
Fracture Load of CAD/CAM Fabricated Cantilever Implant-Supported Zirconia Framework: An In Vitro Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
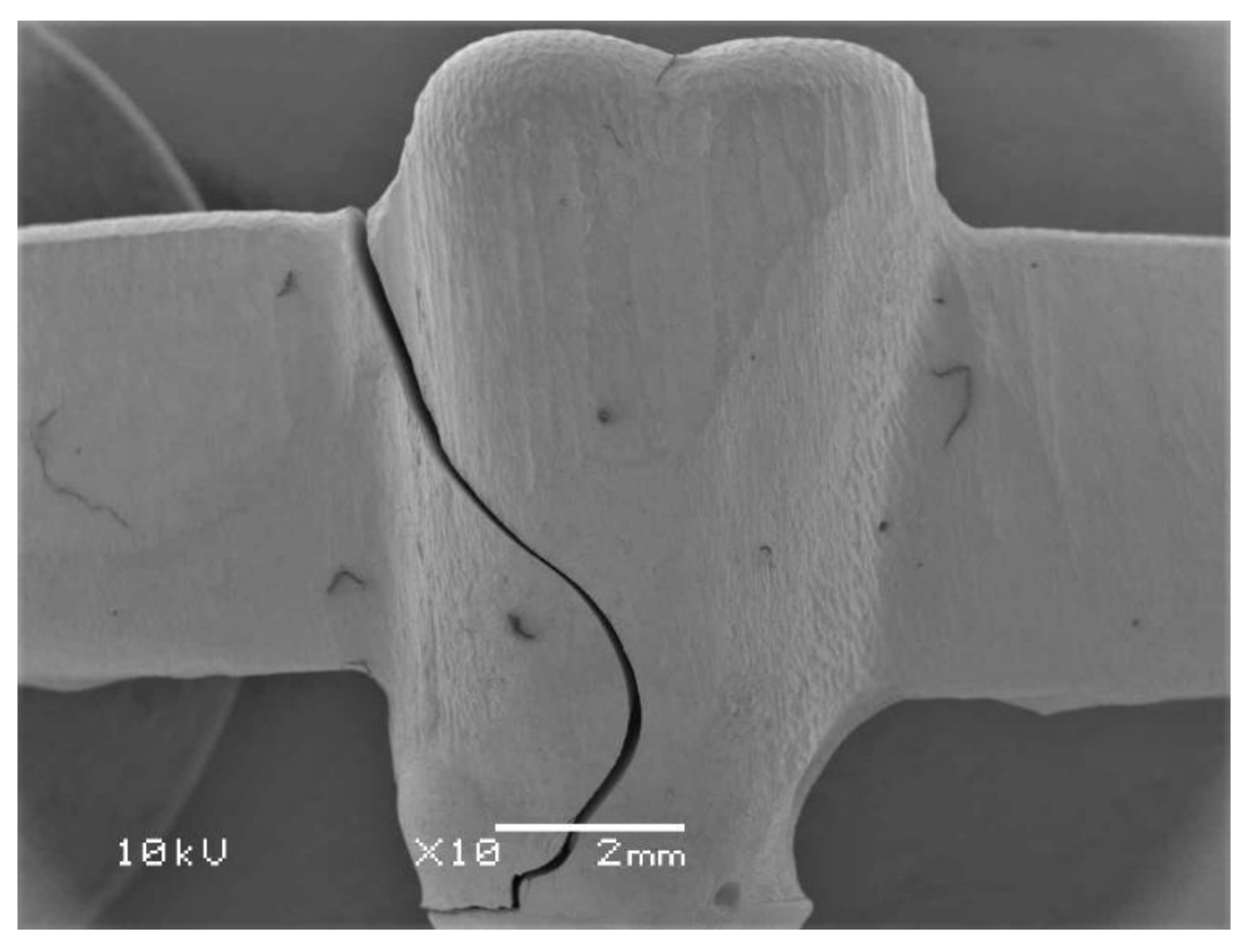
2. Results and Discussion
3. Materials and Methods
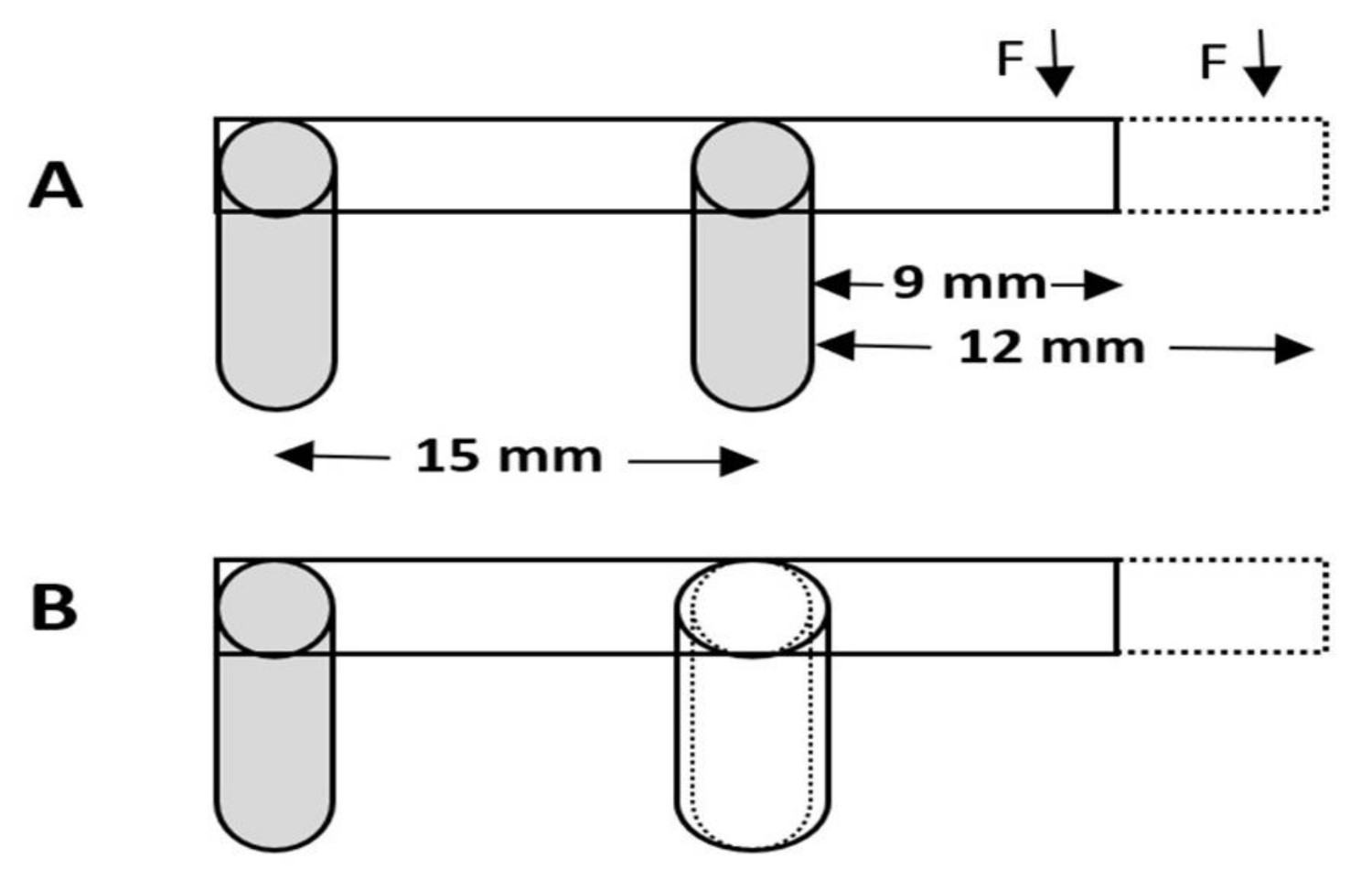
3.1. Sample Preparation
3.2. Thermocycling of the Specimens
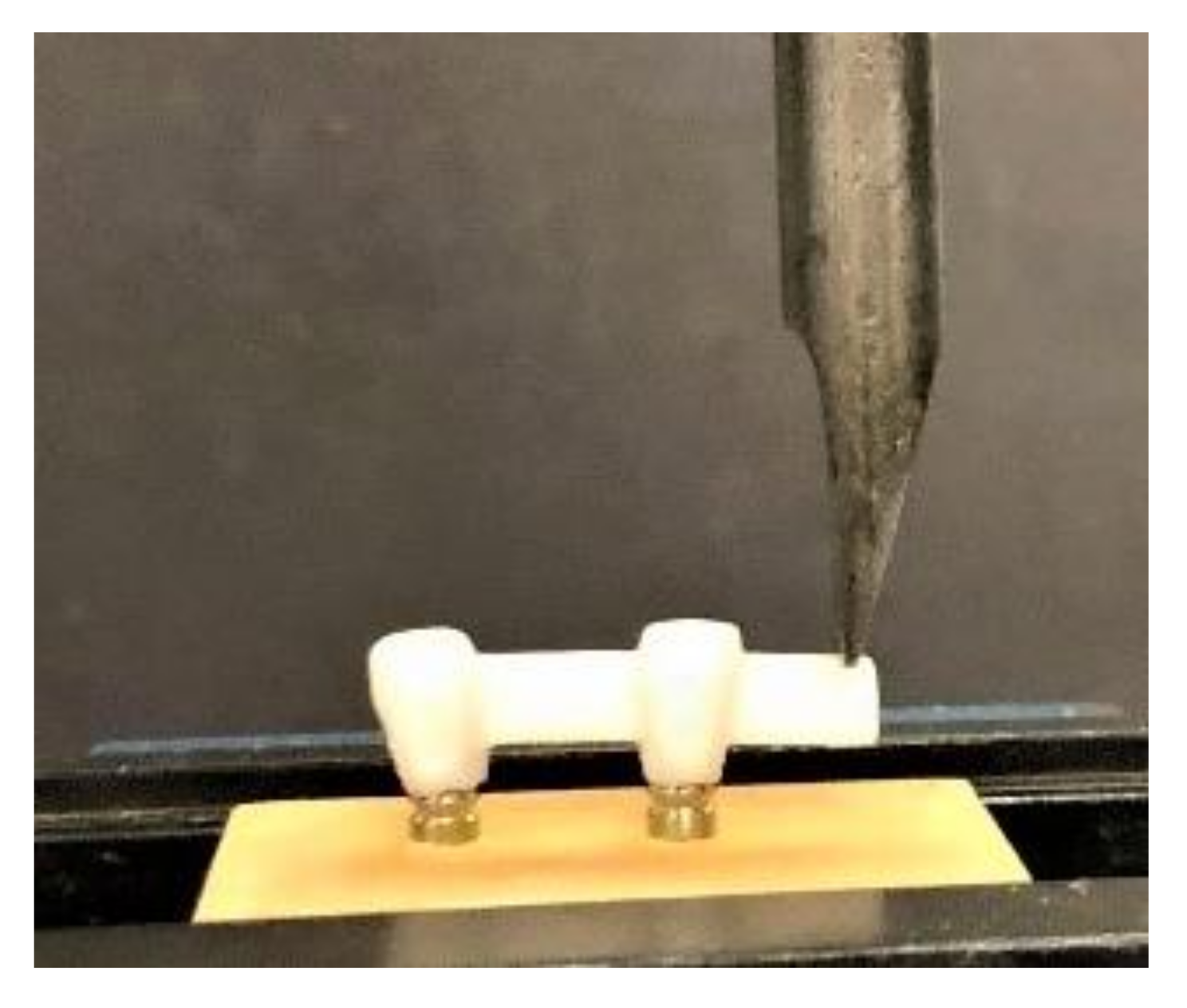
3.3. Testing of the Fracture Strength
3.4. Statistical Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Nistor, L.; Grădinaru, M.; Rîcă, R.; Mărășescu, P.; Stan, M.; Manolea, H.; Ionescu, A.; Moraru, I. Zirconia Use in Dentistry—Manufacturing and Properties. Curr. Health Sci. J. 2019, 45, 28–35. [Google Scholar] [PubMed]
- Miyazaki, T.; Nakamura, T.; Matsumura, H.; Ban, S.; Kobayashi, T. Current status of zirconia restoration. J. Prosthodont. Res. 2013, 57, 236–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solá-Ruiz, M.F.; Leon-Martine, R.; Labaig-Rueda, C.; Selva-Otalaorrouchi, E.; Agustín-Panadero, R. Clinical outcomes of veneered zirconia anterior partial fixed dental prostheses: A 12-year prospective clinical trial. J. Prosthet. Dent. 2020, in press. [Google Scholar] [CrossRef]
- Solá-Ruiz, M.F.; Baixauli-López, M.; Roig-Vanaclocha, A.; Amengual-Lorenzo, J.; Agustín-Panadero, R. Prospective study of monolithic zirconia crowns: Clinical behavior and survival rate at a 5-year follow-up. J. Prosthodont. Res. 2020. [Google Scholar] [CrossRef]
- Zarone, F.; Russo, S.; Sorrentino, R. From porcelain-fused-to-metal to zirconia: Clinical and experimental considerations. Dent. Mater. 2011, 27, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Kelly, J.R. Dental Ceramics for Restoration and Metal Veneering. Dent Clin N. Am. 2017, 61, 797–819. [Google Scholar] [CrossRef]
- Agustín-Panadero, R.; Román-Rodríguez, J.L.; Ferreiroa, A.; Solá-Ruíz, M.F.; Fons-Font, A. Zirconia in fixed prosthesis. A literature review. J. Clin. Exp. Dent. 2014, 6, e66–e73. [Google Scholar] [CrossRef]
