
Assessment of Novel Inhaler Technique Reminder Labels in Image Format on the Correct Demonstration of Inhaler Technique Skills in Asthma: A Single-Blinded Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Results
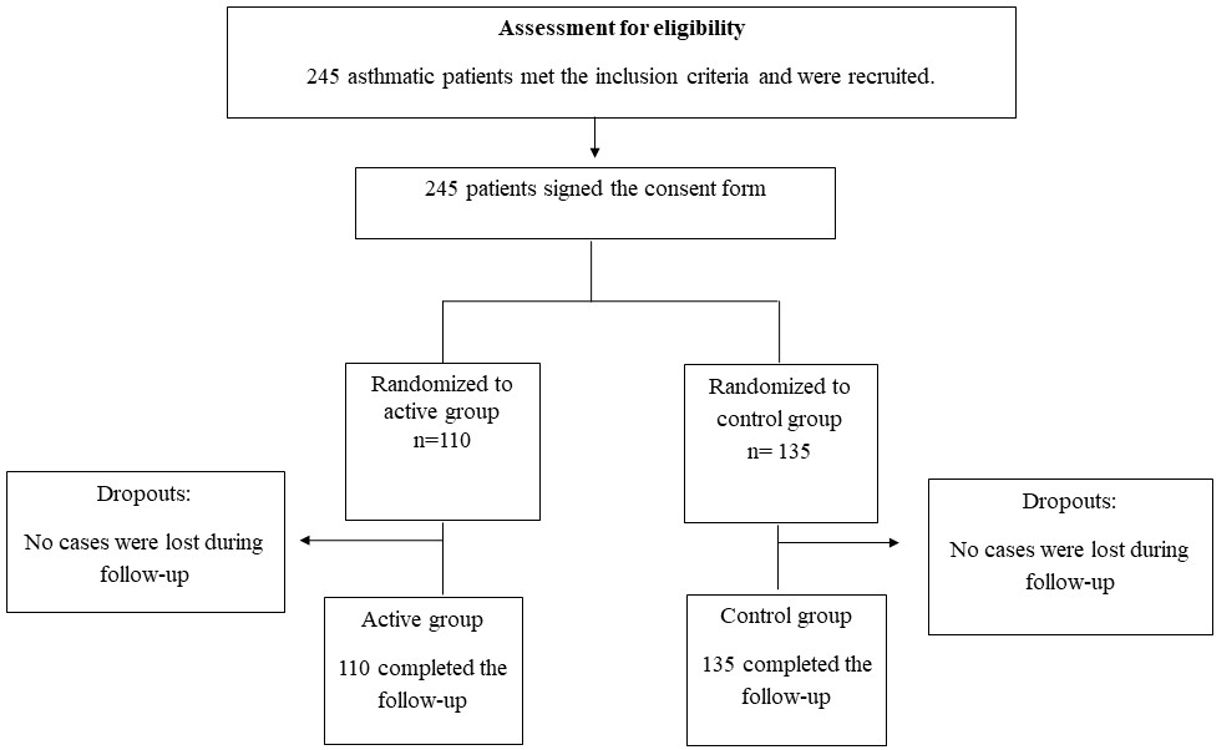
2.1. Basic Demographic Information for the Active and Control Groups
2.2. Inhaler Technique Assessment for the Active and Control Groups
2.3. ACT Assessment
2.4. Factors Associated with Inhaler Technique Scores and ACT Scores at Follow-Up
2.5. PEF and FEV Outcomes
3. Discussion
4. Materials and Methods
4.1. Baseline Assessments
4.2. Intervention Delivered to the Active and Control Groups
4.3. Statistical Analysis
4.4. Sample Size Calculations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Initiative For Asthma. 2020 GINA Report, Global Strategy for Asthma Management and Prevention; The Global Initiative for Asthma: Fontana, WI, USA, 2020. [Google Scholar]
- CDC.gov. CDC—Asthma. 2019. Available online: https://www.cdc.gov/nchs/fastats/asthma.htm (accessed on 12 October 2020).
