced and purified in the Markland laboratory [
27,
28]. Female 5-week-old 20 g Balb/c
nu/nu mice were obtained from Simonsen Laboratories (Gilroy, CA, USA), and 5-week old C57
bl/6 mice were obtained from Charles River Laboratories (Boston, MA, USA). Sodium iodine (
131I) was obtained from Perkin-Elmer (Billerica, MA, USA). All other reagents were purchased from Sigma Chemical Co. (St. Louis, MO, USA). External beam radiotherapy was administered in a X-RAD320 irradiator (Precision X-Ray, North Branford, CT, USA). Temozolomide (TMZ) was obtained from TCI America (Portland, OR, USA).
4.2. Radioactive and Radioinert Iodination of VCN
VCN in solution was directly iodinated with radioiodine (
131I) or radioinert sodium iodide using a modification of the chloramine T method [
29]. Briefly, chloramine T was dissolved in PBS and added to a buffered VCN solution (100–600 µg at 0.3–2.0 mg/mL in PBS) containing Na
131I. Five successive aliquots of 15 µg chloramine T (in 5 µL) were added at 5-min intervals to the reaction mixture (final volume 400 µL). Following the final chloramine T addition, excess
131I was quenched through the addition of sodium metabisulfite (100 µg/400 µL reaction). Unreacted iodine was removed from the
131I-VCN solution and the buffer exchanged by 2× repeated filtration through a centrifugal 4-kDa cutoff filter (VWR, Atlanta, GA, USA). This allows iodine to pass through the membrane and be separated from the iodinated VCN solution.
4.3. Evaluation of Stoichiometry of Iodine Addition
The stoichiometry of iodine addition to VCN was determined by use of mass spectrometry. A LC-Electro-spray ionization mass spectrometry system was employed in the positive ion mode (Agilent, Santa Clara, CA, USA). A control of non-iodinated VCN was used as a standard.
4.4. FACS Analysis of VCN Binding to Glioma Cell Lines
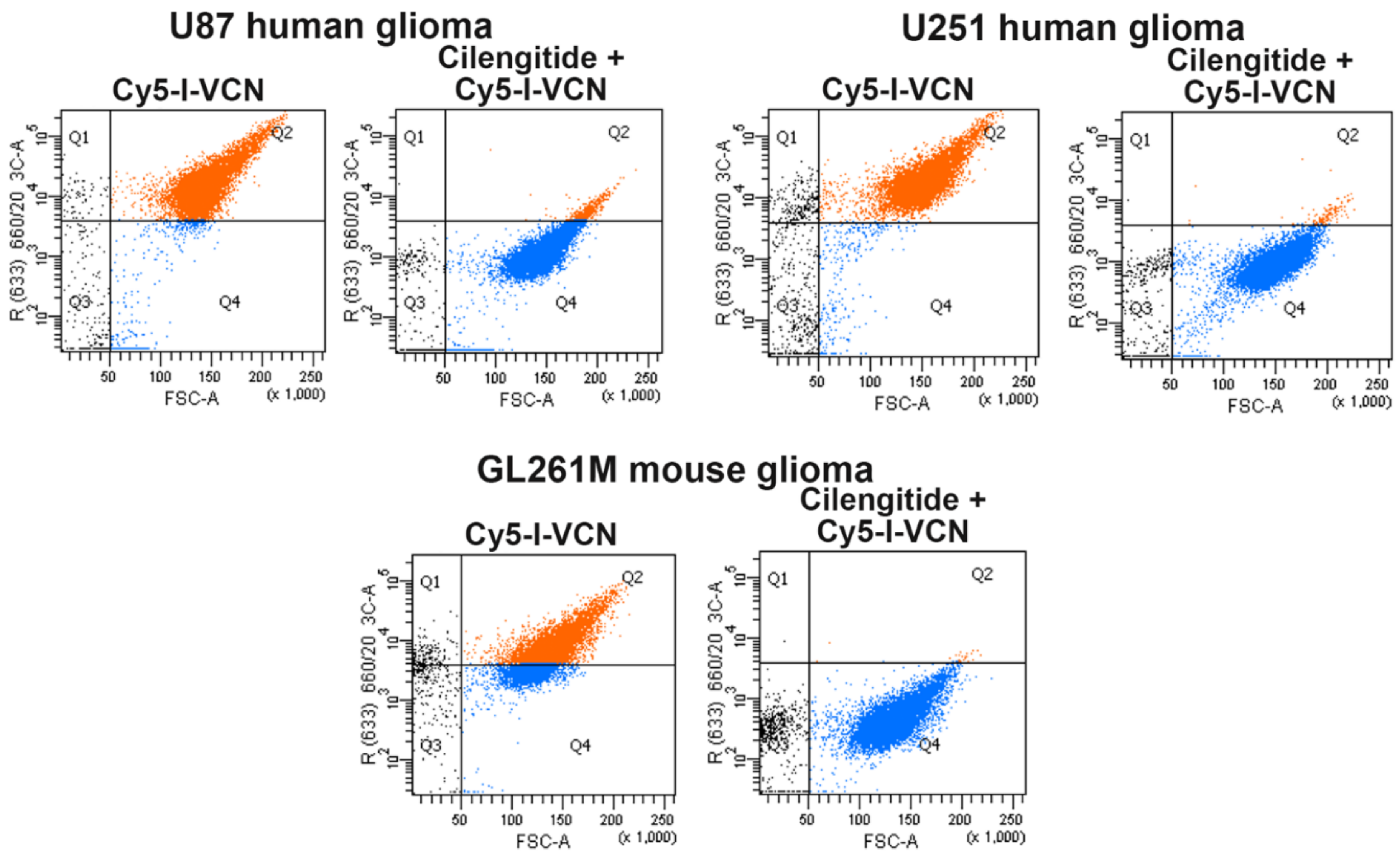
The cold iodinated VCN (I-VCN) was further conjugated with Cy5-NHS (Lumiprobe, Hunt Valley, MD, USA) according to manufacturer’s protocol. For FACS analysis, 10