- Poggio, C.E.; Ercoli, C.; Rispoli, L.; Maiorana, C.; Esposito, M. Metal-free materials for fixed prosthodontic restorations. Cochrane Database Syst. Rev. 2017, 12, CD009606. [Google Scholar] [CrossRef]
- Özkurt, Z.; Kazazoğlu, E. Zirconia dental implants: A literature review. J. Oral Implantol. 2011, 37, 367–376. [Google Scholar] [CrossRef]
- Lancellotta, V.; Pagano, S.; Tagliaferri, L.; Piergentini, M.; Ricci, A.; Montecchiani, S.; Saldi, S.; Chierchini, S.; Cianetti, S.; Valentini, V.; et al. Individual 3-dimensional printed mold for treating hard palate carcinoma with brachytherapy: A clinical report. J. Prosthet. Dent. 2019, 121, 690–693. [Google Scholar] [CrossRef]
- Kanat, B.; Cömlekoğlu, E.M.; Dündar-Çömlekoğlu, M.; Hakan Sen, B.; Ozcan, M.; Ali Güngör, M. Effect of various veneering techniques on mechanical strength of computer-controlled zirconia framework designs. J. Prosthodont. 2014, 23, 445–455. [Google Scholar] [CrossRef]
- Meirowitz, A.; Bitterman, Y.; Levy, S.; Mijiritsky, E.; Dolev, E. An in vitro evaluation of marginal fit zirconia crowns fabricated by a CAD-CAM dental laboratory and a milling center. BMC Oral Health 2019, 19, 103. [Google Scholar] [CrossRef] [Green Version]
- Habib, S.R.; Al Otaibi, A.K.; Al Anazi, T.A.; Al Anazi, S.M. Comparison between five CAD/CAM systems for fit of zirconia copings. Quintessence Int. 2018, 49, 437–444. [Google Scholar]
- Ahmadzadeh, A.; Ghanavati, S. Comparison of bond strength of two porcelains and two base metal alloys in metal-ceramic restorations. Dent. Res. J. 2019, 16, 298–303. [Google Scholar]
- Wang, H.; Feng, Q.; Li, N.; Xu, S. Evaluation of metal-ceramic bond characteristics of three dental Co-Cr alloys prepared with different fabrication techniques. J. Prosthet. Dent. 2016, 116, 916–923. [Google Scholar] [CrossRef]
- Roberts, H.W.; Berzins, D.W.; Moore, B.K.; Charlton, D.G. Metal-ceramic alloys in dentistry: A review. J. Prosthodont. 2009, 18, 188–194. [Google Scholar] [CrossRef]
