CT- and MRI-Based Assessment of Body Composition and Pancreatic Fibrosis Reveals High Incidence of Clinically Significant Metabolic Changes That Affect the Quality of Life and Treatment Outcomes of Patients with Chronic Pancreatitis and Pancreatic Cancer

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Patients
2.1.1. Quality of Life
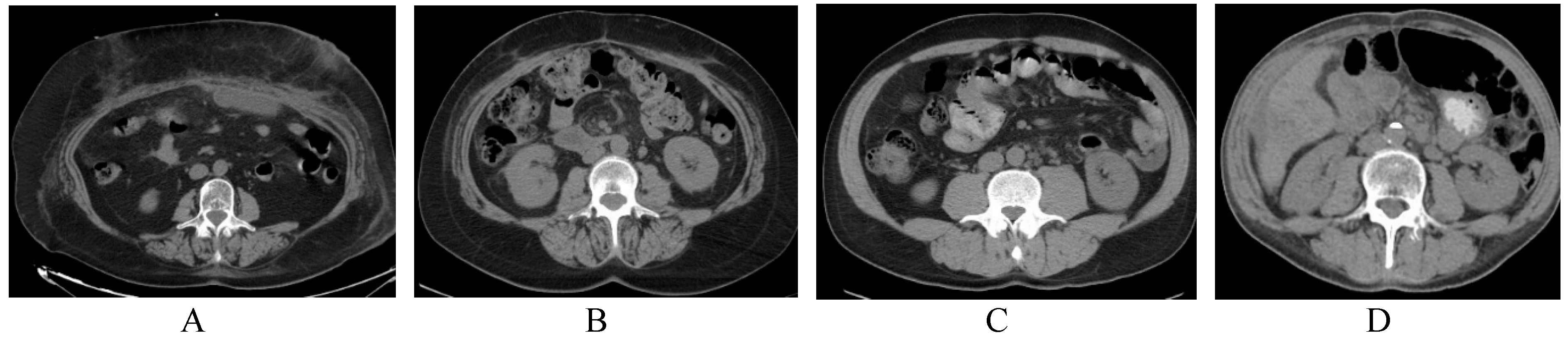
2.1.2. Assessment of Pancreatic Volume
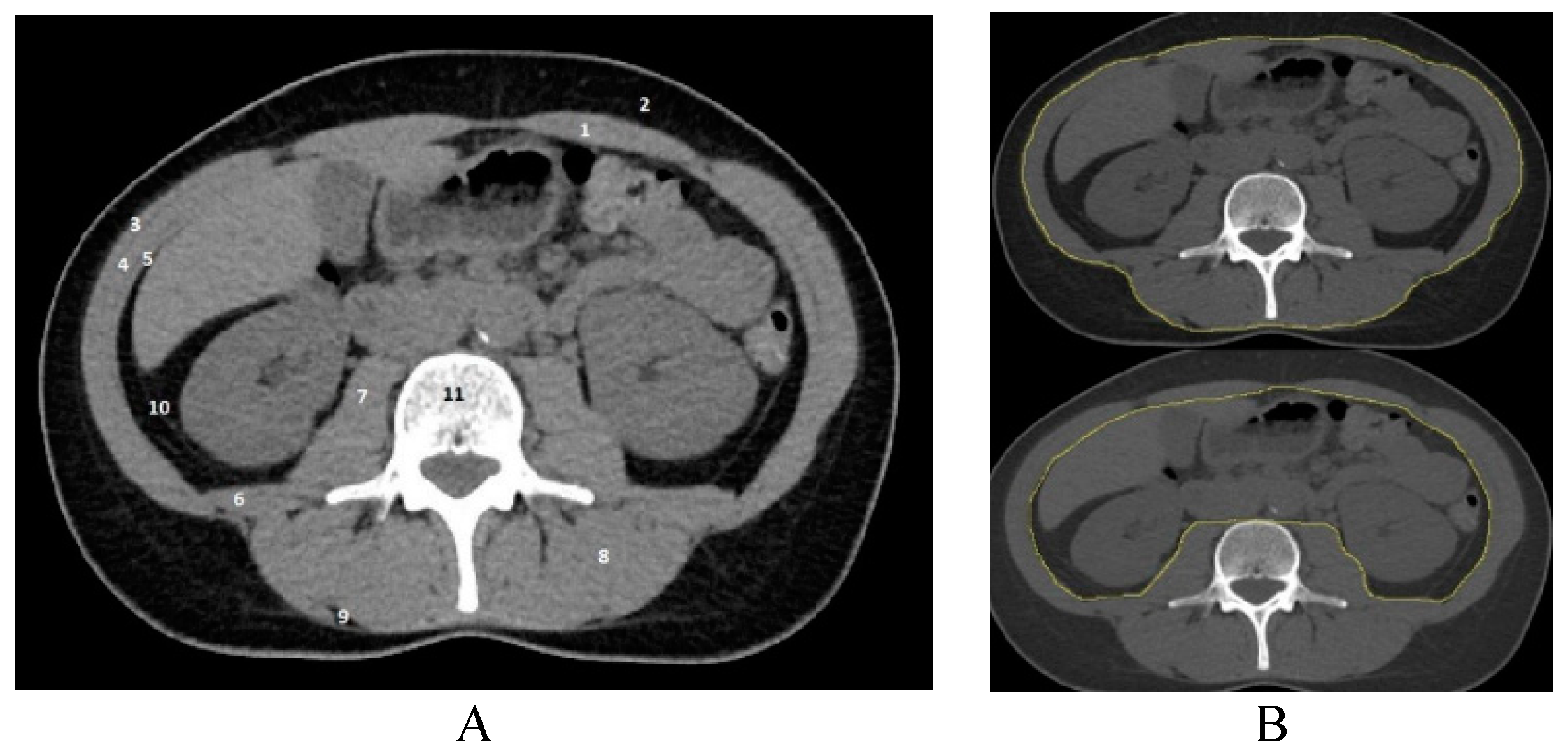
2.2. Assessment of Skeletal Muscle Mass
2.3. MRI Examination
2.4. Assessment of Bone Density
2.5. Pancreatic Exocrine Function Testing
2.6. Statistical Analysis
3. Results
3.1. Sarcopenia and Low Bone Density in Patients with Chronic Pancreatitis and Pancreatic Cancer
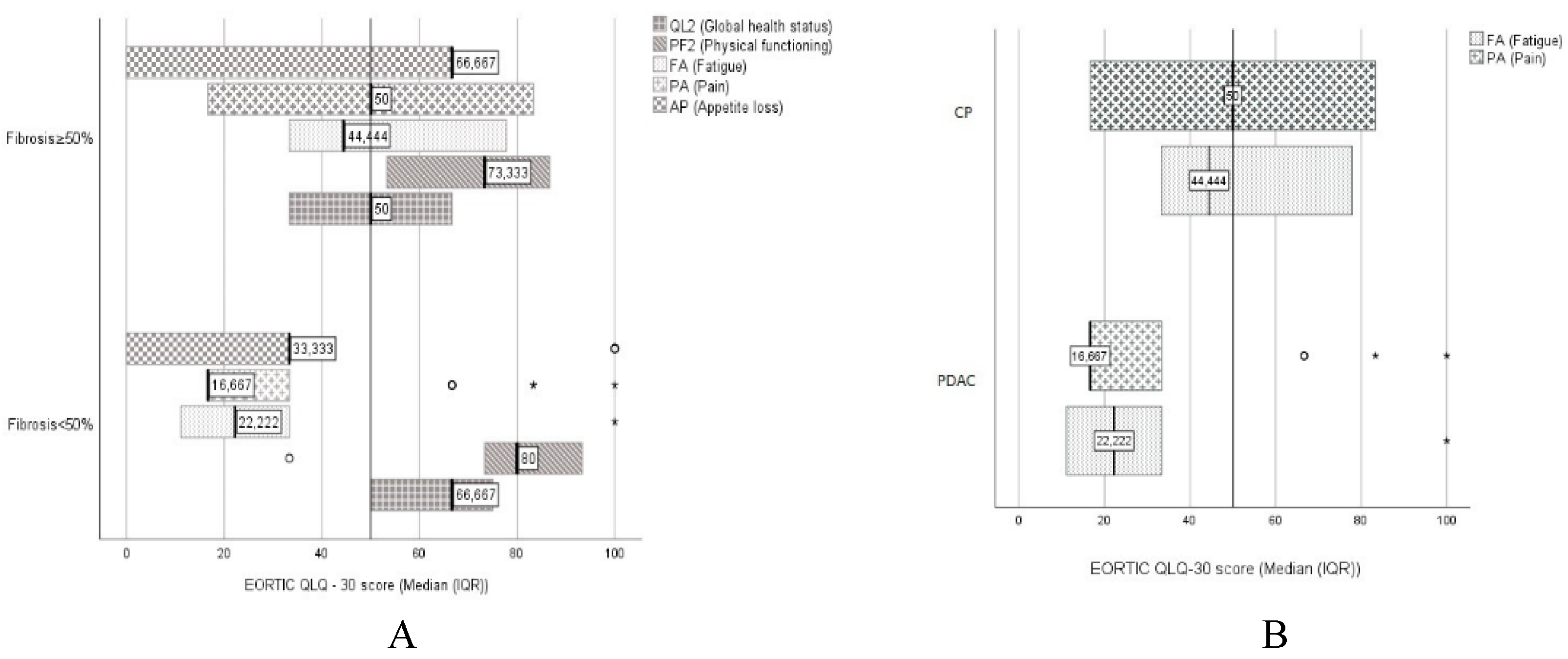
3.2. Symptoms Influencing Quality of Life in Patients with Severe Pancreatic Fibrosis and CP
4. Discussion
5. Conclusions
Study Limitations
Author Contributions
Conflicts of Interest
References
- Shimizu, K. Mechanisms of pancreatic fibrosis and applications to the treatment of chronic pancreatitis. J. Gastroenterol. 2008, 43, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Apte, M.V.; Wilson, J.S. Mechanisms of pancreatic fibrosis. Dig. Dis. 2004, 22, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Forsmark, C.E. Management of chronic pancreatitis. Gastroenterology 2013, 144, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Gupte, A.R.; Forsmark, C.E. Chronic pancreatitis. Curr. Opin. Gastroenterol. 2014, 30, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Lew, D.; Afghani, E.; Pandol, S. Chronic pancreatitis: Current status and challenges for prevention and treatment. Dig. Dis. Sci. 2017, 62, 1702–1712. [Google Scholar] [CrossRef] [PubMed]
- Bieliuniene, E.; Frøkjær, J.B.; Pockevicius, A.; Kemesiene, J.; Lukosevicius, S.; Basevicius, A.; Barauskas, G.; Dambrauskas, Z.; Gulbinas, A. Magnetic Resonance Imaging as a Valid Noninvasive Tool for the Assessment of Pancreatic Fibrosis. Pancreas 2019, 48, 85–93. [Google Scholar] [CrossRef]
