The Role of 18-Fluoro-2-Deoxy-Glucose Positron Emission Tomography/Computed Tomography as Response and Prognosis Predictive Factor of Concurrent Chemoradiotherapy after Induction Chemotherapy in Head and Neck Squamous Cell Carcinoma: A Prospective Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Therapeutic Principle
2.3. 18F-FDG PET/CT Examination
2.4. Image Interpretation
2.5. End Points
2.6. Statistics
3. Results
3.1. Patient Characteristics
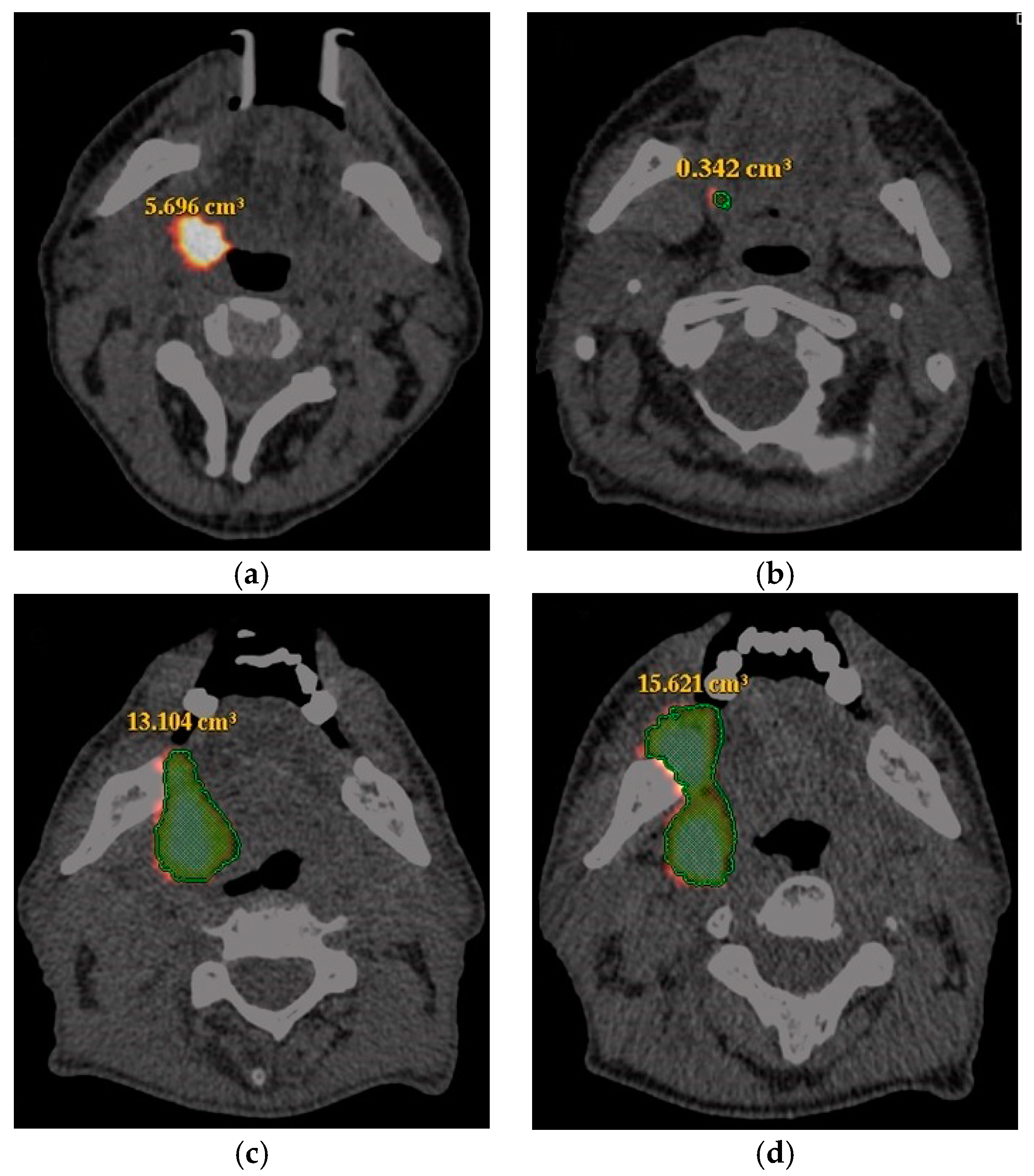
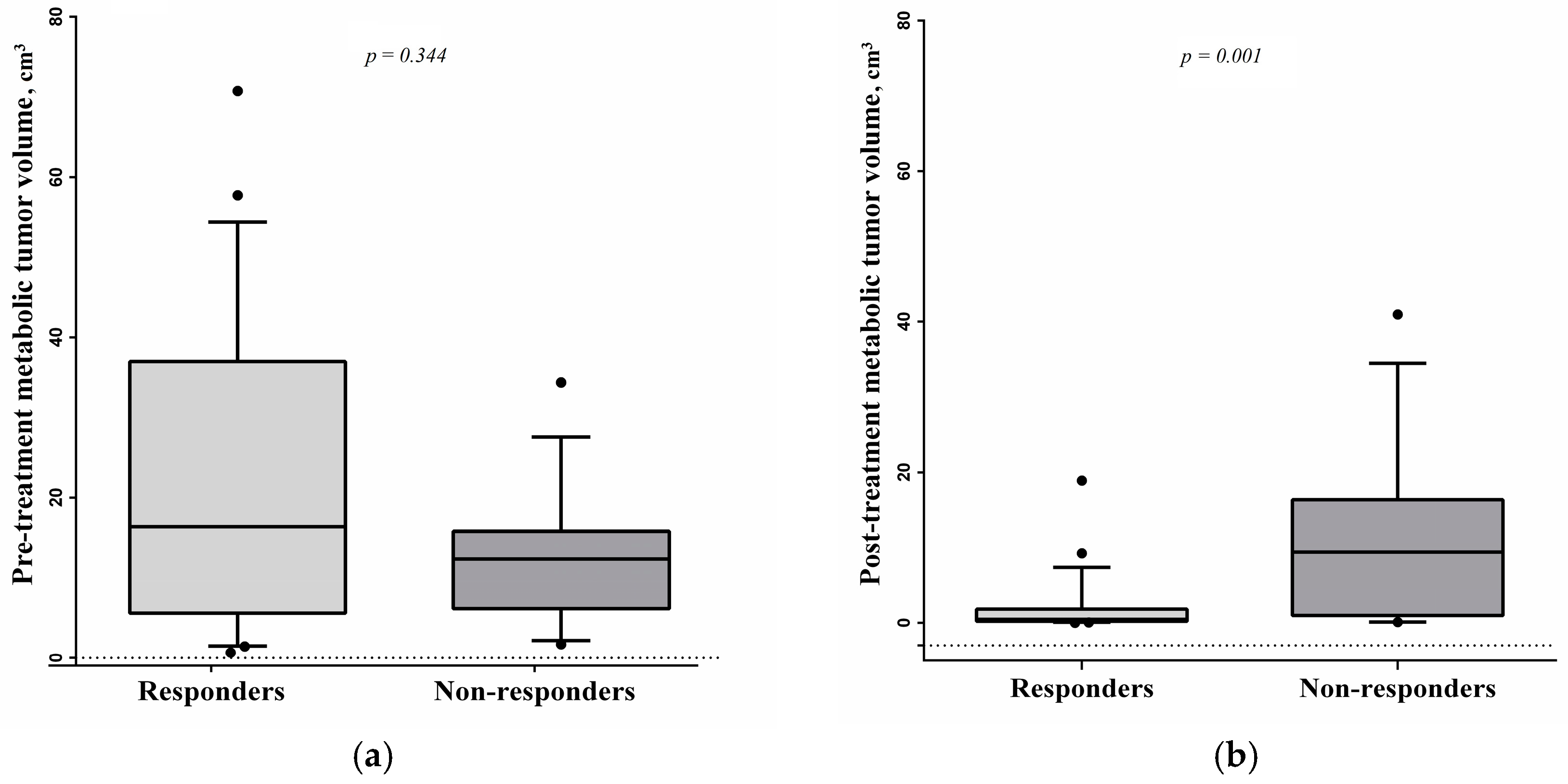
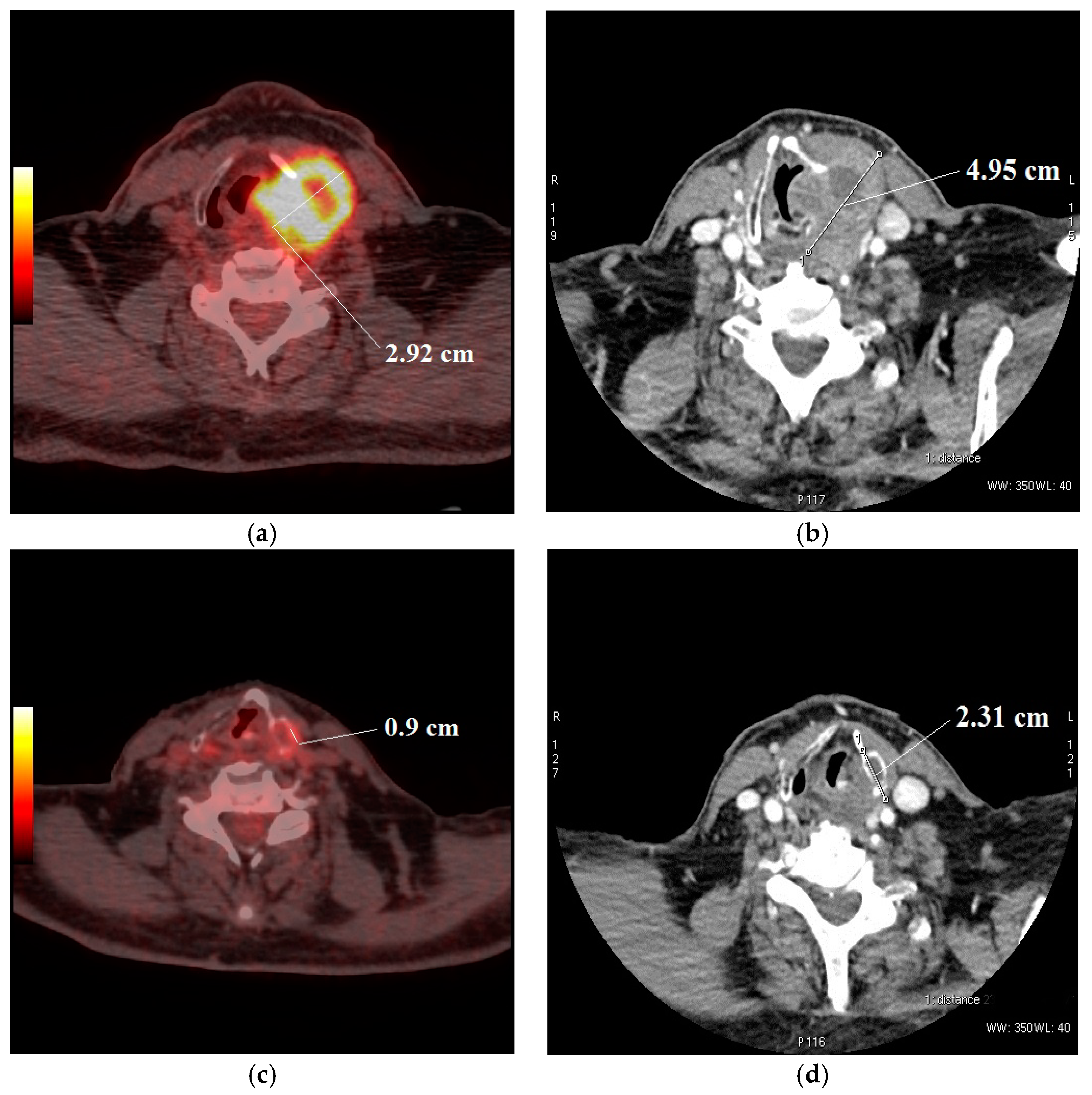
3.2. Response Evaluation
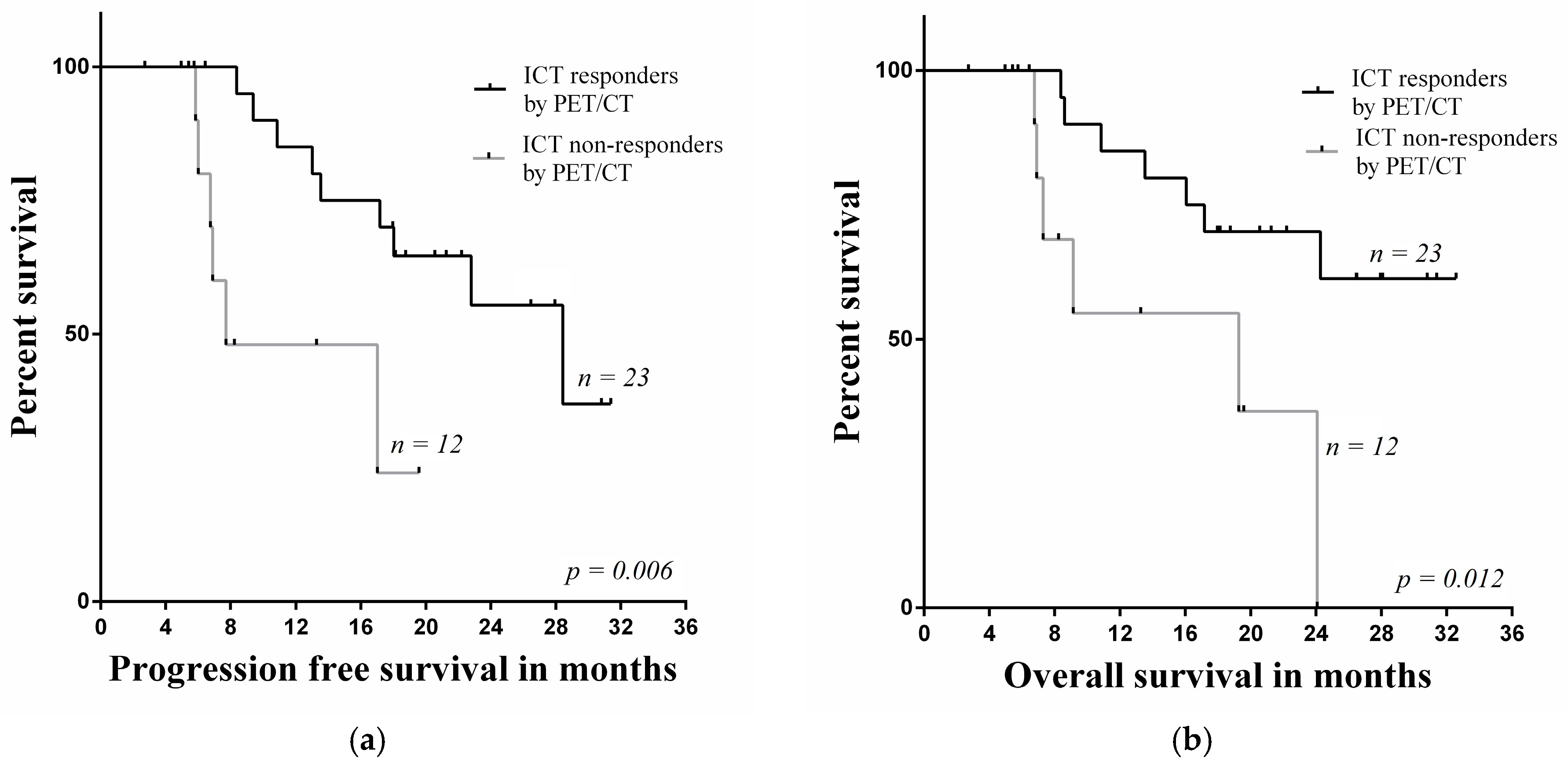
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bower, W.F.; Vlantis, A.C.; Chun, T.M.L.; Cheung, S.K.C.; Bjordal, K.; van Hasselt, C.A. Quality of life in head and neck cancer patients after surgical resection: Translation into Cantonese and validation of the EORTC QLQ-H&N35. Acta Oto-Laryngol. 2009, 129, 779–785. [Google Scholar]
- Mücke, T.; Koschinski, J.; Wolff, K.D.; Kanatas, A.; Mitchell, D.A.; Loeffelbein, D.J.; Deppe, H.; Rau, A. Quality of life after different oncologic interventions in head and neck cancer patients. J. Cranio-Maxillo-Facial Surg. 2015, 43, 1895–1898. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.R.; Park, H.S.; An, Y.; Contessa, J.N.; Yarbrough, W.G.; Burtness, B.A.; Decker, R.; Husain, Z. Comparison of Survival Outcomes Among Human Papillomavirus–Negative cT1-2 N1-2b Patients with Oropharyngeal Squamous Cell Cancer Treated with Upfront Surgery vs Definitive Chemoradiation Therapy: An Observational Study. JAMA Oncol. 2017, 3, 1107–1111. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, D.; Seikaly, H.; Murphy, R.; Fung, C.; Cooper, T.; Knox, A.; Scrimger, R.; Harris, J.R. Primary surgery versus chemoradiotherapy for advanced oropharyngeal cancers: A longitudinal population study. J. Otolaryngol. Head Neck Surg. 2013, 42, 31. [Google Scholar] [CrossRef] [PubMed]
