
Influence of Pathogenic and Metabolic Genes on the Pharmacogenetics of Mood Disorders in Alzheimer’s Disease

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Sex-Related Biochemical, Hematological, Metabolic and Clinical Phenotypes
2.2. Cognition
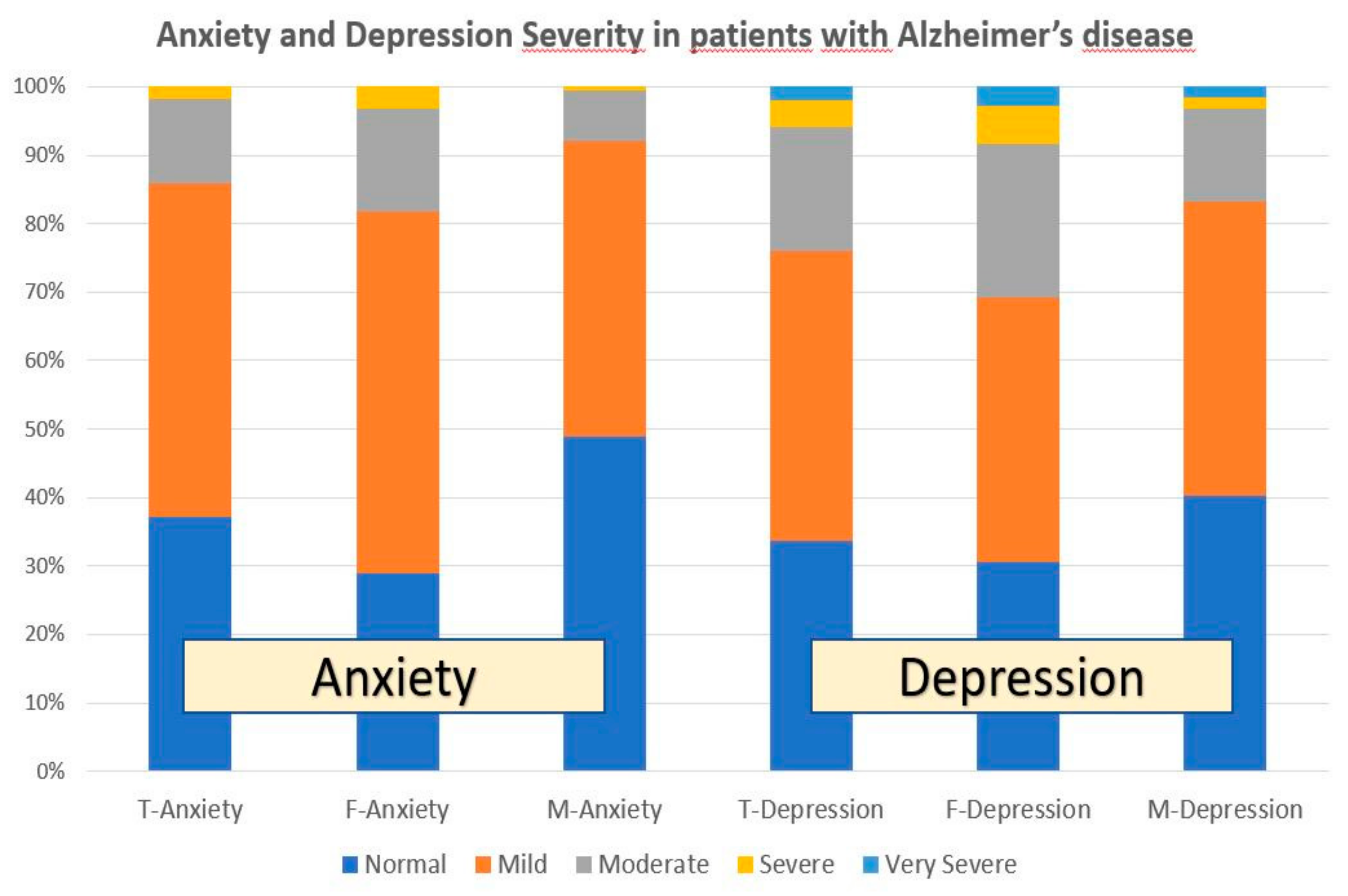
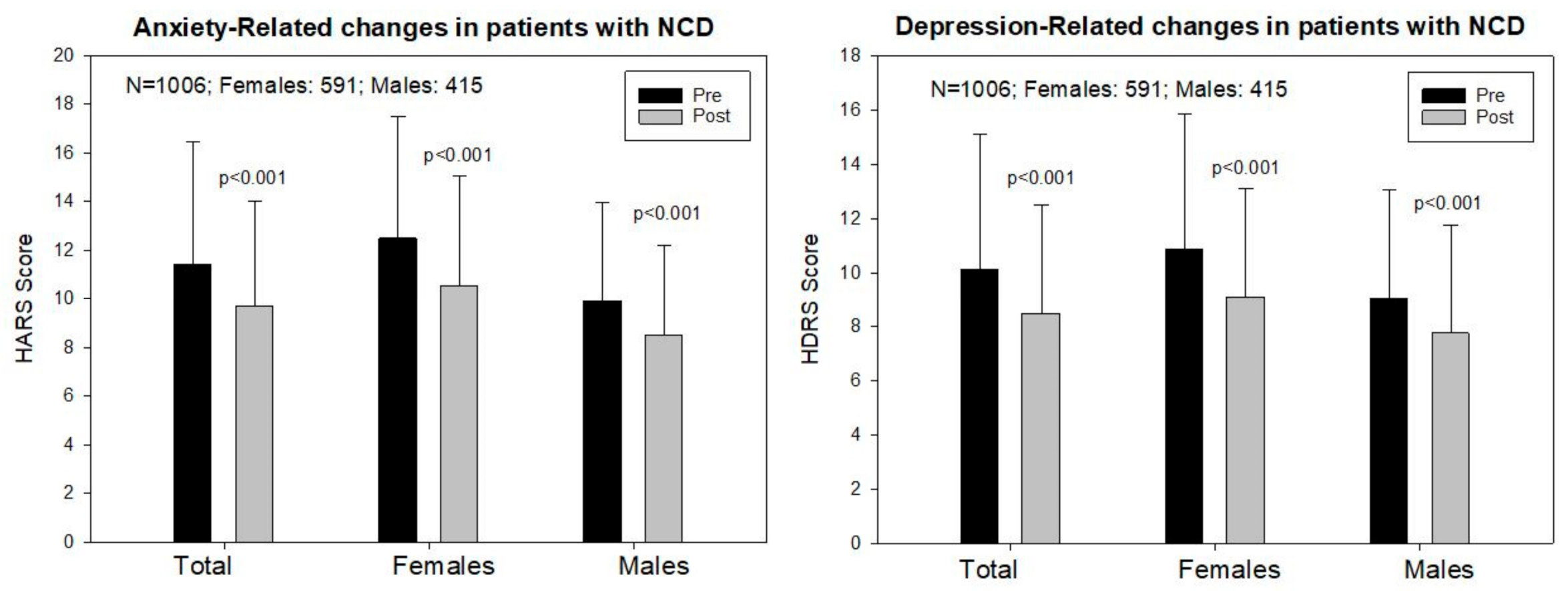
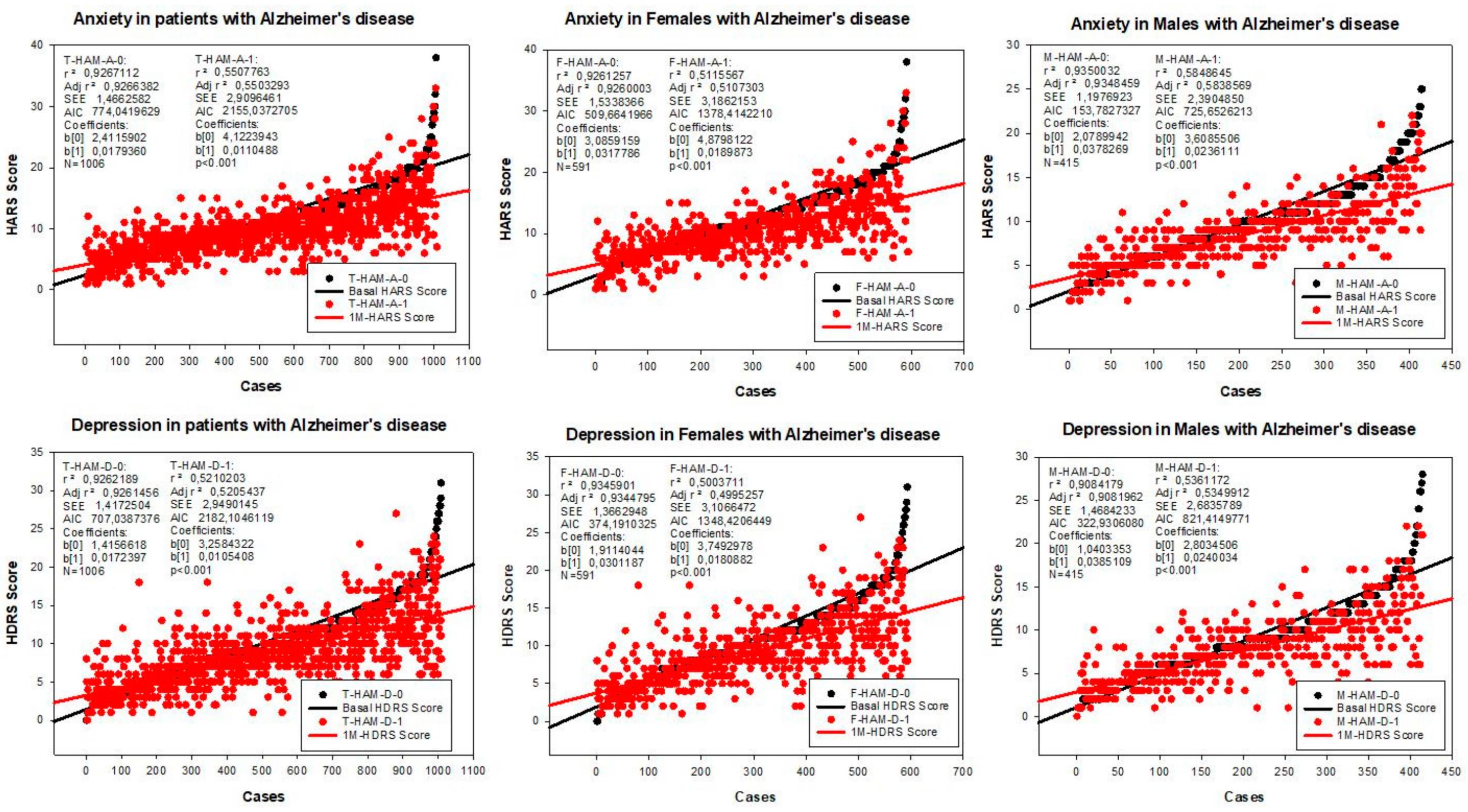
2.3. Anxiety
2.4. Depression
2.5. Pharmacogenomics
3. Discussion
3.1. Parametric Differences
3.2. Pharmacogenetic Determinants
3.3. Metabolic Genes
3.4. Pharmacogenetics of Antidepressants
3.5. Pharmacogenetics of Anxiolytics
4. Materials and Methods
4.1. Patients and Clinical Protocol
4.2. Genotyping
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Cacabelos, R. Pharmacogenomics of Cognitive Dysfunction and Neuropsychiatric Disorders in Dementia. Int. J. Mol. Sci. 2020, 21, 3059. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Fernández-Novoa, L.; Lombardi, V.; Kubota, Y.; Takeda, M. Molecular genetics of Alzheimer’s disease and aging. Meth. Find. Exp. Clin. Pharmacol. 2005, 27, 1–573. [Google Scholar]
- Cacabelos, R. Pharmacogenomics in Alzheimer’s disease. Methods Mol. Biol. 2008, 448, 213–357. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Cacabelos, P.; Torrellas, C.; Tellado, I.; Carril, J.C. Pharmacogenomics of Alzheimer’s disease: Novel therapeutic strategies for drug development. Methods Mol. Biol. 2014, 1175, 323–556. [Google Scholar] [CrossRef]
- Cacabelos, R.; Carril, J.C.; Cacabelos, P.; Teijido, O.; Goldgaber, D. Pharmacogenomics of Alzheimer’s Disease: Genetic determinants of phenotypic variation and therapeutic outcome. J. Genomic Med. Pharm. 2016, 1, 151–209. [Google Scholar]
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and Management of Dementia: Review. JAMA 2019, 322, 1589–1599. [Google Scholar] [CrossRef]
- Defrancesco, M.; Marksteiner, J.; Kemmler, G.; Dal-Bianco, P.; Ransmayr, G.; Benke, T.; Mosbacher, J.; Holler, Y.; Schmidt, R. Specific Neuropsychiatric Symptoms Are Associated with Faster Progression in Alzheimer’s Disease: Results of the Prospective Dementia Registry (PRODEM-Austria). J. Alzheimers Dis. 2020, 73, 125–133. [Google Scholar] [CrossRef]
- Sr, P.A.A.; DeFeis, B.; De Wit, L.; O’Shea, D.; Mejia, A.; Chandler, M.; Locke, D.E.C.; Fields, J.; Phatak, V.; Dean, P.M.; et al. Functional ability is associated with higher adherence to behavioral interventions in mild cognitive impairment. Clin. Neuropsychol. 2020, 34, 937–955. [Google Scholar] [CrossRef] [Green Version]
- Ilik, F.; Büyükgöl, H.; Kayhan, F.; Ertem, D.H.; Ekiz, T. Effects of Inappropriate Sexual Behaviors and Neuropsychiatric Symptoms of Patients with Alzheimer Disease and Caregivers’ Depression on Caregiver Burden. J. Geriatr. Psychiatry Neurol. 2020, 33, 243–249. [Google Scholar] [CrossRef]
- Burhanullah, M.H.; Tschanz, J.T.; Peters, M.E.; Leoutsakos, J.M.; Matyi, J.; Lyketsos, C.G.; Nowrangi, M.A.; Rosenberg, P.B. Neuropsychiatric Symptoms as Risk Factors for Cognitive Decline in Clinically Normal Older Adults: The Cache County Study. Am. J. Geriatr. Psychiatry 2020, 28, 64–71. [Google Scholar] [CrossRef]
- Lai, A.X.; Kaup, A.R.; Yaffe, K.; Byers, A.L. High Occurrence of Psychiatric Disorders and Suicidal Behavior across Dementia Subtypes. Am. J. Geriatr. Psychiatry 2018, 26, 1191–1201. [Google Scholar] [CrossRef]
- Cummings, J.; Lai, T.J.; Hemrungrojn, S.; Mohandas, E.; Yun Kim, S.; Nair, G.; Dash, A. Role of Donepezil in the Management of Neuropsychiatric Symptoms in Alzheimer’s Disease and Dementia with Lewy Bodies. CNS Neurosci. Ther. 2016, 22, 159–166. [Google Scholar] [CrossRef]
- Deardorff, W.J.; Grossberg, G.T. Behavioral and psychological symptoms in Alzheimer’s dementia and vascular dementia. Handb. Clin. Neurol. 2019, 165, 5–32. [Google Scholar] [CrossRef]
