
Characterization and Applications of Colloidal Systems as Versatile Drug Delivery Carriers for Parenteral Formulations




Abstract
:1. Introduction
2. Discussion
2.1. Necessity and Potential of Biphasic Colloidal Carriers in Parenteral Drug Delivery
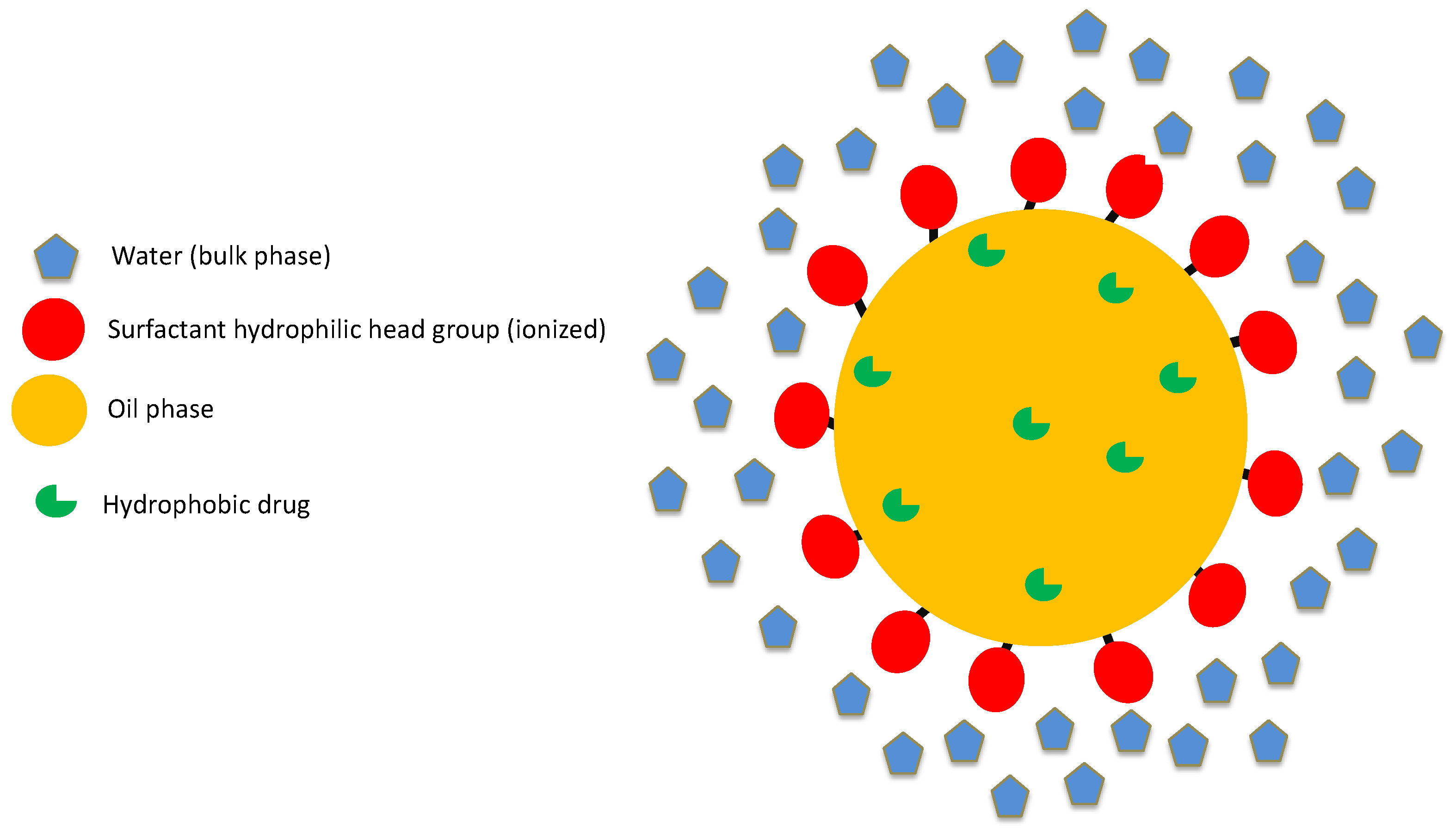
2.2. Structure of Lipid-Based Biphasic Colloidal Systems
2.3. Structure of Nanoparticulate Systems
2.4. FDA Perspective on Excipients
- Drug-excipient compatibility.