- Abgral, R.; Le Roux, P.Y.; Keromnes, N.; Rousset, J.; Valette, G.; Gouders, D.; Leleu, C.; Mollon, D.; Nowak, E.; Querellou, S.; et al. Early prediction of survival following induction chemotherapy with DCF (docetaxel, cisplatin, 5-fluorouracil) using FDG PET/CT imaging in patients with locally advanced head and neck squamous cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Abgral, R.; Querellou, S.; Potard, G.; Le Roux, P.-Y.; Le Duc-Pennec, A.; Marianovski, R.; Pradier, O.; Bizais, Y.; Kraeber-Bodere, F.; Salaun, P.Y.; et al. Does 18F-FDG PET/CT improve the detection of posttreatment recurrence of head and neck squamous cell carcinoma in patients negative for disease on clinical follow-up? J. Nucl. Med. 2009, 50, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Cho, Y.; Kim, S.Y.; Nam, S.; Choi, S.; Lee, S.; Lee, J.; Kim, J.; Cho, K. Usefulness of interim FDG-PET after induction chemotherapy in patients with locally advanced squamous cell carcinoma of the head and neck receiving sequential induction chemotherapy followed by concurrent chemoradiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Adelstein, D.J.; Manola, J. Induction chemotherapy meta-analysis in head and neck cancer: Right answer, wrong question. J. Clin. Oncol. 2013, 31, 2844–2846. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, J.; Rolland, F.; Tesselaar, M.; Bardet, E.; Leemans, C.R.; Geoffrois, L.; Hupperets, P.; Barzan, L.; de Raucourt, D.; Chevalier, D.; et al. Phase 3 randomized trial on larynx preservation comparing sequential vs alternating chemotherapy and radiotherapy. J. Natl. Cancer Inst. 2009, 101, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Kawakita, D.; Masui, T.; Hanai, N.; Ozawa, T.; Hirakawa, H.; Terada, A.; Nishio, M.; Hosoi, H.; Hasegawa, Y. Impact of positron emission tomography with the use of fluorodeoxyglucose on response to induction chemotherapy in patients with oropharyngeal and hypopharyngeal squamous cell carcinoma. Acta Oto-Laryngol. 2013, 133, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Remenar, E.; Herpen, C.; Gorlia, T.; Mesia, R.; Degardin, M.; Stewart, J.S.; Jelic, S.; Betka, J.; Preiss, J.H.; et al. Cisplatin, Fluorouracil, and Docetaxel in unresectable head and neck cancer. N. Engl. J. Med. 2007, 357, 1695–16704. [Google Scholar] [CrossRef] [PubMed]
- Lorch, J.H.; Goloubeva, O.; Haddad, R.I.; Cullen, K.; Sarlis, N.; Tishler, R.; Tan, M.; Fasciano, J.; Sammartino, D.E.; Posner, M.R. Induction chemotherapy with cisplatin and fluorouracil alone or in combination with docetaxel in locally advanced squamous-cell cancer of the head and neck: Long-term results of the TAX 324 randomised phase 3 trial. Lancet Oncol. 2011, 12, 153–159. [Google Scholar] [CrossRef]
- Hitt, R.; Grau, J.J.; Lόpez-Pousa, A.; Berrocal, A.; García-Girón, C.; Irigoyen, A.; Sastre, J.; Martínez-Trufero, J.; Brandariz Castelo, J.A.; Verger, E.; et al. A randomized phase III trial comparing induction chemotherapy followed by chemoradiotherapy versus chemoradiotherapy alone as treatment of unresectable head and cancer. Ann. Oncol. 2013, 25, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.E.W.; Karrison, T.; Kocherginsky, M.; Mueller, J.; Egan, R.; Huang, C.H.; Brockstein, B.E.; Agulnik, M.B.; Mittal, B.B.; Yunus, F.; et al. Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J. Clin. Oncol. 2014, 32, 2735–2743. [Google Scholar] [CrossRef] [PubMed]
