
A Robust and Fast/Multiplex Pharmacogenetics Assay to Simultaneously Analyze 17 Clinically Relevant Genetic Polymorphisms in CYP3A4, CYP3A5, CYP1A2, CYP2C9, CYP2C19, CYP2D6, ABCB1, and VKORC1 Genes

 ,
,
Abstract
:1. Introduction
2. Results
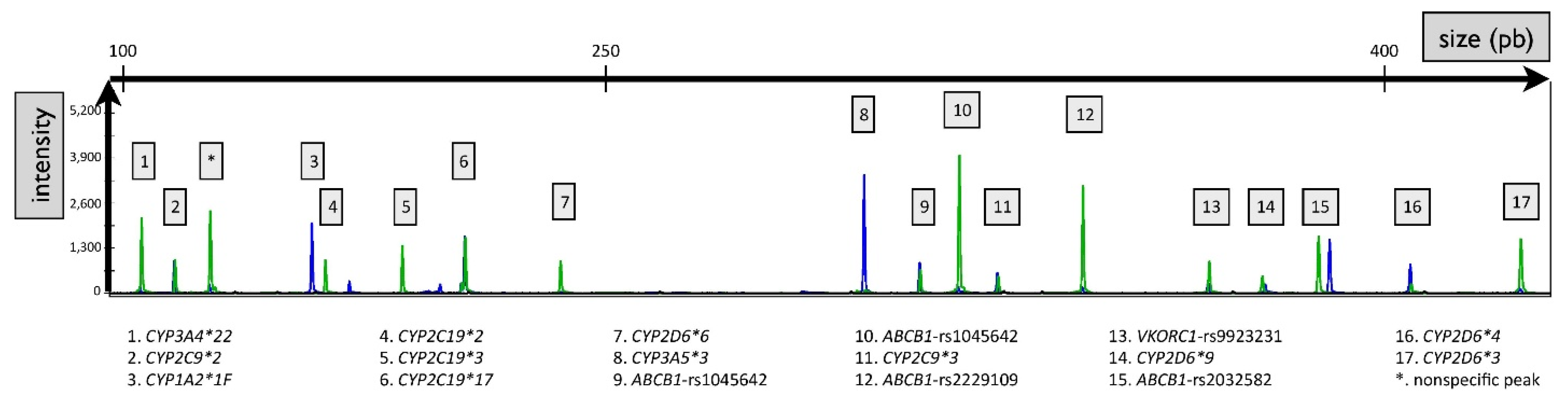
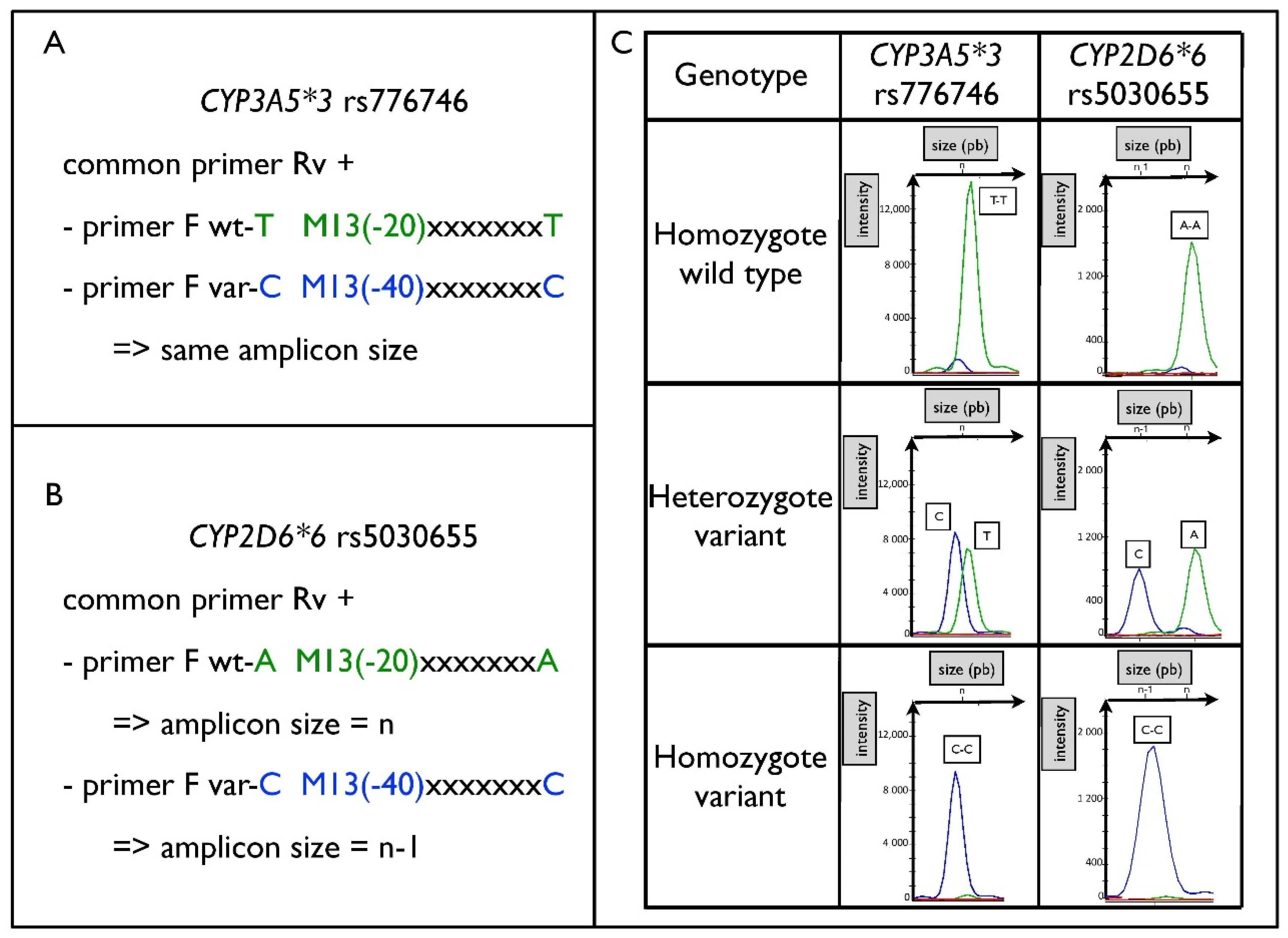
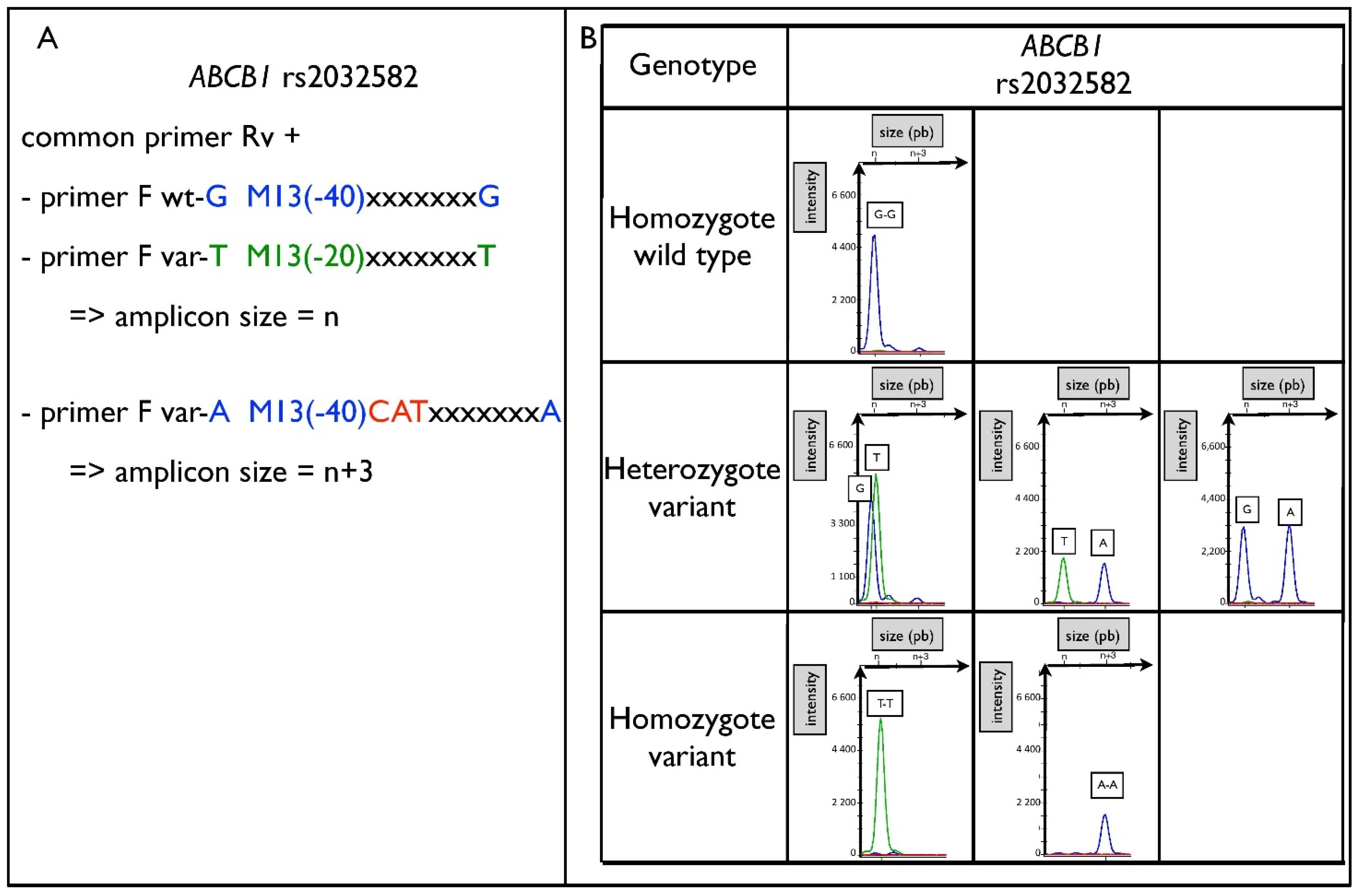
2.1. Optimization of the Assay
2.2. Validation of the Assay
2.3. Genotyping Method Comparison
2.3.1. Evaluation of the Accuracy of the Assay Compared to Reference Methods
2.3.2. Comparison of Cost and Analytical Workflow with Reference Methods
2.4. Clinical Cases
3. Discussion
4. Materials and Methods
4.1. Material and Reagent
4.2. Principle of the Assay and Optimization
4.3. Validation of the Assay
4.4. Genotyping Methods Comparisons
4.4.1. Evaluation of the Accuracy of the Assay Compared to Reference Methods
4.4.2. Comparison with Reference Methods Regarding Cost and Analytical Workflow
4.5. Clinical Cases
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scott, S.A. Personalizing Medicine with Clinical Pharmacogenetics. Genet. Med. 2011, 13, 987–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woillard, J.-B.; Chouchana, L.; Picard, N.; Loriot, M.-A. French Network of Pharmacogenetics (RNPGX) Pharmacogenetics of Immunosuppressants: State of the Art and Clinical Implementation-Recommendations from the French National Network of Pharmacogenetics (RNPGx). Therapies 2017, 72, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, S.; Dupouey, J.; Colle, R.; Verstuyft, C. Pharmacogenetics of Antidepressant Drugs: State of the Art and Clinical Implementation-Recommendations from the French National Network of Pharmacogenetics. Therapies 2017, 72, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Picard, N.; Boyer, J.