- Van de Beek, M.; van Steenoven, I.; Ramakers, I.H.G.B.; Aalten, P.; Koek, H.L.; Olde Rikkert, M.G.M.; Mannien, J.; de Jong, F.J.; Lemstra, A.W.; van der Flier, W.M. Trajectories and Determinants of Quality of Life in Dementia with Lewy Bodies and Alzheimer’s Disease. J. Alzheimers Dis. 2019, 70, 389–397. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Wilson, L.; Kornak, J.; Dudley, R.A.; Merrilees, J.; Bonasera, S.J.; Byrne, C.M.; Lee, K.; Chiong, W.; Miller, B.L.; et al. The costs of dementia subtypes to California Medicare fee-for-service, 2015. Alzheimers Dement. 2019, 15, 899–906. [Google Scholar] [CrossRef]
- Desmarais, P.; Weidman, D.; Wassef, A.; Bruneau, M.A.; Friedland, J.; Bajsarowicz, P.; Thibodeau, M.P.; Herrmann, N.; Nguyen, Q.D. The Interplay between Post-traumatic Stress Disorder and Dementia: A Systematic Review. Am. J. Geriatr. Psychiatry 2020, 28, 46–60. [Google Scholar] [CrossRef]
- Cacabelos, R. Pharmacogenetic considerations when prescribing cholinesterase inhibitors for the treatment of Alzheimer’s disease. Exp. Opin. Drug Metab. Toxicol. 2020, 16, 673–701. [Google Scholar] [CrossRef]
- Cacabelos, R. Have there been improvement in Alzheimer’s disease drug discovery over the past 5 years? Expert Opin. Drug Discov. 2018, 13, 523–538. [Google Scholar] [CrossRef]
- Pirker-Kees, A.; Dal-Bianco, P.; Schmidt, R. Effects of Psychotropic Medication on Cognition, Caregiver Burden, and Neuropsychiatric Symptoms in Alzheimer’s Disease over 12 Months: Results from a Prospective Registry of Dementia in Austria (PRODEM). J. Alzheimers Dis. 2019, 71, 623–630. [Google Scholar] [CrossRef]
- Bravo-José, P.; Sáez-Lleó, C.I.; Peris-Martí, J.F. Deprescribing antipsychotics in long term care patients with dementia. Farm. Hosp. 2019, 43, 140–145. [Google Scholar] [CrossRef]
- Mantri, S.; Fullard, M.; Gray, S.L.; Weintraub, D.; Hubbard, R.A.; Hennessy, S.; Willis, A.W. Patterns of Dementia Treatment and Frank Prescribing Errors in Older Adults With Parkinson Disease. JAMA Neurol. 2019, 76, 41–49. [Google Scholar] [CrossRef]
- Cacabelos, R.; Cacabelos, N.; Carril, J.C. The role of pharmacogenomics in adverse drug reactions. Expert Rev. Clin. Pharmacol. 2019, 12, 407–442. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R. Population-level pharmacogenomics for precision drug development in dementia. Expert Rev. Precis. Med. Drug Dev. 2018, 3, 163–188. [Google Scholar] [CrossRef]
- Cacabelos, R. World Guide for Drug Use and Pharmacogenomics; EuroEspes Publishing: Corunna, Spain, 2012. [Google Scholar]
- Cacabelos, R. Pharmacogenomic of drugs to treat brain disorders. Expert Rev. Precis. Med. Drug Dev. 2020, 16, 673–701. [Google Scholar] [CrossRef]
- Cacabelos, R.; Torrellas, C.; Teijido, O.; Carril, J.C. Pharmacogenetic considerations in the treatment of Alzheimer’s disease. Pharmacogenomics 2016, 17, 1041–1074. [Google Scholar] [CrossRef]
- Kozyra, M.; Ingelman-Sundberg, M.; Lauschke, V.M. Rare genetic variants in cellular transporters, metabolic enzymes, and nuclear receptors can be important determinants of interindividual differences in drug response. Genet. Med. 2017, 19, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.W.; Chen, X.W.; Sneed, K.B.; Yang, Y.X.; Zhang, X.; He, Z.X.; Chow, K.; Yang, T.; Duan, W.; Zhou, S.F. Clinical association between pharmacogenomics and adverse drug reactions. Drugs 2015, 75, 589–631. [Google Scholar] [CrossRef]
- Marcath, L.A.; Pasternak, A.L.; Hertz, D.L. Challenges to assess substrate-dependent allelic effects in CYP450 enzymes and the potential clinical implications. Pharmacogenom. J. 2019, 19, 501–515. [Google Scholar] [CrossRef]
- Lesche, D.; Mostafa, S.; Everall, I.; Pantelis, C.; Bousman, C. Impact of CYP1A2, CYP2C19, and CYP2D6 genotype- and phenoconversion-predicted enzyme activity on clozapine exposure and symptom severity. Pharmacogenom. J. 2020, 20, 192–201. [Google Scholar] [CrossRef]
- Cacabelos, R.; Tellado, I.; Cacabelos, P. The epigenetic machinery in the life cycle and pharmacoepigenetics. In Pharmacoepigenetics; Cacabelos, R., Ed.; Academic Press/Elsevier: Oxford, UK, 2019; pp. 1–100. [Google Scholar]