- Haddad, R.I.; Rabinowits, G.; Tishler, R.B.; Khuri, F.; Adkins, D.; Clark, J.; Sarlis, N.; Lorch, J.; Beitler, J.J.; Limaye, S.; et al. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 257–264. [Google Scholar] [CrossRef]
- Powell, C.; Schmidt, M.; Borri, M. Changes in functional imaging parameters following induction chemotherapy have important implications for individualized patient-based treatment regimens for advanced head and neck cancer. Radiother. Oncol. 2013, 106, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Gavid, M.; Prevot-Bitot, N.; Timoschenko, A.; Gallet, P.; Martin, C.; Prades, J.-M. [18F]-FDG PET-CT prediction of response to induction chemotherapy in head and neck squamous cell carcinoma: Preliminary findings. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-R.; Shim, H.-J.; Hwang, J.-E.; Cho, S.-H.; Chung, I.-J.; Park, K.S.; Kang, S.-R.; Kwon, S.-Y.; Chung, W.-K.; Bae, W.K. The role of interim PET-CT after induction chemotherapy as a predictor of concurrent chemoradiotherapy efficacy and prognosis for head and neck cancer. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Allal, A.S.; Dulguerov, P.; Allaoua, M.; Haenggeli, C.-A.; El Ghazi, E.A.; Lehmann, W.; Slosman, D.O. Standardized uptake value of 2-[18F] fluoro-2-deoxy-D-glucose in predicting outcome in head and neck carcinomas treated by radiotherapy with or without chemotherapy. J. Clin. Oncol. 2002, 20, 1398–1404. [Google Scholar] [CrossRef] [PubMed]
- Hentschel, M.; Appold, S.; Schreiber, A.; Abolmaali, N.; Abramyuk, A.; Dörr, W.; Kotzerke, J.; Baumann, M.; Zöphel, K. Early FDG PET at 10 or 20Gy under chemoradiotherapy is prognostic for locoregional control and overall survival in patients with head and neck cancer. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Yen, R.-F.; Chen, T.H.-H.; Ting, L.-L.; Tzen, K.-Y.; Pan, M.-H.; Hong, R.