- Masamune, A.; Kikuta, K.; Watanabe, T.; Satoh, K.; Hirota, M.; Shimosegawa, T. Hypoxia stimulates pancreatic stellate cells to induce fibrosis and angiogenesis in pancreatic cancer. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 295, G709–G717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apte, M.; Pirola, R.C.; Wilson, J.S. Pancreatic stellate cell: Physiologic role, role in fibrosis and cancer. Curr. Opin. Gastroenterol. 2015, 31, 416–423. [Google Scholar] [CrossRef]
- Evans, W.J.; Morley, J.E.; Argilés, J.; Bales, C.; Baracos, V.; Guttridge, D.; Jatoi, A.; Kalantar-Zadeh, K.; Lochs, H.; Mantovani, G.; et al. Cachexia: A New Definition. Clin. Nutr. 2008, 27, 793–799. [Google Scholar] [CrossRef]
- Tan, B.H.L.; Birdsell, L.A.; Martin, L.; Baracos, V.E.; Fearon, K.C.H. Sarcopenia in an Overweight or Obese Patient Is an Adverse Prognostic Factor in Pancreatic Cancer. Clin. Cancer Res. 2009, 15, 6973. [Google Scholar] [CrossRef]
- Uomo, G.; Gallucci, F.; Rabitti, P.G. Anorexia-Cachexia Syndrome in Pancreatic Cancer: Recent Development in Research and Management. JOP 2006, 7, 157–162. [Google Scholar] [PubMed]
- Deborah, F.; Stefan, K.; Giovanni, B.; Van Wyk, M.; Phillipus, B.; Claudio, B.; Peter, M.; George, S.L.; Johnson, C.D. Symptoms and Quality of Life in Chronic Pancreatitis Assessed by Structured Interview and the EORTC QLQ-C30 and QLQ-PAN26. Am. J. Gastroenterol. 2005, 100, 918. [Google Scholar]
- Gomez-Perez, S.L.; Haus, J.M.; Sheean, P.; Patel, B.; Mar, W.; Chaudhry, V.; McKeever, L.; Braunschweig, C. Measuring Abdominal Circumference and Skeletal Muscle from a Single Cross-Sectional CT Image: A Step-by-Step Guide for Clinicians Using National Institutes of Health ImageJ. JPEN J. Parenter. Enter. Nutr. 2016, 40, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Van der Werf, A.; Langius, J.A.E.; de van der Schueren, M.A.E.; Nurmohamed, S.A.; van der Pant, K.A.M.I.; Blauwhoff-Buskermolen, S.; Wierdsma, N.J. Percentiles for skeletal muscle index, area and radiation attenuation based on computed tomography imaging in a healthy Caucasian population. Eur. J. Clin. Nutr. 2018, 72, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Derstine, B.A.; Holcombe, S.A.; Ross, B.E.; Wang, N.C.; Su, G.L.; Wang, S.C. Skeletal Muscle Cutoff Values for Sarcopenia Diagnosis Using T10 to L5 Measurements in a Healthy US Population. Sci. Rep. 2018, 8, 11369. [Google Scholar] [CrossRef] [PubMed]
