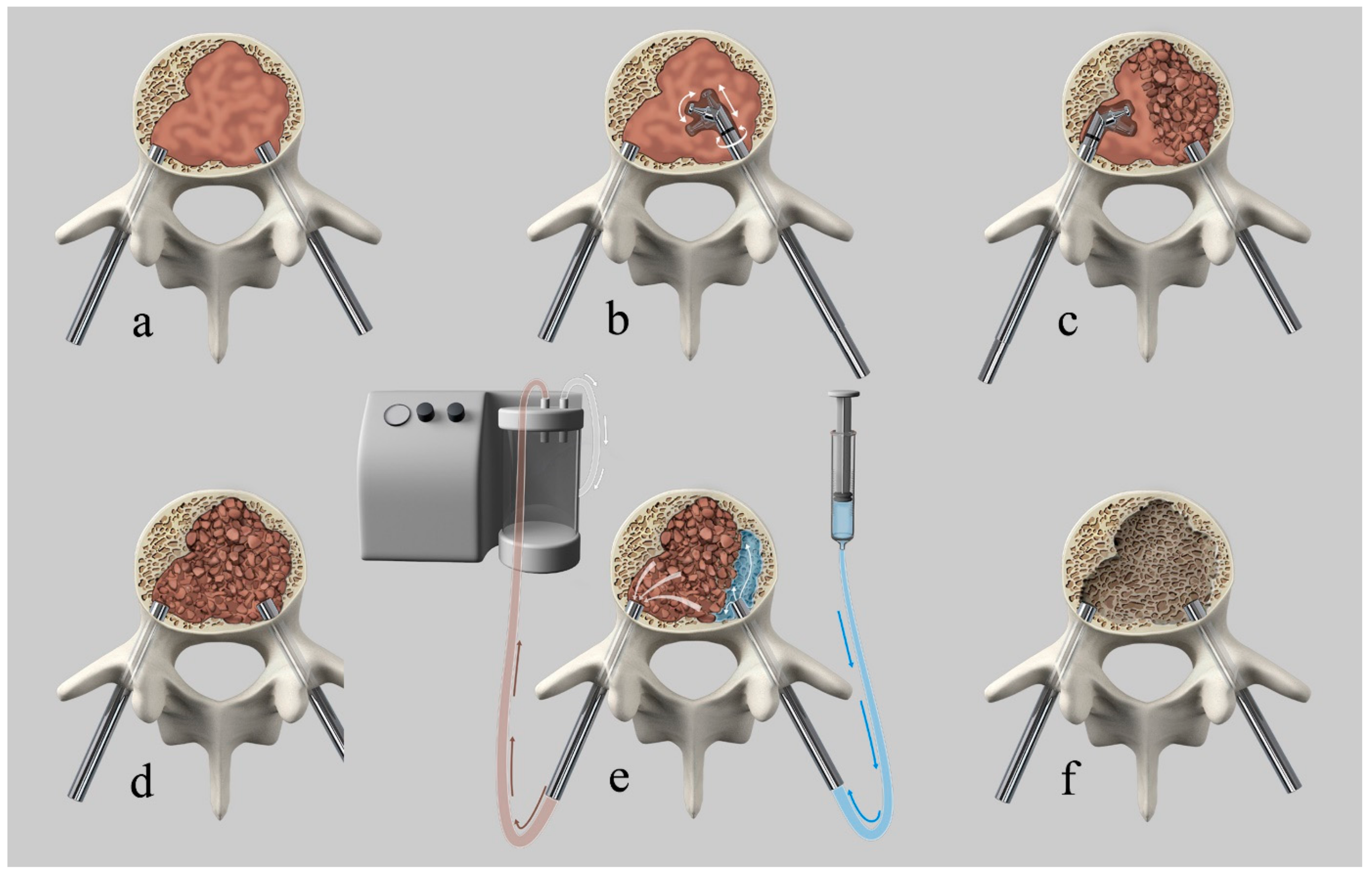
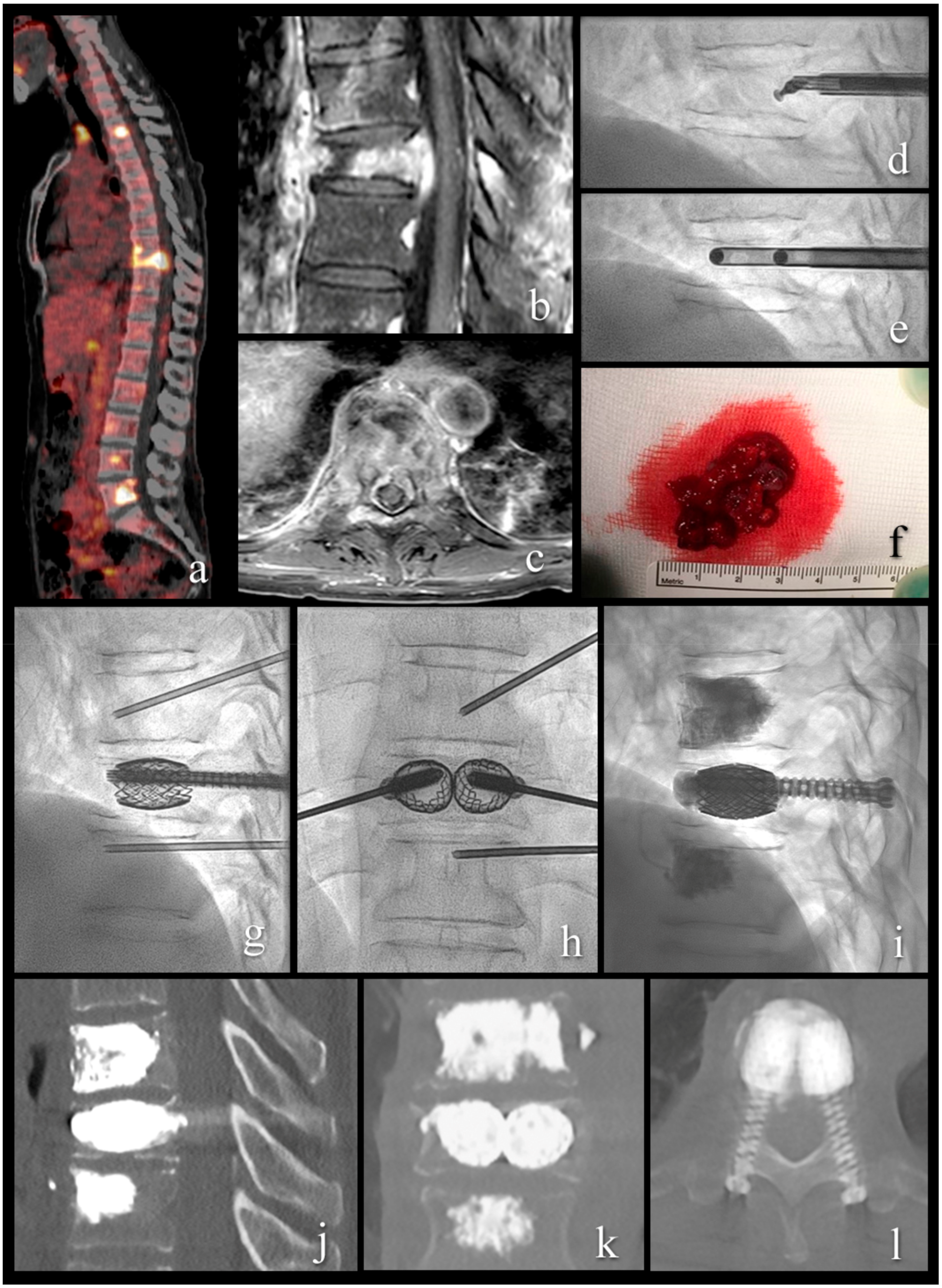
Mechanical Cavity Creation with Curettage and Vacuum Suction (Q-VAC) in Lytic Vertebral Body Lesions with Posterior Wall Dehiscence and Epidural Mass before Cement Augmentation

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
Procedural Details
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alvarez, L.; Perez-Higueras, A.; Quinones, D.; Calvo, E.; Rossi, R.E. Vertebroplasty in the treatment of vertebral tumors: Postprocedural outcome and quality of life. Eur. Spine J. 2003, 12, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Berenson, J.; Pflugmacher, R.; Jarzem, P.; Zonder, J.; Schechtman, K.; Tillman, J.B.; Bastian, L.; Ashraf, T.; Vrionis, F.; Cancer Patient Fracture Evaluation. Balloon kyphoplasty versus non-surgical fracture management for treatment of painful vertebral body compression fractures in patients with cancer: A multicentre, randomised controlled trial. Lancet Oncol. 2011, 12, 225–235. [Google Scholar] [CrossRef]
- Cianfoni, A.; Raz, E.; Mauri, S.; Di Lascio, S.; Reinert, M.; Pesce, G.; Bonaldi, G. Vertebral augmentation for neoplastic lesions with posterior wall erosion and epidural mass. Am. J. Neuroradiol. 2015, 36, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Mikami, Y.; Numaguchi, Y.; Kobayashi, N.; Fuwa, S.; Hoshikawa, Y.; Saida, Y. Therapeutic effects of percutaneous vertebroplasty for vertebral metastases. Jpn. J. Radiol. 2011, 29, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Cianfoni, A.; Zecchi, V.; Cortese, M.C.; Rumi, N.; Colosimo, C. Instability and impending instability in patients with vertebral metastatic disease. Skelet. Radiol. 2019, 48, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Jha, R.M.; Hirsch, A.E.; Yoo, A.J.; Ozonoff, A.; Growney, M.; Hirsch, J.A. Palliation of compression fractures in cancer patients by vertebral augmentation: A retrospective analysis. J. Neurointerv. Surg. 2010, 2, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Chiras, J.; Depriester, C.; Weill, A.; Sola-Martinez, M.T.; Deramond, H. Percutaneous vertebral surgery. Technics and indications. J. Neuroradiol. 1997, 24, 45–59. [Google Scholar]
