
Metformin Modifies the Gut Microbiota of Mice Infected with Helicobacter pylori


1
INSERM, University of Bordeaux, UMR 1053 Bordeaux Research in Translational Oncology, BaRITOn, F-33000 Bordeaux, France
2
French National Reference Center for Campylobacters & Helicobacters in Bordeaux (CNRCH), University Hospital of Bordeaux, 33000 Bordeaux, France
*
Author to whom correspondence should be addressed.
Pharmaceuticals 2021, 14(4), 329; https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040329
Submission received: 15 January 2021
/
Revised: 11 March 2021
/
Accepted: 24 March 2021
/
Published: 3 April 2021
(This article belongs to the Special Issue Metformin: Mechanism and Application 2022)
Abstract
:Metformin is widely prescribed to treat type 2 diabetes. Diabetes patients treated with metformin have a decreased risk of cancers, including gastric cancer. Among the factors influencing digestive carcinogenesis, gut microbiota interactions have been intensively studied. Metformin exhibits direct antimicrobial activity toward Helicobacter pylori, which plays a crucial role in gastric carcinogenesis. Mice were infected with H. pylori and treated for 12 days with either metformin or phosphate-buffered saline (PBS) as a control. At the end of the treatment period, the mice were euthanized and cecal and intestinal contents and stool were collected. The gut microbiota of the three different digestive sites (stool, cecal, and intestinal contents) were characterized through 16S RNA gene sequencing. In mice infected with H. pylori, metformin significantly decreased alpha diversity indices and led to significant variation in the relative abundance of some bacterial taxa including Clostridium and Lactobacillus, which were directly inhibited by metformin in vitro. PICRUSt analysis suggested that metformin modifies functional pathway expression, including a decrease in nitrate reducing bacteria in the intestine. Metformin significantly changed the composition and predicted function of the gut microbiota of mice infected with H. pylori; these modifications could be implicated in digestive cancer prevention.
1. Introduction
Metformin, also known as 1,1-dimethylbiguanide, is the most widely prescribed glucose metabolism regulator for the treatment of type 2 diabetes mellitus globally [1]. The pharmaceutical effect of metformin is partially determined by AMP-activated protein kinase (AMPK) activation [2]. In response, the digestive system modifies glucose absorption and enhances anaerobic glucose metabolism [3]. In animals, metformin is accumulated at very high concentrations in the wall of the intestine [4]. For several years metformin has also been studied intensively for its antitumor properties in different types of cancer [5].
In 2005, a Scottish study hypothesized that metformin treatment may reduce cancer risk in diabetic patients [6]. A meta-analysis of seven cohort studies of gastric cancer, which has the third greatest mortality among cancers worldwide [7], showed that gastric cancer risk decreased in diabetic patients treated with metformin [8]. Helicobacter pylori plays a crucial role in gastric carcinogenesis by promoting inflammation and degradation of the gastric epithelium [9]. This Gram-negative bacterium colonizes the stomach mucosa in more than 90% of all gastric cancer patients [10]. H. pylori infection is among the most prevalent infections worldwide [11]; however, only 1% of infected patients develop gastric adenocarcinoma [12]. Factors influencing gastric cancer occurrence in infected patients include genetic host factors and environmental factors including the host microbiota [13].
The gut microbiota have many functions, including intestinal homeostasis regulation, immune response, and metabolism energy regulation [14]. Modification of the gut microbiota can be associated with a number of diseases, including cancer [15]. In colorectal cancer, bacteria composing the digestive microbiota help to form the micro-tumoral-environment and may influence cancer development [16]. H. pylori colonization influences the gastric microbiota; its infection leads to a significant decrease in gastric bacterial diversity [17]. Changes in the gastric microbiota with the evolution of gastric mucosa were shown including mucosal microbiome dysbiosis in gastric carcinogenesis [18]. Metformin has been shown to inhibit H. pylori growth directly in vivo and in vitro. Mice infected with H. pylori and treated with metformin show a decrease in gastric H. pylori colonization [19]. Therefore, in the present study, we hypothesized that metformin may affect other bacteria, especially gut bacteria.
In this context, the aim of this study was to describe the effects of metformin on the gut microbiota in H. pylori-infected mice. We studied metformin-induced changes in the composition and metabolic functions of the gut microbiota in three different digestive sites (stool, cecal, and intestinal contents), in mice infected with H. pylori that were treated with either metformin or phosphate-buffered saline (PBS) as a control.
2. Results
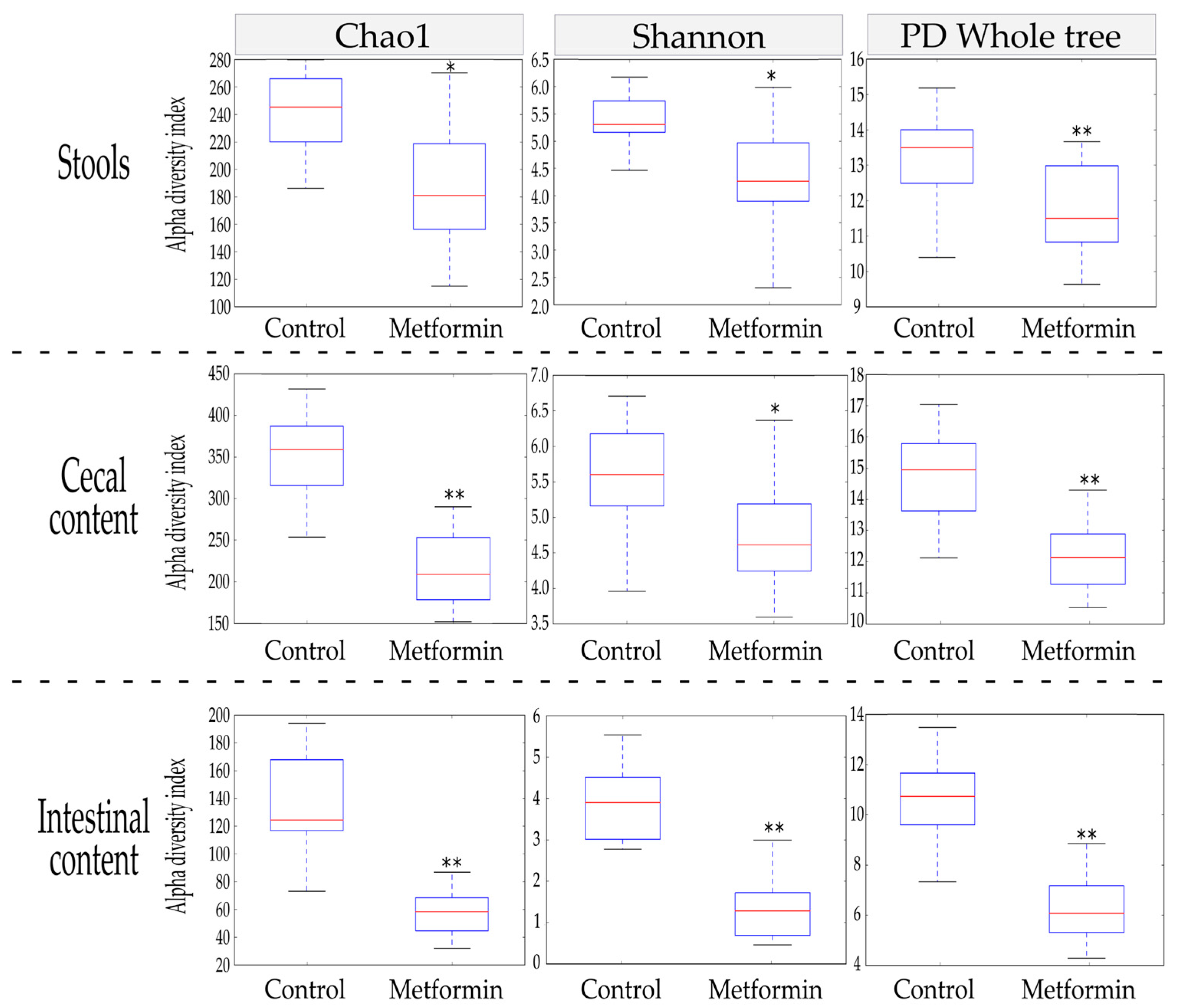
2.1. Alpha Diversity Indices Are Reduced in the Gut Microbiota of Mice Infected with H. pylori and Treated with Metformin
The Chao1, Shannon, and phylogenetic diversity (PD) whole tree alpha diversity indices were used to characterize the richness and diversity of the bacterial community within each sample. At the end of the treatment period, alpha diversity indices were compared between the metformin and control groups for three different sample types: stool, cecal content, and intestinal content.
In stool, metformin treatment induced a significant reduction in alpha diversity indices (p ≤ 0.002; Figure 1). These significant decreases were also observed in the other anatomical digestive sites studied (cecum and intestine). Thus, metformin treatment led to reductions in all alpha diversity indices studied in a homogenous manner throughout the mouse digestive system.