- Dalibalta, S.; Samara, F.; Qadri, H.; Adouchana, H.J.R. Potential causes of asthma in the United Arab Emirates: Drawing insights from the Arabian Gulf. Rev. Environ. Health 2018, 33, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Bener, A.; Abdulrazzaq, Y.; Al-Mutawwa, J.; Debuse, P.J.H. Genetic and environmental factors associated with asthma. Hum. Biol. 1996, 68, 405–414. [Google Scholar] [PubMed]
- Plaza Moral, V.; Giner Donaire, J. Inhaled therapy in asthma. Med. Clin. 2016, 146, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Lavorini, F.; Mannini, C.; Chellini, E.J.E.R. Challenges of inhaler use in the treatment of asthma and chronic obstructive pulmonary disease. EMJ Respir. 2015, 3, 98–105. [Google Scholar]
- Capstick, T.G.; Clifton, I.J. Inhaler technique and training in people with chronic obstructive pulmonary disease and asthma. Expert Rev. Respir. Med. 2012, 6, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.L.; Hardwell, A.; McKnight, E.; Holmes, J.J. Asthma patients’ inability to use a pressurised metered-dose inhaler (pMDI) correctly correlates with poor asthma control as defined by the global initiative for asthma (GINA) strategy: A retrospective analysis. Prim. Care Respir. J. 2013, 22, 406–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, S.F.; O’Mahony, M.S.; Steward, J.A.; Breay, P.; Burr, M.L. Inhaler technique in older people in the community. Age Ageing 2004, 33, 185–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basheti, I.A.; Armour, C.L.; Bosnic-Anticevich, S.Z.; Reddel, H.K. Evaluation of a novel educational strategy, including inhaler-based reminder labels, to improve asthma inhaler technique. Patient Educ. Couns. 2008, 72, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Basheti, I.A.; Obeidat, N.M.; Reddel, H.K. Effect of novel inhaler technique reminder labels on the retention of inhaler technique skills in asthma: A single-blind randomized controlled trial. NPJ Prim. Care Respir. Med. 2017, 27, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basheti, I.A.; Reddel, H.K.; Armour, C.L.; Bosnic-Anticevich, S.Z. Improved asthma outcomes with a simple inhaler technique intervention by community pharmacists. J. Allergy Clin. Immunol. 2007, 119, 1537–1538. [Google Scholar] [CrossRef] [PubMed]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Basheti, I.A.; Bosnic-Anticevich, S.Z.; Armour, C.L.; Reddel, H.K. Checklists for Powder Inhaler Technique: A Review and Recommendations. Respir. Care 2014, 59, 1140–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lababidi, H.; Hijaoui, A.; Zarzour, M. Validation of the Arabic version of the asthma control test. Ann. Thorac. Med. 2008, 3, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Bosnic-Anticevich, S.Z.; Sinha, H.; So, S.; Reddel, H.K. Metered-dose inhaler technique: The effect of two educational interventions delivered in community pharmacy over time. J. Asthma 2010, 47, 251–256. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | All Patients (n = 245) | |||||||
|---|---|---|---|---|---|---|---|---|
| All | TH | ACC | pMDI | |||||
| Active (n = 110) | Control (n = 135) | Active (n = 42) | Control (n = 51) | Active (n = 39) | Control (n = 31) | Active (n = 29) | Control (n = 29) | |