- Sun, G.; Li, L.; Jin, P.; Liu, X.W.; Li, M. Percutaneous vertebroplasty for painful spinal metastasis with epidural encroachment. J. Surg. Oncol. 2014, 110, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Anselmetti, G.C.; Zoarski, G.; Manca, A.; Masala, S.; Eminefendic, H.; Russo, F.; Regge, D. Percutaneous vertebroplasty and bone cement leakage: Clinical experience with a new high-viscosity bone cement and delivery system for vertebral augmentation in benign and malignant compression fractures. Cardiovasc. Interv. Radiol. 2008, 31, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yang, H.; Tang, T.; Qian, Z.; Chen, L.; Zhang, Z. Comparison of kyphoplasty and vertebroplasty for treatment of painful osteoporotic vertebral compression fractures: Twelve-month follow-up in a prospective nonrandomized comparative study. J. Spinal Disord. Tech. 2012, 25, 142–149. [Google Scholar] [CrossRef]
- Lis, E.; Laufer, I.; Barzilai, O.; Yamada, Y.; Karimi, S.; McLaughlin, L.; Krol, G.; Bilsky, M.H. Change in the cross-sectional area of the thecal sac following balloon kyphoplasty for pathological vertebral compression fractures prior to spine stereotactic radiosurgery. J. Neurosurg. Spine 2018, 30, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Cruz, J.P.; Sahgal, A.; Whyne, C.; Fehlings, M.G.; Smith, R. Tumor extravasation following a cement augmentation procedure for vertebral compression fracture in metastatic spinal disease. J. Neurosurg. Spine 2014, 21, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Axelsen, M.; Thomassen, L.D.; Bunger, C.; Bendtsen, M.; Zou, X.; Flo, C.; Wang, Y.; Rehling, M. Estimating risk of pulmonary neoplastic embolism during vertebroplasty. Spine 2012, 37, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, E.; Kroft, L.J.; Dijkstra, P.D. Treatment of vertebral tumor with posterior wall defect using image-guided radiofrequency ablation combined with vertebroplasty: Preliminary results in 12 patients. J. Vasc. Interv. Radiol. 