- Compatibility of the excipient with manufacturing process and container–closure system.
- Excipient impact on quality, safety, and effectiveness of the drug product.
- Route of administration.
- Dose volume and intended use of the drug product: single versus multiple dose.
- New chemical excipients: A full safety evaluation program is required for these excipients. A drug master file (DMF) must be filed with the FDA for a new excipient. The DMF contains relevant safety information.
- Existing chemical excipients—first use in man: Animal safety data are available for this class of excipients. Additional safety information is required when there is a change in dosage form, route of administration, higher dose, etc.
- New modifications or combinations of existing excipients: This class of excipients indicate a physical reaction and not a chemical reaction. Thus, no additional safety evaluation is necessary.
2.5. Physico-Chemical Barriers in Development of Submicron Drug Delivery Systems
3. Scientific and Regulatory Considerations for Approval of Biphasic Colloidal Systems
- Comprehensive comparison of physico-chemical characterization of at least three batches of test and reference products.
- In-vivo studies to demonstrate BE.
3.1. Critical Quality Attributes of Colloidal Drug Delivery Systems
3.1.1. Particle Size Distribution
3.1.2. In-vitro Dissolution Test
3.1.3. Amorphous/Crystalline Content
3.1.4. Rheology and Sterility
4. Applications of Colloidal Carriers
4.1. Total Parenteral Nutrition
4.2. Vaccine Delivery
4.3. Long-Acting Injectable (LAI) Therapy
4.4. Anti-Cancer Drugs and Diagnostic Agents
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Preparation by a size-reduction technique. Int. J. Pharm. 1998, 160, 229–237.
- Müller, R.H.; Jacobs, C.; Kayser, O. Nanosuspensions as particulate drug formulations in therapy: Rationale for development and what we can expect for the future. Adv. Drug Deliv. Rev. 2001, 47, 3–19. [Google Scholar] [CrossRef]
- Date, A.A.; Nagarsenker, M. Parenteral microemulsions: An overview. Int. J. Pharm. 2008, 355, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Marti-Mestres, G.; Nielloud, F. Emulsions in health care applications—An overview. J. Dispers. Sci. Technol. 2002, 23, 419–439. [Google Scholar] [CrossRef]
- Patravale, V.B.; Date, A.A.; Kulkarni, R.M. Nanosuspensions: A promising drug delivery strategy. J. Pharm. Pharmacol. 2004, 56, 827–840. [Google Scholar] [CrossRef] [Green Version]
- Morais, J.M.; Burgess, D.J. Micro-and nanoemulsions (controlled release parenteral drug delivery systems). In Long Acting Injections and Implants; Springer: Berlin/Heidelberg, Germany, 2012; pp. 221–238. [Google Scholar]
- Giri, T.K.; Goswami, N.G.; Jha, V.K. Prospective and challenges of micro-emulsion as a novel carrier for drug delivery. J. PharmaSciTech 2013, 2, 56–61. [Google Scholar]
- Rhee, Y.-S.; Park, C.; Nam, T.-Y.; Shin, Y.-S.; Chi, S.-C.; Park, E.-S. Formulation of parenteral microemulsion containing itraconazole. Arch. Pharmacal Res. 2007, 30, 114–123. [Google Scholar] [CrossRef]
- Nesamony, J.; Zachar, C.L.; Jung, R.; Williams, F.E.; Nauli, S. Preparation, characterization, sterility validation, and in vitro cell toxicity studies of microemulsions possessing potential parenteral applications. Drug Dev. Ind. Pharm. 2012, 39, 240–251. [Google Scholar] [CrossRef]