| Age | ||||||||
| mean ± SD | 43.3 ± 16.5 | 49.6 ± 18 | 47 ± 15.2 | 49.7 ± 16.3 | 44.9 ± 17.6 | 46.6 ± 15.8 | 35.6 ± 15 | 35.6 ± 15 |
| Height (cm) | ||||||||
| mean ± SD | 160.4 ± 12.4 | 162 ± 10 | 158.7 ± 15.7 | 162 ± 10 | 159.2 ± 9.8 | 161.4 ± 10 | 164.6 ± 9.2 | 164.6 ± 9.2 |
| Weight (Kg) | ||||||||
| mean ± SD | 77.6 ± 18.8 | 79.4 ± 17.4 | 78.2 ± 19.3 | 77.6 ± 17.7 | 75.5 ± 18.8 | 82.3 ± 16.3 | 79.5 ± 18.4 | 79.5 ± 18.4 |
| BMI | ||||||||
| mean ± SD | 30.3 ± 7.7 | 30.4 ± 7 | 30.4 ± 7 | 29.6 ± 7.4 | 30.7 ± 8.6 | 31.7 ± 7 | 29.6 ± 7.5 | 29.6 ± 7.5 |
| Gender | ||||||||
| Male n (%) | 36 (43.4%) | 47 (56.6%) | 13 (40.6%) | 19 (59.4%) | 9 (52.9%) | 8 (47.1%) | 14 (41.2%) | 14 (41.2%) |
| Female n (%) | 74 (45.7%) | 88 (54.3%) | 29 (47.5%) | 32 (52.5%) | 30 (56.6%) | 23 (43.4%) | 15 (31.3%) | 15 (31.3%) |
| Smoking status | ||||||||
| Never n (%) | 92 (46.2%) | 107 (53.8%) | 36 (48.6%) | 38 (51.4%) | 34 (56.7%) | 26 (43.3%) | 22 (33.8%) | 22 (33.8%) |
| Current n (%) | 12 (48%) | 13 (52%) | 4 (57.1%) | 3 (42.9%) | 4 (57.1%) | 3 (42.9%) | 4 (36.4%) | 4 (36.4%) |
| Ex-smoker n (%) | 6 (28.6%) | 15 (71.4%) | 2 (16.7%) | 10 (83.3%) | 1 (33.3%) | 2 (66.7%) | 3 (50%) | 3 (50%) |
| Onset of asthma | ||||||||
| 0–4 years n (%) | 2 (50%) | 2 (50%) | 0 (0%) | 0 (0%) | 1 (100%) | 0 (0%) | 1 (33.3%) | 1 (33.3%) |
| 5–11 years n (%) | 54 (55.7%) | 43 (44.3%) | 19 (55.9%) | 15 (44.1%) | 17 (53.1%) | 15 (46.9%) | 18 (58.1%) | 18 (58.1%) |
| ≥12 years n (%) | 54 (37.5%) | 90 (62.5%) | 23 (39%) | 36 (61%) | 21 (56.8%) | 16 (43.2%) | 10 (20.8%) | 10 (20.8%) |
| Parameters | All Patients (n = 245) | |||||||
|---|---|---|---|---|---|---|---|---|
| All | TH | ACC | pMDI | |||||
| Active (n = 110) | Control (n = 135) | Active (n = 42) | Control (n = 51) | Active (n = 39) | Control (n = 31) | Active (n = 29) | Control (n = 53) | |
| Receiving education on how to use the inhalers Yes | 110(45.3%) | 133(54.7%) | 42(45.2%) | 51(54.8%) | 39(55.7%) | 31(44.3%) | 29(36.3%) | 51(63.8%) |
| Education method received by patient on inhaler technique (n = 243) | ||||||||
| Verbal information | 6 (28.6%) | 15 (71.4%) | 3 (37.5%) | 5 (62.5%) | 1 (50%) | 1 (50%) | 2 (18.2%) | 9 (81.1%) |
| Written information | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Physical demonstration | 104 (46.8%) | 118 (53.2%) | 39 (45.9%) | 46 (54.1%) | 38 (55.9%) | 30 (44.1%) | 27 (39.1%) | 42 (60.9%) |
| Being provided with a plan on asthma management (n = 245) Yes | 0 (0%) | 9 (100%) | 0 (0%) | 2 (100%) | 0 (0%) | 1 (100%) | 0 (0%) | 6 (100%) |
| Parameters | All Patients (n = 245) | |||||||
|---|---|---|---|---|---|---|---|---|
| All | pMDI | TH | ACC | |||||
| Active (n = 110) | Control (n = 135) | Active (n = 29) | Control (n = 53) | Active (n = 42) | Control (n = 51) | Active (n = 39) | Control (n = 31) | |
| Complementary treatment use | ||||||||
| Yes | 4 (23.5%) | 13 (76.5%) | 0 (0%) | 8 (100%) | 0 (0%) | 8 (100%) | 0 (0%) | 1 (100%) |
| No | 106 (46.5%) | 122 (53.5%) | 29 (39.2%) | 45 (60.8%) | 29 (39.2%) | 45 (60.8%) | 39 (56.5%) | 30 (43.5%) |
| Believe that complementary treatment works in managing patients’ asthma | ||||||||