- Cacabelos, R.; Carril, J.C.; Sanmartín, A.; Cacabelos, P. Pharmacoepigenetic processors: Epigenetic drugs, Drug resistance, Toxicoepigenetics, and Nutriepigenetics. In Pharmacoepigenetics; Cacabelos, R., Ed.; Academic Press/Elsevier: Oxford, UK, 2019; pp. 191–424. [Google Scholar]
- Cacabelos, R.; Fernández-Novoa, L.; Martínez-Bouza, R.; McKay, A.; Carril, J.C.; Lombardi, V.; Corzo, L.; Carrera, I.; Tellado, I.; Nebril, L.; et al. Future trends in the pharmacogenomics of brain disorders and dementia: Influence of APOE and CYP2D6 variants. Pharmaceuticals 2010, 3, 3040–3100. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R. Pharmacogenomics of Alzheimer’s and Parkinson’s diseases. Neurosci. Lett. 2020, 726, 133807. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Martínez, R.; Fernández-Novoa, L.; Carril, J.C.; Lombardi, V.; Carrera, I.; Corzo, L.; Tellado, I.; Leszek, J.; McKay, A.; et al. Genomics of dementia: APOE- and CYP2D6-related pharmacogenetics. Intern. J. Alzheimer Dis. 2012, 2012, 518901. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R. Donepezil in Alzheimer’s disease: From conventional trials to pharmacogenetics. Neuropsychiat. Dis. Treat. 2007, 3, 303–333. [Google Scholar]
- Chi, S.; Wang, C.; Jiang, T.; Zhu, X.C.; Yu, J.T.; Tan, L. The prevalence of depression in Alzheimer’s disease: A systematic review and meta-analysis. Curr. Alzheimer Res. 2015, 12, 189–198. [Google Scholar] [CrossRef]
- Kuring, J.K.; Mathias, J.L.; Ward, L. Prevalence of Depression, Anxiety and PTSD in People with Dementia: A Systematic Review and Meta-Analysis. Neuropsychol. Rev. 2018, 28, 393–416. [Google Scholar] [CrossRef]
- Sol, K.; Zaheed, A.B.; Kraal, A.Z.; Sharifian, N.; Arce Rentería, M.; Zahodne, L.B. Psychological Predictors of Memory Decline in a Racially and Ethnically Diverse Longitudinal Sample of Older Adults in the United States. Int. J. Geriatr. Psychiatry 2019. [Google Scholar] [CrossRef]
- Bennett, S.; Thomas, A.J. Depression and dementia: Cause, consequence or coincidence? Maturitas 2014, 79, 184–190. [Google Scholar] [CrossRef]
- Norton, J.; Carrière, I.; Pérès, K.; Gabelle, A.; Berr, C.; Ritchie, K.; Ancelin, M.L. Sex-specific depressive symptoms as markers of pre-Alzheimer dementia: Findings from the Three-City cohort study. Transl. Psychiatry 2019, 9, 291. [Google Scholar] [CrossRef] [Green Version]
- Youn, H.; Lee, S.; Han, C.; Kim, S.H.; Jeong, H.G. Association between brain amyloid accumulation and neuropsychological characteristics in elders with depression and mild cognitive impairment. Int. J. Geriatr. Psychiatry 2019, 34, 1907–1915. [Google Scholar] [CrossRef]
- Capogna, E.; Manca, R.; De Marco, M.; Hall, A.; Soininen, H.; Venneri, A. Understanding the effect of cognitive/brain reserve and depression on regional atrophy in early Alzheimer’s disease. Postgrad. Med. 2019, 131, 533–538. [Google Scholar] [CrossRef]
- Fischer, C.E.; Kortebi, I.; Karameh, W.K.; Kumar, S.; Gallagher, D.; Golas, A.; Munoz, D.; Barfett, J.; Butter, M.A.; Bowie, C.R.; et al. Examining the Link Between Cardiovascular Risk Factors and Neuropsychiatric Symptoms in Mild Cognitive Impairment and Major Depressive Disorder in Remission. J. Alzheimers Dis. 2019, 67, 1305–1311. [Google Scholar] [CrossRef]
- Becker, E.; Orellana Rios, C.L.; Lahmann, C.; Rücker, G.; Bauer, J.; Boeker, M. Anxiety as a risk factor of Alzheimer’s disease and vascular dementia. Br. J. Psychiatry 2018, 213, 654–660. [Google Scholar] [CrossRef] [Green Version]
- Santabárbara, J.; Lipnicki, D.M.; Bueno-Notivol, J.; Olaya-Guzmán, B.; Villagrasa, B.; López-Antón, R. Updating the evidence for an association between anxiety and risk of Alzheimer’s disease: A meta-analysis of prospective cohort studies. J. Affect. Disord. 2020, 262, 397–404. [Google Scholar] [CrossRef]
- Baillon, S.; Gasper, A.; Wilson-Morkeh, F.; Pritchard, M.; Jesu, A.; Velayudhan, L. Prevalence and Severity of Neuropsychiatric Symptoms in Early- Versus Late-Onset Alzheimer’s Disease. Am. J. Alzheimers Dis. Other Demen. 2019, 34, 433–438. [Google Scholar] [CrossRef]