- Daou, E.E. The zirconia ceramic: Strengths and weaknesses. Open Dent. J. 2014, 8, 33–42. [Google Scholar] [CrossRef]
- Shahdad, S.; Cattell, M.J.; Cano-Ruiz, J.; Gamble, E.; Gambôa, A. Clinical Evaluation of All Ceramic Zirconia Framework Resin Bonded Bridges. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 203–211. [Google Scholar]
- Sailer, I.; Fehér, A.; Filser, F.; Gauckler, L.J.; Lüthy, H.; Hämmerle, C.H. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int. J. Prosthodont. 2007, 20, 383–388. [Google Scholar]
- Sax, C.; Hämmerle, C.H.; Sailer, I. 10-year clinical outcomes of fixed dental prostheses with zirconia frameworks. Int. J. Comput. Dent. 2011, 14, 183–202. [Google Scholar]
- Komiyama, O.; Lobbezoo, F.; De Laat, A.; Iida, T.; Kitagawa, T.; Murakami, H.; Kato, T.; Kawara, M. Clinical management of implant prostheses in patients with bruxism. Int. J. Biomater. 2012, 2012, 369063. [Google Scholar] [CrossRef]
- Ferrato, G.; Falisi, G.; Ierardo, G.; Polimeni, A.; Di Paolo, C. Digital evaluation of occlusal forces: Comparison between healthy subjects and TMD patients. Ann. Stomatol. 2017, 8, 79–88. [Google Scholar] [CrossRef]
- Kasai, K.; Takayama, Y.; Yokoyama, A. Distribution of occlusal forces during occlusal adjustment of dental implant prostheses: A nonlinear finite element analysis considering the capacity for displacement of opposing teeth and implants. Int. J. Oral Maxillofac. Implants 2012, 27, 329–335. [Google Scholar] [PubMed]
- Koc, D.; Dogan, A.; Bek, B. Bite force and influential factors on bite force measurements: A literature review. Eur. J. Dent. 2010, 4, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Pott, P.C.; Eisenburger, M.; Stiesch, M. Survival rate of modern all-ceramic FPDs during an observation period from 2011 to 2016. J. Adv. Prosthodont. 2018, 10, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Norström Saarva, V.; Bjerkstig, G.; Örtorp, A.; Svanborg, P. A Three-Year Retrospective Study on Survival of Ceramic-Veneered Zirconia (Y-TZP) Fixed Dental Prostheses Performed in Private Practices. Int. J. Dent. 2017, 2017, 9618306. [Google Scholar] [CrossRef] [Green Version]
