
Limitations and Challenges in the Stability of Cysteamine Eye Drop Compounded Formulations

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation of Cysteamine Hydrochloride Sterile Aqueous Solutions
2.3. Long-Term Stability Study
2.4. In-Use Stability Study
2.5. Physical Stability
2.5.1. Appearance, Color and Odor
2.5.2. pH and Viscosity
2.6. Chemical Stability
2.7. Microbiological Stability
3. Results
3.1. Preparation and Characterization of Cysteamine Hydrochloride Sterile Aqueous Solutions
3.2. Long-Term Stability Study
3.2.1. Appearance, Color and Odor
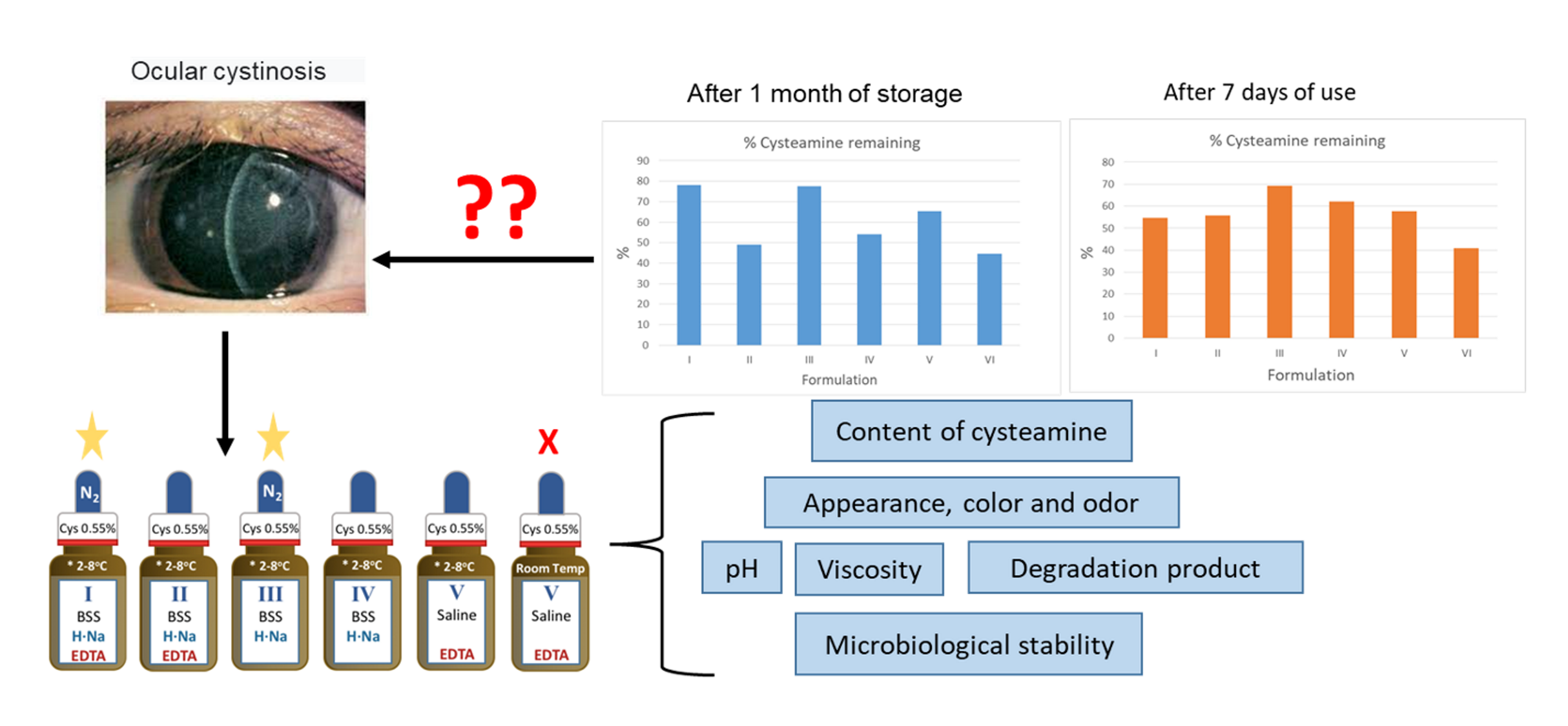
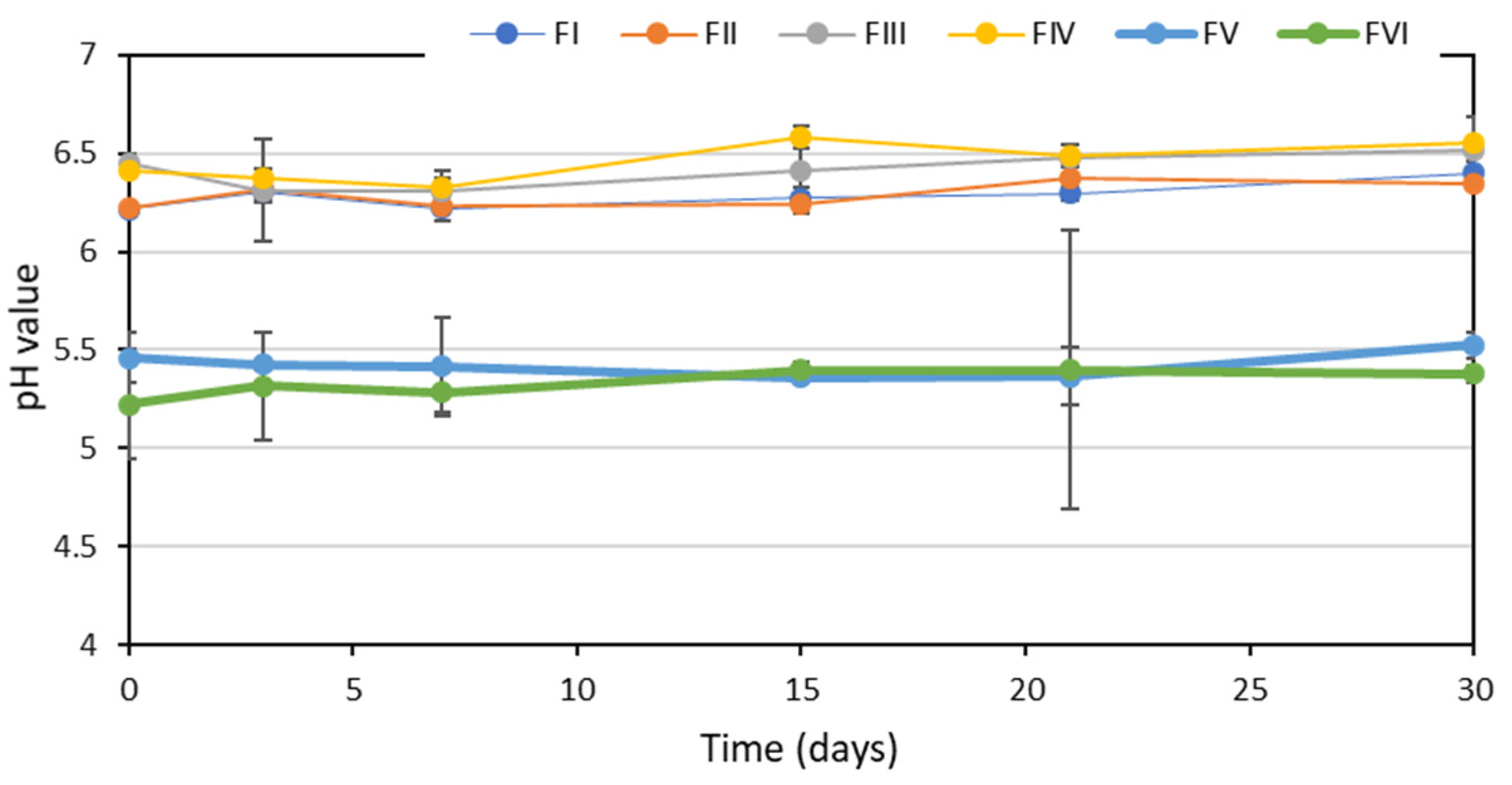
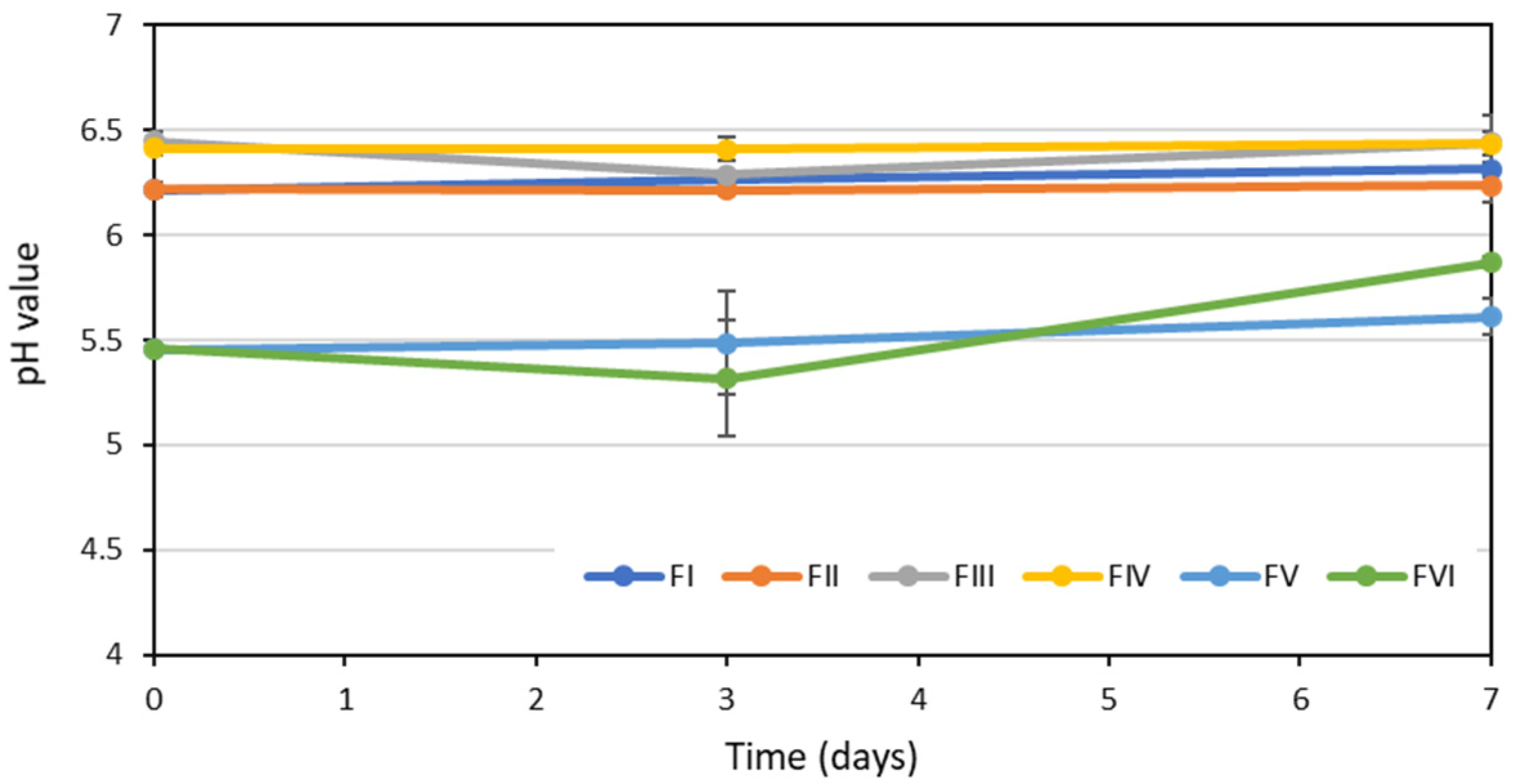
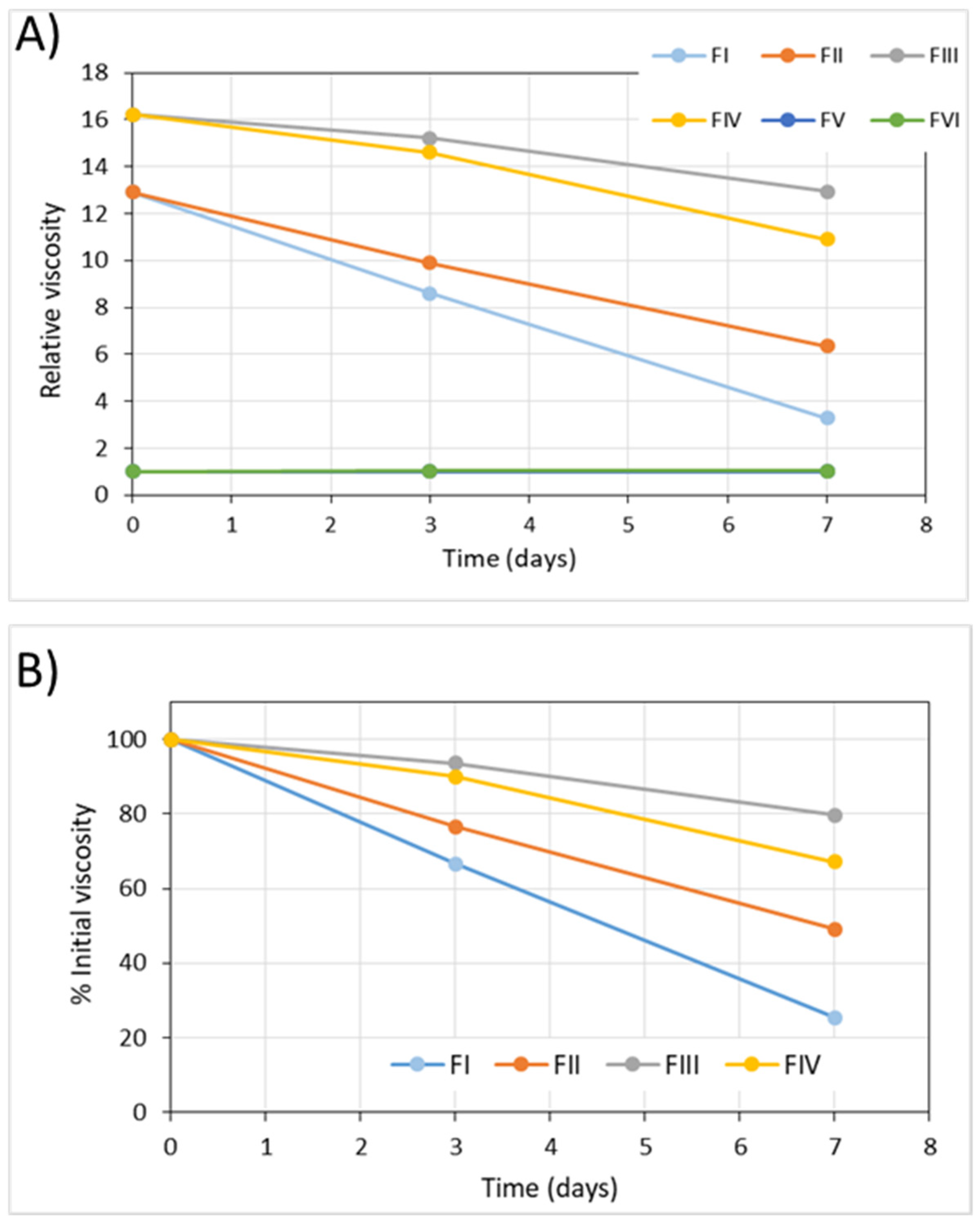
3.2.2. pH and Viscosity
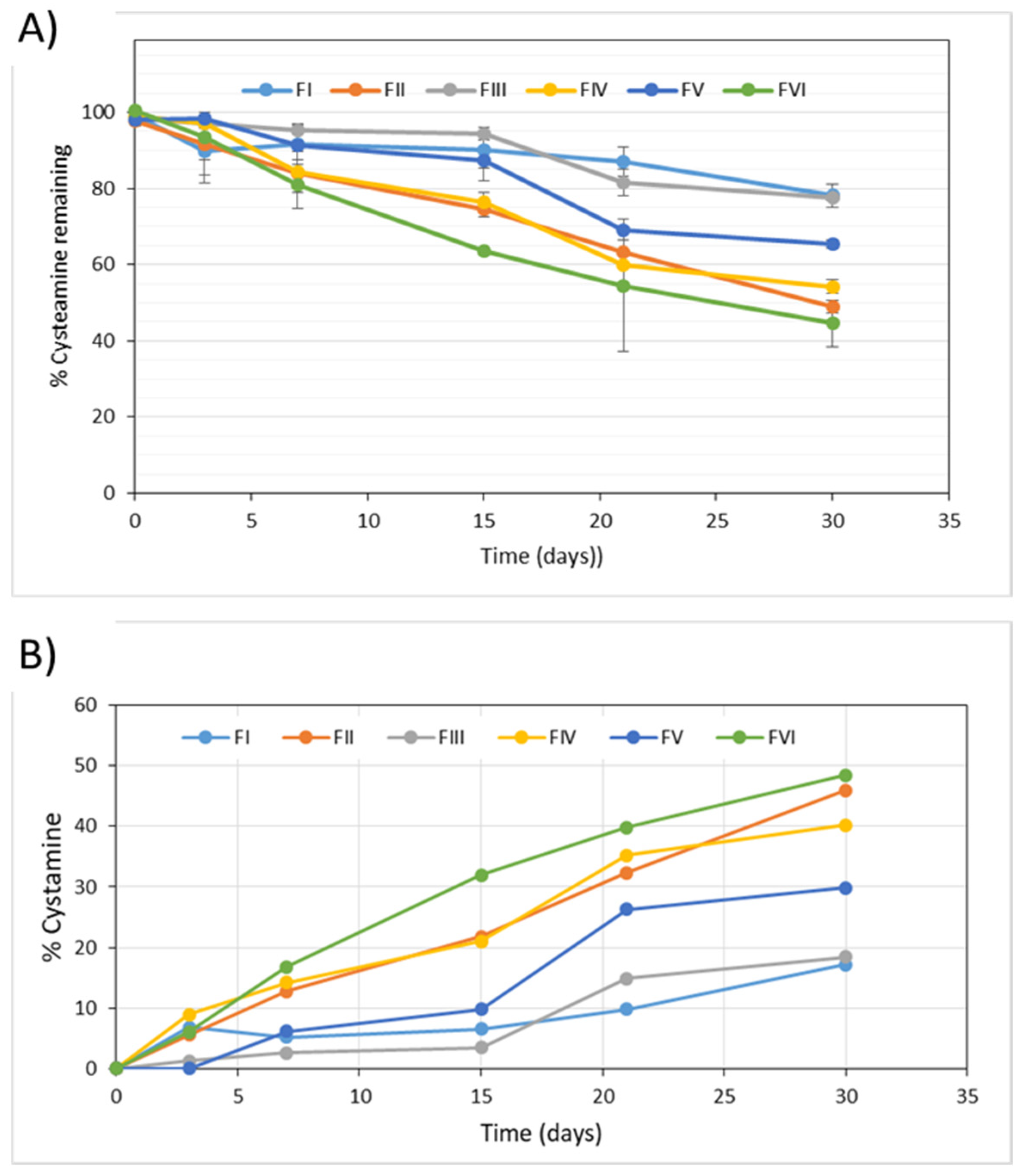
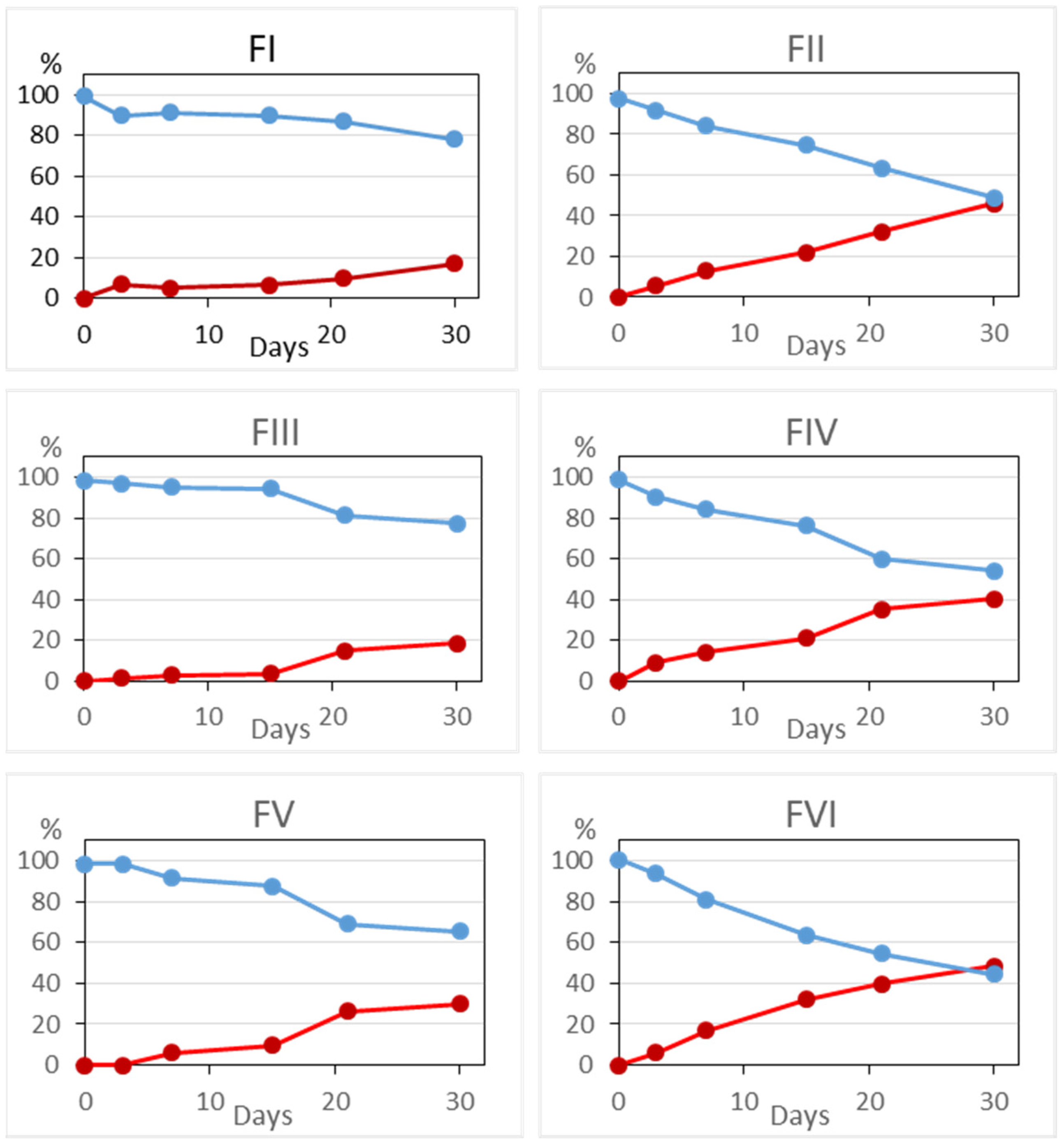
3.2.3. Chemical Stability
3.2.4. Microbiological Stability
3.3. In-Use Stability Study