- Cacabelos, R. Molecular pathology and pharmacogenomics in Alzheimer’s disease: Polygenic-related effects of multifactorial treatments on cognition, anxiety and depression. Methods Find. Exp. Clin. Pharmacol. 2007, 29, 1–91. [Google Scholar]
- Cacabelos, R.; Goldgaber, D.; Vostrov, A.; Matsuki, H.; Torrellas, C.; Corzo, D.; Carril, J.C.; Roses, A.D. APOE-TOMM40 in the Pharmacogenomics of demetia. J. Pharm. Pharm. 2014, 5, 135. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R.; Carril, J.C.; Cacabelos, N.; Kazantsev, A.G.; Vostrov, A.V.; Corzo, L.; Cacabelos, P.; Goldgaber, D. Sirtuins in Alzheimer’s Disease: SIRT2-Related GenoPhenotypes and Implications for PharmacoEpiGenetics. Int. J. Mol. Sci. 2019, 20, 1249. [Google Scholar] [CrossRef] [Green Version]
- Ni, H.; Xu, M.; Zhan, G.L.; Fan, Y.; Zhou, H.; Jiang, H.Y.; Lu, W.H.; Tan, L.; Zhang, D.F.; Yao, Y.G.; et al. The GWAS Risk Genes for Depression May Be Actively Involved in Alzheimer’s Disease. J. Alzheimers Dis. 2018, 64, 1149–1161. [Google Scholar] [CrossRef]
- Cacabelos, R. Pleiotropy and promiscuity in pharmacogenomics for the treatment of Alzheimer’s disease and related risk factors. Future Neurol. 2018, 13, 71–86. [Google Scholar] [CrossRef]
- Cacabelos, R.; Torrellas, C. Pharmacogenomics of antidepressants. HSOA J. Psychiatry Depress. Anxiety 2015, 1, 001. [Google Scholar] [CrossRef] [Green Version]
- Orgeta, V.; Tabet, N.; Nilforooshan, R.; Howard, R. Efficacy of Antidepressants for Depression in Alzheimer’s Disease: Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2017, 58, 725–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassano, T.; Calcagnini, S.; Carbone, A.; Bukke, V.N.; Orkisz, S.; Villani, R.; Romano, A.; Avolio, C.; Gaetani, S. Pharmacological Treatment of Depression in Alzheimer’s Disease: A Challenging Task. Front. Pharmacol. 2019, 10, 1067. [Google Scholar] [CrossRef] [Green Version]
- Diniz, B.S.; Butters, M.A.; Albert, S.M.; Dew, M.A.; Reynolds, C.F. Late-life depression and risk of vascular dementia and Alzheimer’s disease: Systematic review and meta-analysis of community-based cohort studies. Br. J. Psychiatry 2013, 202, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.Y.; Stachiv, I.; Nikolai, T. Association of Late Life Depression, (Non-) Modifiable Risk and Protective Factors with Dementia and Alzheimer’s Disease: Literature Review on Current Evidences, Preventive Interventions and Possible Future Trends in Prevention and Treatment of Dementia. Int. J. Environ. Res. Public. Health 2020, 17, 7475. [Google Scholar] [CrossRef]
- Khundakar, A.A.; Thomas, A.J. Neuropathology of depression in Alzheimer’s disease: Current knowledge and the potential for new treatments. J. Alzheimers Dis. 2015, 44, 27–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagnino, P.; Ugarte, M.J.; Morales, F.; Gonzalez, S.; Saralegui, D.; Ehrenthal, I.C. Risk factors for adult depression: Adverse Childhood experiences and personality functioning. Front. Psychol. 2020, 11, 594698. [Google Scholar] [CrossRef] [PubMed]
- Mullins, N.; Lewis, C.M. Genetics of Depression: Progress at Last. Curr. Psychiatry Rep. 2017, 19, 43. [Google Scholar] [CrossRef] [Green Version]
- Howard, D.M.; Adams, M.J.; Clarke, T.K.; Hafferty, J.D.; Gibson, J.; Shirali, M.; Coleman, J.R.I.; Hagenaars, S.P.; Ward, J.; Wigmore, E.M.; et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat. Neurosci. 2019, 22, 343–352. [Google Scholar] [CrossRef] [Green Version]
- El Haj, M.; Altintas, E.; Chapelet, G.; Kapogiannis, D.; Gallouj, K. High depression and anxiety in people with Alzheimer’s disease living in retirement homes during the COVID-19 crisis. Psychiatry Res. 2020, 291, 113294. [Google Scholar] [CrossRef]
- Cacabelos, R. Trial-and-Error versus Personalized Treatment in Depression: The Power of Pharmacogenomics. J. Psychiatry Depress. Anxiety 2016, 2. [Google Scholar] [CrossRef] [Green Version]
