Population-Based Registry Analysis of Antidiabetics Dispensations: Trend Use in Spain between 2015 and 2018 with Reference to Driving

 ,
, 
 and
and 
Abstract
:1. Introduction
Study Aim
2. Results
3. Discussion
4. Materials and Methods
4.1. Real-World Study Details
4.2. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hostiuc, S.; Negoi, I.; Hostiuc, M. Diabetes and collision risk. A meta-analysis and meta-regression. Int. J. Clin. Pract. 2016, 70, 554–568. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas 2019; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Stork, A.D.M.; van Haeften, T.W.; Veneman, T.F. Diabetes and driving: Desired data, research methods and their pitfalls, current knowledge, and future research. Diabetes Care 2006, 29, 1942–1949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skurtveit, S.; Strøm, H.; Skrivarhaug, T.; Mørland, J.; Bramness, J.G.; Engeland, A. Road traffic accident risk in patients with diabetes mellitus receiving blood glucose-lowering drugs. Prospective follow-up study. Diabet. Med. 2009, 26, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Canada Clinical Practice Guidelines Expert Committee; Houlden, R.L.; Berard, L.; Lakoff, J.M.; Woo, V.; Yale, J.-F. Diabetes and Driving. Can. J. Diabetes 2018, 42 (Suppl. S1), S150–S153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, D.J.; Singh, H.; Lorber, D.; Hermayer, K. Diabetes and driving safety: Science, ethics, legality and practice. Am. J. Med. Sci. 2013, 345, 263–265. [Google Scholar] [CrossRef] [Green Version]
- Laberge-Nadeau, C.; Dionne, G.; Ekoé, J.M.; Hamet, P.; Desjardins, D.; Messier, S.; Maag, U. Impact of diabetes on crash risks of truck-permit holders and commercial drivers. Diabetes Care 2000, 23, 612–617. [Google Scholar] [CrossRef] [Green Version]
- Graveling, A.J.; Frier, B.M. Driving and diabetes: Problems, licensing restrictions and recommendations for safe driving. Clin. Diabetes Endocrinol. 2015, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Inkster, B.; Frier, B.M. Diabetes and driving. Diabetes Obes. Metab. 2013, 15, 775–783. [Google Scholar] [CrossRef]