- Walls, A.W. Cantilever FPDs have lower success rates than end abutted FPDs after 10-years of follow-up. J. Evid. Based Dent. Pract. 2010, 10, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Himmel, R.; Pilo, R.; Assif, D.; Aviv, I. The cantilever fixed partial denture—A literature review. J. Prosthet. Dent. 1992, 67, 484–487. [Google Scholar] [CrossRef]
- Kim, P.; Ivanovski, S.; Latcham, N.; Mattheos, N. The impact of cantilevers on biological and technical success outcomes of implant-supported fixed partial dentures. A retrospective cohort study. Clin. Oral Implants Res. 2014, 25, 175–184. [Google Scholar] [CrossRef]
- Becker, C.M.; Kaiser, D.A. Implant-retained cantilever fixed prosthesis: Where and when. J. Prosthet. Dent. 2000, 84, 432–435. [Google Scholar] [CrossRef]
- Romanos, G.E.; Gupta, B.; Eckert, S.E. Distal cantilevers and implant dentistry. Int. J. Oral Maxillofac. Implants 2012, 27, 1131–1136. [Google Scholar] [PubMed]
- Sharma, A.; Rahul, G.R.; Poduval, S.T.; Shetty, K. Assessment of various factors for feasibility of fixed cantilever bridge: A review study. ISRN Dent. 2012, 2012, 259891. [Google Scholar] [CrossRef]
- Romeed, S.A.; Fok, S.L.; Wilson, N.H. Biomechanics of cantilever fixed partial dentures in shortened dental arch therapy. J. Prosthodont. 2004, 13, 90–100. [Google Scholar] [CrossRef]
- Takaba, M.; Tanaka, S.; Ishiura, Y.; Baba, K. Implant-supported fixed dental prostheses with CAD/CAM-fabricated porcelain crown and zirconia-based framework. J. Prosthodont. 2013, 22, 402–407. [Google Scholar] [CrossRef]
- Habib, S.R. Digital microscopic evaluation of vertical marginal discrepancies of CAD/CAM fabricated zirconia cores. Biomed. Tech. 2019, 64, 207–214. [Google Scholar] [CrossRef]