-C.; Etienne-Grimaldi, M.-C.; Barin-Le Guellec, C.; Thomas, F.; Loriot, M.-A. French National Network of Pharmacogenetics (RNPGx) Pharmacogenetics-Based Personalized Therapy: Levels of Evidence and Recommendations from the French Network of Pharmacogenetics (RNPGx). Therapies 2017, 72, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Lamoureux, F.; Duflot, T. French Network of Pharmacogenetics (RNPGX) Pharmacogenetics in Cardiovascular Diseases: State of the Art and Implementation-Recommendations of the French National Network of Pharmacogenetics (RNPGx). Therapies 2017, 72, 257–267. [Google Scholar] [CrossRef]
- Abdullah-Koolmees, H.; van Keulen, A.M.; Nijenhuis, M.; Deneer, V.H.M. Pharmacogenetics Guidelines: Overview and Comparison of the DPWG, CPIC, CPNDS, and RNPGx Guidelines. Front. Pharmacol. 2020, 11, 595219. [Google Scholar] [CrossRef]
- Di Nunno, N.; Esposito, M.; Argo, A.; Salerno, M.; Sessa, F. Pharmacogenetics and Forensic Toxicology: A New Step towards a Multidisciplinary Approach. Toxics 2021, 9, 292. [Google Scholar] [CrossRef]
- Esposito, M.; Cocimano, G.; Ministrieri, F.; Rosi, G.L.; Nunno, N.D.; Messina, G.; Sessa, F.; Salerno, M. Smart Drugs and Neuroenhancement: What Do We Know? Front. Biosci.-Landmark 2021, 26, 347–359. [Google Scholar] [CrossRef]
- Fujikura, K.; Ingelman-Sundberg, M.; Lauschke, V.M. Genetic Variation in the Human Cytochrome P450 Supergene Family. Pharm. Genom. 2015, 25, 584–594. [Google Scholar] [CrossRef]