- Kolluru, L.P.; Chandran, T.; Shastri, P.N.; Rizvi, S.A.; D’Souza, M.J. Development and evaluation of polycaprolactone based docetaxel nanoparticle formulation for targeted breast cancer therapy. J. Nanopart. Res. 2020, 22, 372. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Z.; Zhang, N.; Miao, L.; Huang, G. Development of etoposide-loaded bovine serum albumin nanosuspensions for parenteral delivery. Drug Deliv. 2014, 22, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Tian, X.; Li, H.; Zhang, D.; Liu, G.; Jia, L.; Zheng, D.; Shen, J.; Shen, Y.; Zhang, Q. Nanosuspension for parenteral delivery of a p-terphenyl derivative: Preparation, characteristics and pharmacokinetic studies. Colloids Surfaces B Biointerfaces 2013, 108, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Ganta, S.; Talekar, M.; Singh, A.; Coleman, T.P.; Amiji, M. Nanoemulsions in Translational Research—Opportunities and Challenges in Targeted Cancer Therapy. AAPS PharmSciTech 2014, 15, 694–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, A.C.; Schechter, R.S. The theory of diffusion in microemulsion. J. Colloid Interface Sci. 1987, 120, 56–63. [Google Scholar] [CrossRef]
- Muzaffar, F.; Singh, U.; Chauhan, L. Review on microemulsion as futuristic drug delivery. Int. J. Pharm. Pharm. Sci. 2013, 5, 39–53. [Google Scholar]
- Kahlweit, M.; Strey, R.; Busse, G. Microemulsions: A qualitative thermodynamic approach. J. Phys. Chem. 1990, 94, 3881–3894. [Google Scholar] [CrossRef]
- Ghosh, P.; Murthy, R. Microemulsions: A potential drug delivery system. Curr. Drug Deliv. 2006, 3, 167–180. [Google Scholar] [CrossRef]
- Nigade, P.M.; Patil, S.L.; Tiwari, S.S. Self emulsifying drug delivery system (SEDDS): A review. Int. J. Pharm. Biol. Sci. 2012, 2, 42–52. [Google Scholar]
- Lawrence, M.J.; Rees, G.D. Microemulsion-based media as novel drug delivery systems. Adv. Drug Deliv. Rev. 2000, 45, 89–121. [Google Scholar] [CrossRef]
- Kumar, S.; Burgess, D.J. Nanosuspensions. In Long Acting Injections and Implants; Springer: Berlin/Heidelberg, Germany, 2012; pp. 239–261. [Google Scholar]
- Martinez, M.N.; Khan, M.A. Regulatory Issues and Challenges Associated with the Development of Per-formance Specifications for Modified Release Parenteral Products. In Long Acting Injections and Implants; Springer: Berlin/Heidelberg, Germany, 2012; pp. 505–535. [Google Scholar]
- Pramanick, S.; Singodia, D.; Chandel, V. Excipient selection in parenteral formulation development. Pharma Times 2013, 45, 65–77. [Google Scholar]
- Shrestha, H.; Bala, R.; Arora, S. Lipid-Based Drug Delivery Systems. J. Pharm. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Bansal, M.; Visht, S.; Sharma, P.K.; Kulkarni, G.T. Nanoemulsion: A new concept of delivery system. Chron. Young Sci. 2010, 1, 2. [Google Scholar]
- Tadros, T.F. Emulsion Science and Technology: A General Introduction; Wiley-VCH: Weinheim, Germany, 2009. [Google Scholar]