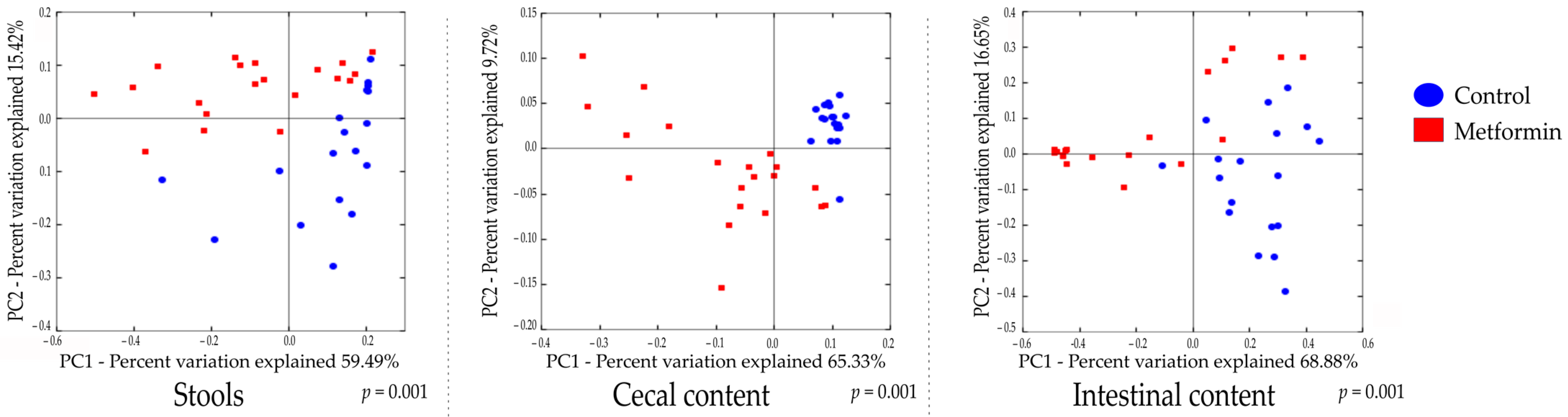
2.2. Beta Diversity Analysis Shows Changes in the Gut Microbiota of Mice Infected with H. pylori and Treated with Metformin
Beta diversity analysis of the three types of digestive samples clearly showed that the metformin and control treatment groups clustered separately at each digestive site (Figure 2 and Figure S2). Weighted UniFrac distances showed that the total diversity values of the two principal coordinates were 74.91%, 75.05%, and 85.53% for stool, cecal, and intestinal content, respectively.
A comparison of bacterial profiles based on weighted and unweighted UniFrac and Bray–Curtis distances showed significant differences between the metformin and control groups (Figure 2 and Figure S2). Adonis statistical tests showed that these observed differences were statistically significant (p = 0.001 for weighted UniFrac, unweighted UniFrac, and Bray–Curtis distances). Thus, metformin induced significant modification of the gut microbiota composition in H. pylori-infected mice.
2.3. Metformin Treatment Changes Taxonomic Repartition in the Gut Microbiota of Mice Infected with H. pylori
The microbial compositions of the three digestive sites at the phylum, class, order, and family levels are shown in Table 1. Only taxa with a relative abundance of ≥0.1% were computed. Bacterial taxa with the most significantly different microbial abundance between treatment groups (p < 1.10−4) are highlighted.
At the phylum level, fecal microbiota was dominated by Firmicutes in both groups, followed by Actinobacteria in the metformin group (8.52% control vs. 28.76% metformin, p = 5.6 × 10–4) and Bacteroidetes in the control group (17.94% control vs. 6.50% metformin, p = 6.8 × 10–5). The × same trend occurred in cecal microbiota composition. In the intestinal microbiota, the control group was dominated by Firmicutes (54.14% control vs. 22.63% metformin, p = 4.2 × 10–5), whereas the metformin group was dominated by Actinobacteria (37.08% control vs. 70.97% metformin, p = 1.5 × 10–5). Metformin treatment decreased abundance of Firmicutes and Bacteroidetes for the benefit of increased Actinobacteria, in the three digestive sites.
Notably, metformin treatment significantly decreased the abundance of Clostridiales in the cecum and intestine (90.33% control vs. 72.38% metformin, p < 1 × 10–6, 25.2% control vs. 2.89% metformin, p = 9 × 10–6 in cecal and intestinal samples, respectively). However, in the three digestive sites, metformin treatment increased Bifidobacteriales abundance (7.28% control vs. 28.14% metformin, p = 2.83 × 10–4, 1.39% control vs. 18.15% metformin, p = 2 × 10–6, 20.79% control vs. 67.44% metformin, p < 1 × 10–6, in stool, cecal, and intestinal samples, respectively).
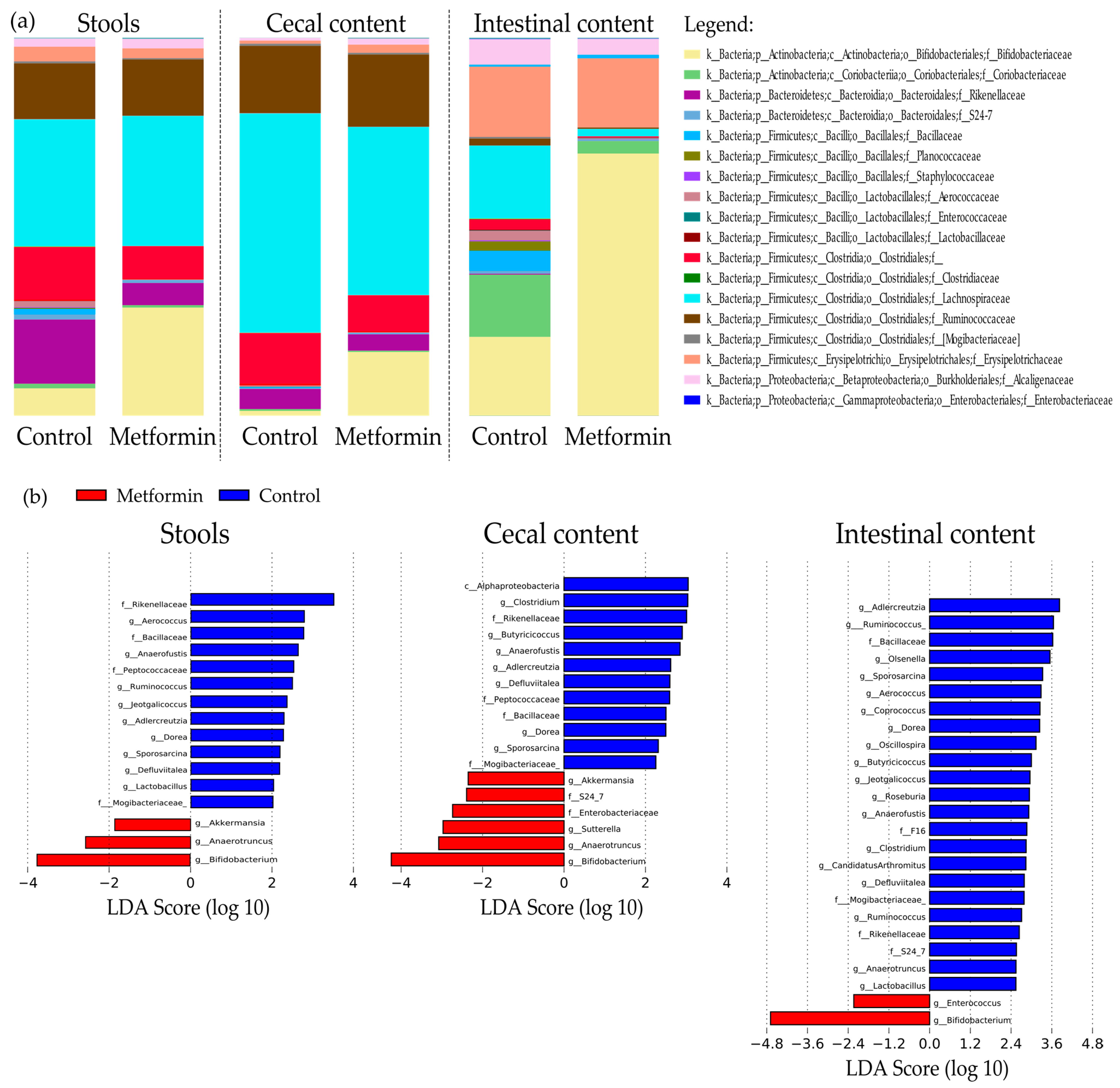
Taxonomic repartition at the family level is shown as bar plots in Figure 3a. Interestingly, family Bifidobacteriacea was significantly more abundant in the microbiota of the metformin group than in that of the control in all three digestive sites (7.3% control vs. 28.1% metformin, p = 2.8 × 10–4, 1.4% control vs. 18.2% metformin, p = 2 × 10–6; 20.8% control vs. 67.4% metformin, p < 1 × 10–6 in fecal, cecal, and intestinal samples, respectively). Metformin treatment significantly decreased Lachnospiraceae abundance in cecal and intestinal contents, but this effect was not observed in fecal samples (34.13% control vs. 34.93% metformin, non-significant, 57.86% control vs. 43.3% metformin, p = 3.5 × 10–4; 19.8% control vs. 2.11% metformin, p = 9 × 10–6 in fecal, cecal, and intestinal samples, respectively; Table 1, Figure 3a).
Liner discriminant analysis (LDA) effect size analysis (LEfSe) was conducted to identify differentially abundant taxa in the three sample types. LDA scores were determined, and the specific taxa associated with metformin treatment were identified (Figure 3b). Among the fecal samples, 16 bacterial taxa were identified, including 12 genera that were differentially abundant between treatment groups (Figure 3b). Compared to the metformin group, 13 taxa were more abundant in the fecal microbiota of control mice.