- van der Wouden, C.H.; van Rhenen, M.H.; Jama, W.O.M.; Ingelman-Sundberg, M.; Lauschke, V.M.; Konta, L.; Schwab, M.; Swen, J.J.; Guchelaar, H.-J. Development of the PGx-Passport: A Panel of Actionable Germline Genetic Variants for Pre-Emptive Pharmacogenetic Testing. Clin. Pharmacol. Ther. 2019, 106, 866–873. [Google Scholar] [CrossRef]
- Gulilat, M.; Lamb, T.; Teft, W.A.; Wang, J.; Dron, J.S.; Robinson, J.F.; Tirona, R.G.; Hegele, R.A.; Kim, R.B.; Schwarz, U.I. Targeted next Generation Sequencing as a Tool for Precision Medicine. BMC Med. Genom. 2019, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, U.I.; Gulilat, M.; Kim, R.B. The Role of Next-Generation Sequencing in Pharmacogenetics and Pharmacogenomics. Cold Spring Harb. Perspect. Med. 2019, 9, a033027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiita, A.P.; Schrijver, I. Clinical Application of High Throughput Molecular Screening Techniques for Pharmacogenomics. Pharm. Pers. Med. 2011, 4, 109–121. [Google Scholar] [CrossRef] [Green Version]
- Mulder, T.A.M.; van Eerden, R.A.G.; de With, M.; Elens, L.; Hesselink, D.A.; Matic, M.; Bins, S.; Mathijssen, R.H.J.; van Schaik, R.H.N. CYP3A4∗22 Genotyping in Clinical Practice: Ready for Implementation? Front. Genet. 2021, 12, 711943. [Google Scholar] [CrossRef]
- Owen, R.P.; Gong, L.; Sagreiya, H.; Klein, T.E.; Altman, R.B. VKORC1 Pharmacogenomics Summary. Pharm. Genom. 2010, 20, 642–644. [Google Scholar] [CrossRef] [Green Version]
- Owen, R.P.; Sangkuhl, K.; Klein, T.E.; Altman, R.B. Cytochrome P450 2D6. Pharm. Genom. 2009, 19, 559–562. [Google Scholar] [CrossRef] [Green Version]