- Partelli, S.; Frulloni, L.; Minniti, C.; Bassi, C.; Barugola, G.; D’Onofrio, M.; Crippa, S.; Falconi, M. Fecal elastase-1 is an independent predictor of survival in advanced pancreatic cancer. Dig. Liver Dis. 2012, 44, 945–951. [Google Scholar] [CrossRef]
- Arthur, S.T.; Noone, J.M.; Van Doren, B.A.; Roy, D.; Blanchette, C.M. One-year prevalence, comorbidities and cost of cachexia-related inpatient admissions in the USA. Drugs Context 2014, 3, 212265. [Google Scholar] [CrossRef] [PubMed]
- Dodson, S.; Baracos, V.E.; Jatoi, A.; Evans, W.J.; Cella, D.; Dalton, J.T.; Steiner, M.S. Muscle Wasting in Cancer Cachexia: Clinical Implications, Diagnosis, and Emerging Treatment Strategies. Annu. Rev. Med. 2011, 62, 265–279. [Google Scholar] [CrossRef]
- Shintakuya, R.; Uemura, K.; Murakami, Y.; Kondo, N.; Nakagawa, N.; Urabe, K.; Okano, K.; Awai, K.; Higaki, T.; Sueda, T. Sarcopenia Is Closely Associated with Pancreatic Exocrine Insufficiency in Patients with Pancreatic Disease. Pancreatology 2017, 17, 70–75. [Google Scholar] [CrossRef]
- Grimby, G.; Saltin, B. The ageing muscle. Clin. Physiol. 1983, 3, 209–218. [Google Scholar] [CrossRef]
- Prado, C.M.; Heymsfield, S.B. Lean Tissue Imaging. JPEN J. Parenter. Enter. Nutr. 2018, 38, 940–953. [Google Scholar] [CrossRef] [PubMed]
- Dujsikova, H.; Dítě, P.; Tomandl, J.; Sevcikova, A.; Precechtelova, M. Occurrence of Metabolic Osteopathy in Patients with Chronic Pancreatitis. Pancreatology 2008, 8, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, Y. Age-Related Pathological Changes in the Pancreas. Front. Biosci. 2018, 10, 137–142. [Google Scholar] [CrossRef]
- Vitali, G.C.; Ronot, M.; Assalino, A.; Andres, A.; Terraz, S.; Puppa, G.; Giudicelli, G.; Toso, C.; Morel, P.; Berney, T. Sarcopenia Is a Predictor of Pancreatic Fistula Occurence after Duodenopancreatectomy. HPB 2016, 18, e385. [Google Scholar]