-L. Early restaging whole-body 18F-FDG PET during induction chemotherapy predicts clinical outcome in patients with locoregionally advanced nasopharyngeal carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Allegra, E.; Saita, V.; De Natale, M.; Trapasso, S.; Tamburrini, S.; Alessio, C.; Ippolito, M. Use of PET/CT to detect local and regional laryngeal cancer recurrence after surgery. Rep. Med. Imaging 2017, 10, 31–36. [Google Scholar] [CrossRef]
- Kikuchi, M.; Nakamoto, Y.; Shinohara, S.; Fujiwara, K.; Yamazaki, H.; Kanazawa, Y.; Kurihara, R.; Kishimoto, I.; Harada, H.; Naito, Y. Early evaluation of neoadjuvant chemotherapy response using FDG-PET/CT predicts survival prognosis in patients with head and neck squamous cell carcinoma. Int. J. Clin. Oncol. 2013, 18, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Brun, E.; Kjellen, E.; Tennvall, J.; Ohlsson, T.; Sandell, A.; Perfekt, R.; Perfekt, R.; Wennerberg, J.; Strand, S.E. FDG PET studies during treatment: Prediction of therapy outcome in head and neck squamous cell carcinoma. Head Neck 2002, 24, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Allal, A.S.; Slosman, D.O.; Kebdani, T.; Allaoua, M.; Lehmann, W.; Dulguerov, P. Prediction of outcome in head-and-neck cancer patients using the standardized uptake value of 2-[18F] fluoro-2-deoxy-d-glucose. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Dalsaso, T.A., Jr.; Lowe, V.J.; Dunphy, F.R.; Martin, D.S.; Boyd, J.H.; Stack, B.C., Jr. FDG-PET and CT in evaluation of chemotherapy in advanced head and neck cancer. Clin. Positron Imaging 2000, 3, 1–5. [Google Scholar] [CrossRef]