- Van Booven, D.; Marsh, S.; McLeod, H.; Carrillo, M.W.; Sangkuhl, K.; Klein, T.E.; Altman, R.B. Cytochrome P450 2C9-CYP2C9. Pharm. Genom. 2010, 20, 277–281. [Google Scholar] [CrossRef]
- Scott, S.A.; Sangkuhl, K.; Shuldiner, A.R.; Hulot, J.-S.; Thorn, C.F.; Altman, R.B.; Klein, T.E. PharmGKB Summary: Very Important Pharmacogene Information for Cytochrome P450, Family 2, Subfamily C, Polypeptide 19. Pharm. Genom. 2012, 22, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Swen, J.J.; Nijenhuis, M.; de Boer, A.; Grandia, L.; der Zee, A.M.; Mulder, H.; Rongen, G.; van Schaik, R.; Schalekamp, T.; Touw, D.J.; et al. Pharmacogenetics: From Bench to Byte— An Update of Guidelines. Clin. Pharmacol. Ther. 2011, 89, 662–673. [Google Scholar] [CrossRef]
- Luzum, J.A.; Petry, N.; Taylor, A.K.; Van Driest, S.L.; Dunnenberger, H.M.; Cavallari, L.H. Moving Pharmacogenetics Into Practice: It’s All About the Evidence! Clin. Pharmacol. Ther. 2021, 110, 649–661. [Google Scholar] [CrossRef]
- Birdwell, K.A.; Decker, B.; Barbarino, J.M.; Peterson, J.F.; Stein, C.M.; Sadee, W.; Wang, D.; Vinks, A.A.; He, Y.; Swen, J.J.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for CYP3A5 Genotype and Tacrolimus Dosing. Clin. Pharmacol. Ther. 2015, 98, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamba, J.; Hebert, J.M.; Schuetz, E.G.; Klein, T.E.; Altman, R.B. PharmGKB Summary: Very Important Pharmacogene Information for CYP3A5. Pharm. Genom. 2012, 22, 555–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorn, C.F.; Aklillu, E.; Klein, T.E.; Altman, R.B. PharmGKB Summary: Very Important Pharmacogene Information for CYP1A2. Pharm. Genom. 