3.3.1. Appearance, Color and Odor
3.3.2. pH and Viscosity
3.3.3. Chemical Stability
3.3.4. Microbiological Stability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Town, M.M.; Jean, G.; Cherqui, S.; Attard, M.; Forestier, L.; Whitmore, S.A.; Callen, D.F.; Gribouval, O.; Broyer, M.; Bates, G.; et al. A novel gene encoding an integral membrane protein is mutated in nephropathic cystinosis. Nat. Genet. 1998, 18, 319–324. [Google Scholar] [CrossRef]
- Brodin-Sartorius, A.; Tête, M.-J.; Niaudet, P.; Antignac, C.; Guest, G.; Ottolenghi, C.; Charbit, M.; Moyse, D.; Legendre, C.; Lesavre, P.; et al. Cysteamine therapy delays the progression of nephropathic cystinosis in late adolescents and adults. Kidney Int. 2012, 81, 179–189. [Google Scholar] [CrossRef] [Green Version]
- Langman, C.B.; Barshop, B.A.; Deschenes, G.; Emma, F.; Goodyer, P.; Lipkin, G.; Midgley, J.P.; Ottolenghi, C.; Servais, A.; Soliman, N.A.; et al. Controversies and research agenda in nephropathic cystinosis: Conclusions from a “Kidney Disease: Improving Global Outcomes” (KDIGO) Controversies Conference. Kidney Int. 2016, 89, 1192–1203. [Google Scholar] [CrossRef]
- Nesterova, G.; Gahl, W. Nephropathic cystinosis: Late complications of a multisystemic disease. Pediatr. Nephrol. 2007, 23, 863–878. [Google Scholar] [CrossRef] [PubMed]
- Hathout, R.; Omran, M.K. Gelatin-based particulate systems in ocular drug delivery. Pharm. Dev. Technol. 2015, 21, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Gahl, W.A.; Thoene, J.G.; Schneider, J.A. Cystinosis. N. Engl. J. Med. 2002, 347, 111–121. [Google Scholar] [CrossRef]
- Bäumner, S.; Weber, L.T. Nephropathic Cystinosis: Symptoms, Treatment, and Perspectives of a Systemic Disease. Front. Pediatr. 2018, 6, 58. [Google Scholar] [CrossRef] [Green Version]