- Torrellas, C.; Carril, J.C.; Cacabelos, R. Optimization of antidepressant use with pharmacogenetic strategies. Curr. Genom. 2017, 18, 442–449. [Google Scholar] [CrossRef] [Green Version]
- Thase, M.E.; Parikh, S.V.; Rothschild, A.J.; Dunlop, B.W.; De Battista, C.; Conway, C.R.; Mondimore, F.M.; Shelton, R.C.; Macaluso, M.; Li, J.; et al. Impact of Pharmacogenomics on Clinical Outcomes for Patients Taking Medications With Gene-Drug Interactions in a Randomized Controlled Trial. J. Clin. Psychiatry 2019, 80, 19m12910. [Google Scholar] [CrossRef] [Green Version]
- Maggo, S.D.S.; Sycamore, K.L.V.; Miller, A.L.; Kennedy, M.A. The Three Ps: Psychiatry, Pharmacy, and Pharmacogenomics, a Brief Report from New Zealand. Front. Psychiatry 2019, 10, 690. [Google Scholar] [CrossRef]
- Eugene, A.R. Optimizing drug selection in psychopharmacology based on 40 significant CYP2C19- and CYP2D6-biased adverse drug reactions of selective serotonin reuptake inhibitors. PeerJ 2019, 7, e7860. [Google Scholar] [CrossRef]
- Kanders, S.H.; Pisanu, C.; Bandstein, M.; Jonsson, J.; Castelao, E.; Pistis, G.; Gholam-Rezaee, M.; Eap, C.B.; Preisig, M.; Schioth, H.B.; et al. A pharmacogenetic risk score for the evaluation of major depression severity under treatment with antidepressants. Drug Dev. Res. 2020, 81, 102–113. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, F.F.; Berretta, J.M.; de Almeida Junior, G.V.; de Almeida, S.S.; Chen, E.S.; Smith, M.C.; Bertolucci, P.H.F. Pharmacogenetic analyses of variations of measures of cardiovascular risk in Alzheimer’s dementia. Indian J. Med. Res. 2019, 150, 261–271. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, X.; Wang, Y.; Dong, H.; Lu, J.; Scheininger, T.; Ewers, M.; Jesse, F.; Zuo, X.; Han, Y. Anxiety correlates with cortical surface area in subjective cognitive decline: APOE ε4 carriers versus APOE ε4 non-carriers. Alzheimers Res. Ther. 2019, 11, 50. [Google Scholar] [CrossRef]
- Ehrenberg, A.J.; Suemoto, C.K.; França Resende, E.P.; Petersen, C.; Leite, R.E.P.; Rodriguez, R.D.; Ferretti-Rebustini, R.E.L.; You, M.; Oh, J.; Nitrini, R.; et al. Neuropathologic Correlates of Psychiatric Symptoms in Alzheimer’s Disease. J. Alzheimers Dis. 2018, 66, 115–126. [Google Scholar] [CrossRef]
- De Gage, S.B.; Moride, Y.; Ducruet, T.; Kurth, T.; Verdoux, H.; Tournier, M.; Pariente, A.; Bégaud, B. Benzodiazepine use and risk of Alzheimer’s disease: Case-control study. BMJ 2014, 349, g5205. [Google Scholar] [CrossRef] [Green Version]
- Nafti, M.; Sirois, C.; Kröger, E.; Carmichael, P.H.; Laurin, D. Is Benzodiazepine Use Associated with the Risk of Dementia and Cognitive Impairment-Not Dementia in Older Persons? The Canadian Study of Health and Aging. Ann. Pharmacother. 2020, 54, 219–225. [Google Scholar] [CrossRef]
- Folstein, M.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State” a Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Rosen, W.G.; Mohs, R.C.; Davis, K.L. A new rating scale for Alzheimer’s disease. Am. J. Psychiatry. 1984, 41, 1356–1364. [Google Scholar]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total | Females | Males | Differences |
|---|---|---|---|---|
| N | 1006 | 591 | 415 | |
| Age (Years) | 67.51 ± 9.62 | 67.52 ± 9.68 | 67.50 ± 9.54 | p = 0.97 |
| Systolic Blood Pressure (mm Hg) | 138.70 ± 20.06 | 137.40 ± 19.83 | 140.54 ± 1.96 | p < 0.02 |
| Diastolic Blood Pressure (mm Hg) | 79.74 ± 10.81 | 79.25 ± 10.70 | 80.45 ± 10.94 | p < 0.04 |
| Pulse (bpm) | 66.67 ± 11.71 | 68.10 ± 11.28 | 64.86 ± 12.06 | p < 0.001 |
| Weight (Kg) | 72.01 ± 13.66 | 66.84 ± 12.20 | 79.49 ± 12.12 | p < 0.001 |
| Hight (m) | 1.60 ± 0.09 | 1.54 ± 0.06 | 1.67 ± 0.06 | p < 0.001 |
| BMI (Kg/m2) | 28.14 ± 4.57 | 28.01 ± 5.11 | 28.31 ± 3.63 | p < 0.03 |
| Glucose (mg/dL) | 100.01 ± 24.91 | 96.47 ± 22.56 | 105.03 ± 27.15 | p < 0.001 |
| Cholesterol (mg/dL) | 225.69 ± 46.03 | 235.02 ± 44.92 | 212.43 ± 44.35 | p < 0.001 |