In the metformin group, a higher abundance of Akkermansia, Anaerotruncus, and Bifidobacterium genera were observed in the fecal microbiota and also in the cecal content. Among them, Bifidobacterium was also more abundant in intestinal microbiota (Figure 3b).
Within the genera Akkermansia and Bifidobacterium, the species Akkermansia muciniphila and Bifidobacterium pseudolongum were identified.
Table S2 shows the LEfSe analysis results for the different digestive sites. Only bacterial taxa with LDA scores > 2 in at least two of the three digestive sites were included; this criterion was met by 12 bacterial taxa in the control group and three bacterial genera in the metformin group (Bifidobacterium, Anaerotruncus, and Akkermansia). Operational taxonomic units (OTUs) number associated to these taxa were listed in Table S3.
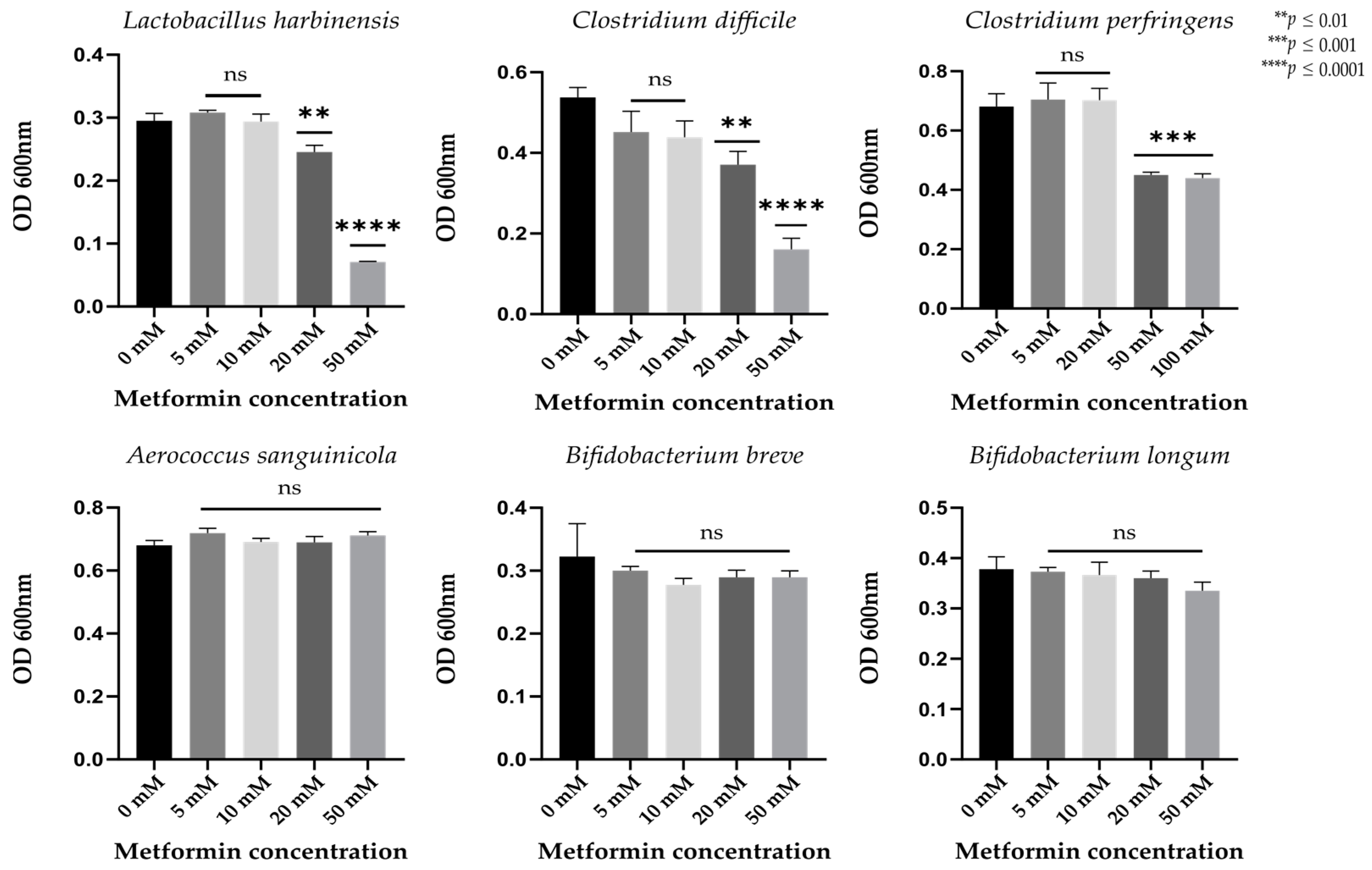
2.4. Metformin Directly Inhibits the Lactobacillus and Clostridium Gut Bacterial Strains In Vitro
To determine which bacterial strains are directly affected by metformin in the gut, we further examined those strains with significantly different relative abundance between the metformin and control groups and easily cultivable. Metformin treatment decreased the abundance of Lactobacillus, Aerococcus, and Clostridiales strains, and increased that of Bifidobacterium strains (Table S2).
We observed no significant growth differences in Aerococcus sanguinicola, Bifidobacterium breve, or Bifidobacterium longum at different metformin concentrations (p > 0.01, Figure 4). Significant decreases in growth were observed in Lactobacillus harbinensis and Clostridium difficile strains incubated with metformin concentrations of 20 and 50 mM (p < 0.01) and in Clostridium perfringens strains treated with higher metformin concentrations (50 and 100 mM, p < 0.01, Figure 4).
2.5. Potential Functional Pathways of Gut Microbiota Are Modified by Metformin Treatment in Mice Infected with H. pylori
Functional analysis of the gut microbiota was performed using the Phylogenetic Investigation of Communities by Reconstruction of Unobserved States (PICRUSt) software based on closed-reference selection of operational taxonomic units (OTUs). We examined 159 pathways based on the Kyoto Encyclopedia of Genes and Genomes (KEGG) reference database. Only KEGG pathways with a relative abundance > 0.001% were considered; these represented 124, 119, and 132 KEGG pathways in stool, cecal, and intestinal samples, respectively. Pathways with a significantly different abundance between the metformin and control groups were identified for all three different digestive sites (p < 0.05, after Bonferroni correction). These differentially enriched KEGG pathways are shown in Figure 5 and Figure S3.
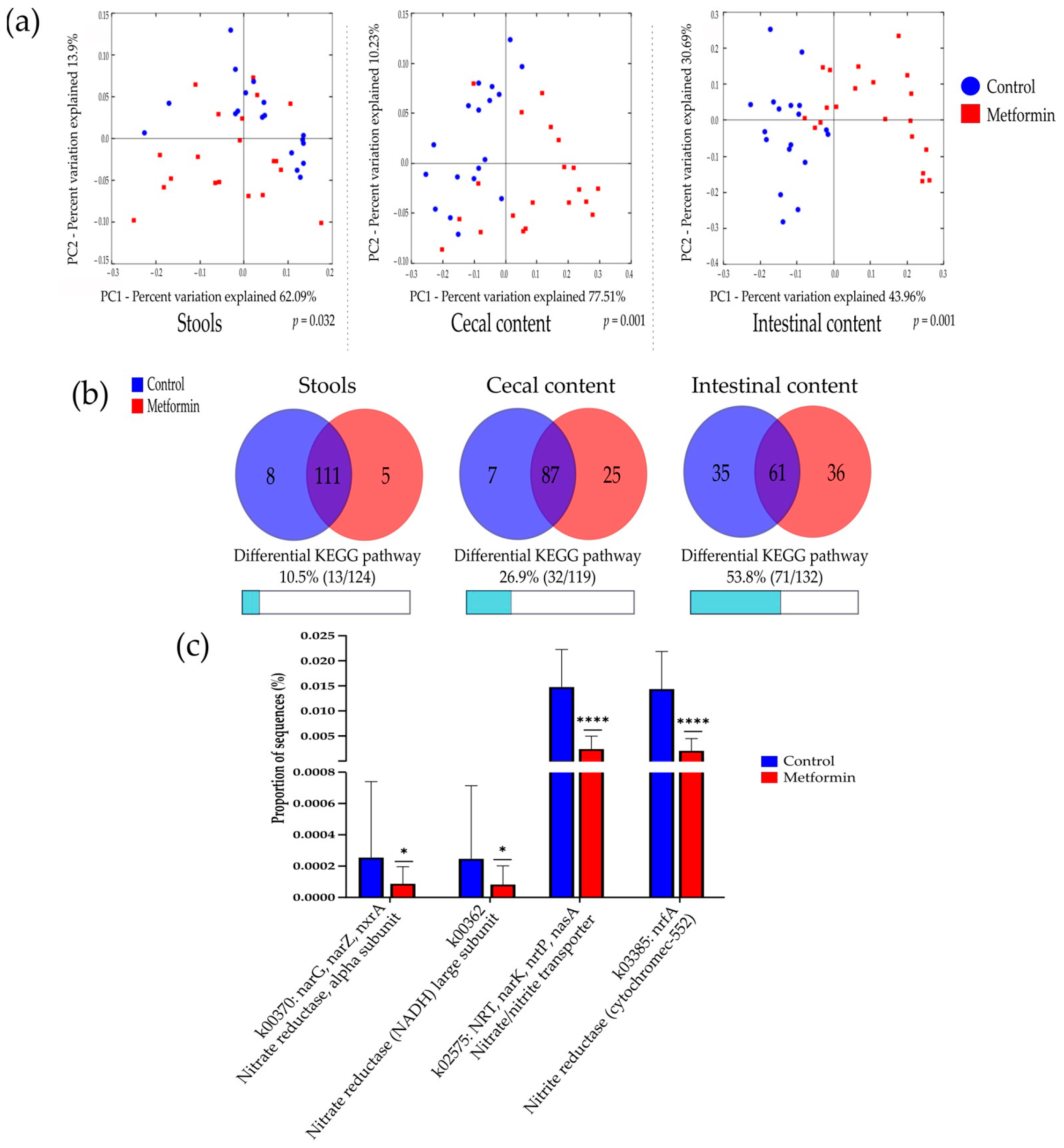
Beta diversity analysis according to the predicted functional pathways for each group was performed. A comparison of the microbiota of the metformin and control groups based on metabolic function showed differential bacterial profiles on 2D PCoA plots (Figure 6a). Adonis statistical tests performed on these data showed significant differences among Bray–Curtis distances in all sample types (p = 0.001).