2012, 22, 73–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouvet, R.; Verdier, M.-C.; El Baroudi, Y.; Galibert, M.-D.; David, V.; Schutz, S.; Tron, C. PharmFrag: An Easy and Fast Multiplex Pharmacogenetics Assay to Simultaneously Analyze 9 Genetic Polymorphisms Involved in Response Variability of Anticancer Drugs. Int. J. Mol. Sci. 2020, 21, 9650. [Google Scholar] [CrossRef] [PubMed]
- Thorn, C.F.; Müller, D.J.; Altman, R.B.; Klein, T.E. PharmGKB Summary: Clozapine Pathway, Pharmacokinetics. Pharm. Genom. 2018, 28, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Kudo, S.; Ishizaki, T. Pharmacokinetics of Haloperidol: An Update. Clin. Pharmacokinet. 1999, 37, 435–456. [Google Scholar] [CrossRef] [PubMed]
- Vinka Alkaloid Pathway, Pharmacokinetics. Available online: https://www.pharmgkb.org/pathway/PA150981002 (accessed on 28 July 2021).
- Bank, P.C.D.; Swen, J.J.; Guchelaar, H.J. Estimated Nationwide Impact of Implementing a Preemptive Pharmacogenetic Panel Approach to Guide Drug Prescribing in Primary Care in The Netherlands. BMC Med. 2019, 17, 110. [Google Scholar] [CrossRef] [Green Version]
- van Schaik, R.H.N.; Müller, D.J.; Serretti, A.; Ingelman-Sundberg, M. Pharmacogenetics in Psychiatry: An Update on Clinical Usability. Front. Pharmacol. 2020, 11, 575540. [Google Scholar] [CrossRef]
- Ubiquitous Pharmacogenomics (U-PGx)|Making Actionable Pharmacogenomic Data and Effective Treatment Optimization Accessible to Every European Citizen. Available online: https://upgx.eu/ (accessed on 3 August 2021).