- Lee, B.; Oh, K.C.; Haam, D.; Lee, J.H.; Moon, H.S. Evaluation of the fit of zirconia copings fabricated by direct and indirect digital scanning procedures. J. Prosthet. Dent. 2018, 120, 225–231. [Google Scholar] [CrossRef]
- Zucuni, C.P.; Guilardi, L.F.; Fraga, S.; May, L.G.; Pereira, G.K.R.; Valandro, L.F. CAD/CAM machining Vs pre-sintering in-lab fabrication techniques of Y-TZP ceramic specimens: Effects on their mechanical fatigue behavior. J. Mech. Behav. Biomed. Mater. 2017, 71, 201–208. [Google Scholar] [CrossRef]
- Alao, A.R.; Stoll, R.; Zhang, Y.; Yin, L. Influence of CAD/CAM milling, sintering and surface treatments on the fatigue behavior of lithium disilicate glass ceramic. J. Mech. Behav. Biomed. Mater. 2021, 113, 104133. [Google Scholar] [CrossRef]
- Chong, K.K.; Palamara, J.; Wong, R.H.; Judge, R.B. Fracture force of cantilevered zirconia frameworks: An in vitro study. J. Prosthet. Dent. 2014, 112, 849–856. [Google Scholar] [CrossRef]
- Jiménez-Melendo, M.; Llena-Blasco, O.; Bruguera, A.; Llena-Blasco, J.; Yáñez-Vico, R.M.; García-Calderón, M.; Vaquero-Aguilar, C.; Velázquez-Cayón, R.; Gutiérrez-Pérez, J.L.; Torres-Lagares, D. Mechanical behavior of single-layer ceramized zirconia abutments for dental implant prosthetic rehabilitation. J. Clin. Exp. Dent. 2014, 6, e485–e490. [Google Scholar] [CrossRef]
- Ghavami Lahiji, M.; Firouzmanesh, M.; Bagheri, H.; Jafarzadeh, T.S.; Razazpour, F.; Behroozibakhsh, M. The effect of thermocycling on the degree of conversion and mechanical properties of a microhybrid dental resin composite. Restor. Dent. Endod. 2018, 43, e26. [Google Scholar] [CrossRef]
- Guarda, G.B.; Correr, A.B.; Gonçalves, L.S.; Costa, A.R.; Borges, G.A.; Sinhoreti, M.A.; Correr-Sobrinho, L. Effects of surface treatments, thermocycling, and cyclic loading on the bond strength of a resin cement bonded to a lithium disilicate glass ceramic. Oper. Dent. 2013, 38, 208–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshahrani, F.A.; Yilmaz, B.; Seidt, J.D.; McGlumphy, E.A.; Brantley, W.A. A load-to-fracture and strain analysis of monolithic zirconia cantilevered frameworks. J. Prosthet. Dent. 2017, 118, 752–758. [Google Scholar] [CrossRef] [Green Version]