- Ratnayake, C.B.; Loveday, B.P.; Shrikhande, S.V.; Windsor, J.A.; Pandanaboyana, S. Impact of preoperative sarcopenia on postoperative outcomes following pancreatic resection: A systematic review and meta-analysis. Pancreatology 2018, 18, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Gianotti, L.; Besselink, M.G.; Sandini, M.; Hackert, T.; Conlon, K.; Gerritsen, A.; Griffin, O.; Fingerhut, A.; Probst, P.; Abu Hilal, M.; et al. Nutritional support and therapy in pancreatic surgery: A position paper of the International Study Group on Pancreatic Surgery (ISGPS). Surgery 2018, 164, 1035–1048. [Google Scholar] [CrossRef] [PubMed]
- Duggan, S.N.; O’Sullivan, M.; Hamilton, S.; Feehan, S.M.; Ridgway, P.F.; Conlon, K.C. Patients with Chronic Pancreatitis Are at Increased Risk for Osteoporosis. Pancreas 2011, 41, 1119–24. [Google Scholar] [CrossRef] [PubMed]
- Haas, S.; Krins, S.; Knauerhase, A.; Löhr, M. Altered Bone Metabolism and Bone Density in Patients with Chronic Pancreatitis and Pancreatic Exocrine Insufficiency. JOP 2015, 16, 58–62. [Google Scholar] [PubMed]
- Messina, C.; Maffi, G.; Vitale, J.A.; Ulivieri, F.M.; Guglielmi, G.; Sconfienza, L.M. Diagnostic imaging of osteoporosis and sarcopenia: A narrative review. Quant. Imaging Med. Surg. 2018, 8, 86–99. [Google Scholar] [CrossRef]
- Domínguez-Muñoz, J.E.; Phillips, M. Nutritional Therapy in Chronic Pancreatitis. Gastroenterol. Clin. N. Am. 2018, 47, 95–106. [Google Scholar] [CrossRef]
- Duggan, S.N. Negotiating the complexities of exocrine and endocrine dysfunction in chronic pancreatitis. Proc. Nutr. Soc. 2017, 76, 484–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokrowiecka, A.; Pinkowski, D.; Malecka-Panas, E.; Johnson, C.D. Clinical, emotional and social factors associated with quality of life in chronic pancreatitis. Pancreatology 2010, 10, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Machicado, J.D.; Amann, S.T.; Anderson, M.A.; Abberbock, J.; Sherman, S.; Conwell, D.L.; Cote, G.A.; Singh, V.K.; Lewis, M.D.; Alkaade, S.; et al. Quality of Life in Chronic Pancreatitis is Determined by Constant Pain, Disability/Unemployment, Current Smoking, and Associated Co-Morbidities. Am. J. Gastroenterol. 2017, 112, 633–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamada, S.; Shimosegawa, T.; Masamune, A. Pancreatic Fibrosis. Pancreapedia: The Exocrine Pancreas Knowledge Base, 18 November 2015. [Google Scholar] [CrossRef]