- Chepeha, D.B.; Sacco, A.G.; Oxford, L.E.; Karamchandani, R.; Miller, T.H.; Teknos, T.N.; Bradford, C.R.; Eisbruch, A.; Worden, F.M.; Urba, S.G.; et al. Advanced squamous cell carcinoma of the oropharynx: Efficacy of positron emission tomography and computed tomography for determining primary tumor response during induction chemotherapy. Head Neck 2009, 31, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Jacene, H.A.; Leboulleux, S.; Baba, S.; Chatzifotiadis, D.; Goudarzi, B.; Teytelbaum, O.; Horton, K.M.; Kamel, I.; Macura, K.J.; Tsai, H.-L.; et al. Assessment of interobserver reproducibility in quantitative 18F-FDG PET and CT measurements of tumor response to therapy. J. Nucl. Med. 2009, 50, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Kostakoglu, L.; Goldsmith, S.J. PET in the Assessment of Therapy Response in Patients with Carcinoma of the Head and Neck and of the Esophagus. J. Nucl. Med. 2004, 45, 56–68. [Google Scholar] [PubMed]
- Remeijer, P.; Rasch, C.; Lebesque, J.V.; van Herk, M. A general methodology for three-dimensional analysis of variation in target volume delineation. Med. Phys. 1999, 26, 931–940. [Google Scholar] [CrossRef] [PubMed]
- Senft, A.; De Bree, R.; Golding, R.P.; Comans, E.F.I.; Van Waesberghe, J.-H.T.M.; Kuik, J.D.; Hoekstra, O.S.; Leemans, C.R. Interobserver variability in chest CT and whole body FDG-PET screening for distant metastases in head and neck cancer patients. Mol. Imaging Biol. 2011, 13, 385–390. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total, n (%) (n = 35) |
|---|---|
| Age (mean, years) | 56.5 ± 8.6 |
| Sex | |
| Male | 33 (94.3) |
| Female | 2 (5.7) |
| Stage of tumor | |
| T1 | 1 (2.9) |
| T2 | 7 (20) |
| T3 | 8 (22.9) |
| T4 | 19 (54.3) |
| Nodal stage | |
| N0–1 | 9 (25.7) |
| N2 | 25 (71.4) |
| N3 | 1 (2.9) |
| Overall stage | |
| III | 6 (17.1) |
| IV | 29 (82.9) |
| Histological grade | |
| G2 | 24 (68.6) |
| G3 | 11 (31.4) |
| Variables | Univariate Analysis | ||
|---|---|---|---|
| HR | 95% CI | p | |
| Age (<65 vs. ≥65) | 1.402 | 0.306–6.414 | 0.663 |