In stool samples, five predicted KEGG pathways were significantly more abundant in the metformin group, compared with eight KEGG pathways in the control group. The differential KEGG pathways between the metformin and control groups represented 10.5% and 26.9% of all pathways examined for stool and cecal content, respectively. The highest number of differential KEGG pathways was found in intestinal content (53.8%, Figure 6b).
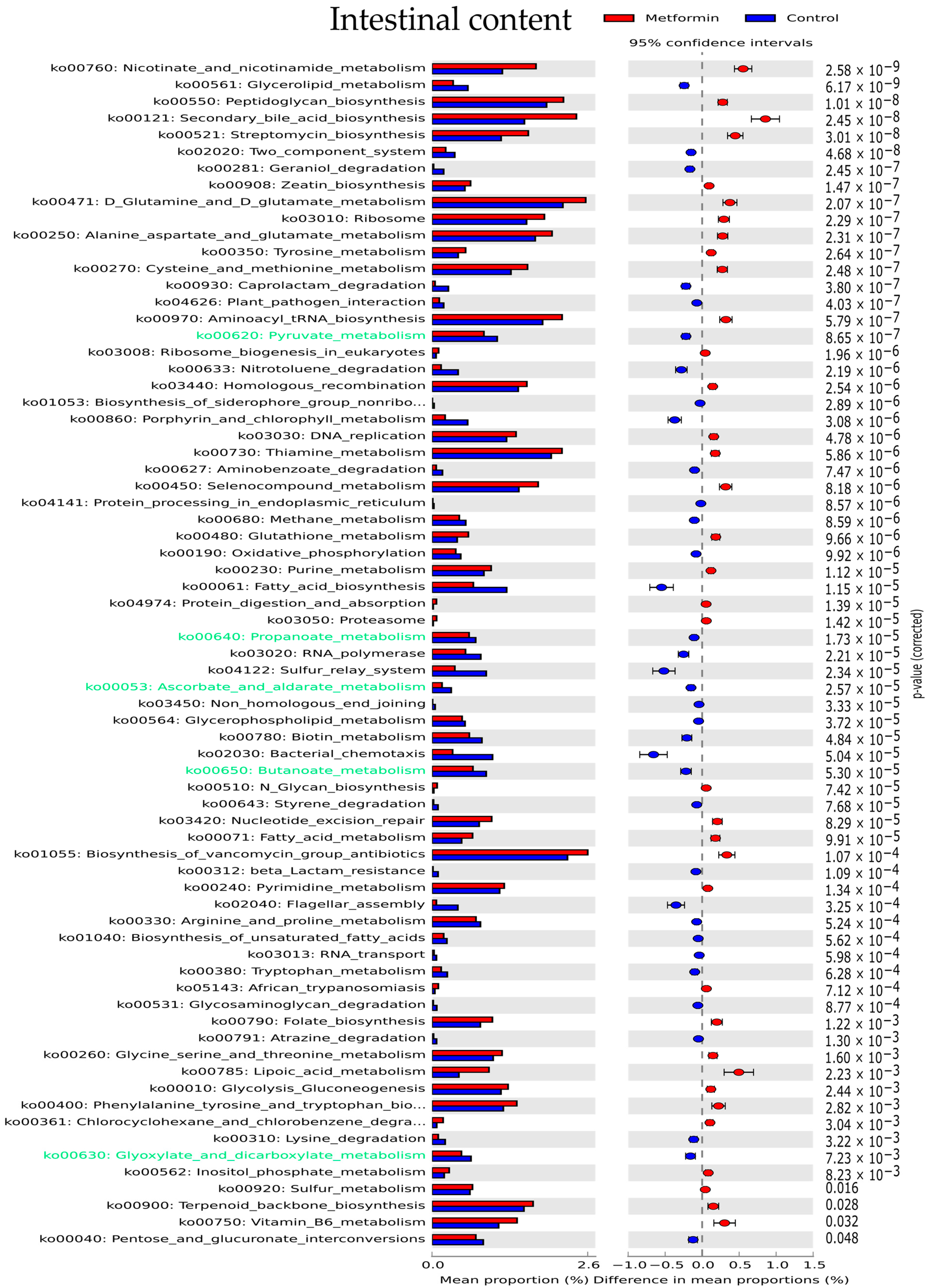
In intestinal samples, the most significantly enriched KEGG pathways in the metformin group were nicotinate and nicotinamide metabolism, peptidoglycan biosynthesis, secondary bile acid biosynthesis, and streptomycin biosynthesis (Figure 5). Carbohydrate metabolism was predicted to be higher in the microbiota of control group mice than in metformin-treated mice. Pathways implicated in carbohydrate metabolism (green text, Figure 5) including pyruvate, propanoate, ascorbate, butanoate, and glyoxylate metabolism were predicted to be overexpressed in the control group.
Finally, nitrate and nitrite-reducing bacterial species were specifically studied in intestinal content by focusing on the KEGG gene expression of k02575, k00370, k00363, and k03385, which code for nitrate or nitrite-reductase enzymes. Intestinal bacteria in the microbiota of metformin-treated mice showed significantly decreased nitrate and nitrite-reductase functions (p < 0,05, Mann–Whitney U test) (Figure 6c).
PICRUSt analyses showed that metformin treatment led to significant changes in predicted metabolic functions by gut bacteria in infected mice, specifically in intestinal sites.
3. Discussion
In the present study, we examined changes in the gut microbiota at three different digestive sites, represented by stool, cecal, and intestinal samples, induced by oral metformin treatment of mice infected with H. pylori. We performed 16S rRNA gene sequencing and characterized the gut microbial profiles of mice infected with H. pylori and treated with metformin.
Our results showed that metformin decreased richness and diversity of the microbiota of mice. High microbiota diversity and richness are usually considered to be markers of a healthy microbiota; however, decreases in the abundance of any bacterial taxa may lead to the relative emergence of metabolically beneficial microorganisms such as Akkermansia muciniphila, which is associated with metabolic improvement [20]. In this study, Akkermansia muciniphila was found to be more abundant in metformin-treated mice than in control mice, which is consistent with the results of a previous study of diabetic patients that suggested that these effects could contribute to the therapeutic effect of metformin in diabetes treatment [21].
Beta diversity analyses showed that microbial features depended on the treatment received. Other studies have reported significant changes in the microbiota of obese mice, healthy mice, and diabetic humans following metformin treatment [21,22,23,24].
The direct effect of metformin on bacterial growth was measured on six bacterial strains. Thanks to taxonomic composition analysis, we selected six bacterial species that were available in the laboratory, easily cultivable, and with relative abundance either positively or negatively influenced by metformin treatment. This experiment showed that metformin directly inhibited the growth of Lactobacillus and Clostridium gut bacteria. Metformin can also indirectly modify the microbiota by acting on host physiology; for example, metformin increases the bile acid pool within the intestine [25], which may affect stool consistency and the microbiome [26]. More recently, metformin treatment was revealed to enhance the release of glucose into the intraluminal space of the intestine in humans [27]; therefore, high glucose concentration in the intestinal lumen may impact bacterial development. Thus, metformin-induced microbiota changes are probably the result of both direct and indirect effects.
The effects of metformin on human health have been intensively studied in recent years. Beyond its implication in diabetes treatment, metformin represents a promising anticancer drug in combination with conventional chemotherapies for different types of cancer [28]. Recent studies have also demonstrated the antiaging effects of metformin [29] and its direct antimicrobial effect against H. pylori, which has opened new avenues of research [19]. In cancer prevention, metformin has been shown to reduce cancer incidence in diabetic patients [6]. Microbiota composition and function are well recognized as influencing carcinogenesis through different mechanisms [30]. H. pylori is the best example of a specific bacterial pathogen that can trigger carcinogenesis by promoting inflammation and degradation of the gastric epithelium [9]. The bacterial microbiota may also influence intestinal barrier preservation, inflammation modulation, and the production of cancer-promoting metabolites [31]. In this context, we investigated the influence of metformin treatment on microbiota mechanisms potentially implicated in gut carcinogenesis.
Concerning specific bacterial taxa, despite decreases global richness, metformin treatment led to increases in Bifidobacterium abundance. Bifidobacterium species have demonstrated anti-colorectal cancer activity by producing metabolites that directly inhibit the growth of colon cancer cells in vitro [32]. Bifidobacterium species are often integrated into probiotic products for health treatments, including cancer prevention. It has been suggested that probiotics containing Bifidobacterium species can contribute to colorectal cancer prevention and improvement of safety and effectiveness of colorectal cancer therapy [33].