2007, 18, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Aebli, N.; Krebs, J.; Schwenke, D.; Davis, G.; Theis, J.C. Cardiovascular changes during multiple vertebroplasty with and without vent-hole: An experimental study in sheep. Spine 2003, 28, 1502–1511. [Google Scholar] [CrossRef]
- Aebli, N.; Schwenke, D.; Davis, G.; Hii, T.; Theis, J.C.; Krebs, J. Polymethylmethacrylate causes prolonged pulmonary hypertension during fat embolism: A study in sheep. Acta Orthop. 2005, 76, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Kyriakou, C.; Molloy, S.; Vrionis, F.; Alberico, R.; Bastian, L.; Zonder, J.A.; Giralt, S.; Raje, N.; Kyle, R.A.; Roodman, D.G.D.; et al. The role of cement augmentation with percutaneous vertebroplasty and balloon kyphoplasty for the treatment of vertebral compression fractures in multiple myeloma: A consensus statement from the International Myeloma Working Group (IMWG). Blood Cancer J. 2019, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Yan, J.; Yang, Q.; Li, Z.; Li, J. The effect of void creation prior to vertebroplasty on intravertebral pressure and cement distribution in cadaveric spines with simulated metastases. J. Orthop. Surg. Res. 2015, 10, 20. [Google Scholar] [CrossRef]
- Nakatsuka, A.; Yamakado, K.; Maeda, M.; Yasuda, M.; Akeboshi, M.; Takaki, H.; Hamada, A.; Takeda, K. Radiofrequency ablation combined with bone cement injection for the treatment of bone malignancies. J. Vasc. Interv. Radiol. 2004, 15, 707–712. [Google Scholar] [CrossRef]
- Gardner, C.S.; Ensor, J.E.; Ahrar, K.; Huang, S.Y.; Sabir, S.H.; Tannir, N.M.; Lewis, V.O.; Tam, A.L. Cryoablation of Bone Metastases from Renal Cell Carcinoma for Local Tumor Control. J. Bone Jt. Surg. 2017, 99, 1916–1926. [Google Scholar] [CrossRef]