- Klein, K.; Tremmel, R.; Winter, S.; Fehr, S.; Battke, F.; Scheurenbrand, T.; Schaeffeler, E.; Biskup, S.; Schwab, M.; Zanger, U.M. A New Panel-Based Next-Generation Sequencing Method for ADME Genes Reveals Novel Associations of Common and Rare Variants With Expression in a Human Liver Cohort. Front. Genet. 2019, 10, 7. [Google Scholar] [CrossRef] [Green Version]
- Pratt, V.M.; Cavallari, L.H.; Del Tredici, A.L.; Gaedigk, A.; Hachad, H.; Ji, Y.; Kalman, L.V.; Ly, R.C.; Moyer, A.M.; Scott, S.A.; et al. Recommendations for Clinical CYP2D6 Genotyping Allele Selection: A Joint Consensus Recommendation of the Association for Molecular Pathology, College of American Pathologists, Dutch Pharmacogenetics Working Group of the Royal Dutch Pharmacists Association, and the European Society for Pharmacogenomics and Personalized Therapy. J. Mol. Diagn. 2021, 21, 746–755. [Google Scholar] [CrossRef]
- Dorado, P.; Cáceres, M.; Pozo-Guisado, E.; Wong, M.-L.; Licinio, J.; Llerena, A. Development of a PCR-Based Strategy for CYP2D6 Genotyping Including Gene Multiplication of Worldwide Potential Use. Biotechniques 2005, 39, S571–S574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puaprasert, K.; Chu, C.; Saralamba, N.; Day, N.P.J.; Nosten, F.; White, N.J.; Dondorp, A.M.; Imwong, M. Real Time PCR Detection of Common CYP2D6 Genetic Variants and Its Application in a Karen Population Study. Malar. J. 2018, 17, 427. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Vnencak-Jones, C.L.; Roland, B.P.; Gatto, C.L.; Mathe, J.L.; Just, S.L.; Peterson, J.F.; Van Driest, S.L.; Weitkamp, A.O. A Tutorial for Pharmacogenomics Implementation Through End-to-End Clinical Decision Support Based on Ten Years of Experience from PREDICT. Clin. Pharmacol. Ther. 2021, 109, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Schuelke, M. An Economic Method for the Fluorescent Labeling of PCR Fragments. Nat. Biotechnol. 2000, 18, 233–234. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Gene | rsID | Type of Polymorphism | Frequency of the Variant Allele * | Consequence of Allelic Variant on Protein Functionality ** | Example of Drugs Potentially Impacted by the Polymorphism |
|---|---|---|---|---|---|
| ABCB1 | rs1045642 | SNP C > T | 0.507 | Reduced | Tacrolimus, Vincristine, Dabigatran, Some antipsychotics |
| ABCB1 | rs1128503 | SNP C > T | 0.427 | Reduced | |
| ABCB1 | rs2032582 | SNP G/T/A | T = 0.44 A = 0.001 | Reduced | |
| ABCB1 | rs2229109 | SNP G > A | 0.039 | Reduced | |
| CYP1A2 | rs762551 (*1F) | SNP C > A | 0.681 | Higher inducibility | Clozapine, Clopidogrel, Carbamazepine, Imatinib |
| CYP2C9 | rs1799853 (*2) | SNP C > T | 0.110 | Reduced | Warfarin, phenytoin |
| CYP2C9 | rs1057910 (*3) | SNP A > C | 0.065 | No function | |
| CYP2C19 | rs4244285 (*2) | SNP G > A | 0.150 | No function | Clopidogrel, Citalopram, Escitalopram, Sertraline, Imipramine, protons pump inhibitors, Voriconazole |
| CYP2C19 | rs4986893 (*3) | SNP G > A | 0.008 | No function | |
| CYP2C19 | rs12248560 (*17) | SNP C > T | 0.222 | Increased | |