| Gender (female vs. male) | 0.792 | 0.101–6.198 | 0.824 |
| pT status (T1-2 vs T3-4) | 0.676 | 0.148–3.089 | 0.613 |
| N status (N0–1 vs. N2–3) | 0.368 | 0.079–1.711 | 0.202 |
| Stage (III vs. IV) | 0.281 | 0.036–2.193 | 0.226 |
| Differentiation (poor vs. moderate) | 2.435 | 0.533–11.127 | 0.251 |
| SUVmax (<30% vs. ≥30%) | 0.228 | 0.073–0.715 | 0.011 |
| SUVmax groups (<10 vs. >10 and <14.5 vs. ≥14.5) | 0.580 | 0.176–1.914 | 0.371 |
| SUVmax groups (<3.5 vs. ≥3.5) | 0.033 | 0.001–11.414 | 0.253 |
| Volume (<55% vs. ≥55%) | 0.108 | 0.032–0.363 | 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šedienė, S.; Kulakienė, I.; Rudžianskas, V.; Ambrazienė, R. The Role of 18-Fluoro-2-Deoxy-Glucose Positron Emission Tomography/Computed Tomography as Response and Prognosis Predictive Factor of Concurrent Chemoradiotherapy after Induction Chemotherapy in Head and Neck Squamous Cell Carcinoma: A Prospective Study. Medicina 2018, 54, 31. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54020031
Šedienė S, Kulakienė I, Rudžianskas V, Ambrazienė R. The Role of 18-Fluoro-2-Deoxy-Glucose Positron Emission Tomography/Computed Tomography as Response and Prognosis Predictive Factor of Concurrent Chemoradiotherapy after Induction Chemotherapy in Head and Neck Squamous Cell Carcinoma: A Prospective Study. Medicina. 2018; 54(2):31. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54020031
Chicago/Turabian StyleŠedienė, Severina, Ilona Kulakienė, Viktoras Rudžianskas, and Rita Ambrazienė. 2018. "The Role of 18-Fluoro-2-Deoxy-Glucose Positron Emission Tomography/Computed Tomography as Response and Prognosis Predictive Factor of Concurrent Chemoradiotherapy after Induction Chemotherapy in Head and Neck Squamous Cell Carcinoma: A Prospective Study" Medicina 54, no. 2: 31. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54020031