- Tomasian, A.; Wallace, A.; Northrup, B.; Hillen, T.J.; Jennings, J.W. Spine Cryoablation: Pain Palliation and Local Tumor Control for Vertebral Metastases. Am. J. Neuroradiol. 2016, 37, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Bastian, L.; Schils, F.; Tillman, J.B.; Fueredi, G.; Investigators, S. A randomized trial comparing 2 techniques of balloon kyphoplasty and curette use for obtaining vertebral body height restoration and angular-deformity correction in vertebral compression fractures due to osteoporosis. Am. J. Neuroradiol. 2013, 34, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Hershkovich, O.; Lucantoni, C.; Kapoor, S.; Boszczyk, B. Bone marrow washout for multilevel vertebroplasty in multiple myeloma spinal involvement. Technical note. Eur. Spine J. 2018, 28, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Cianfoni, A.; Distefano, D.; Pravata, E.; Espeli, V.; Pesce, G.; Mordasini, P.; La Barbera, L.; Scarone, P.; Bonaldi, G. Vertebral body stent augmentation to reconstruct the anterior column in neoplastic extreme osteolysis. J. Neurointerv. Surg. 2019, 11, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Cianfoni, A.; Distefano, D.; Isalberti, M.; Reinert, M.; Scarone, P.; Kuhlen, D.; Hirsch, J.A.; Bonaldi, G. Stent-screw-assisted internal fixation: The SAIF technique to augment severe osteoporotic and neoplastic vertebral body fractures. J. Neurointerv. Surg. 2018, 11, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Kam, N.M.; Maingard, J.; Kok, H.K.; Ranatunga, D.; Brooks, D.; Torreggiani, W.C.; Munk, P.L.; Lee, M.J.; Chandra, R.V.; Asadi, H. Combined Vertebral Augmentation and Radiofrequency Ablation in the Management of Spinal Metastases: An Update. Curr. Treat. Opt. Oncol. 2017, 18, 74. [Google Scholar] [CrossRef] [PubMed]
- Dabravolski, D.; Esser, J.; Lahm, A.; Merk, H. Surgical treatment of tumours and metastases of the spine by minimally invasive cavity-coblation method. J. Orthop. Surg. 2017, 25. [Google Scholar] [CrossRef]
- Trial, C.; Brancati, A.; Marnet, O.; Teot, L. Coblation technology for surgical wound debridement: Principle, experimental data, and technical data. Int. J. Low. Extrem. Wounds 2012, 11, 286–292. [Google Scholar] [CrossRef]