| Yes | 4 (23.5%) | 13 (76.5%) | 0 (0%) | 8 (100%) | 4 (50%) | 4 (50%) | 0 (0%) | 1 (100%) |
| Inhaler Technique Scores | |||||||
|---|---|---|---|---|---|---|---|
| Active (n = 110) | Control (n = 135) | ||||||
| Time of Assessment | Mean in % 95% CI | Mean in % 95% CI | p Value | ||||
| All | |||||||
| Baseline assessment | 32.02 | 29.65 | 34.4 | 36.79 | 34.65 | 38.93 | 0.004 |
| One month follow up | 4.646 | 2.621 | 6.672 | 23.13 | 21.29 | 24.96 | <0.001 |
| TH | |||||||
| Baseline assessment | 29.89 | 26.40 | 33.39 | 38.99 | 35.83 | 42.17 | <0.001 |
| One month follow up | 5.29 | 1.86 | 8.73 | 24.4 | 21.28 | 27.52 | <0.001 |
| ACC | |||||||
| Baseline assessment | 33.90 | 30.27 | 37.53 | 40.50 | 36.43 | 44.57 | 0.018 |
| One month follow up | 3.99 | 1.43 | 6.55 | 25.45 | 22.57 | 28.32 | <0.001 |
| pMDI | |||||||
| Baseline assessment | 32.57 | 27.3 | 37.83 | 32.49 | 28.6 | 36.4 | 0.983 |
| One month follow up | 4.59 | 0.10 | 9.1 | 20.55 | 17.2 | 23.87 | <0.001 |
| Asthma Control Score | |||||||
|---|---|---|---|---|---|---|---|
| Active (n = 110) | Control (n = 135) | ||||||
| Time of Assessment | 20–25 | 16–19 | <16 | 20–25 | 16–19 | <16 | p Value |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Well Controlled Asthma | Intermediately Controlled Asthma | Uncontrolled Asthma | Well Controlled Asthma | Intermediately Controlled Asthma | Uncontrolled Asthma | ||
| All | |||||||
| Baseline assessment | 11 (10%) | 42 (38.2%) | 57 (51.8%) | 35 (25.9%) | 47 (34.8%) | 53 (39.3%) | 0.005 |
| One month follow up | 95 (86.4%) | 9 (8.2%) | 6 (5.5%) | 69 (51.1%) | 40 (29.6%) | 26 (19.3%) | <0.001 |
| pMDI | |||||||
| Baseline assessment | 2 (6.9%) | 11 (37.9%) | 16 (55.2%) | 15 (28.3%) | 20 (37.7%) | 18 (34.0%) | 0.046 |
| One month follow up | 26 (89.7%) | 1 (3.4%) | 2 (6.9%) | 24 (45.3%) | 17 (32.1%) | 12 (22.6%) | <0.001 |
| TH | |||||||
| Baseline assessment | 6 (14.3%) | 10 (23.8% | 26 (61.9%) | 17 (33.3%) | 18 (35.3%) | 16 (31.4%) | 0.010 |
| One month follow up | 37 (88.1%) | 3 (7.1%) | 2 (4.8%) | 27 (52.9%) | 14 (27.5%) | 10 (19.6%) | 0.001 |
| ACC | |||||||
| Baseline assessment | 3 (7.7%) | 21 (53.8%) | 15 (38.5%) | 3 (9.7%) | 9 (29%) | 19 (61.3%) | 0.110 |
| One month follow up | 32 (82.1%) | 5 (12.8%) | 2 (5.1%) | 18 (58.1%) | 9 (29%) | 4 (12.9%) | 0.087 |
| Independent Variables | Inhaler Technique Score | |||
|---|---|---|---|---|
| B | 95% CI | p Value | ||
| Education group (Ref. Control) | ||||
| Active | −18.48 | −21.21 | −15.75 | <0.001 |
| Gender (Ref. Female) | ||||
| Male | 2.47 | −1.28 | 6.24 | 0.196 |
| Age | 0.149 | 0.049 | 0.249 | 0.004 |
| Smoking status (Ref. Smoker) | ||||
| Never | −6.13 | −10.64 | −1.62 | 0.008 |
| Onset of asthma (≥12 years) | ||||
| 0–11 years | −6.14 | −9.68 | −2.59 | 0.001 |
| Education (Ref. no) | ||||
| Yes | −13.05 | −32.84 | 6.73 | 0.195 |
| Complementary treatment (Ref. no) | ||||
| Yes | −1.19 | −8.22 | 5.84 | 0.740 |
| BMI | 0.144 | −0.100 | 0.389 | 0.245 |
| Inhaler type (Ref.) | ||||
| pMDI | 1.41 | −3.136 | 5.963 | 0.541 |
| TH | 2.28 | −2.145 | 6.702 | 0.311 |
| PFM | 0.005 | −0.018 | 0.029 | 0.672 |
| FEV | −0.141 | −0.298 | 0.016 | 0.077 |