- Wang, Y.; Zheng, Y.; Zhang, L.; Wang, Q.; Zhang, D. Stability of nanosuspensions in drug delivery. J. Control. Release 2013, 172, 1126–1141. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.S.; York, P.; Blagden, N. Preparation of hydrocortisone nanosuspension through a bottom-up nanoprecipitation technique using microfluidic reactors. Int. J. Pharm. 2009, 375, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.W.; Mitchnick, M. Early-Stage Formulation Considerations. Curr. Protoc. Chem. Biol. 2017, 9, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Rahman, Z.; Charoo, N.A.; Akhter, S.; Beg, S.; Reddy, I.K.; Khan, M.A. Nanotechnology-based drug products: Science and regulatory considerations. In Nanoscale Fabrication, Optimization, Scale-Up and Biological Aspects of Pharmaceutical Nanotechnology; Elsevier: Amsterdam, The Netherlands, 2018; pp. 619–655. [Google Scholar]
- Zheng, N.; Sun, D.D.; Zou, P.; Jiang, W. Scientific and regulatory considerations for generic complex drug products containing na-nomaterials. AAPS J. 2017, 19, 619–631. [Google Scholar] [CrossRef]
- Benita, S.; Levy, M. Submicron emulsions as colloidal drug carriers for intravenous administration: Comprehensive physicochemical characterization. J. Pharm. Sci. 1993, 82, 1069–1079. [Google Scholar] [CrossRef]
- Ha, W.N.; Bentz, D.P.; Kahler, B.; Walsh, L.J. D90: The Strongest Contributor to Setting Time in Mineral Trioxide Aggregate and Portland Cement. J. Endod. 2015, 41, 1146–1150. [Google Scholar] [CrossRef]
- Shen, J.; Burgess, D.J. In vitro dissolution testing strategies for nanoparticulate drug delivery systems: Recent developments and challenges. Drug Deliv. Transl. Res. 2013, 3, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Dash, S.; Murthy, P.N.; Nath, L.; Chowdhury, P. Kinetic modeling on drug release from controlled drug delivery systems. Acta Pol. Pharm. 2010, 67, 217–223. [Google Scholar]
- Agrawal, O.P.; Agrawal, S. An overview of new drug delivery system: Microemulsion. Asian J. Pharm. Sci. Tech. 2012, 2, 5–12. [Google Scholar]
- Nesamony, J.; Shah, I.S.; Kalra, A.; Jung, R. Nebulized oil-in-water nanoemulsion mists for pulmonary delivery: Development, physico-chemical characterization andin vitroevaluation. Drug Dev. Ind. Pharm. 2013, 40, 1253–1263. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Jensen, G.L.; Koletzko, B.V.; Singer, P.; Wanten, G.J.A. Lipid emulsions in parenteral nutrition of intensive care patients: Current thinking and future directions. Intensiv. Care Med. 2010, 36, 735–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boullata, J.I.; Berlana, D.; Pietka, M.; Klek, S.; Martindale, R. Use of Intravenous Lipid Emulsions with Parenteral Nutrition: Practical Handling Aspects. J. Parenter. Enter. Nutr. 2020, 44, S74–S81. [Google Scholar] [CrossRef] [PubMed]
- Shahiwala, A.; Vyas, T.K.; Amiji, M. Nanocarriers for systemic and mucosal vaccine delivery. Recent Patents Drug Deliv. Formul. 2007, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gregory, A.E.; Titball, R.W.; Ewilliamson, D. Vaccine delivery using nanoparticles. Front. Cell. Infect. Microbiol. 2013, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Souza, B.D.; Shastri, P.N.; Hammons, G.; Kim, E.; Kolluru, L.P.; Carlone, G.M.; Rajam, G.; Souza, M.J.D. Immune-potentiation of Pneumococcal Capsular Polysaccharide Antigen using Albumin Microparticles. J. Pharmacovigil. 2018, 6, 1–6. [Google Scholar] [CrossRef]
- D’Souza, M.J. Microparticulate Formulation for a Pneumococcal Capsular Polysaccharide Antigen. In Nanoparticulate Vaccine Delivery Systems; Jenny Stanford Publishing: Temasek Avenue, Singapore, 2015; pp. 136–147. [Google Scholar]