- Cox, D.J.; Kovatchev, B.P.; Anderson, S.M.; Clarke, W.L.; Gonder-Frederick, L.A. Type 1 Diabetic Drivers With and Without a History of Recurrent Hypoglycemia—Related Driving Mishaps. Diabetes Care 2010, 33, 2430–2435. [Google Scholar] [CrossRef] [Green Version]
- Ma, S.; Zhang, J.; Zeng, X.; Wu, C.; Zhao, G.; Lv, C.; Sun, X. Type 2 diabetes can undermine driving performance of middle-aged male drivers through its deterioration of perceptual and cognitive functions. Accid. Anal. Prev. 2020, 134, 105334. [Google Scholar] [CrossRef]
- UK Hypoglycaemia Study Group. Risk of hypoglycaemia in types 1 and 2 diabetes: Effects of treatment modalities and their duration. Diabetologia 2007, 50, 1140–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signorovitch, J.E.; Macaulay, D.; Diener, M.; Yan, Y.; Wu, E.Q.; Gruenberger, J.-B.; Frier, B.M. Hypoglycaemia and accident risk in people with type 2 diabetes mellitus treated with non-insulin antidiabetes drugs. Diabetes Obes. Metab. 2013, 15, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, D.J.; Gonder-Frederick, L.A.; Kovatchev, B.P.; Julian, D.M.; Clarke, W.L. Progressive hypoglycemia’s impact on driving simulation performance. Occurrence, awareness and correction. Diabetes Care 2000, 23, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilpatrick, E.S.; Rigby, A.S.; Warren, R.E.; Atkin, S.L. Implications of new European Union driving regulations on patients with Type 1 diabetes who participated in the Diabetes Control and Complications Trial. Diabet. Med. 2013, 30, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Simó Miñana, J. Utilización de medicamentos en España y en Europa. Aten. Primaria 2012, 44, 335–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agencia Española del Medicamento y Productos Sanitarios. Informe de Utilización de Medicamentos U/AN/V1/03092015: Utilización de Medicamentos Antidiabéticos en España durante el Periodo 2000–2014; Agencia Española del Medicamento y Productos Sanitarios: Madrid, Spain, 2015. [Google Scholar]