6 glioma cells (U87, U251, and GL261M) in complete DMEM (Dulbecco’s Modified Eagle Medium) were incubated with or without 100-fold molar excess of a small cyclic RGD peptide called Cilengitide (Selleck Chemicals, Houston, TX, USA) [
30] for 20 min at 37 °C, then pelleted and resuspended in ice-cold PBS. The cells were further incubated for 60 min at 4 °C with Cy5-I-VCN, then pelleted, washed and resuspended in ice-cold PBS. The cells were further analyzed on a BD FACSAria II instrument (BD Biosciences, Franklin Lakes, NJ, USA) equipped with a 642 nm red laser. Cells incubated with unlabeled disintegrin (i.e., negative control) were used to calibrate the instrument.
4.5. Confirmation of Biological Activity of Iodinated VCN
The inhibition of ADP-induced platelet aggregation by iodinated-VCN (both I-VCN and Cy5-I-VCN) was measured by determining the light absorption of human platelet-rich plasma (PRP) in a specialized spectrophotometer (Chrono-log 490 optical aggregometer, Chrono-log, Havertown, PA, USA) as previously described [
39]. The iodinated disintegrins (I-VCN and Cy5-I-VCN) were tested for activity against unlabeled VCN.
4.6. Functional Analysis of GL261M Cells to Confirm MGMT Expression and Activity
Lysates prepared from wildtype GL261 and TMZ-resistant GL261M cells were analyzed by Western-blotting for MGMT expression levels. A rabbit polyclonal antibody that cross-reacts with the mouse MGMT protein was purchased from Boster Biological Technology (Pleasanton, CA, USA) and used in this Western-blot analysis. This antibody was raised against a synthetic peptide PVFQQESFTRQVLWK, which corresponds to a sequence in the middle region of human MGMT which is different from the related rat and mouse sequences by only one amino acid. Furthermore, to check the functionality of the MGMT enzyme resulting from transfection of the MGMT gene into GL261 cells, we completed a colony formation assay (CFA) with GL261M cells incubated in a range of TMZ concentrations in the presence or absence of the MGMT inhibitor O6-benzylguanine (Millipore Sigma, Burlington, MA, USA).