- Pinxten, A.-M.; Hua, M.-T.; Simpson, J.; Hohenfellner, K.; Levtchenko, E.; Casteels, I. Clinical Practice: A Proposed Standardized Ophthalmological Assessment for Patients with Cystinosis. Ophthalmol. Ther. 2017, 6, 93–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsilou, E.T.; Rubin, B.I.; Reed, G.F.; Iwata, F.; Gahl, W.; Kaiser-Kupfer, M.I. Age-Related Prevalence of Anterior Segment Complications in Patients with Infantile Nephropathic Cystinosis. Cornea 2002, 21, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Gahl, W.A.; Kuehl, E.M.; Iwata, F.; Lindblad, A.; Kaiser-Kupfer, M.I. Corneal Crystals in Nephropathic Cystinosis: Natural History and Treatment with Cysteamine Eyedrops. Mol. Genet. Metab. 2000, 71, 100–120. [Google Scholar] [CrossRef] [Green Version]
- Shams, F.; Oladiwura, D.; Ramaesh, K.; Livingstone, I. Treatment of corneal cystine crystal accumulation in patients with cystinosis. Clin. Ophthalmol. 2014, 8, 2077–2084. [Google Scholar] [CrossRef] [Green Version]
- Marcano, D.C.; Shin, C.S.; Lee, B.; Isenhart, L.C.; Liu, X.; Li, F.; Jester, J.V.; Pflugfelder, S.C.; Simpson, J.; Acharya, G. Synergistic Cysteamine Delivery Nanowafer as an Efficacious Treatment Modality for Corneal Cystinosis. Mol. Pharm. 2016, 13, 3468–3477. [Google Scholar] [CrossRef]
- Atallah, C.; Charcosset, C.; Greige-Gerges, H. Challenges for cysteamine stabilization, quantification, and biological effects improvement. J. Pharm. Anal. 2020, 10, 499–516. [Google Scholar] [CrossRef]
- Iwata, F.; Kuehl, E.M.; Reed, G.F.; McCain, L.M.; Gahl, W.A.; Kaiser-Kupfer, M.I. A Randomized Clinical Trial of Topical Cysteamine Disulfide (Cystamine) versus Free Thiol (Cysteamine) in the Treatment of Corneal Cystine Crystals in Cystinosis. Mol. Genet. Metab. 1998, 64, 237–242. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency. Cystadrops. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/cystadrops#authorisation-details-section (accessed on 29 October 2021).