| IGE | −0.001 | −0.004 | 0.001 | 0.246 |
| Independent Variables | Inhaler Technique Score | ||||||
|---|---|---|---|---|---|---|---|
| B | S.E. | Beta | t | 95% CI | p Value | ||
| Study randomization group (Active) | −23.05 | 1.56 | −0.878 | −14.79 | −25.93 | −19.52 | <0.001 |
| Gender (Male) | 4.59 | 1.6 | 0.164 | 2.86 | 1.38 | 7.81 | 0.006 |
| Type of inhaler (pMDI) | −4.03 | 1.82 | −0.130 | −2.21 | −7.67 | −0.38 | 0.031 |
| Independent Variables | Asthma Control Test Score | |||
|---|---|---|---|---|
| OR | 95% CI | p Value | ||
| study randomization group (active vs. control), (Ref. Control) | ||||
| Active | 5.835 | 3.091 | 11.015 | <0.001 |
| Gender (Ref. Female) | ||||
| Male | 1.101 | 0.631 | 1.922 | 0.735 |
| Age | 0.990 | 0.975 | 1.004 | 0.171 |
| Smoking status (Ref. Smoker) | ||||
| Never | 1.477 | 0.771 | 2.828 | 0.239 |
| Onset of asthma (≥ 12 years) | ||||
| 0–4 years | 0.057 | 0.006 | 0.543 | 0.013 |
| 5–11 years | 3.035 | 1.658 | 5.557 | <0.001 |
| Education (Ref. no) | ||||
| Yes | 1.425 | 0.119 | 17.089 | 0.780 |
| Complementary treatment (Ref. no) | ||||
| Yes | 0.573 | 0.236 | 1.394 | 0.220 |
| BMI | 0.994 | 0.960 | 1.029 | 0.738 |
| Inhaler type (Ref.) | ||||
| TH | 0.846 | 0.434 | 1.652 | 0.625 |
| ACC | 1.0 | 1.0 | 1.001 | 0.453 |
| pMDI | 0.598 | 0.307 | 1.168 | 0.132 |
| PFM | 1.003 | 0.999 | 1.007 | 0.147 |
| FEV | 1.017 | 0.987 | 1.048 | 0.282 |
| Time of Assessment | Paired Difference | |||||
|---|---|---|---|---|---|---|
| All (n = 245) | Baseline Assessment | 1 Month Follow Up | Mean Difference | 95% Confidence Interval of the Difference | Sig | |
| PFM | 279.85 | 333.12 | 53.26 | 46.83 | 59.68 | <0.001 |
| FEV | 71.98 | 75.61 | 3.63 | 1.58 | 5.68 | 0.001 |
| Control group | ||||||
| PFM | 296.09 | 334.13 | 38.04 | 32.22 | 43.86 | <0.001 |
| FEV | 72.86 | 72.44 | 0.42 | −2.63 | 3.47 | 0.783 |
| Active group | ||||||
| PFM | 266.15 | 332.25 | 66.10 | 55.83 | 76.37 | <0.001 |
| FEV | 71.54 | 78.22 | 6.68 | 4.17 | 9.19 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basheti, I.; Mahboub, B.; Salameh, L.; Al-Ani, M.; Jairoun, A.A.; Saddik, B.; Abu-Gharbieh, E. Assessment of Novel Inhaler Technique Reminder Labels in Image Format on the Correct Demonstration of Inhaler Technique Skills in Asthma: A Single-Blinded Randomized Controlled Trial. Pharmaceuticals 2021, 14, 150. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020150
Basheti I, Mahboub B, Salameh L, Al-Ani M, Jairoun AA, Saddik B, Abu-Gharbieh E. Assessment of Novel Inhaler Technique Reminder Labels in Image Format on the Correct Demonstration of Inhaler Technique Skills in Asthma: A Single-Blinded Randomized Controlled Trial. Pharmaceuticals. 2021; 14(2):150. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020150
Chicago/Turabian StyleBasheti, Iman, Bassam Mahboub, Laila Salameh, Mena Al-Ani, Ammar Abdulrahman Jairoun, Basema Saddik, and Eman Abu-Gharbieh. 2021. "Assessment of Novel Inhaler Technique Reminder Labels in Image Format on the Correct Demonstration of Inhaler Technique Skills in Asthma: A Single-Blinded Randomized Controlled Trial" Pharmaceuticals 14, no. 2: 150. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020150