| HDL-Cholesterol (mg/dL) | 54.36 ± 14.81 | 59.42 ± 14.93 | 47.18 ± 11.27 | p < 0.001 |
| LDL-Cholesterol (mg/dL) | 148.28 ± 39.75 | 153.55 ± 40.23 | 140.80 ± 37.88 | p < 0.001 |
| Triglycerides (mg/dL) | 115.42 ± 69.97 | 108.14 ± 55.18 | 125.77 ± 85.79 | p < 0.005 |
| Urea (mg/dL) | 42.49 ± 12.44 | 41.30 ± 11.76 | 44.20 ± 13.16 | p < 0.001 |
| Creatinine (mg/dL) | 0.87 ± 0.21 | 0.79 ± 0.17 | 0.98 ± 0.22 | p < 0.001 |
| Uric Acid (mg/dL) | 4.38 ± 1.97 | 3.77 ± 1.20 | 5.26 ± 2.47 | p < 0.001 |
| Total Protein (g/dL) | 6.89 ± 0.46 | 6.90 ± 0.41 | 6.88 ± 0.52 | p = 0.99 |
| Albumin (g/dL) | 4.32 ± 0.32 | 4.31 ± 0.27 | 4.35 ± 0.38 | p < 0.05 |
| Calcium (mg/dL) | 9.20 ± 0.49 | 9.24 ± 0.46 | 9.14 ± 0.53 | p < 0.02 |
| Phosphorus (mg/dL) | 3.42 ± 0.54 | 3.52 ± 0.52 | 3.27 ± 0.52 | p < 0.001 |
| GOT/ASAT (IU/L) | 22.44 ± 19.95 | 22.57 ± 23.45 | 22.26 ± 13.53 | p = 0.66 |
| GPT/ALAT (IU/L) | 23.97 ± 20.75 | 22.57 ± 21.31 | 25.95 ± 19.79 | p < 0.001 |
| GGT (IU/L) | 30.55 ± 39.93 | 26.85 ± 37.52 | 35.79 ± 42.61 | p < 0.001 |
| Alkaline Phosphatase IU/L) | 74.69 ± 28.30 | 77.12 ± 29.20 | 71.23 ± 26.63 | p < 0.001 |
| Bilirubin (mg/dL) | 0.79 ± 2.04 | 0.78 ± 2.64 | 0.81 ± 0.41 | p < 0.001 |
| CPK (IU/L) | 92.48 ± 124.94 | 88.61 ± 153.17 | 97.98 ± 66.60 | p < 0.001 |
| LDH (IU/L) | 292.63 ± 62.05 | 303.52 ± 63.80 | 277.12 ± 56.01 | p < 0.001 |
| Na+ (mEq/L) | 142.40 ± 2.32 | 142.50 ± 2.15 | 142.26 ± 2.54 | p = 0.17 |
| K+ (mEq/L) | 4.37 ± 0.37 | 4.30 ± 0.36 | 4.46 ± 0.36 | p < 0.001 |
| Cl− (mEq/L) | 104.46 ± 2.47 | 104.64 ± 2.37 | 104.20 ± 2.60 | p < 0.01 |
| Fe2+ (µg/dL) | 87.42 ± 33.67 | 82.89 ± 31.78 | 93.81 ± 35.23 | p < 0.001 |
| Ferritin (ng/mL) | 114.81 ± 125.83 | 83.87 ± 95.10 | 158.58 ± 149.01 | p < 0.001 |
| Folate (ng/mL) | 7.24 ± 3.86 | 7.50 ± 3.92 | 6.87 ± 3.76 | p < 0.003 |
| Vitamin B12 (pg/mL) | 502.17 ± 297.90 | 516.45 ± 302.12 | 481.80 ± 290.92 | p < 0.003 |
| TSH (µIU/mL) | 1.48 ±1.77 | 1.56 ± 2.03 | 1.37 ± 1.29 | p < 0.01 |
| T4 (ng/mL) | 0.88 ± 0.18 | 0.88 ± 0.17 | 0.89 ± 0.18 | p = 0.47 |
| RBC (x106/µL) | 4.63 ± 0.44 | 4.48 ± 0.37 | 4.84 ± 0.45 | p < 0.001 |
| HCT (%) | 42.06 ± 4.05 | 40.59 ± 3.57 | 44.16 ± 3.75 | p < 0.001 |
| Hb (g/dL) | 14.04 ± 1.32 | 13.51 ± 1.06 | 14.80 ± 1.29 | p < 0.001 |
| VCM (fL) | 90.84 ± 5.02 | 90.45 ± 5.05 | 91.38 ± 4.92 | p < 0.001 |
| HCM (pg) | 30.38 ± 1.89 | 30.20 ± 1.90 | 30.64 ± 1.84 | p < 0.001 |
| CHCM (g/dL) | 33.41 ± 1.21 | 33.34 ± 1.45 | 33.51 ± 0.74 | p < 0.02 |
| ADE (RDW)(%) | 13.04 ± 1.41 | 13.06 ± 1.60 | 13.00 ± 1.09 | p = 0.74 |
| WBC (x103/µL) | 6.22 ± 1.86 | 6.02 ± 1.90 | 6.51 ± 1.76 | p < 0.001 |
| %Neutrophils | 59.64 ± 9.38 | 59.62 ± 9.23 | 59.66 ± 9.61 | p = 0.98 |
| %Lymphocytes | 30.01 ± 8.54 | 30.54 ± 8.47 | 29.25 ± 8.59 | p < 0.01 |
| %Monocytes | 7.33 ± 2.04 | 7.14 ± 2.00 | 7.61 ± 2.06 | p < 0.001 |
| %Eosinophils | 2.75 ± 2.06 | 2.61 ± 2.93 | 2.95 ± 2.03 | p < 0.001 |
| %Basophils | 0.53 ± 0.28 | 0.49 ± 0.19 | 0.59 ± 0.37 | p < 0.001 |
| PLT (x103/µL) | 225.13 ± 62.29 | 237.40 ± 59.71 | 207.61 ± 61.78 | p < 0.001 |
| VPM (fL) | 8.36 ± 0.91 | 8.27 ± 0.89 | 8.48 ± 0.96 | p < 0.001 |
| ESR (mm/hr) | 19.08 ± 15.75 | 21.66 ± 15.38 | 15.37 ± 15.55 | p < 0.001 |
| EKG | N: 51.18%; AN: 47.82% | N: 56.64% AN: 43.36% | N: 45.00% AN: 55.00% | p < 0.001 * |
| MMSE Score (30) | 23.16 ± 5.95 | 22.42 ± 5.88 | 24.22 ± 5.90 | p < 0.001 |
| ADAS-Cog | 19.14 ± 12.88 | 19.64 ± 12.71 | 18.40 | p = 0.06 |
| ADAS-Non Cog | 4.60 ± 3.82 | 5.17 ± 4.02 | 3.77 ± 3.36 | p < 0.001 |
| ADAS-Total | 22.78 ± 15.22 | 23.76 ± 15.07 | 21.36 ± 15.35 | p < 0.002 |
| HARS | 11.44 ± 5.41 | 12.49 ± 5.63 | 9.94 ± 4.69 | p < 0.001 |
| HDRS | 10.11 ± 5.21 | 10.85 ± 5.33 | 9.05 ± 4.84 | p < 0.001 |
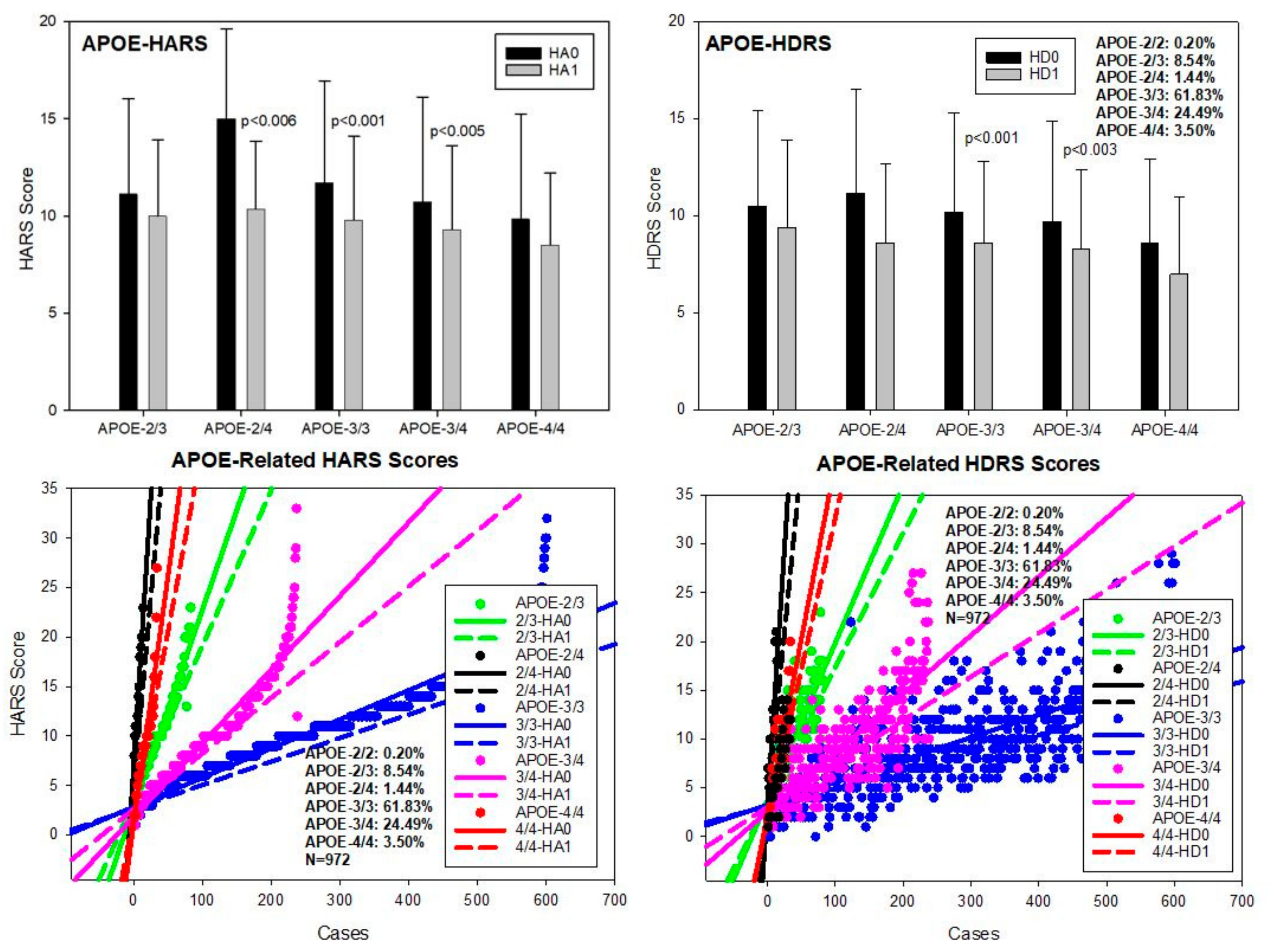
| GenoPhenotype | N | % | HARS-0 | HARS-1 | p Value |
|---|---|---|---|---|---|
| APOE-2/2 | 2 | 0.20 | 15.5 ± 10.6 | 11.50 ± 12.02 | p = 0.70 |
| APOE-2/3 | 83 | 8.54 | 11.13 ± 4.96 (1) | 10.03 ± 3.98 (7–8) | p = 0.19 |