- US Food and Drug Administration. CystaranTM (Cysteamine Ophthalmic Solution) Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/200740s000lbl.pdf (accessed on 29 October 2021).
- US Food and Drug Administration. Cystadrops (Cysteamine Ophthalmic Solution) Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/211302s000lbl.pdf (accessed on 29 October 2021).
- Labbé, A.; Baudouin, C.; Deschênes, G.; Loirat, C.; Charbit, M.; Guest, G.; Niaudet, P. A new gel formulation of topical cysteamine for the treatment of corneal cystine crystals in cystinosis: The Cystadrops OCT-1 study. Mol. Genet. Metab. 2014, 111, 314–320. [Google Scholar] [CrossRef]
- Liang, H.; Labbé, A.; Le Mouhaër, J.; Plisson, C.; Baudouin, C. A New Viscous Cysteamine Eye Drops Treatment for Ophthalmic Cystinosis: An Open-Label Randomized Comparative Phase III Pivotal Study. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2275–2283. [Google Scholar] [CrossRef]
- Liang, H.; Labbé, A.; Baudouin, C.; Plisson, C.; Giordano, V. Long-term follow-up of cystinosis patients treated with 0.55% cysteamine hydrochloride. Br. J. Ophthalmol. 2020, 105, 608–613. [Google Scholar] [CrossRef]
- Reda, A.; Van Schepdael, A.; Adams, E.; Paul, P.; Devolder, D.; Elmonem, M.A.; Veys, K.; Casteels, I.; Heuvel, L.V.D.; Levtchenko, E. Effect of Storage Conditions on Stability of Ophthalmological Compounded Cysteamine Eye Drops. JIMD Rep. 2017, 42, 47–51. [Google Scholar] [CrossRef]
- Peeters, F.; Cassiman, C.; Van Keer, K.; Levtchenko, E.; Veys, K.; Casteels, I. Ophthalmic Outcome in a Belgian Cohort of Cystinosis Patients Treated with a Compounded Preparation of Cysteamine Eye Drops: Retrospective Analysis. Ophthalmol. Ther. 2019, 8, 623–633. [Google Scholar] [CrossRef] [Green Version]
- Biswas, S.; Sornalingam, K. The Ocular Status of Cystinosis Patients Receiving a Hospital Pharmacy-Made Preparation of Cysteamine Eye Drops: A Case Series. Ophthalmol. Ther. 2018, 8, 125–136. [Google Scholar] [CrossRef] [Green Version]
- Al-Hemidan, A.; Shoughy, S.S.; Kozak, I.; Tabbara, K.F. Efficacy of topical cysteamine in nephropathic cystinosis. Br. J. Ophthalmol. 2017, 101, 1234–1237. [Google Scholar] [CrossRef] [PubMed]
- Helmi, H.A.; El Mansoury, J.; Al Hazzaa, S.; Al Zoba, A.; Dirar, Q.S. Asymmetrical Ocular Manifestations of Nephropathic Cystinosis; A Case Report. Am. J. Case Rep. 2019, 20, 1308–1313. [Google Scholar] [CrossRef]
- Fernández-Ferreiro, A.; Luaces-Rodríguez, A.; Díaz-Tomé, V.; Gil-Martínez, M.; Rodríguez Ares, M.T.; Touriño Peralba, R.; Blanco-Méndez, J.; González-Barcia, M.; Otero-Espinar, F.J.; Lamas, M.J. Cysteamine ophthalmic hydrogel for the treatment of ocular cystinosis. Farm. Hosp. 2017, 41, 678–687. [Google Scholar] [PubMed]
- Molina-Molero, J.M. Colirio de Cisteamina 5.5 mg/mL (0,55%) CSP 10 mL. Asociación de Formulistas de Andalucía. Available online: http://www.formulistasdeandalucia.es/noticia.php?id=264 (accessed on 20 October 2021).
- European Medicines Agency. ICH Q1A(R2): Stability Testing of New Drug Substances and Products. 2003. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-q-1-r2-stability-testing-new-drug-substances-products-step-5_en.pdf (accessed on 22 October 2021).
- European Medicines Agency. ICH Q3A(R2): Impurities in New Drug Substances. 2006. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-q-3-r2-impurities-new-drug-substances-step-5_en.pdf (accessed on 22 October 2021).
- Real Farmacopea Española, 3rd ed.; Agencia Española del Medicamento, Ministerio de Sanidad y Consumo: Madrid, Spain, 2005; pp. 153–157.