- Ravera, S.; Monteiro, S.P.; de Gier, J.J.; van der Linden, T.; Gómez-Talegón, T.; Álvarez, F.J. A European approach to categorizing medicines for fitness to drive: Outcomes of the DRUID project. Br. J. Clin. Pharmacol. 2012, 74, 920–931. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez-Abejón, E.; Herrera-Gómez, F.; Criado-Espegel, P.; Alvarez, F.J. Use of driving-impairing medicines by a Spanish population: A population-based registry study. BMJ Open 2017, 7. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Gómez, F.; Gutierrez-Abejón, E.; Criado-Espegel, P.; Álvarez, F.J. The Problem of Benzodiazepine Use and Its Extent in the Driver Population: A Population-Based Registry Study. Front. Pharmacol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Gómez, F.; Gutierrez-Abejón, E.; Álvarez, F.J. Antipsychotics in the general population and the driver population: Comparisons from a population-based registry study. Int. Clin. Psychopharmacol. 2019, 34, 184–188. [Google Scholar] [CrossRef]
- Herrera-Gómez, F.; Gutierrez-Abejón, E.; Ayestarán, I.; Criado-Espegel, P.; Álvarez, F.J. The Trends in Opioid Use in Castile and Leon, Spain: A Population-Based Registry Analysis of Dispensations in 2015 to 2018. J. Clin. Med. 2019, 8, 2148. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Abejón, E.; Herrera-Gómez, F.; Criado-Espegel, P.; Álvarez, F.J. Trends in Antidepressants Use in Spain between 2015 and 2018: Analyses from a Population-Based Registry Study with Reference to Driving. Pharmaceuticals 2020, 13, 61. [Google Scholar] [CrossRef] [Green Version]
- Songer, T.J.; Dorsey, R.R. High Risk Characteristics for Motor Vehicle Crashes in Persons with Diabetes by Age. Annu. Proc. Assoc. Adv. Automot. Med. 2006, 50, 335–351. [Google Scholar] [PubMed]