A recent study of diabetic and non-diabetic mice with induced colorectal cancer showed that metformin treatment in association with probiotics containing Bifidobacterium species actively prevented inflammatory and carcinogenic processes [34]. Furthermore a study of H. pylori-related gastric lesions showed a higher relative abundance of Firmicute in gastritis and gastric metaplasia patients [35]. Interestingly, our results showed a decreased relative abundance of Firmicute bacteria in H. pylori-infected mice in response to metformin treatment.
Functional features of the microbiota of mice in this study were examined using the PICRUSt software [36]. The resulting bacterial predicted profiles showed that the metformin and control groups had distinct metabolic functional signatures. The intestinal microbiota showed the highest expression among differential metabolic KEGG pathways between groups, indicating that metformin treatment leads to significant modification of the functional properties of the digestive microbiota, particularly in intestinal sites.
Specifically, metformin treatment decreased nitrate and nitrite reductase functions in intestinal bacteria. The nitrate-reducing bacterial pathway was analyzed because it has been suggested to participate in the increase of intragastric concentrations of nitrite and N-nitroso-compounds [37]. N-nitroso-compounds promote mutagenesis and protooncogene expression, and inhibit apoptosis; they can also contribute to gastric carcinogenesis [38,39]. Increased functional activity of nitrate reductase has been observed in the gastric microbiota of gastric cancer patients in comparison with chronic gastritis patients [40]. In the present study, KEGG pathways involved in carbohydrate metabolism were enriched in the control group, which comprised mice infected with H. pylori but not treated with metformin. These pathways are predictive of bacterial production of short-chain fatty acids [41], which have been linked to cell hyperproliferation in colorectal and esophageal cancer [42,43]. These pathways have also been found to be enriched in the gastric microbiota of gastric cancer patients [18]. Together, these findings demonstrate the potential contribution of bacteria-producing short-chain fatty acids to digestive tumorigenesis. These first results suggest that metformin, by modulating microbiota function, could be considers as a potentially interesting agent for digestive cancer prevention. Molecular mechanisms that sustain the anticancer effect of metformin through the regulation of glucose metabolism have been reported [44]. Thus, host physiology and the microbiota constitute different potential targets for metformin action in preventing cancer occurrence. In diabetic patients, metformin reduced the incidence of adenomas that could transform into colorectal cancer; therefore, metformin may be useful for the prevention of colorectal cancer in patients with type 2 diabetes [45]. In mice, metformin use in association with probiotics reinforces beneficial effect on colorectal cancer prevention [34].
The limitations of this study were the lack of information about gastric microbiota; more experiments should be performed to understand the metabolic modifications induced with metformin microbiota changes. We used female mice, which are less aggressive than male and easier to use in animal facilities. Consequently, results obtained are only valid in female and cannot completely be extrapolated to male as there are few differences in the composition of gut microbiota between genders and between female of different hormonal status [46,47]. However, a female from either the control or metformin group had the same age at the beginning and during all the length of the experiment; therefore, mice from the two groups were exposed to the same sexual hormonal modifications, allowing the groups comparison.
In conclusion, the results of this study show that metformin significantly alters the composition and predicted function of the gut microbiota of mice infected with H. pylori. These modifications could be implicated in gut cancer prevention.
4. Materials and Methods
4.1. Animal Protocol and Sample Collection
The animal protocol used in this study was previously described [19]. Five-week-old Specific Pathogen-Free C57Bl6J female mice were chosen for their better ability to live with partners. Mice were infected intragastrically on 3 consecutive days with 0.1 mL of a highly concentrated suspension of mouse-adapted H. pylori strains SS1 and B47 (Mc Farland 7 opacity standard) [48,49]. Three days after the last infection, the mice were divided randomly into two groups: an infected group treated with PBS as a control (n = 18, two mice died before the beginning of treatment) and an infected group treated with metformin (Sigma Aldrich, St. Louis, MO, USA) at 10 mg/mouse (n = 20). This dosage was determined using the method of dose conversion between human and animal studies [50]. With this method, 10 mg/mouse/day corresponds to 2.4 g of metformin/day for a human adult. The maximal dosage of metformin used to treat Type 2 diabetes patients is 3 g/day. Each group received a daily treatment (0.1 mL) for 12 days by gavage. During this period all mice had access to water ad libitum and a normal diet. Stool samples were collected before infection with H. pylori and after 12 days of treatment. Weight was controlled during the study. After the treatment, no differences were observed in mice weight between the two groups (data not shown). At the end of the treatment, mice were euthanized by cervical dislocation. Cecum and intestine were aseptically taken to collect cecal and intestinal content separately. Intestinal content corresponds to the entire content of mice intestine, no specific region in intestine was selected. Gastric samples were not available for use in this study.
All collected samples were immediately stored in a sterile tube at −80 °C. Mouse experiments were performed in level 2 animal facilities at Bordeaux University with the approval of the local Ethical Committee, and in conformity with the French Ministry of Agriculture (approval no. 4608).
Initially, alpha and beta diversity were analyzed using mouse stool samples collected from both groups prior to infection and treatment. This analysis confirmed that the groups were comparable and presented no differences in alpha or beta diversity (Figure S1). Same analysis was also performed on stools collected after infection with H. pylori and before any treatment with the same results (data not shown).
4.2. DNA Extraction and rRNA Gene Sequencing
DNA was extracted from samples using the QIAamp PowerFecal Pro DNA kit with a PowerLyzer (Qiagen, Hilden, Germany) according to the manufacturer’s protocol. Quantification, sequencing of the V3–V4 region of 16S rRNA, and assembly were performed by Genoscreen (Lille, France; further details provided in Supplementary material S1). The 16S rRNA sequencing datasets generated in this study can be found in the SRA database (http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/bioproject/701274, accessed on 3 April 2021).
4.3. Functional Metagenome Predictions
Phylogenetic Investigation of Communities by Reconstruction of Unobserved States (PICRUSt) 1.1.0 software was used to predict virtual metagenomes for each sample using the 16S rRNA gene sequencing results [36]. The Kyoto Encyclopedia of Genes and Genomes (KEGG) was used as a reference database. Based on the predicted metagenomes, the relative abundance of KEGG genes or KEGG pathways (ko) within each sample was determined.
4.4. Bioinformatics Analysis
Alpha and beta diversity were computed using the QIIME v1.9.1 software. The samples have been rarefied to 32,606 sequences for these analyses. Alpha diversity was calculated in terms of the Chao1, Shannon, and phylogenetic diversity (PD) whole-tree metrics. Beta diversity was calculated using weighted and unweighted UniFrac or Bray–Curtis distances. Ordination was performed using principal coordinate analysis (PCoA). The strength and statistical significance of beta diversity were computed using the Adonis method with QIIME.
Statistically significant differences in the relative abundance of taxa associated with the treatment groups were detected using linear discriminant analysis (LDA) effect size (LEfSe) [51]. Only taxa with LDA > 2 and p < 0.05 were considered significantly enriched.
Predicted functional genes were compared between groups and the results visualized using the STAMP v2.1.3 software [52]. Statistical differences in KEGG pathway frequencies were determined using White’s nonparametric t-test, followed by Bonferroni correction to adjust p values.
4.5. In Vitro Bacterial Growth Experiments
Strains of Aerococcus sanguinicola, Lactobacillus harbinensis, Bifidobacterium longum, Bifidobacterium breve, Clostridium difficile, and Clostridium perfringens were obtained from a collection at the University Hospital of Bordeaux. Strains were identified using matrix-assisted laser desorption ionization–time-of-flight (MALDI–TOF) mass spectrometry. All strains were pre-cultured for 24 h by inoculation on Columbia blood agar (Thermo Scientific, Waltham, MA, USA) under anaerobic conditions (5% H2, 10% CO2, and 85% N2) at 35 °C. Pre-cultures were resuspended in sterile water at a concentration equivalent to the MC Farland 4 opacity standard for each strain. These solutions were mixed at 1:4 dilution with BH broth (Thermo Scientific) containing various concentrations of metformin (0, 5, 10, 20, 50, and 100 mM). Solutions were then inoculated into a 96-well microplate and incubated under anaerobic conditions. The effect of metformin on bacterial growth was analyzed in terms of the optical density at a wavelength of 600 nm (OD600) using a Nanodrop microplate reader (BMG Labtech, Champigny-sur-Marne, France) after 24 h of incubation.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/ph14040329/s1. Figure S1: Alpha and beta diversity comparison of fecal microbiota of the metformin and control treatment groups before the beginning of treatment. Figure S2: Principal coordinate analysis (PCoA) plots created using unweighted UniFrac and Bray distances. Figure S3: Differentially enriched Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways in fecal and cecal microbiota. Figure S4: Rarefaction curves showing the number of observed OTU as a function of the number of sequences per samples. Table S1: Comparison of the relative abundance of bacteria between the metformin and control treatment groups at species level. Table S2: Bacterial taxa with LDA scores > 2 in at least two of the three digestive sites in the metformin and control groups. Table S3: OTUs number of bacterial taxa with LDA scores > 2 in at least two of the three digestive sites in the metformin and control groups Table S4: Number of reads obtained in each sample after preprocessing. Supplementary material S1: rRNA gene sequencing details.
Author Contributions
Conceptualization, E.B.; methodology, E.B., P.L., and M.J.; formal analysis M.J.; resources, E.B. and P.L.; data curation, S.C.; writing (original draft preparation), M.J.; writing (review and editing), E.B., S.C., and P.L.; supervision, E.B. and P.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Experiments on mice were carried out in level 2 animal facilities at the University of Bordeaux in agreement with the local Ethics Committee on Animal Experiments CEEA50 of Bordeaux (approval number 10174, July 2017).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article or supplementary material.