| APOE-2/4 | 14 | 1.44 | 15.00 ± 4.64 (2–4) | 10.35 ± 3.50 | p < 0.006 |
| APOE-3/3 | 601 | 61.83 | 11.72 ± 5.27 (5–6) | 9.83 ± 4.34 | p < 0.001 |
| APOE-3/4 | 238 | 24.49 | 10.72 ± 5.41 | 9.33 ± 4.22 | p < 0.001 |
| APOE-4/4 | 34 | 3.50 | 9.85 ± 5.47 | 8.50 ± 3.77 | 0.39 |
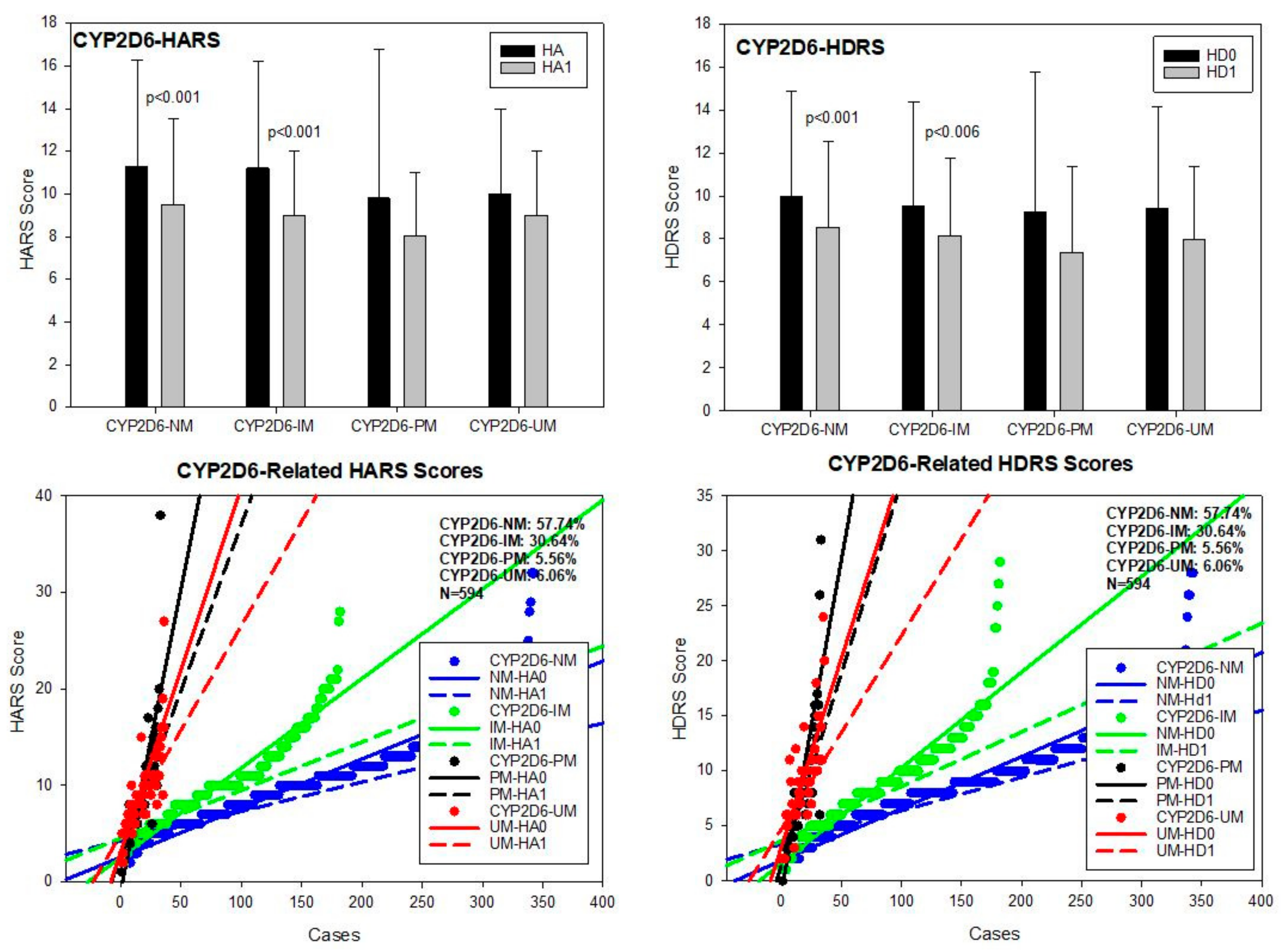
| CYP2D6-NM | 343 | 57.74 | 11.30 ± 5.31 (9) | 9.51 ± 4.07 | p < 0.001 |
| CYP2D6-IM | 182 | 30.64 | 11.02 ± 5.06 (10) | 9.07 ± 3.57 | p < 0.001 |
| CYP2D6-PM | 33 | 5.56 | 9.75 ± 7.01 | 8.48 ± 3.89 | 0.76 |
| CYP2D6-UM | 36 | 6.06 | 10.05 ± 4.52 | 8.94 ± 3.02 | 0.37 |
| CYP2C19-NM | 423 | 71.21 | 11.41 ± 5.67 | 9.42 ± 3.92 | p < 0.001 |
| CYP2C19-IM | 153 | 25.76 | 10.59 ± 5.12 | 9.03 ± 3.84 | p < 0.01 |
| CYP2C19-PM | 8 | 1.35 | 9.65 ± 4.80 | 8.00 ± 3.11 | 0.43 |
| CYP2C19-UM | 10 | 1.68 | 13.50 ± 6.06 | 11.30 ± 4.11 | 0.35 |
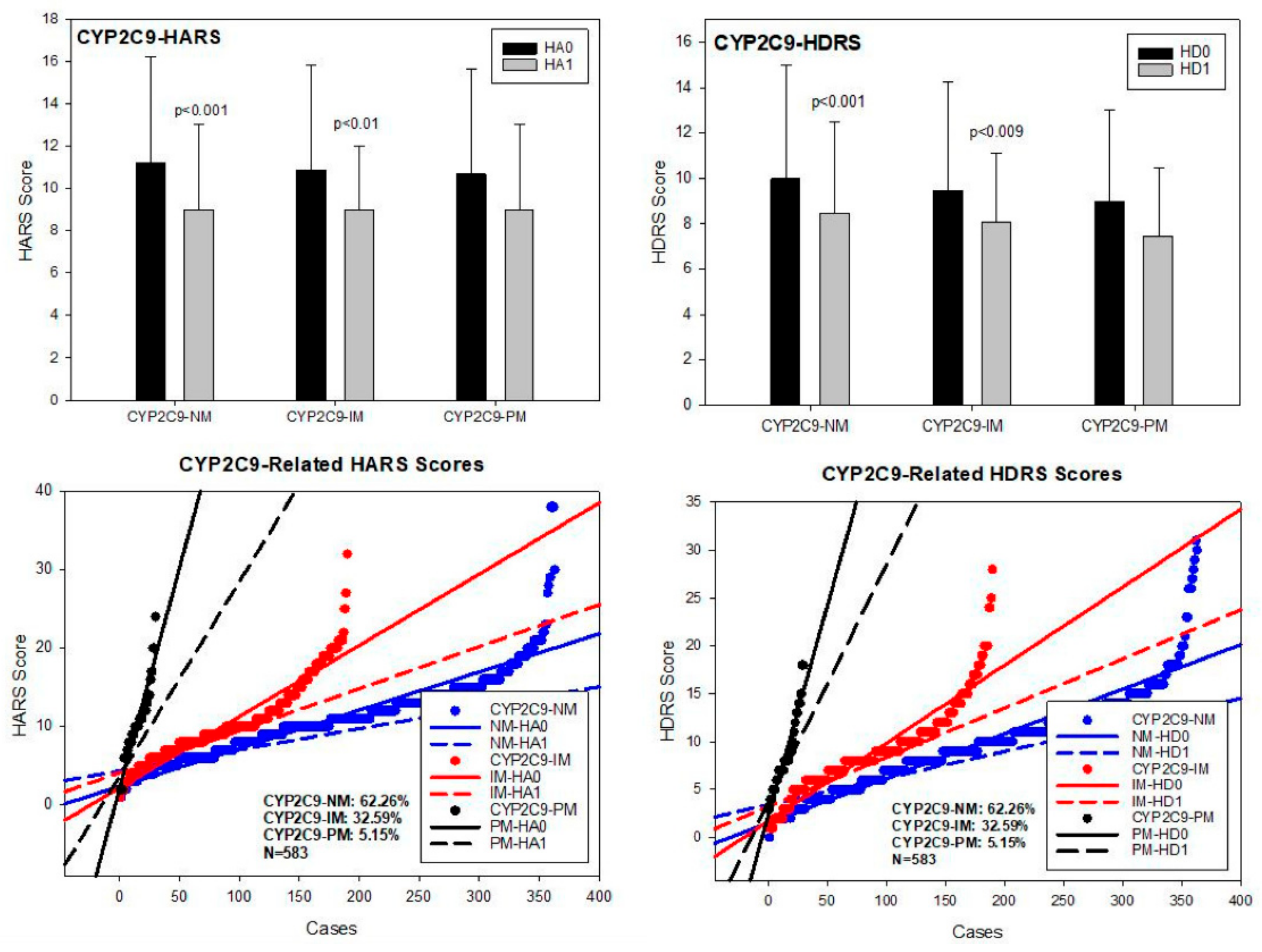
| CYP2C9-NM | 363 | 62.26 | 11.21 ± 5.35 | 9.23 ± 3.93 | p < 0.001 |
| CYP2C9-IM | 190 | 32.59 | 10.84 ± 5.26 | 9.26 ± 3.72 | p < 0.01 |
| CYP2C9-PM | 30 | 5.15 | 10.66 ± 5.20 | 9.50 ± 3.95 | 0.33 |
| GenoPhenotype | N | % | HDRS-0 | HDRS-1 | p Value |
|---|---|---|---|---|---|
| APOE-2/2 | 2 | 0.20 | 10.00 ± 5.65 | 7.50 ± 7.77 | p = 0.13 |
| APOE-2/3 | 83 | 8.54 | 10.50 ± 4.91 (1–2) | 9.39 ± 4.55 (5–6) | p = 0.13 |
| APOE-2/4 | 14 | 1.44 | 11.14 ± 4.44 (3) | 8.64 ± 4.19 | p = 0.18 |
| APOE-3/3 | 601 | 61.83 | 10.19 ± 5.17 (4) | 8.61 ± 4.21 (7) | p < 0.001 |
| APOE-3/4 | 238 | 24.49 | 9.76 ± 5.24 | 8.33 ± 4.16 | p < 0.003 |
| APOE-4/4 | 34 | 3.50 | 8.58 ± 4.34 | 7.08 ± 3.76 | 0.13 |
| CYP2D6-NM | 343 | 57.74 | 9.98 ± 4.91 (8) | 8.55 ± 4.18 | p < 0.001 |
| CYP2D6-IM | 182 | 30.64 | 9.54 ± 4.86 (9) | 8.16 ± 3.68 | p < 0.006 |
| CYP2D6-PM | 33 | 5.56 | 9.24 ± 6.55 | 7.36 ± 4.13 | 0.33 |
| CYP2D6-UM | 36 | 6.06 | 9.44 ± 4.79 | 7.97 ± 3.43 | 0.25 |
| CYP2C19-NM | 423 | 71.21 | 10.06 ± 5.12 (10–11) | 8.44 ± 4.00 | p < 0.001 |
| CYP2C19-IM | 153 | 25.76 | 9.16 ± 4.78 | 7.92 ± 4.01 | p < 0.02 |
| CYP2C19-PM | 8 | 1.35 | 8.75 ± 3.88 | 8.00 ± 2.33 | 0.64 |
| CYP2C19-UM | 10 | 1.68 | 10.80 ± 5.18 | 9.20 ± 3.12 | 0.41 |
| CYP2C9-NM | 363 | 62.26 | 9.97 ± 5.18 | 8.47 ± 4.81 | p < 0.001 |
| CYP2C9-IM | 190 | 32.59 | 9.46 ± 4.80 | 8.10 ± 3.82 | p < 0.009 |
| CYP2C9-PM | 30 | 5.15 | 9.00 ± 4.02 | 7.46 ± 3.35 | 0.14 |
| Gene Symbol | Gene Name | Locus | dbSNP | Polymorphism | Assay ID |
|---|---|---|---|---|---|
| A2M | alpha-2-macroglobulin | 12p13.31 | rs669 | c. 2998A > G, V1000I | C____517658_10 |
| ABCA7 | ATP binding cassette subfamily A member | 19p13.3 | rs3764650 | c. 1622+115T > G | C__27478162_10 |
| ACE | angiotensin I converting enzyme | 17q23.3 | rs4332 | c. 496-66T > C | C__11942538_20 |
| APOE | apolipoprotein E | 19q13.32 | rs429358 | c. 3932T > C, Cys112Arg | C___3084793_20 |
| rs7412 | c. 4070C > T, Cys158Arg | C____904973_10 | |||
| BIN1 | bridging integrator 1 | 2q14.3 | rs744373 | g. 127137039A > G | C___1042213_10 |
| C9ORF72 | chromosome 9 open reading frame 72 | 9p21.2 | rs3849942 | g. 27543283T > C | C__27515934_20 |
| CLU | clusterin | 8p21.1 | rs11136000 | c. 247-478A > G | C__11227737_10 |
| CPZ | carboxypeptidase Z | 4p16.1 | rs7436874 | g. 8649098C > T | C____506568_20 |
| CR1 | complement C3b/C4b receptor 1 | 1q32.2 | rs3818361 | c. 4946-54A > G | C__25598588_10 |
| DISC1 LHFPL6 MS4A4E | disrupted in schizophrenia 1 LHFPL tetraspan subfamily member 6 membrane spanning 4-domains A4E | 1q42.2 13q13.3-q14.11 11q12.2 | rs16856202 | c. 2242-7030T > G | C__33950435_10 |
| rs7995844 | g. 39298100G > A | C__29428261_10 | |||
| rs670139 | c. 279-2443C > A | C___7512835_20 | |||
| MS4A6A | membrane spanning 4-domains A6A | 11q12.2 | rs610932 | c. *149 + 175A > C | C__27161626_10 |
| NOS3 | nitric oxyde synthse 3 | 7q36.1 | rs1799983 | c. 894G > T, E298D | C___3219460_20 |
| PICALM | phosphatidylinositol binding clathrin assembly protein | 11q14.2 | rs3851179 | g. 85868640T > C | C___8748810_10 |
| PRNP | prion protein | 20p13 | rs1799990 | c. 385A > G, M129V | C___2969398_10 |