- Nauck, M.A.; Meininger, G.; Sheng, D.; Terranella, L.; Stein, P.P.; Sitagliptin Study 024 Group. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: A randomized, double-blind, non-inferiority trial. Diabetes Obes. Metab. 2007, 9, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Karagiannis, T.; Paschos, P.; Paletas, K.; Matthews, D.R.; Tsapas, A. Dipeptidyl peptidase-4 inhibitors for treatment of type 2 diabetes mellitus in the clinical setting: Systematic review and meta-analysis. BMJ 2012, 344, e1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Ashoor, H.M.; Antony, J.; Beyene, J.; Veroniki, A.A.; Isaranuwatchai, W.; Harrington, A.; Wilson, C.; Tsouros, S.; Soobiah, C.; et al. Safety, effectiveness, and cost effectiveness of long acting versus intermediate acting insulin for patients with type 1 diabetes: Systematic review and network meta-analysis. BMJ 2014, 349, g5459. [Google Scholar] [CrossRef] [Green Version]
- Koepsell, T.D.; Wolf, M.E.; McCloskey, L.; Buchner, D.M.; Louie, D.; Wagner, E.H.; Thompson, R.S. Medical conditions and motor vehicle collision injuries in older adults. J. Am. Geriatr. Soc. 1994, 42, 695–700. [Google Scholar] [CrossRef]
- Cox, D.J.; Penberthy, J.K.; Zrebiec, J.; Weinger, K.; Aikens, J.E.; Frier, B.; Stetson, B.; DeGroot, M.; Trief, P.; Schaechinger, H.; et al. Diabetes and driving mishaps: Frequency and correlations from a multinational survey. Diabetes Care 2003, 26, 2329–2334. [Google Scholar] [CrossRef] [Green Version]
- ECRI. Diabetes and Commercial Motor Vehicle Safety (Federal Motor Carrier Safety Administration); ECRI: Plymouth Meeting, PA, USA, 2011. [Google Scholar]
- Harsch, I.A.; Stocker, S.; Radespiel-Tröger, M.; Hahn, E.G.; Konturek, P.C.; Ficker, J.H.; Lohmann, T. Traffic hypoglycaemias and accidents in patients with diabetes mellitus treated with different antidiabetic regimens. J. Intern. Med. 2002, 252, 352–360. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Gómez, F.; Asensio-González, M.; González-López, A.; Álvarez, F.J. Effects of Intensive Control of Glycemia on Clinical Kidney Outcomes in Type 2 Diabetes Patients Compared with Standard Control: A Meta-Analysis. Front. Pharmacol. 2017, 8, 845. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association; Lorber, D.; Anderson, J.; Arent, S.; Cox, D.J.; Frier, B.M.; Greene, M.A.; Griffin, J.W.; Gross, G.; Hathaway, K.; et al. Diabetes and driving. Diabetes Care 2012, 35 (Suppl. S1), S81–S86. [Google Scholar] [CrossRef] [Green Version]
- Min, T.; Younis, N. Driving and insulin-treated diabetes: Are we aware of changes in the Third European Driving Licence Directive? Diabet. Med. 2016, 33, 553–554. [Google Scholar] [CrossRef] [PubMed]
- Watson, W.A.; Currie, T.; Lemon, J.S.; Gold, A.E. Driving and insulin-treated diabetes: Who knows the rules and recommendations? Pract. Diabetes Int. 2007, 24, 201–206. [Google Scholar] [CrossRef]
- Sigona, N.; Williams, K.G. Driving under the influence, public policy, and pharmacy practice. J. Pharm. Pract. 2015, 28, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Legrand, S.-A.; Boets, S.; Meesmann, U.; Verstraete, A.G. Medicines and driving: Evaluation of training and software support for patient counselling by pharmacists. Int. J. Clin. Pharm. 2012, 34, 633–643. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M.; RECORD Working Committee. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes-2012. Diabetes Care 2012, 35 (Suppl. S1), S11–S63. [Google Scholar] [CrossRef] [Green Version]
- Fierro, I.; Gómez-Talegón, T.; Alvarez, F.J. The Spanish pictogram on medicines and driving: The population’s comprehension of and attitudes towards its use on medication packaging. Accid. Anal. Prev. 2013, 50, 1056–1061. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Global Status Report on Road Safety 2018. Available online: https://www.who.int/violence_injury_prevention/road_safety_status/2018/en/ (accessed on 19 July 2020).




{kind=link}