Acknowledgments
The authors thank Raphaël Enaud for helpful discussion and useful advice regarding the DNA extraction protocol. The English in this document has been checked by at least two professional editors, both native speakers of English. For a certificate, please see: http://www.textcheck.com/certificate/Rvelva, accessed on 3 April 2021.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Ferrannini, E.; Holman, R.R.; Sherwin, R.; Zinman, B. Medical management of hyperglycemia in type diabetes: A consensus algorithm for the initiation and adjustment of therapy: A consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009, 32, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, G.; Myers, R.; Li, Y.; Chen, Y.; Shen, X.; Fenyk-Melody, J.; Wu, M.; Ventre, J.; Doebber, T.; Fujii, N.; et al. Role of AMP-activated protein kinase in mechanism of metformin action. J. Clin. Investig. 2001, 108, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.J.; Mynett, K.J.; Page, T. Importance of the intestine as a site of metformin-stimulated glucose utilization. Br. J. Pharm. 1994, 112, 671–675. [Google Scholar] [CrossRef] [Green Version]
- Wilcock, C.; Bailey, C.J. Accumulation of metformin by tissues of the normal and diabetic mouse. Xenobiotica 1994, 24, 49–57. [Google Scholar] [CrossRef]
- Morales, D.R.; Morris, A.D. Metformin in cancer treatment and prevention. Annu. Rev. Med. 2015, 66, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.M.M.; Donnelly, L.A.; Emslie-Smith, A.M.; Alessi, D.R.; Morris, A.D. Metformin and reduced risk of cancer in diabetic patients. Br. Med. Assoc. 2005, 330, 1304–1305. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.-L.; Xue, W.-H.; Ding, X.-F.; Li, L.-F.; Dou, M.-M.; Zhang, W.-J.; Lv, Z.; Fan, Z.-R.; Zhao, J.; Wang, L.-X. Association between metformin and the risk of gastric cancer in patients with type 2 diabetes mellitus: A meta-analysis of cohort studies. Oncotarget 2017, 8, 55622–55631. [Google Scholar] [CrossRef] [Green Version]
- Correa, P. Human gastric carcinogenesis: A multistep and multifactorial process—First American cancer society award lecture on cancer epidemiology and prevention. Cancer Res. 1992, 52, 6735–6740. [Google Scholar]
- González, C.A.; Megraud, F.; Buissonniere, A.; Barroso, L.L.; Agudo, A.; Duell, E.J.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Palli, D.; Krogh, V.; et al. Helicobacter pylori infection assessed by ELISA and by immunoblot and noncardia gastric cancer risk in a prospective study: The Eurgast-EPIC project. Ann. Oncol. 2012, 23, 1320–1324. [Google Scholar] [CrossRef]
- Brown, L.M. Helicobacter pylori: Epidemiology and routes of transmission. Epidemiol. Rev. 2000, 22, 283–297. [Google Scholar] [CrossRef]
- Mégraud, F.; Bessède, E.; Varon, C. Helicobacter pylori infection and gastric carcinoma. Clin. Microbiol. Infect. 2015, 21, 984–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lofgren, J.L.; Whary, M.T.; Ge, Z.; Muthupalani, S.; Taylor, N.S.; Mobley, M.; Potter, A.; Varro, A.; Eibach, D.; Suerbaum, S.; et al. Lack of commensal flora in Helicobacter pylori-infected INS-GAS mice reduces gastritis and delays intraepithelial neoplasia. Gastroenterology 2011, 140, 210–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jandhyala, S.M.; Talukdar, R.; Subramanyam, C.; Vuyyuru, H.; Sasikala, M.; Reddy, D.N. Role of the normal gut microbiota. World J. Gastroenterol. 2015, 21, 8787–8803. [Google Scholar] [CrossRef] [PubMed]
- Rooks, M.G.; Garrett, W.S. Gut microbiota, metabolites and host immunity. Nat. Rev. Immunol. 2016, 16, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Cremonesi, E.; Governa, V.; Garzon, J.F.G.; Mele, V.; Amicarella, F.; Muraro, M.G.; Trella, E.; Galati-Fournier, V.; Oertli, D.; Däster, S.R.; et al. Gut microbiota modulate T cell trafficking into human colorectal cancer. Gut 2018, 67, 1984–1994. [Google Scholar] [CrossRef] [PubMed]
- Maldonado-Contreras, A.; Goldfarb, K.C.; Godoy-Vitorino, F.; Karaoz, U.; Contreras, M.; Blaser, M.J.; Brodie, E.L.; Dominguez-Bello, M.G. Structure of the human gastric bacterial community in relation to Helicobacter pylori status. ISME J. 2011, 5, 574–579. [Google Scholar] [CrossRef]
- Coker, O.O.; Dai, Z.; Nie, Y.; Zhao, G.; Cao, L.; Nakatsu, G.; Wu, W.K.; Wong, S.H.; Chen, Z.; Sung, J.J.Y.; et al. Mucosal microbiome dysbiosis in gastric carcinogenesis. Gut 2018, 67, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Courtois, S.; Bénéjat, L.; Izotte, J.; Mégraud, F.; Varon, C.; Lehours, P.; Bessède, E. Metformin can inhibit Helicobacter pylori growth. Future Microbiol. 2018, 13, 1575–1583. [Google Scholar] [CrossRef]
- Derrien, M.; Belzer, C.; De Vos, W.M. Akkermansia muciniphila and its role in regulating host functions. Microb. Pathog. 2017, 106, 171–181. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Esteve, E.; Tremaroli, V.; Khan, M.T.; Caesar, R.; Mannerås-Holm, L.; Ståhlman, M.; Olsson, L.M.; Serino, M.; Planas-Fèlix, M.; et al. Metformin alters the gut microbiome of individuals with treatment-naive type 2 diabetes, contributing to the therapeutic effects of the drug. Nat. Med. 2017, 23, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, Y.; Kim, J.; An, J.; Lee, S.; Kong, H.; Song, Y.; Lee, C.-K.; Kim, K. Modulation of the gut microbiota by metformin improves metabolic profiles in aged obese mice. Gut Microbes 2018, 9, 155–165. [Google Scholar] [CrossRef] [Green Version]
- Ma, W.; Chen, J.; Meng, Y.; Yang, J.; Cui, Q.; Zhou, Y. Metformin alters gut microbiota of healthy mice: Implication for Its potential role in gut microbiota homeostasis. Front. Microbiol. 2018, 9, 1336. [Google Scholar] [CrossRef] [Green Version]
- Forslund, K.; Hildebrand, F.; Nielsen, T.R.; Falony, G.; Le Chatelier, E.; Sunagawa, S.; Prifti, E.; Vieira-Silva, S.; Gudmundsdottir, V.; Pedersen, H.K.; et al. Disentangling type 2 diabetes and metformin treatment signatures in the human gut microbiota. Nature 2015, 528, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Yi, F.; Sun, J.; Lim, G.E.; Fantus, I.G.; Brubaker, P.L.; Jin, T. Cross talk between the insulin and Wnt signaling pathways: Evidence from intestinal endocrine L cells. Endocrinology 2008, 149, 2341–2351. [Google Scholar] [CrossRef] [Green Version]
- McCreight, L.J.; Bailey, C.J.; Pearson, E.R. Metformin and the gastrointestinal tract. Diabetologia 2016, 59, 426–435. [Google Scholar] [CrossRef] [Green Version]
- Morita, Y.; Nogami, M.; Sakaguchi, K.; Okada, Y.; Hirota, Y.; Sugawara, K.; Tamori, Y.; Zeng, F.; Murakami, T.; Ogawa, W. enhanced release of glucose into the intraluminal space of the intestine associated with metformin treatment as revealed by [18F]fluorodeoxyglucose PET-MRI. Diabetes Care 2020, 43, 1796–1802. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-H.; Guo, X.-L. Combinational strategies of metformin and chemotherapy in cancers. Cancer Chemother. Pharm. 2016, 78, 13–26. [Google Scholar] [CrossRef]
- Barzilai, N.; Crandall, J.P.; Kritchevsky, S.B.; Espeland, M.A. Metformin as a tool to target aging. Cell Metab. 2016, 23, 1060–1065. [Google Scholar] [CrossRef] [Green Version]
- Rajagopala, S.V.; Vashee, S.; Oldfield, L.M.; Suzuki, Y.; Venter, J.C.; Telenti, A.; Nelson, K.E. The human microbiome and cancer. Cancer Prev. Res. 2017, 10, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Schwabe, R.F.; Jobin, C. The microbiome and cancer. Nat. Rev. Cancer 2013, 13, 800–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahmani, S.; Azarpira, N.; Moazamian, E. Anti-colon cancer activity of Bifidobacterium metabolites on colon cancer cell line SW742. Turk. J. Gastroenterol. 2019, 30, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Eslami, M.; Yousefi, B.; Kokhaei, P.; Hemati, M.; Nejad, Z.R.; Arabkari, V.; Namdar, A. Importance of probiotics in the prevention and treatment of colorectal cancer. J. Cell Physiol. 2019, 234, 17127–17143. [Google Scholar] [CrossRef] [PubMed]
- Al Kattar, S.; Jurjus, R.; Pinon, A.; Leger, D.Y.; Jurjus, A.; Boukarim, C.; Diab-Assaf, M.; Liagre, B. Metformin and probiotics in the crosstalk between colitis-associated colorectal cancer and diabetes in mice. Cancers 2020, 12, 1857. [Google Scholar] [CrossRef]