| PSEN1 | presenilin 1 | 14q24.2 | rs165932 | c. 856+16G > T | C____579315_20 |
| TNF | tumor necrosis factor | 6p21.33 | rs1800629 | c. -308G > A | C___7514879_10 |
| Gene Symbol | Gene Name | Locus | dbSNP | Polymorphism | Assay ID |
|---|---|---|---|---|---|
| CYP1A1 | cytochrome P450 family 1 subfamily A member 1 | 15q24.1 | rs1378942 | c. −66 + 2306C > A | C___1642446_10 |
| CYP1A2 | cytochrome P450 family 1 subfamily A member 2 | 15q24.1 | rs2069514 | g. −3860G > A | C__15859191_30 |
| rs35694136 | g. −2467delT | C__60142977_10 | |||
| rs762551 | g. −163C > A | C___8881221_40 | |||
| CYP1B1 | cytochrome P450 family 1 subfamily B member 1 | 2p22.2 | rs1056836 | c. 1294C > G; p. Leu432Val | C___3099976_30 |
| CYP2A6 | cytochrome P450 family 2 subfamily A member 6 | 19q13.2 | rs28399433 | g.−48T > G | C__30634332_10 |
| CYP2B6 | cytochrome P450 family 2 subfamily B member 6 | 19q13.2 | rs3745274 | c.516G > T; p.Gln172His | C___7817765_60 |
| CYP2C19 | cytochrome P450 family 2 subfamily C member 19 | 10q23.33 | rs12248560 | g. −806C > T | C____469857_10 |
| rs4244285 | c.681G > A | C__25986767_70 | |||
| CYP2C9 | cytochrome P450 family 2 subfamily C member 9 | 10q23.33 | rs1057910 | c. 1075A > C | C__27104892_10 |
| rs1799853 | c. 430C > T | C__25625805_10 | |||
| rs28371685 | c. 1003C > T | C__30634132_70 | |||
| rs28371686 | c. 1080C > A | C__27859817_40 | |||
| rs7900194 | c. 449G > T | C__25625804_10 | |||
| rs9332131 | c. 817delA | C__32287221_20 | |||
| CYP2D6 | cytochrome P450 family 2 subfamily D member 6 | 22q13.2 | indel | Gene duplication/deletion | Hs00010001_cn |
| rs28371725 | g. 2988G > A | C__34816116_20 | |||
| rs35742686 | g. 2549delA | C__32407232_50 | |||
| rs3892097 | g. 1846G > A | C__27102431_D0 | |||
| rs5030655 | g. 1707T > del | C__32407243_20 | |||
| CYP2E1 | cytochrome P450 family 2 subfamily E member 1 | 10q26.3 | rs3813867 | g. −1293G > C | C___2431875_10 |
| rs6413420 | g. −71G > T | C__25594209_10 | |||
| CYP3A4 | cytochrome P450 family 3 subfamily A member 4 | 7q22.1 | rs2242480 | g. 20230G > A | C__26201900_30 |
| rs35599367 | g. 20493C > T | C__59013445_10 | |||
| CYP3A5 | cytochrome P450 family 3 subfamily A member 5 | 7q22.1 | rs776746 | g. 6986A > G | C__26201809_30 |
| CYP4F2 | cytochrome P450 family 4 subfamily F member 2 | 19p13.12 | rs2108622 | c. 1297G > A | C__16179493_40 |
| DPYD | dihydropyrimidine dehydrogenase | 1p21.3 | rs3918290 | c. 1905+1G > A/C | C__30633851_20 |
| rs55886062 | c. 1679T > G; p.Ile560Ser | C__11985548_10 | |||
| rs67376798 | c. 2846A > T; p. Asp949Val | C__27530948_10 | |||
| G6PD | glucose-6-phosphate dehydrogenase | Xq28 | rs1050828 | c. 202G > A; p.Val68Met | C___2228686_20 |
| rs5030868 | c. 563C > T; Ser188Phe | C___2228708_20 | |||
| MAOB | monoamine oxidase B | Xp11.3 | rs1799836 | c. 1300−36A > G | C___8878790_10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacabelos, R.; Carril, J.C.; Corzo, L.; Fernández-Novoa, L.; Pego, R.; Cacabelos, N.; Cacabelos, P.; Alcaraz, M.; Tellado, I.; Naidoo, V. Influence of Pathogenic and Metabolic Genes on the Pharmacogenetics of Mood Disorders in Alzheimer’s Disease. Pharmaceuticals 2021, 14, 366. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040366
Cacabelos R, Carril JC, Corzo L, Fernández-Novoa L, Pego R, Cacabelos N, Cacabelos P, Alcaraz M, Tellado I, Naidoo V. Influence of Pathogenic and Metabolic Genes on the Pharmacogenetics of Mood Disorders in Alzheimer’s Disease. Pharmaceuticals. 2021; 14(4):366. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040366
Chicago/Turabian StyleCacabelos, Ramón, Juan C. Carril, Lola Corzo, Lucía Fernández-Novoa, Rocío Pego, Natalia Cacabelos, Pablo Cacabelos, Margarita Alcaraz, Iván Tellado, and Vinogran Naidoo. 2021. "Influence of Pathogenic and Metabolic Genes on the Pharmacogenetics of Mood Disorders in Alzheimer’s Disease" Pharmaceuticals 14, no. 4: 366. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040366