- Sondang, P.; Kumagai, H.; Tanaka, E.; Ozaki, H.; Nikawa, H.; Tanne, K.; Hamada, T. Correlation between maximum bite force and craniofacial morphology of young adults in Indonesia. J. Oral Rehabil. 2003, 30, 1109–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, J.; Stafford GHarrison, A. Masticatory function—a review of the literature: I.I.I. Masticatory performance and efficiency. J. Oral Rehabil. 1976, 3, 57–67. [Google Scholar] [CrossRef]
- Waltimo, A.; Könönen, M. A novel bite force recorder and maximal isometric bite force values for healthy young adults. Eur. J. Oral Sci. 1993, 101, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Ohlmann, B.; Marienburg, K.; Gabbert, O.; Hassel, A.; Gilde, H.; Rammelsberg, P. Fracture-load values of all-ceramic cantilevered FPDs with different framework designs. Int. J. Prosthodont. 2009, 22, 49–52. [Google Scholar] [PubMed]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A general power analysis program. Behav. Res. Methods Instrum. Comput. 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Gomes, R.; Bergamo, E.; Bordin, D.; Cury, A. The substitution of the implant and abutment for their analogs in mechanical studies: In vitro and in silico analysis. Mater. Sci. Eng. C 2017, 75, 50–54. [Google Scholar] [CrossRef]
- Zortuk, M.; Bolpaca, P.; Kilic, K.; Ozdemir, E.; Aguloglu, S. Effects of Finger Pressure Applied By Dentists during Cementation of All-Ceramic Crowns. Eur. J. Dent. 2010, 4, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Medina Tirado, J.I.; Nagy, W.W.; Dhuru, V.B.; Ziebert, A.J. The effect of thermocycling on the fracture toughness and hardness of core buildup materials. J. Prosthet. Dent. 2001, 86, 474–480. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cantilever Length | Material Groups | N | Minimum | Maximum | * Mean | Std. Deviation | 95% Confidence Interval for Mean | Anova p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||||