- Gao, J.-J.; Zhang, Y.; Gerhard, M.; Mejias-Luque, R.; Zhang, L.; Vieth, M.; Ma, J.-L.; Bajbouj, M.; Suchanek, S.; Liu, W.-D.; et al. Association between gut microbiota and Helicobacter pylori—Related gastric lesions in a high-risk population of gastric cancer. Front. Cell Infect. Microbiol. 2018, 8, 202. [Google Scholar] [CrossRef] [Green Version]
- Langille, M.G.; Zaneveld, J.; Caporaso, J.G.; McDonald, D.; Knights, D.; A Reyes, J.; Clemente, J.C.; E Burkepile, D.; Thurber, R.L.V.; Knight, R.; et al. Predictive functional profiling of microbial communities using 16S rRNA marker gene sequences. Nat. Biotechnol. 2013, 31, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Leach, S.A.; Thompson, M.; Hill, M. Bacterially catalysed N-nitrosation reactions and their relative importance in the human stomach. Carcinogenesis 1987, 8, 1907–1912. [Google Scholar] [CrossRef]
- Ambs, S.; Ogunfusika, M.O.; Merriam, W.G.; Bennett, W.P.; Billiar, T.R.; Harris, C.C. Up-regulation of inducible nitric oxide synthase expression in cancer-prone p53 knockout mice. Proc. Natl. Acad. Sci. USA 1998, 95, 8823–8828. [Google Scholar] [CrossRef] [Green Version]
- Feng, C.W.; Wang, L.D.; Jiao, L.H.; Liu, B.; Zheng, S.; Xie, X.J. Expression of p53, inducible nitric oxide synthase and vascular endothelial growth factor in gastric precancerous and cancerous lesions: Correlation with clinical features. BMC Cancer 2002, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, R.M.; Pereira-Marques, J.; Pinto-Ribeiro, I.; Costa, J.L.; Carneiro, F.; Machado, J.C.; Figueiredo, C. Gastric microbial community profiling reveals a dysbiotic cancer-associated microbiota. Gut 2018, 67, 226–236. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.M.W.; De Souza, R.; Kendall, C.W.C.; Emam, A.; Jenkins, D.J.A. Colonic health: Fermentation and short chain fatty acids. J. Clin. Gastroenterol. 2006, 40, 235–243. [Google Scholar] [CrossRef]
- Kaakoush, N.O.; Morris, M.J. The oesophageal microbiome: An unexplored link in obesity-associated oesophageal adenocarcinoma. FEMS Microbiol. Ecol. 2016, 92. [Google Scholar] [CrossRef] [Green Version]
- Belcheva, A.; Irrazabal, T.; Robertson, S.J.; Streutker, C.; Maughan, H.; Rubino, S.; Moriyama, E.H.; Copeland, J.K.; Surendra, A.; Kumar, S.; et al. Gut microbial metabolism drives transformation of MSH2-deficient colon epithelial cells. Cell 2014, 158, 288–299. [Google Scholar] [CrossRef] [Green Version]
- Salani, B.; Del Rio, A.; Marini, C.; Sambuceti, G.; Cordera, R.; Maggi, D. Metformin, cancer and glucose metabolism. Endocr. Relat. Cancer 2014, 21, R461–R471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.H.; Ko, B.M.; Kim, S.H.; Myung, Y.S.; Choi, J.H.; Han, J.P.; Hong, S.J.; Jeon, S.R.; Kim, H.G.; Kim, J.O.; et al. Does metformin affect the incidence of colonic polyps and adenomas in patients with type 2 diabetes mellitus? Intest. Res. 2014, 12, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Org, E.; Mehrabian, M.; Parks, B.W.; Shipkova, P.; Liu, X.; Drake, T.A.; Lusis, A.J. Sex differences and hormonal effects on gut microbiota composition in mice. Gut Microbes 2016, 7, 313–322. [Google Scholar] [CrossRef] [Green Version]
- Santos-Marcos, J.A.; Rangel-Zuñiga, O.A.; Jimenez-Lucena, R.; Quintana-Navarro, G.M.; Garcia-Carpintero, S.; Malagon, M.M.; Landa, B.B.; Tena-Sempere, M.; Perez-Martinez, P.; Lopez-Miranda, J.; et al. Influence of gender and menopausal status on gut microbiota. Maturitas 2018, 116, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; O’Rourke, J.; De Ungria, M.C.; Robertson, B.; Daskalopoulos, G.; Dixon, M.F. A standardized mouse model of Helicobacter pylori infection: Introducing the Sydney strain. Gastroenterology 1997, 112, 1386–1397. [Google Scholar] [CrossRef]
- Lehours, P.; Ménard, A.; Dupouy, S.; Bergey, B.; Richy, F.; Zerbib, F.; Ruskoné-Fourmestraux, A.; Delchier, J.C.; Mégraud, F. Evaluation of the association of nine Helicobacter pylori virulence factors with strains involved in low-grade gastric mucosa-associated lymphoid tissue lymphoma. Infect. Immun. 2004, 72, 880–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, A.B.; Jacob, S. A simple practice guide for dose conversion between animals and human. J. Basic Clin. Pharm. 2016, 7, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic biomarker discovery and explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parks, D.H.; Beiko, R.G. Identifying biologically relevant differences between metagenomic communities. Bioinformatics 2010, 26, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Comparison of alpha diversity indices between metformin (n = 20) and control (n = 18) treatment groups in stool, cecal, and intestinal content (Student’s t-test; * p ≤ 0.002; ** p ≤ 0.001).
Figure 1.
Comparison of alpha diversity indices between metformin (n = 20) and control (n = 18) treatment groups in stool, cecal, and intestinal content (Student’s t-test; * p ≤ 0.002; ** p ≤ 0.001).

Figure 2.
2D principal coordinate analysis (PCoA) plots created using weighted UniFrac distances. Adonis statistical Table 999. permutations; R2 = 0.224, 0.388, and 0.377 for stool, cecal, and intestinal content, respectively, p = 0.001).
Figure 2.
2D principal coordinate analysis (PCoA) plots created using weighted UniFrac distances. Adonis statistical Table 999. permutations; R2 = 0.224, 0.388, and 0.377 for stool, cecal, and intestinal content, respectively, p = 0.001).

Figure 3.
(a) Taxonomic distribution of the digestive microbiota in mice infected with Helicobacter pylori at the family level. (b) Histogram obtained using linear discriminant analysis (LDA) effect size analysis (LEfSe) to identify differentially abundant taxa in fecal, cecal, and intestinal samples. Genera and families with LDA scores >2 were identified as significantly more abundant between the metformin and control groups (p < 0.01).
Figure 3.
(a) Taxonomic distribution of the digestive microbiota in mice infected with Helicobacter pylori at the family level. (b) Histogram obtained using linear discriminant analysis (LDA) effect size analysis (LEfSe) to identify differentially abundant taxa in fecal, cecal, and intestinal samples. Genera and families with LDA scores >2 were identified as significantly more abundant between the metformin and control groups (p < 0.01).

Figure 4.
Growth of different bacterial strains at different metformin concentrations after 24 h of anaerobic incubation. Ns, non-significant. ** p < 0.01; *** p < 0.001; **** p < 0.0001 (Student’s t-test; n = 3).
Figure 4.
Growth of different bacterial strains at different metformin concentrations after 24 h of anaerobic incubation. Ns, non-significant. ** p < 0.01; *** p < 0.001; **** p < 0.0001 (Student’s t-test; n = 3).

Figure 5.
Differentially enriched Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways (relative abundance > 0.001%) in intestinal microbiota (p < 0.05). KEGG pathways implicated in carbohydrate metabolism are indicated with green text.
Figure 5.
Differentially enriched Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways (relative abundance > 0.001%) in intestinal microbiota (p < 0.05). KEGG pathways implicated in carbohydrate metabolism are indicated with green text.

Figure 6.
Potential functional pathways in the gut microbiota of metformin and control group mice. (a) PCoA plot comparing the microbiota of the metformin and control groups based on potential functional pathways identified using Bray–Curtis distances. Adonis statistical tests showed significant differences between the two groups (999 permutations, R2 = 0.103, 0.318, and 0.310 for stool, cecal, and intestinal content, respectively, p = 0.032 for stool, p = 0.001 for cecal and intestinal content). (b) Characteristics of differential KEGG pathway numbers in stool, cecal, and intestinal content. Red and blue circles indicate the numbers of KEGG pathways predicted to be relatively overexpressed in the metformin and control group, respectively. (c) Proportion of sequences of specific genes coding for nitrate reductase and nitrite reductase enzyme in the intestinal microbiota for the metformin (n = 20) and control (n = 18) groups. * p < 0.05; **** p < 0.0001; Mann–Whitney U test.
Figure 6.