4.7. Establishment of Orthotopic Xenograft Glioma Models
All animal protocols were approved by the University of Southern California, IACUC (20707-CR001, 29 March 2018), and animals maintained according to approved guidelines. To perform this orthotopic xenograft model, tumors were implanted 3 mm deep in the midline of mice brains using stereotactic injections. Following surgical exposure of the skull and drilling a small-bore hole with a dental drill, U87 or U251 (2 × 105/2 µL) glioma cells were injected using a slow controlled injection followed by a one-minute rest period with syringe in place to minimize leakage from the injection track. The syringe was slowly removed, the hole covered with wax, and the surgical incision was then closed with 2 stitches (3.0 silk). Following implantation (7–14 days) tumor take was evaluated by bioluminescent imaging. This was only possible in the U87 and U251 models in which the injected tumor cells were labeled with GFP and firefly luciferase. In these xenograft models, the tumors were imaged by intravenous injection of luciferin followed by a 90 s wait period when the animal was placed in a Xenogen IVIS 200 imaging instrument (Perkin Elmer, Waltham, MA, USA) before acquiring optical images. In our experience with these xenograft models, >90% of mice show a bioluminescent signal at 7 days post-implantation. Positive, tumor bearing, mice were then randomized into treatment and control groups.
4.8. Evaluation of Brain-Uptake of Radioiodinated-VCN
To determine tumor specific brain uptake and retention of iodinated VCN, mice were implanted with human gliomas (U87 as above) and the tumors were allowed to grow for 14 days. At this point mice with confirmed tumors and control non-tumor bearing mice were injected with a single dose of 125I-VCN (100 µCi) administered intravenously. Radioactively labeled VCN was allowed to circulate for 18 h at which time the animals were euthanized, and brains removed, rinsed and counted in a 2480 WIZARD2 gamma counter available in the Molecular Imaging Center at the Health Sciences Campus, University of Southern California.
4.9. Establishment of a Syngeneic Model of Glioma
For these studies, immunocompetent syngeneic C57BL/6 mice were implanted orthotopically with TMZ-resistant GL261M glioma cells. Following a protocol identical to the method used with the orthotopic xenograft model, tumors were implanted, and 13 days post implantation treatment was initiated. Due to immune rejection concerns, these tumor cells were not labeled with foreign transgenes such as GFP and luciferase, thus tumor growth could not be confirmed by bioluminescent imaging in this syngeneic model. However, based on survival curves that were previously generated by us after implanting various numbers of GL261M cells in vivo, we expected tumor growth in 100% of the mice implanted with 1 × 105 GL261M cells.
4.10. Treatment of Animal Models
For the U87 glioma studies, the following groups were employed (five mice per group): (i) untreated control, (ii) treatment with
131I alone (administered IV as Na
131I) and (iii)
131I-VCN. The dose of radioactivity administered was 100 µCi either iodine alone or radioiodinated VCN (
131I-VCN). The mice were treated with a single dose and monitored daily for changes in weight and physical status. For the
131I-VCN combination with TMZ chemotherapy U251 glioma positive mice were randomized into 4 groups of 10 mice each. These groups were: (i) untreated control, (ii)
131I alone, (administered IV as Na
131I), (iii)
131I-VCN alone, and (iv)
131I-VCN plus TMZ. The radioactivity was delivered as 100µCi either sodium iodine alone or radioiodinated VCN (
131I-VCN) given in two doses separated by three days (each with 100 μCi
131I-VCN). The groups receiving TMZ had the agent delivered as a daily 25 mg/kg gavage over five consecutive days. The efficacy of
131I-VCN plus TMZ was further compared to external beam radiation therapy (EBRT) plus TMZ in a TMZ-resistant syngeneic model. In this model, we evaluated the following groups (five mice per group): (i) untreated control, (ii)
131I-VCN alone, (iii) EBRT plus TMZ and (iv)
131I-VCN plus TMZ. The radioactivity was delivered as 100 µCi either iodine alone or
131I-VCN given in two doses separated by three days (each with 100 μCi). In comparison, the EBRT plus TMZ group followed a dosing regimen mimicking the Stupp protocol [
4] with TMZ delivered as a daily 25 mg/kg gavage concurrently with 2 Gy EBRT daily for five consecutive days. External beam irradiation was performed at 250 kv and 16 mA with a dose of 200 cGy delivered over 47 s to the skull of each animal over five consecutive days. Except for the skull area, the rest of each animal’s body was protected by a 3 mm-thick lead shield.
4.11. Statistical Significance
To determine statistical significance, the outcomes of the individual treatments were compared to the untreated controls using the Wilcoxon–Mann–Whitney two-sample rank-sum test. The treatment effect (difference between treatments) was quantified using the Hodges–Lehmann (HL) estimator, which is consistent with the Wilcoxon test. p values were determined and values less than 0.05 were considered significant.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}