- Baker, J.; Bielinska, A.; Myc, A. Compositions and Methods for Human Immunodeficiency Virus Vaccination. U.S. Patent 11/786,855, 2008. [Google Scholar]
- Nkanga, C.I.; Fisch, A.; Rad-Malekshahi, M.; Romic, M.D.; Kittel, B.; Ullrich, T.; Wang, J.; Krause, R.W.M.; Adler, S.; Lammers, T.; et al. Clinically established biodegradable long acting injectables: An industry perspective. Adv. Drug Deliv. Rev. 2020, 167, 19–46. [Google Scholar] [CrossRef]
- Owen, A.; Rannard, S. Strengths, weaknesses, opportunities and challenges for long acting injectable therapies: Insights for applications in HIV therapy. Adv. Drug Deliv. Rev. 2016, 103, 144–156. [Google Scholar] [CrossRef] [Green Version]
- Kolluru, L.P.; Rizvi, S.A.A.; D’Souza, M.; D’Souza, M.J. Formulation development of albumin based theragnostic nanoparticles as a potential delivery system for tumor targeting. J. Drug Target. 2012, 21, 77–86. [Google Scholar] [CrossRef]


{kind=link}
| Excipient | Function | Route of Administration | Maximum Potency Per Unit Dose |
|---|---|---|---|
| Chlorobutanol | Antimicrobial preservative | Parenteral | 0.5% w/v |
| Methylparaben | Antimicrobial preservative | IV | 5% w/v |
| Bisulfite sodium | Antioxidant | IV | 50 mg |
| Polyethyleneglycol 300 | Co-solvent | IM | 50% w/v |
| Disodium EDTA | Chelating agent | IM | 10% w/v |
| Sorbitan monolaurate | Surfactant | IM | 0.38% w/v |
| Castor oil | Lipid phase | IM | 30% w/v |
| Monothioglycerol | Tonicity modifier | IM | 0.5% w/v |
| Dosage Form | Sponsor | Indication | Active Ingredient | Route of Administration |
|---|---|---|---|---|
| Paclitaxel Injection, USP | Grand Pharma Ltd. | Anti-tumor | Paclitaxel | Intravenous |
| Diprivan® | Fresenius Kabi USA LLC | General anesthetic and sedation drug | Propofol | Intravenous |
| ZYPREXA® Intramuscular Injection | Lilly | Treatment of Schizophrenia | Olanzapine | Intramuscular |
| Phytonadione Injection, USP | International Medication Systems Ltd. | Treatment of Hypoprothrombinemia | Phytonadione | Intravenous/Intramuscular |
| Abraxane® for Injectable Suspension, USP | Abraxis Bioscience | Treatment of Metastatic Breast Cancer | Paclitaxel | Intravenous |
| Invega sustenna® | Janssen Pharms | Antipyschotic | Paliperidone Palmitate | Intramuscular |
| Methylprednisolone Acetate Injectable Suspension, USP | Sandoz Inc. | Anti-inflammatory | Methylprednisolone Acetate | Intramuscular, Intraarticular, Intralesional |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolluru, L.P.; Atre, P.; Rizvi, S.A.A. Characterization and Applications of Colloidal Systems as Versatile Drug Delivery Carriers for Parenteral Formulations. Pharmaceuticals 2021, 14, 108. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020108
Kolluru LP, Atre P, Rizvi SAA. Characterization and Applications of Colloidal Systems as Versatile Drug Delivery Carriers for Parenteral Formulations. Pharmaceuticals. 2021; 14(2):108. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020108
Chicago/Turabian StyleKolluru, Lakshmi Prasanna, Prachi Atre, and Syed A. A. Rizvi. 2021. "Characterization and Applications of Colloidal Systems as Versatile Drug Delivery Carriers for Parenteral Formulations" Pharmaceuticals 14, no. 2: 108. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020108