{kind=link}
{kind=link}
| Gender | Population Using Antidiabetics % (95CI) | Drivers Using Antidiabetics % (95CI) | ||||
|---|---|---|---|---|---|---|
| Total | Insulins | Oral Antidiabetics | Total | Insulins | Oral Antidiabetics | |
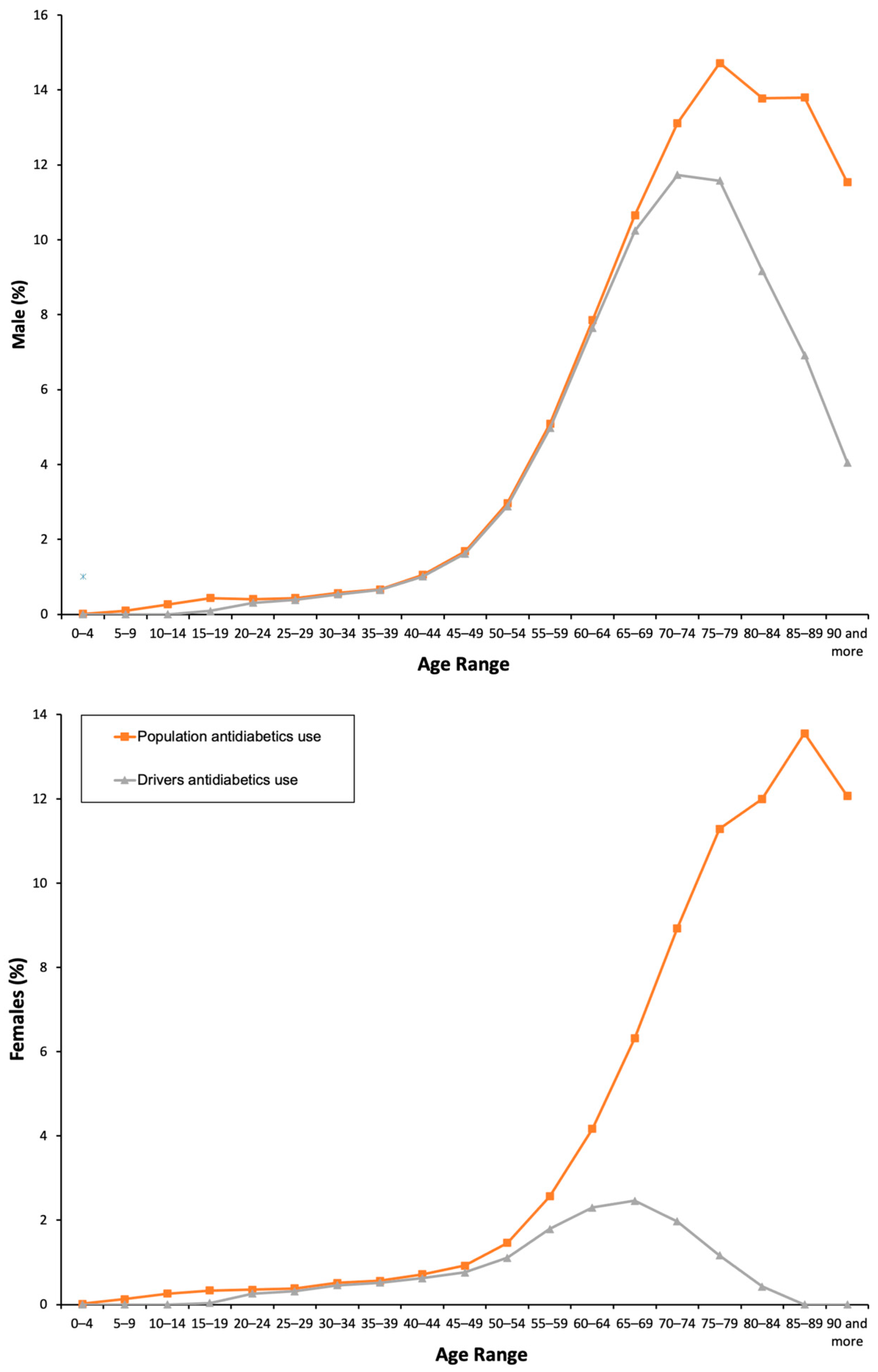
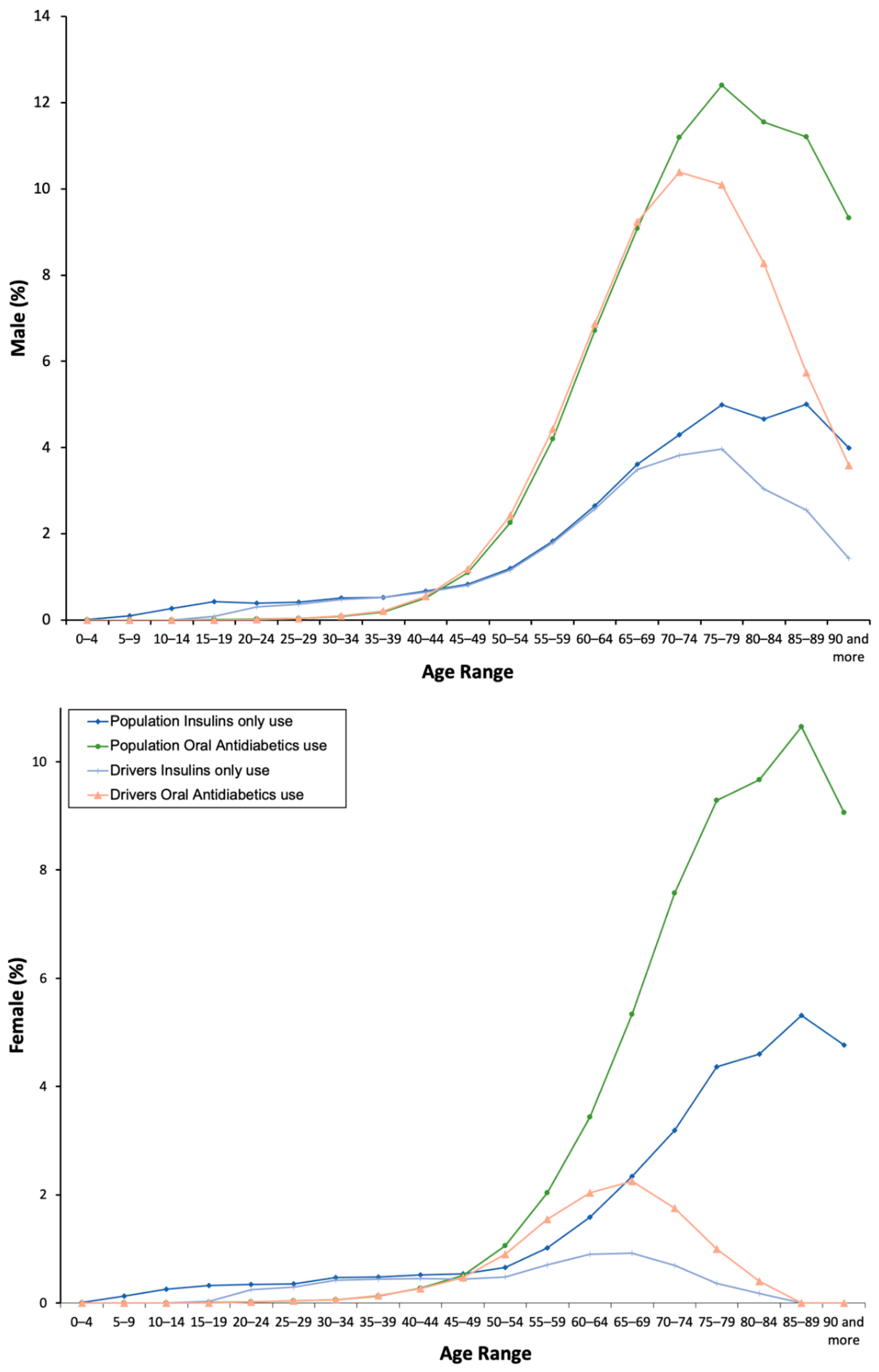
| Total | 3.98 (3.95–4) | 1.56 (1.54–1.58) | 3.13 (3.1–3.15) | 2.92 (2.89–2.94) | 1.15 (1.13–1.16) | 2.44 (2.42–2.47) |
| Male | 4.35 (4.32–4.39) | 1.64 (1.61–1.66) | 3.48 (3.44–3.51) | 4.22 (4.17–4.26) | 1.58 (1.55–1.61) | 3.62 (3.58–3.66) |
| Female | 3.61 (3.58–3.65) | 1.49 (1.47–1.51) | 2.79 (2.76–2.82) | 0.98 (0.96–1.01) | 0.5 (0.49–0.52) | 0.7 (0.68–0.73) |
| Χ2 = 18,831.883; p = 0.001 | Χ2 = 7157.779; p = 0.001 | Χ2 = 14,785.013; p = 0.001 | Χ2 = 17,826.133; p = 0.001 | Χ2 = 8420.777; p = 0.001 | Χ2 = 9520.731; p = 0.001 | |
| Chronic use | ||||||
| Total | 3.93 (3.9–3.95) | 1.56 (1.54–1.58) | 3.06 (3.04–3.09) | 2.88 (2.85–2.91) | 1.15 (1.13–1.16) | 2.23 (2.21–2.26) |
| Male | 4.3 (4.27–4.34) | 1.63 (1.61–1.66) | 3.41 (3.38–3.45) | 4.17 (4.12–4.21) | 1.58 (1.55–1.6) | 3.32 (3.28–3.35) |
| Female | 3.57 (3.53–3.6) | 1.49 (1.47–1.51) | 2.73 (2.7–2.76) | 0.97 (0.94–0.99) | 0.5 (0.48–0.52) | 0.61 (0.59–0.63) |
| Χ2 = 18,734.605; p = 0.001 | Χ2 = 7158.431; p = 0.001 | Χ2 = 14,639.994; p = 0.001 | Χ2 = 17,630.868; p = 0.001 | Χ2 = 8420.042; p = 0.001 | Χ2 = 9172.203; p = 0.001 | |
| Average of driving impairing medicines. Population antidiabetics use | ||||||
| Total | 2.5 ± 1.86 | 2.63 ± 1.95 | 2.48 ± 1.84 | 2.25 ± 1.77 | 2.38 ± 1.88 | 2.22 ± 1.73 |
| Male | 2.19 ± 1.68 | 2.33 ± 1.79 | 2.16 ± 1.65 | 2.17 ± 1.7 | 2.31 ± 1.81 | 2.13 ± 1.65 |
| Female | 2.76 ± 1.96 | 2.87 ± 2.04 | 2.75 ± 1.95 | 2.68 ± 2.07 | 2.68 ± 2.11 | 2.74 ± 2.06 |
| t = −74.63; p = 0.001 | t = −42.45; p = 0.001 | t = −69.96; p = 0.001 | t = −27.53; p = 0.001 | t = −13.22; p = 0.001 | t = −27.94; p = 0.001 | |
| Gender | Population Using Antidiabetics % (95CI) | Drivers Using Antidiabetics % (95CI) | ||||||