| CYP2D6 | rs35742686 (*3) | delA | 0.011 | No function | Amitriptyline, Aripiprazole, Atomoxetine, Clomipramine, Codeine, Doxepin, Eliglustat, Flecainide, Haloperidol, Imipramine, Metoprolol, Nortriptyline, Paroxetine, Pimozide, Propafenone, Tamoxifen, Tramadol, Venlafaxine, Zuclopenthixol |
| CYP2D6 | rs3892097 (*4) | C > T | 0.182 | No function | |
| CYP2D6 | rs5030655 (*6) | delA | 0.002 | No function | |
| CYP2D6 | rs5030656 (*9) | delAAG | 0.019 | Reduced | |
| CYP3A4 | rs35599367 (*22) | C > T | 0.042 | Reduced | Tacrolimus, Statins |
| CYP3A5 | rs776746 (*3) | A > G | 0.887 | No function | Tacrolimus |
| VKORC1 | rs9923231 | −1639 G > A | 0.381 | Reduced | Warfarin |
| DNA Amount | |||||||
|---|---|---|---|---|---|---|---|
| Polymorphism | 1 ng | 2.5 ng | 5 ng | 10 ng | 50 ng | 250 ng | 500 ng |
| ABCB1-rs1045642 | 59 | 97 | 69 | 437 | 1121 | 5151 | 5967 |
| ABCB1-rs1128503 | 53 | 70 | 107 | 256 | 1119 | 2615 | 2638 |
| ABCB1-rs2032582 | 89 | 134 | 110 | 440 | 1365 | 5003 | 4731 |
| ABCB1-rs2229109 | 135 | 441 | 478 | 1241 | 4501 | 10,902 | 10,691 |
| CYP1A2-*1F | 56 | 164 | 131 | 649 | 1393 | 4320 | 3427 |
| CYP2C9-*2 | 118 | 274 | 260 | 1174 | 2683 | 6604 | 5518 |
| CYP2C9-*3 | 237 | 775 | 1011 | 2723 | 8621 | 15,517 | 14,752 |
| CYP2C19-*2 | 52 | 144 | 137 | 554 | 1754 | 4465 | 4096 |
| CYP2C19-*3 | 88 | 182 | 212 | 791 | 2134 | 4897 | 4023 |
| CYP2C19-*17 | 63 | 228 | 222 | 748 | 2658 | 11,053 | 12,688 |
| CYP2D6-*3 | 130 | 385 | 604 | 1266 | 5837 | 9932 | 11,488 |
| CYP2D6-*4 | N.D. | 94 | 141 | 254 | 721 | 762 | 602 |
| CYP2D6-*6 | N.D. | 100 | 242 | 304 | 2268 | 3437 | 4573 |
| CYP2D6-*9 | 53 | 101 | 169 | 361 | 1385 | 2366 | 2675 |
| CYP3A4-*22 | 143 | 356 | 352 | 1337 | 3553 | 8919 | 7619 |
| CYP3A5-*3 | 189 | 534 | 543 | 1579 | 5141 | 11,242 | 10,717 |
| VKORC1-rs9923231 | 136 | 315 | 386 | 948 | 3850 | 7534 | 7429 |
| Polymorphism | Mean Intensity with Fresh Pool | Mean Intensity with Pool FT5 | Mean Bias (%) (FT5 vs. Fresh) |
|---|---|---|---|
| ABCB1-rs1045642 | 1205 | 1138 | −6 |
| ABCB1-rs1128503 | 1281 | 701 | −45 |
| ABCB1-rs2032582 | 2480 | 1793 | −28 |
| ABCB1-rs2229109 | 5049 | 4344 | −14 |
| CYP1A2-*1F | 1660 | 1088 | −34 |
| CYP2C9-*2 | 3111 | 2120 | −32 |
| CYP2C9-*3 | 10,486 | 5711 | −46 |
| CYP2C19-*2 | 2073 | 1790 | −14 |
| CYP2C19-*3 | 2498 | 1100 | −56 |
| CYP2C19-*17 | 3004 | 2742 | −9 |
| CYP2D6-*3 | 7314 | 4187 | −43 |
| CYP2D6-*4 | 830 | 632 | −24 |
| CYP2D6-*6 | 3016 | 682 | −77 |
| CYP2D6-*9 | 1681 | 880 | −48 |
| CYP3A4-*22 | 4114 | 2841 | −31 |
| CYP3A5-*3 | 6126 | 4270 | −30 |
| VKORC1-rs9923231 | 4628 | 3015 | −35 |
| Gene | Genetic Polymorphism | Genotype | Number of DNA Samples (Multiplex Method) | Agreement with Reference Method |
|---|---|---|---|---|
| CYP1A2 | rs762551 (C > A) | WT | 15 | 100% |
| varHz | 21 | 100% | ||
| varHm | 13 | 100% | ||
| CYP2C9 | rs1799853 (C > T) | WT | 36 | 100% |
| varHz | 11 | 100% | ||
| varHm | 3 | 100% | ||
| rs1057910 (C > T) | WT | 36 | 100% | |
| varHz | 12 | 100% | ||
| varHm | 1 | 100% | ||
| CYP2C19 | rs4244285 (G > A) | WT | 31 | 100% |
| varHz | 11 | 100% | ||
| varHm | 1 | 100% | ||
| rs4986893 (G > A) | WT | 31 | 100% | |
| varHz | 1 | 100% | ||