- Pezzilli, R. Pancreatic Diseases: The Need to Assess the Quality of Life. Pancreat. Disord. Ther. 2012, 2, 1–5. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Male (n = 66) | Female (n = 34) | p Value (chi square) | |
|---|---|---|---|
| Weight (kg ± SD) | 74.86 ± 12.70 | 68.21 ± 11.42 | 0.627 |
| Mean age (years ± SD) | 53.38 ± 14.49 | 58.88 ± 14.01 | |
| BMI (kg/m2) mean ± SD | 23.80 ± 3.88 | 24.08 ± 4.47 | 0.217 |
| Patients (no): | |||
| Underweight * | 4 (6%) | 4 (12%) | |
| Normal weight * | 41 (62%) | 15 (44%) | |
| Overweight and obesity * | 21 (32%) | 15 (44%) | |
| Sarcopenia (no) | 25 (38%) | 9 (26%) | 0.254 |
| Abnormal bone density (no) (osteopenia/osteoporosis) | 33 (50%) | 16 (47%) | 0.694 |
| Pancreatic fibrosis (%) | 51.20 ± 32.60 | 49.81 ± 31.66 | 0.381 |
| Mean (± SD) | (n = 30) | (n = 22) |
| Normal Muscle Mass (n = 66) | Sarcopenia (n = 34) | p Value | |
|---|---|---|---|
| (chi square) | |||
| Mean weight (kg) | 74.64 ± 14.02 | 68.21 ± 11.42 | 0.28 |
| BMI (kg/m2) mean ± SD | 25.14 ± 4.33 | 22.03 ± 4.07 | 0.002 |
| Patients (no): | |||
| Underweight * | 1 (2%) | 7 (21%) | |
| Normal weight * | 37 (56%) | 19 (56%) | |
| Overweight and obesity * | 28 (42%) | 8 (24%) | |
| Gender (female/male) | 25/41 | 9/25 | 0.25 |
| Mean age (years ± SD) | 53.67 ± 13.23 | 58.32 ± 16.46 | 0.391 |
| Cancer (no) | 24 (36%) | 13 (38%) | |
| Chronic pancreatitis (no) | 42 (64%) | 21 (62%) | 0.85 |
| Abnormal bone density (no) (osteopenia/osteoporosis) | 27 (41%) | 22 (65%) | 0.02 |
| Pancreas volume (mL) mean (SD) | 43.21 (27.65) | 39.82 (19.86) | 0.37 |
| Diabetes mellitus (DM) (no) | 19 (29%) | 7 (21%) | 0.52 |
| Fecal elastase-1 < 200 µg/g (no) | 40 (61%) | 21 (62%) | 0.91 |
| Fecal elastase-1 Median | 130.50 (183.171) | 111.00 (188.593) | 0.375 |
| (interquartile range(IQR)) |
| <50% Fibrosis | ≥50% Fibrosis | p Value (chi square) | |
|---|---|---|---|
| Number of patients | 39 | 61 | |