| 7 mm | Group A | 12 | 540.90 | 1022.10 | 810.49 | 137.579 | 723.553 | 898.380 | 0.000 |
| Group B | 12 | 950.70 | 1325.50 | 1137.86 | 127.853 | 1056.326 | 1218.800 | ||
| 10 mm | Group C | 12 | 402.80 | 865.30 | 670.39 | 130.963 | 587.685 | 754.106 | |
| Group D | 12 | 609.40 | 1271.20 | 914.58 | 149.635 | 819.779 | 1009.927 | ||
| Total | 48 | 402.80 | 1325.50 | 883.33 | 217.084 | 820.535 | 946.604 | ||
| Dependent Variable | Groups | Comparison | Mean Difference | * Significance |
|---|---|---|---|---|
| Fracture load | Group-A | Group B | −326.59667 * | 0.000 |
| Group C | 140.07083 | 0.072 | ||
| Group D | −103.88667 | 0.260 | ||
| Group-B | Group A | 326.59667 * | 0.000 | |
| Group C | 466.66750 * | 0.000 | ||
| Group D | 222.71000 * | 0.001 | ||
| Group-C | Group A | −140.07083 | 0.072 | |
| Group B | −466.66750 * | 0.000 | ||
| Group D | −243.95750 * | 0.000 | ||
| Group-D | Group A | 103.88667 | 0.260 | |
| Group B | −222.71000 * | 0.001 | ||
| Group C | 243.95750 * | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshiddi, I.F.; Habib, S.R.; Zafar, M.S.; Bajunaid, S.; Labban, N.; Alsarhan, M. Fracture Load of CAD/CAM Fabricated Cantilever Implant-Supported Zirconia Framework: An In Vitro Study. Molecules 2021, 26, 2259. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082259
Alshiddi IF, Habib SR, Zafar MS, Bajunaid S, Labban N, Alsarhan M. Fracture Load of CAD/CAM Fabricated Cantilever Implant-Supported Zirconia Framework: An In Vitro Study. Molecules. 2021; 26(8):2259. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082259
Chicago/Turabian StyleAlshiddi, Ibraheem F., Syed Rashid Habib, Muhammad Sohail Zafar, Salwa Bajunaid, Nawaf Labban, and Mohammed Alsarhan. 2021. "Fracture Load of CAD/CAM Fabricated Cantilever Implant-Supported Zirconia Framework: An In Vitro Study" Molecules 26, no. 8: 2259. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082259