|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2015 | 2016 | 2017 | 2018 | |
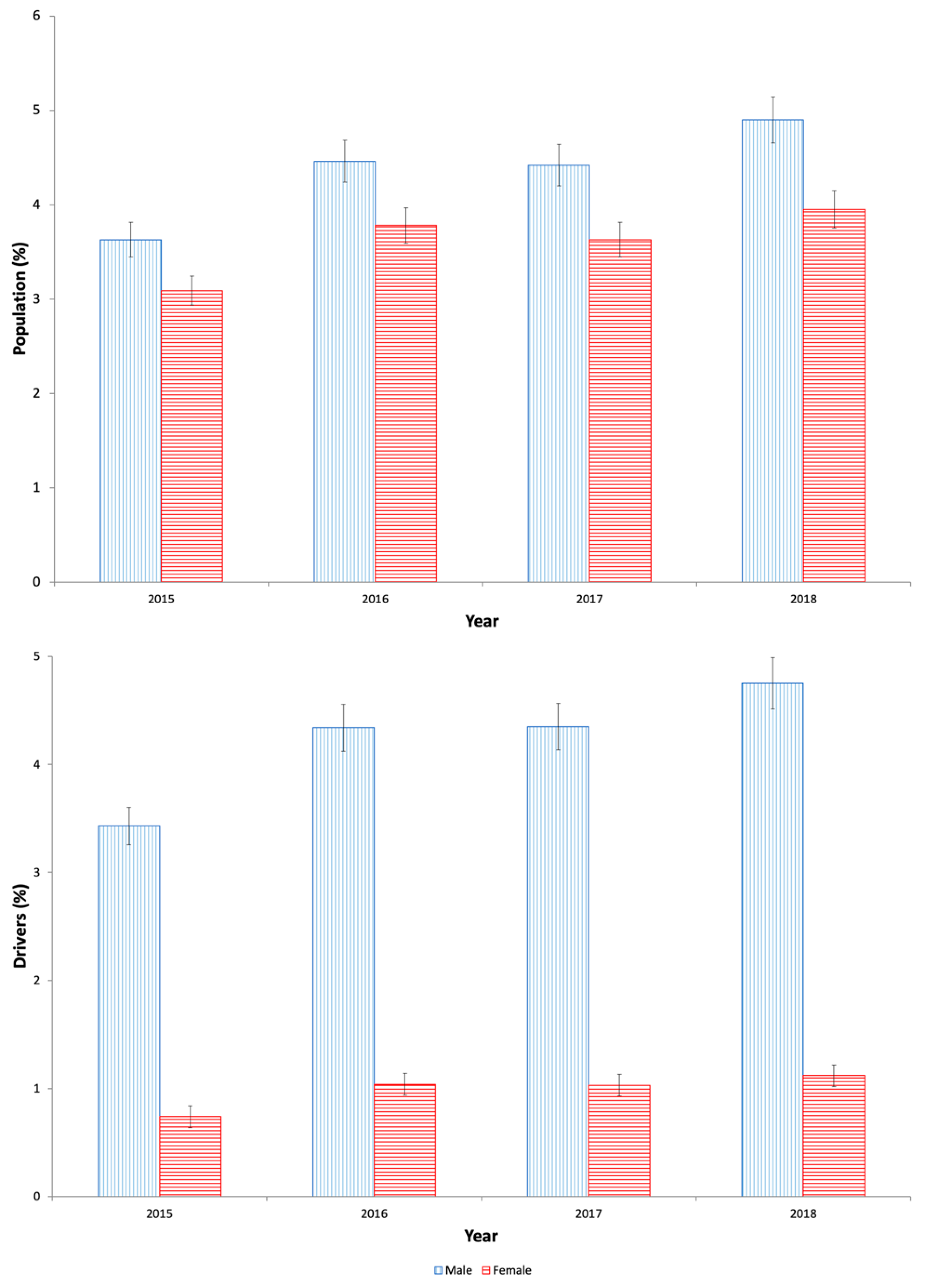
| Total | 3.36 (3.33–3.38) | 4.11 (4.09–4.14) | 4.02 (3.99–4.04) | 4.42 (4.39–4.45) | 2.36 (2.34–2.39) | 3.02 (2.99–3.05) | 3.01 (2.98–3.04) | 3.28 (3.25–3.31) |
| Male | 3.63 (3.6–3.67) | 4.46 (4.42–4.5) | 4.42 (4.39–4.46) | 4.9 (4.86–4.94) | 3.43 (3.39–3.47) | 4.34 (4.3–4.38) | 4.35 (4.3–4.39) | 4.75 (4.7–4.79) |
| Female | 3.09 (3.06–3.12) | 3.78 (3.74–3.81) | 3.63 (3.6–3.66) | 3.95 (3.92–3.99) | 0.74 (0.72–0.76) | 1.04 (1.01–1.06) | 1.03 (1–1.05) | 1.12 (1.1–1.15) |
| Χ2 = 4070.524; p = 0.001 | Χ2 = 4863.585; p = 0.001 | Χ2 = 4741.491; p = 0.001 | Χ2 = 5184.767; p = 0.001 | Χ2 = 4160.909; p = 0.001 | Χ2 = 4389.486; p = 0.001 | Χ2 = 4570.11; p = 0.001 | Χ2 = 4805.053; p = 0.001 | |
| Type of antidiabetic | ||||||||
| Insulins | ||||||||
| Total | 1.31 (1.29–1.32) | 1.65 (1.64–1.67) | 1.57 (1.55–1.58) | 1.72 (1.7–1.74) | 0.95 (0.94–0.97) | 1.21 (1.19–1.23) | 1.17 (1.15–1.18) | 1.26 (1.24–1.28) |
| Male | 1.36 (1.34–1.38) | 1.72 (1.69–1.74) | 1.65 (1.62–1.67) | 1.82 (1.79–1.84) | 1.3 (1.28–1.33) | 1.66 (1.64–1.69) | 1.61 (1.58–1.63) | 1.74 (1.71–1.77) |
| Female | 1.26 (1.24–1.28) | 1.59 (1.57–1.61) | 1.49 (1.46–1.51) | 1.62 (1.6–1.64) | 0.42 (0.41–0.44) | 0.52 (0.51–0.54) | 0.51 (0.49–0.53) | 0.56 (0.54–0.58) |
| Χ2 = 1518.236; p = 0.001 | Χ2 = 1988.255; p = 0.001 | Χ2 = 1785.798; p = 0.001 | Χ2 = 1898.464; p = 0.001 | Χ2 = 1911.783; p = 0.001 | Χ2 = 2146.022; p = 0.001 | Χ2 = 2202.878; p = 0.001 | Χ2 = 2200.603; p = 0.001 | |
| Oral antidiabetic | ||||||||
| Total | 2.59 (2.57–2.61) | 3.19 (3.16–3.21) | 3.19 (3.16–3.21) | 3.55 (3.52–3.57) | 1.78 (1.76–1.8) | 2.33 (2.31–2.36) | 2.38 (2.35–2.4) | 2.62 (2.59–2.65) |
| Male | 2.84 (2.81–2.87) | 3.51 (3.48–3.54) | 3.56 (3.53–3.6) | 4 (3.97–4.04) | 2.67 (2.63–2.7) | 3.43 (3.4–3.47) | 3.52 (3.48–3.56) | 3.9 (3.85–3.94) |