| Age (years ± SD) | 59 ± 2.3 | 53 ± 1.8 | |
| Osteopenia/osteoporosis (no) | 18 (46%) | 31 (51%) | 0.649 |
| Sarcopenia yes no | 15 (38%) 24 (62%) | 19 (31%) 42 (69%) | 0.45 |
| Pathology Ca * CP | 25 (64%) 14 (36%) | 12 (20%) 49 (80%) | <0.001 |
| Pancreas volume (mL) Mean (SD) | 51.82 (25.20) | 35.82 (23.35) | 0.422 |
| DM (no) | 5 (13%) | 21 (34%) | 0.006 |
| Fecal elastase-1 < 200 µg/g (no) | 12 (31%) | 49 (80%) | <0.001 |
| Fecal elastase-1 median (IQR) | 445.00 (179.48) | 123.00 (184.07) | 0.013 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bieliuniene, E.; Brøndum Frøkjær, J.; Pockevicius, A.; Kemesiene, J.; Lukosevicius, S.; Basevicius, A.; Atstupenaite, V.; Barauskas, G.; Ignatavicius, P.; Gulbinas, A.; et al. CT- and MRI-Based Assessment of Body Composition and Pancreatic Fibrosis Reveals High Incidence of Clinically Significant Metabolic Changes That Affect the Quality of Life and Treatment Outcomes of Patients with Chronic Pancreatitis and Pancreatic Cancer. Medicina 2019, 55, 649. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100649
Bieliuniene E, Brøndum Frøkjær J, Pockevicius A, Kemesiene J, Lukosevicius S, Basevicius A, Atstupenaite V, Barauskas G, Ignatavicius P, Gulbinas A, et al. CT- and MRI-Based Assessment of Body Composition and Pancreatic Fibrosis Reveals High Incidence of Clinically Significant Metabolic Changes That Affect the Quality of Life and Treatment Outcomes of Patients with Chronic Pancreatitis and Pancreatic Cancer. Medicina. 2019; 55(10):649. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100649
Chicago/Turabian StyleBieliuniene, Edita, Jens Brøndum Frøkjær, Alius Pockevicius, Jurate Kemesiene, Saulius Lukosevicius, Algidas Basevicius, Vaida Atstupenaite, Giedrius Barauskas, Povilas Ignatavicius, Antanas Gulbinas, and et al. 2019. "CT- and MRI-Based Assessment of Body Composition and Pancreatic Fibrosis Reveals High Incidence of Clinically Significant Metabolic Changes That Affect the Quality of Life and Treatment Outcomes of Patients with Chronic Pancreatitis and Pancreatic Cancer" Medicina 55, no. 10: 649. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100649