- Benneker, L.M.; Heini, P.F.; Suhm, N.; Gisep, A. The effect of pulsed jet lavage in vertebroplasty on injection forces of polymethylmethacrylate bone cement, material distribution, and potential fat embolism: A cadaver study. Spine 2008, 33, E906–E910. [Google Scholar] [CrossRef]
- Benneker, L.M.; Krebs, J.; Boner, V.; Boger, A.; Hoerstrup, S.; Heini, P.F.; Gisep, A. Cardiovascular changes after PMMA vertebroplasty in sheep: The effect of bone marrow removal using pulsed jet-lavage. Eur. Spine J. 2010, 19, 1913–1920. [Google Scholar] [CrossRef]
- Boger, A.; Benneker, L.M.; Krebs, J.; Boner, V.; Heini, P.F.; Gisep, A. The effect of pulsed jet lavage in vertebroplasty on injection forces of PMMA bone cement: An animal study. Eur. Spine J. 2009, 18, 1957–1962. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, S.; Elfiky, T.; Keel, M.J.; Aghayev, E.; Ecker, T.M.; Benneker, L.M. Lavage prior to vertebral augmentation reduces the risk for cement leakage. Eur. Spine J. 2016, 25, 3463–3469. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piechowiak, E.I.; Isalberti, M.; Pileggi, M.; Distefano, D.; Hirsch, J.A.; Cianfoni, A. Mechanical Cavity Creation with Curettage and Vacuum Suction (Q-VAC) in Lytic Vertebral Body Lesions with Posterior Wall Dehiscence and Epidural Mass before Cement Augmentation. Medicina 2019, 55, 633. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100633
Piechowiak EI, Isalberti M, Pileggi M, Distefano D, Hirsch JA, Cianfoni A. Mechanical Cavity Creation with Curettage and Vacuum Suction (Q-VAC) in Lytic Vertebral Body Lesions with Posterior Wall Dehiscence and Epidural Mass before Cement Augmentation. Medicina. 2019; 55(10):633. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100633
Chicago/Turabian StylePiechowiak, Eike I., Maurizio Isalberti, Marco Pileggi, Daniela Distefano, Joshua A. Hirsch, and Alessandro Cianfoni. 2019. "Mechanical Cavity Creation with Curettage and Vacuum Suction (Q-VAC) in Lytic Vertebral Body Lesions with Posterior Wall Dehiscence and Epidural Mass before Cement Augmentation" Medicina 55, no. 10: 633. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100633