| Female | 2.34 (2.32–2.37) | 2.87 (2.84–2.9) | 2.82 (2.8–2.85) | 3.11 (3.08–3.14) | 0.42 (0.41–0.44) | 0.68 (0.66–0.7) | 0.68 (0.66–0.7) | 0.75 (0.73–0.77) |
| Χ2 = 3198.26; p = 0.001 | Χ2 = 3687.492; p = 0.001 | Χ2 = 3749.531; p = 0.001 | Χ2 = 4167.533; p = 0.001 | Χ2 = 1910.429; p = 0.001 | Χ2 = 2355.727; p = 0.001 | Χ2 = 2541.26; p = 0.001 | Χ2 = 2723.007; p = 0.001 | |
| Average of driving impairing medicines; Population antidiabetics use | ||||||||
| Total | 2.5 ± 1.88 | 2.53 ± 1.89 | 2.47 ± 1.84 | 2.51 ± 1.83 | 2.22 ± 1.75 | 2.28 ± 1.81 | 2.23 ± 1.75 | 2.28 ± 1.76 |
| Male | 2.16 ± 1.66 | 2.23 ± 1.73 | 2.16 ± 1.66 | 2.22 ± 1.68 | 2.14 ± 1.68 | 2.2 ± 1.74 | 2.14 ± 1.67 | 2.2 ± 1.69 |
| Female | 2.77 ± 1.99 | 2.78 ± 1.98 | 2.73 ± 1.94 | 2.75 ± 1.92 | 2.69 ± 2.09 | 2.68 ± 2.09 | 2.67 ± 2.08 | 2.69 ± 2.02 |
| t = −37.42; p = 0.001 | t = −36.63; p = 0.001 | t = −37.99; p = 0.001 | t = −37.53; p = 0.001 | t = −12.4; p = 0.001 | t = −13.15; p = 0.001 | t = −14.61; p = 0.001 | t = −14.77; p = 0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Abejón, E.; Criado-Espegel, P.; Herrera-Gómez, F.; Álvarez, F.J. Population-Based Registry Analysis of Antidiabetics Dispensations: Trend Use in Spain between 2015 and 2018 with Reference to Driving. Pharmaceuticals 2020, 13, 165. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080165
Gutiérrez-Abejón E, Criado-Espegel P, Herrera-Gómez F, Álvarez FJ. Population-Based Registry Analysis of Antidiabetics Dispensations: Trend Use in Spain between 2015 and 2018 with Reference to Driving. Pharmaceuticals. 2020; 13(8):165. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080165
Chicago/Turabian StyleGutiérrez-Abejón, Eduardo, Paloma Criado-Espegel, Francisco Herrera-Gómez, and F. Javier Álvarez. 2020. "Population-Based Registry Analysis of Antidiabetics Dispensations: Trend Use in Spain between 2015 and 2018 with Reference to Driving" Pharmaceuticals 13, no. 8: 165. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080165