- Makuloluwa, A.K.; Shams, F. Cysteamine hydrochloride eye drop solution for the treatment of corneal cystine crystal deposits in patients with cystinosis: An evidence-based review. Clin. Ophthalmol. 2018, 12, 227–236. [Google Scholar] [CrossRef] [Green Version]
- Ozdemir, H.B.; Özmen, M.C.; Aktas, Z.; Hasanreisoglu, M. In vivo confocal microscopy and anterior segment optical coherence tomography follow-up of cysteamine treatment in corneal cystinosis. Indian J. Ophthalmol. 2019, 67, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Gaviria, M.; Malheiro, L.; Marques, J.P.; Giordano, V.; Liang, H. Latest Clinical Approaches in the Ocular Management of Cystinosis: A Review of Current Practice and Opinion from the Ophthalmology Cystinosis Forum. Ophthalmol. Ther. 2018, 7, 307–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dixon, P.; Powell, K.; Chauhan, A. Novel approaches for improving stability of cysteamine formulations. Int. J. Pharm. 2018, 549, 466–475. [Google Scholar] [CrossRef]
- Bagiyan, G.A.; Koroleva, I.K.; Soroka, N.V. Oxidation of thiol compounds by molecular oxygen in aqueous solutions. Russ. Chem. Bull. 2003, 52, 1135–1141. [Google Scholar] [CrossRef]
- Pescina, S.; Carra, F.; Padula, C.; Santi, P.; Nicoli, S. Effect of pH and penetration enhancers on cysteamine stability and trans-corneal transport. Eur. J. Pharm. Biopharm. 2016, 107, 171–179. [Google Scholar] [CrossRef]
- Castro-Balado, A.; Mondelo-García, C.; Varela-Rey, I.; Moreda-Vizcaíno, B.; Sierra-Sánchez, J.F.; Rodríguez-Ares, M.T.; Hermelo-Vidal, G.; Zarra-Ferro, I.; González-Barcia, M.; Yebra-Pimentel, E.; et al. Recent Research in Ocular Cystinosis: Drug Delivery Systems, Cysteamine Detection Methods and Future Perspectives. Pharmaceutics 2020, 12, 1177. [Google Scholar] [CrossRef]
- Bozdag, S.; Gumus, K.; Gumus, O.; Unlu, N. Formulation and in vitro evaluation of cysteamine hydrochloride viscous solutions for the treatment of corneal cystinosis. Eur. J. Pharm. Biopharm. 2008, 70, 260–269. [Google Scholar] [CrossRef] [PubMed]
- MacFaul, P.A.; Ruston, L.; Wood, J.M. Activation energies for the decomposition of pharmaceuticals and their application to predicting hydrolytic stability in drug discovery†. Med. Chem. Commun. 2011, 2, 140–142. [Google Scholar] [CrossRef]
- Carstensen, J.T. Solution Kinetics. In Drug Stability. Principles and Practices, 3rd ed.; Carstensen, J.T., Rhodes, C., Eds.; Marcel Dekker, Inc.: New York, NY, USA, 2000; pp. 19–56. [Google Scholar]
- McKenzie, B.; Kay, G.; Matthews, K.; Knott, R.; Cairns, D. Preformulation of cysteamine gels for treatment of the ophthalmic complications in cystinosis. Int. J. Pharm. 2016, 515, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Ariceta, G.; Giordano, V.; Santos, F. Effects of long-term cysteamine treatment in patients with cystinosis. Pediatr. Nephrol. 2019, 34, 571–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higuchi, T. Mechanism of sustained-action medication. Theoretical analysis of rate of release of solid drugs dispersed in solid matrices. J. Pharm. Sci. 1963, 52, 1145–1149. [Google Scholar] [CrossRef] [PubMed]