| rs12248560 (G > A) | WT | 31 | 100% | |
| varHz | 18 | 100% | ||
| varHm | 1 | 100% | ||
| CYP2D6 | rs35742686 (A > G) | WT | 22 | 100% |
| varHz | 3 | 100% | ||
| rs3892097 (G > A) | WT | 22 | 100% | |
| varHz | 15 | 100% | ||
| varHm | 4 | 100% | ||
| rs5030655 (A > C) | WT | 22 | 100% | |
| varHz | 4 | 100% | ||
| rs5030656 (AAG > GAG) | WT | 22 | 100% | |
| varHz | 4 | 100% | ||
| CYP3A4 | rs35599367 (C > T) | WT | 101 | 100% |
| varHz | 14 | 100% | ||
| CYP3A5 | rs776746 (T > C) | WT | 3 | 100% |
| varHz | 37 | 100% | ||
| varHm | 81 | 100% | ||
| VKORC1 | rs9923231 (G > A) | WT | 9 | 100% |
| varHz | 10 | 100% | ||
| varHm | 9 | 100% | ||
| ABCB1 | rs1045642 (A > G) | WT | 17 | 100% |
| varHz | 39 | 100% | ||
| varHm | 33 | 100% | ||
| rs1128503 (A > G) | WT | 17 | 100% | |
| varHz | 27 | 100% | ||
| varHm | 12 | 100% | ||
| rs2032582 (T > G) | WT | 13 | 100% | |
| varHz | 23 | 100% | ||
| varHm | 18 | 100% | ||
| rs2032582 (T > A) | WT | 13 | 100% | |
| varHz | 4 | 100% | ||
| rs2229109 (C > T) | WT | 48 | 100% | |
| varHz | 9 | 100% |
| TaqMan® Genotyping Assays | Next Generation Sequencing | PCR Multiplex | ||
|---|---|---|---|---|
| Cost(1)per patient for 17 variants ($) | For 1 sample | 199.5 | 1450 | 36.7 |
| For 10 samples | 62.5 | 145 | 6 | |
| For 48 samples | 53.7 | 30 | 3 | |
| Time to analyze 17 variants/samples (h) | Time of technical workload/10 samples | 5 | 4 | 1 |
| Time in automate device/10 samples | 10 | 24 | 5 | |
| Time of analysis workload/10 samples | 2 | 1 | 0.5 | |
| Total | 17 | 29 | 6.5 | |
| Analytical parameters | DNA sample amounts needed (ng) | 50 | 5 | 50 |
| Stability of primer and fluorescent probes | Good | Good | Good | |
| Specificity | Good | Excellent | Good | |
| Sensitivity | Good | Excellent | Good | |
| Throughput | Medium | High | Medium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tron, C.; Bouvet, R.; Verdier, M.-C.; Lamoureux, F.; Hennart, B.; Dubourg, C.; Bellissant, E.; Galibert, M.-D. A Robust and Fast/Multiplex Pharmacogenetics Assay to Simultaneously Analyze 17 Clinically Relevant Genetic Polymorphisms in CYP3A4, CYP3A5, CYP1A2, CYP2C9, CYP2C19, CYP2D6, ABCB1, and VKORC1 Genes. Pharmaceuticals 2022, 15, 637. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15050637
Tron C, Bouvet R, Verdier M-C, Lamoureux F, Hennart B, Dubourg C, Bellissant E, Galibert M-D. A Robust and Fast/Multiplex Pharmacogenetics Assay to Simultaneously Analyze 17 Clinically Relevant Genetic Polymorphisms in CYP3A4, CYP3A5, CYP1A2, CYP2C9, CYP2C19, CYP2D6, ABCB1, and VKORC1 Genes. Pharmaceuticals. 2022; 15(5):637. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15050637
Chicago/Turabian StyleTron, Camille, Régis Bouvet, Marie-Clémence Verdier, Fabien Lamoureux, Benjamin Hennart, Christèle Dubourg, Eric Bellissant, and Marie-Dominique Galibert. 2022. "A Robust and Fast/Multiplex Pharmacogenetics Assay to Simultaneously Analyze 17 Clinically Relevant Genetic Polymorphisms in CYP3A4, CYP3A5, CYP1A2, CYP2C9, CYP2C19, CYP2D6, ABCB1, and VKORC1 Genes" Pharmaceuticals 15, no. 5: 637. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15050637