Potential functional pathways in the gut microbiota of metformin and control group mice. (a) PCoA plot comparing the microbiota of the metformin and control groups based on potential functional pathways identified using Bray–Curtis distances. Adonis statistical tests showed significant differences between the two groups (999 permutations, R2 = 0.103, 0.318, and 0.310 for stool, cecal, and intestinal content, respectively, p = 0.032 for stool, p = 0.001 for cecal and intestinal content). (b) Characteristics of differential KEGG pathway numbers in stool, cecal, and intestinal content. Red and blue circles indicate the numbers of KEGG pathways predicted to be relatively overexpressed in the metformin and control group, respectively. (c) Proportion of sequences of specific genes coding for nitrate reductase and nitrite reductase enzyme in the intestinal microbiota for the metformin (n = 20) and control (n = 18) groups. * p < 0.05; **** p < 0.0001; Mann–Whitney U test.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Comparison of the relative abundance of bacteria between the metformin and control treatment groups at all Table 1. 10−4 were highlighted, red and blue indicate greater abundance in the metformin and control groups, respectively. Ctrl: control, Met: metformin, NS: non-significant (p > 0.05).
Table 1.
Comparison of the relative abundance of bacteria between the metformin and control treatment groups at all Table 1. 10−4 were highlighted, red and blue indicate greater abundance in the metformin and control groups, respectively. Ctrl: control, Met: metformin, NS: non-significant (p > 0.05).
| Stools | Caecal Content | Intestinal Content | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control (%) | Metformin (%) | p | Control (%) | Metformin (%) | p | Control (%) | Metformin (%) | p | ||||
| Phylum | Firmicutes | 71.21 | 62.02 | NS | Firmicutes | 91.78 | 74.91 | 0.000004 | Firmicutes | 54.14 | 22.63 | 0.000042 |
| Bacteroidetes | 17.94 | 6.504 | 0.000068 | Bacteroidetes | 5.637 | 4.666 | NS | Actinobacteria | 37.08 | 70.97 | 0.000015 | |
| Actinobacteria | 8.519 | 28.76 | 0.000564 | Actinobacteria | 1.844 | 18.53 | 0.000003 | Proteobacteria | 7.367 | 5.667 | NS | |
| Proteobacteria | 2.157 | 2.455 | NS | Proteobacteria | 0.69 | 1.682 | 0.000717 | Bacteroidetes | 1.046 | 0.4659 | 0.0296 | |
| Verrucomicrobia | 0.1462 | 0.248 | NS | Verrucomicrobia | 0.04292 | 0.2031 | 0.000002 | Verrucomicrobia | 0.2619 | 0.1808 | NS | |
| Class | Clostridia | 64.08 | 59.39 | NS | Clostridia | 90.33 | 72.38 | <0.000001 | Clostridia | 25.2 | 2.885 | 0.000009 |
| Bacteroidia | 17.94 | 6.504 | 0.000068 | Bacteroidia | 5.637 | 4.666 | NS | Actinobacteria | 20.79 | 67.44 | <0.000001 | |
| Actinobacteria | 7.277 | 28.14 | 0.000283 | Actinobacteria | 1.393 | 18.15 | 0.000002 | Erysipelotrichi | 18.29 | 19.24 | NS | |
| Erysipelotrichi | 3.741 | 2.467 | NS | Erysipelotrichi | 0.8205 | 2.44 | NS | Coriobacteriia | 16.29 | 3.529 | 0.000095 | |
| Bacilli | 3.386 | 0.1616 | 0.00416 | Betaproteobacteria | 0.6795 | 1.667 | 0.000663 | Bacilli | 10.65 | 0.5026 | 0.018 | |
| Betaproteobacteria | 2.142 | 2.427 | NS | Bacilli | 0.6257 | 0.08574 | 0.0167 | Betaproteobacteria | 6.716 | 4.445 | NS | |
| Coriobacteriia | 1.241 | 0.6206 | 0.0301 | Coriobacteriia | 0.451 | 0.3785 | NS | Bacteroidia | 1.044 | 0.4628 | 0.0294 | |
| Verrucomicrobiae | 0.1462 | 0.248 | NS | Verrucomicrobiae | 0.04292 | 0.2031 | 0.000002 | Alphaproteobacteria | 0.5376 | 1.076 | NS | |
| Verrucomicrobiae | 0.2619 | 0.1808 | NS | |||||||||
| Order | Clostridiales | 64.08 | 59.39 | NS | Clostridiales | 90.33 | 72.38 | <0.000001 | Clostridiales | 25.2 | 2.885 | 0.000009 |
| Bacteroidales | 17.94 | 6.504 | 0.000068 | Bacteroidales | 5.637 | 4.666 | NS | Bifidobacteriales | 20.79 | 67.44 | <0.000001 | |
| Bifidobacteriales | 7.277 | 28.14 | 0.000283 | Bifidobacteriales | 1.392 | 18.15 | 0.000002 | Erysipelotrichales | 18.29 | 19.24 | NS | |
| Erysipelotrichales | 3.741 | 2.467 | NS | Erysipelotrichales | 0.8205 | 2.44 | NS | Coriobacteriales | 16.29 | 3.529 | 0.000095 | |
| Burkholderiales | 2.142 | 2.427 | NS | Burkholderiales | 0.6795 | 1.667 | 0.000663 | Bacillales | 7.818 | 0.05888 | 0.0213 | |
| Bacillales | 1.779 | 0.02667 | 0.0147 | Coriobacteriales | 0.451 | 0.3785 | NS | Burkholderiales | 6.716 | 4.445 | NS | |
| Lactobacillales | 1.606 | 0.135 | 0.00112 | Bacillales | 0.3566 | 0.01136 | 0.0275 | Lactobacillales | 2.833 | 0.4437 | 0.0178 | |
| Coriobacteriales | 1.241 | 0.6206 | 0.0301 | Lactobacillales | 0.2691 | 0.07438 | 0.014 | Bacteroidales | 1.044 | 0.4628 | 0.0294 | |
| Verrucomicrobiales | 0.1462 | 0.248 | NS | Verrucomicrobiales | 0.04292 | 0.2031 | 0.000002 | Rickettsiales | 0.5069 | 1.056 | NS | |
| Verrucomicrobiales | 0.2619 | 0.1808 | NS | |||||||||
| Family | Lachnospiraceae | 34.13 | 34.93 | NS | Lachnospiraceae | 57.86 | 43.3 | 0.00035 | Bifidobacteriaceae | 20.79 | 67.44 | <0.000001 |
| Rikenellaceae | 16.58 | 5.729 | 0.000128 | Ruminococcaceae | 18.02 | 18.98 | NS | Lachnospiraceae | 19.8 | 2.11 | 0.000009 | |
| Ruminococcaceae | 14.88 | 15.05 | NS | Rikenellaceae | 5.371 | 4.218 | NS | Erysipelotrichaceae | 18.29 | 19.24 | NS | |
| Bifidobacteriaceae | 7.277 | 28.14 | 0.000283 | Bifidobacteriaceae | 1.392 | 18.15 | 0.000002 | Coriobacteriaceae | 16.29 | 3.529 | 0.000095 | |
| Erysipelotrichaceae | 3.741 | 2.467 | NS | Erysipelotrichaceae | 0.8205 | 2.44 | NS | Alcaligenaceae | 6.716 | 4.445 | NS | |
| Alcaligenaceae | 2.138 | 2.427 | NS | Alcaligenaceae | 0.6795 | 1.667 | 0.000663 | Bacillaceae | 5.125 | 0.002976 | 0.0411 | |
| Aerococcaceae | 1.521 | 0.1177 | 0.00143 | [Mogibacteriaceae] | 0.579 | 0.473 | 0.0326 | Aerococcaceae | 2.499 | 0.2731 | 0.0228 | |
| Bacillaceae | 1.361 | 0 | 0.019 | Coriobacteriaceae | 0.451 | 0.3785 | NS | Planococcaceae | 2.439 | 0.001683 | 0.00703 | |
| S24-7 | 1.358 | 0.7749 | 0.0403 | S24-7 | 0.266 | 0.4476 | 0.0237 | Ruminococcaceae | 1.95 | 0.3866 | 0.00399 | |
| Coriobacteriaceae | 1.241 | 0.6206 | 0.0301 | Bacillaceae | 0.2608 | 0 | 0.0373 | S24-7 | 0.7812 | 0.4473 | NS | |
| [Mogibacteriaceae] | 0.548 | 0.3557 | 0.00734 | Aerococcaceae | 0.2524 | 0.0623 | 0.013 | [Mogibacteriaceae] | 0.4774 | 0.03272 | 0.0223 | |
| Planococcaceae | 0.2407 | 0 | 0.0147 | Verrucomicrobiaceae | 0.04292 | 0.2031 | 0.000002 | Rikenellaceae | 0.2633 | 0.01555 | 0.0232 | |
| Verrucomicrobiaceae | 0.1462 | 0.248 | NS | Verrucomicrobiaceae | 0.2619 | 0.1808 | NS | |||||
| Staphylococcaceae | 0.2544 | 0.05422 | NS | |||||||||
| Lactobacillaceae | 0.2505 | 0.0467 | 0.00019 | |||||||||
| Enterococcaceae | 0.08181 | 0.1239 | NS | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Jauvain, M.; Courtois, S.; Lehours, P.; Bessède, E. Metformin Modifies the Gut Microbiota of Mice Infected with Helicobacter pylori. Pharmaceuticals 2021, 14, 329. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040329
AMA Style
Jauvain M, Courtois S, Lehours P, Bessède E. Metformin Modifies the Gut Microbiota of Mice Infected with Helicobacter pylori. Pharmaceuticals. 2021; 14(4):329. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040329
Chicago/Turabian StyleJauvain, Marine, Sarah Courtois, Philippe Lehours, and Emilie Bessède. 2021. "Metformin Modifies the Gut Microbiota of Mice Infected with Helicobacter pylori" Pharmaceuticals 14, no. 4: 329. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040329
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.