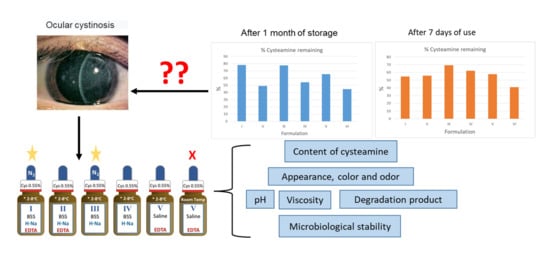
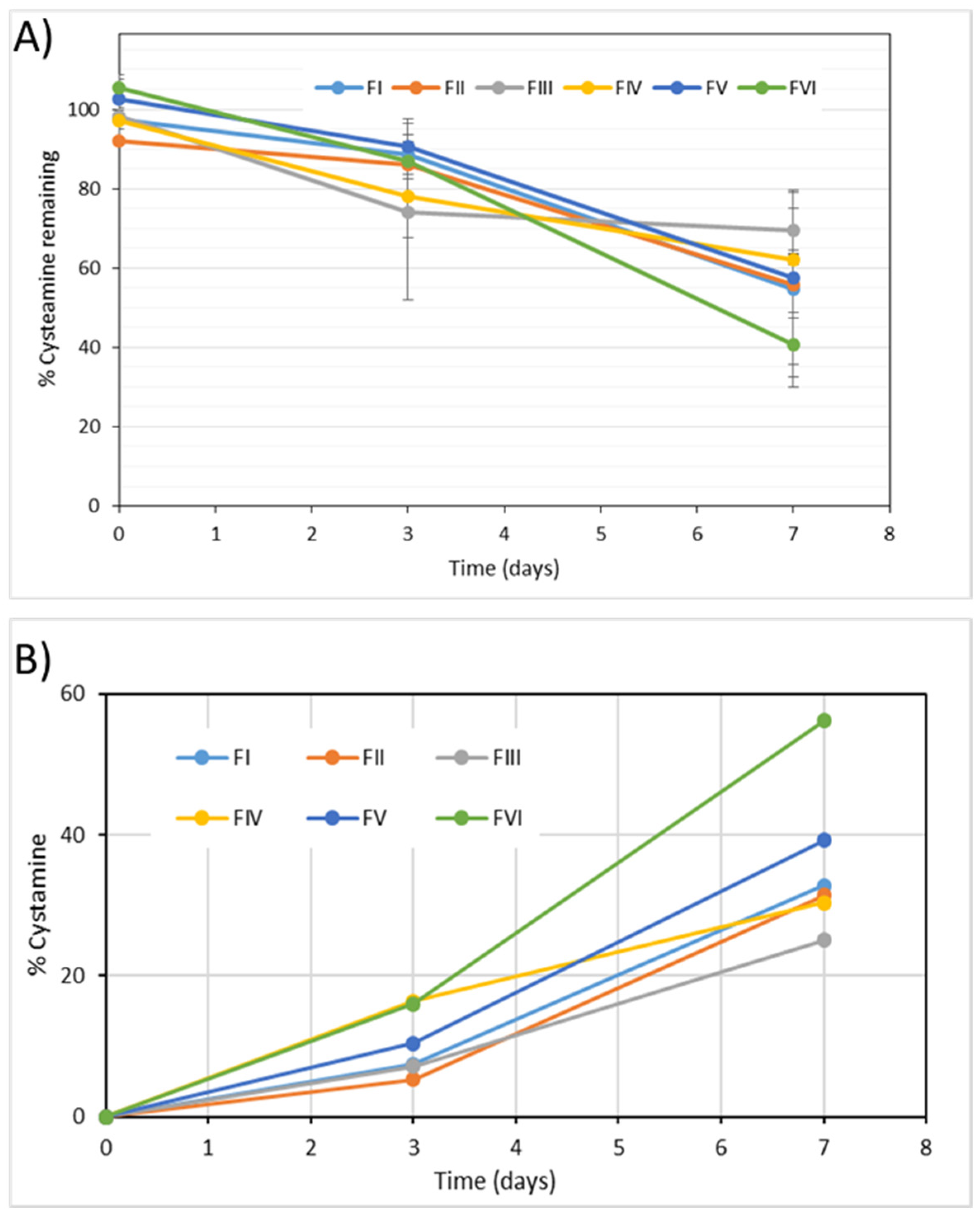
 and cystamine
and cystamine  levels in the six formulae studied.
levels in the six formulae studied.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Composition Per Vial | ||||||
|---|---|---|---|---|---|---|
| F I | F II | F III | F IV | F V | F VI | |
| Cysteamine (%) | 0.55 | 0.55 | 0.55 | 0.55 | 0.55 | 0.55 |
| Hyaluronic Acid (%) | 0.4 | 0.4 | 0.4 | 0.4 | --- | --- |
| EDTA (%) | 0.01 | 0.01 | --- | --- | 0.01 | 0.01 |
| BSS (mL) q.s. | 10 | 10 | 10 | 10 | ||
| Physiological saline solution (mL) q.s. | --- | --- | --- | --- | 10 | 10 |
| Vial | Sterile class I 15 mL amber glass dropper bottle | |||||
| Saturation with N2 | Yes | --- | Yes | --- | --- | --- |
| Storage conditions | Refrigerator (2–8 °C) | Room temperature (25 °C) | ||||
| Time (min) | Mobile Phase A (%) | Mobile Phase B (%) |
|---|---|---|
| 0 | 80 | 20 |
| 1.0 | 80 | 20 |
| 16.0 | 35 | 65 |
| 16.1 | 10 | 90 |
| 19.0 | 10 | 90 |
| 19.5 | 80 | 20 |
| 24.0 | 80 | 20 |
| K (%/day) | Sk (%/day) | r | |
|---|---|---|---|
| FI | 0.5343 | 0.1329 | −0.7859 |
| FII | 1.5866 | 0.0811 | −0.9872 |
| FIII | 0.7328 | 0.0985 | −0.9274 |
| FIV | 1.493 | 0.1191 | −0.9696 |
| FV | 1.2095 | 0.1132 | −0.9589 |
| FVI | 1.906 | 0.2069 | −0.9458 |
| K (%/day) | Sk (%/day) | r | |
|---|---|---|---|
| FI | 5.2301 | 0.9119 | −0.9573 |
| FII | 5.3082 | 1.1188 | −0.9215 |
| FIII | 4.1976 | 1.6782 | −0.781 |
| FIV | 4.9523 | 0.899 | −0.94 |
| FV | 6.5433 | 1.7833 | −0.878 |
| FVI | 9.3489 | 1.0367 | −0.9763 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Sabroso, C.; Alonso-González, M.; Fernández-Carballido, A.; Aparicio-Blanco, J.; Córdoba-Díaz, D.; Navarro-García, F.; Córdoba-Díaz, M.; Torres-Suárez, A.I. Limitations and Challenges in the Stability of Cysteamine Eye Drop Compounded Formulations. Pharmaceuticals 2022, 15, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15010002
Martín-Sabroso C, Alonso-González M, Fernández-Carballido A, Aparicio-Blanco J, Córdoba-Díaz D, Navarro-García F, Córdoba-Díaz M, Torres-Suárez AI. Limitations and Challenges in the Stability of Cysteamine Eye Drop Compounded Formulations. Pharmaceuticals. 2022; 15(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15010002
Chicago/Turabian StyleMartín-Sabroso, Cristina, Mario Alonso-González, Ana Fernández-Carballido, Juan Aparicio-Blanco, Damián Córdoba-Díaz, Federico Navarro-García, Manuel Córdoba-Díaz, and Ana I. Torres-Suárez. 2022. "Limitations and Challenges in the Stability of Cysteamine Eye Drop Compounded Formulations" Pharmaceuticals 15, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15010002