Factors Affecting Psychological Stress in Healthcare Workers with and without Chronic Pain: A Cross-Sectional Study Using Multiple Regression Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcome Measure
2.3. Statistical Analysis
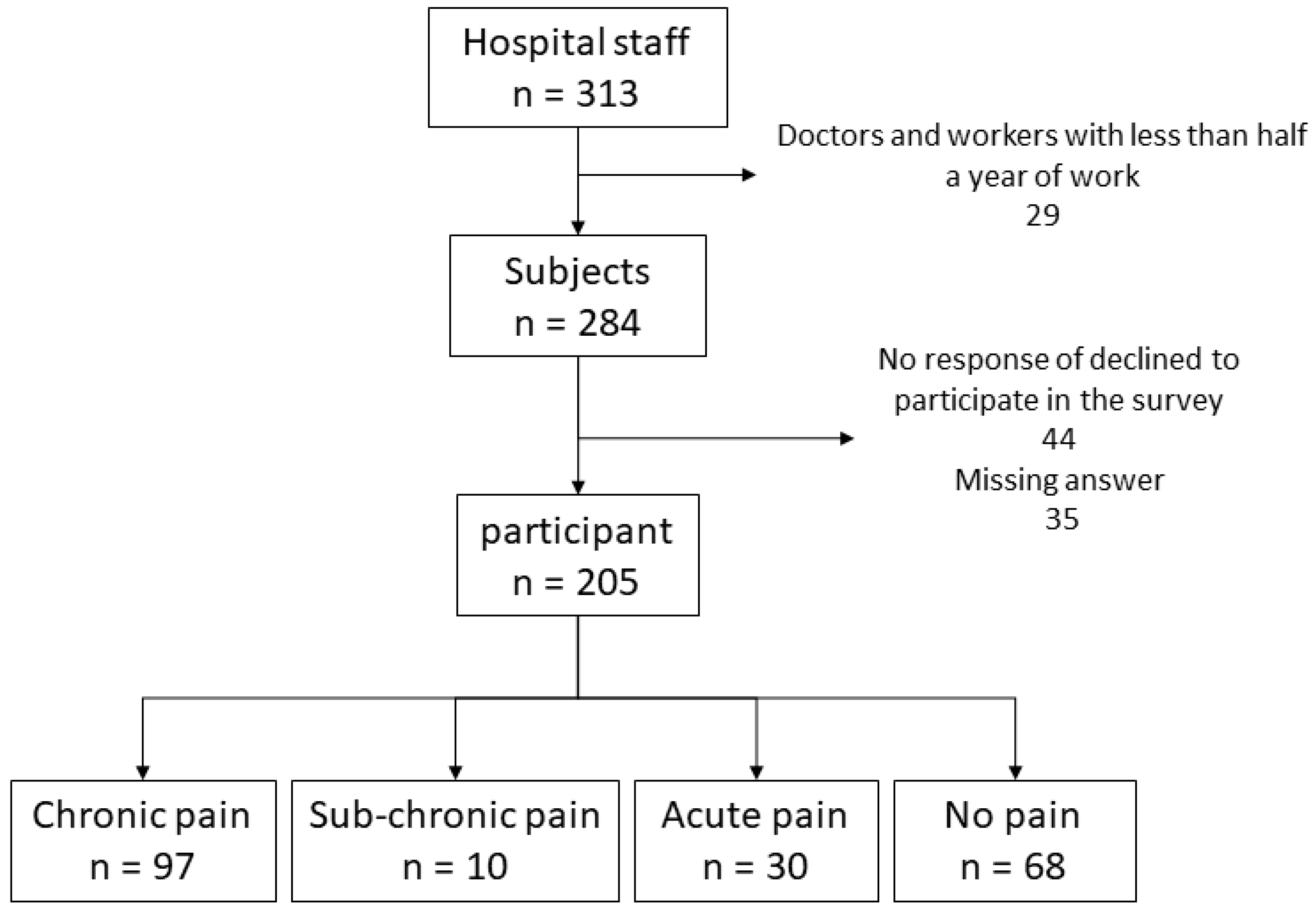
3. Results
4. Discussion
4.1. Participant Characteristics
4.2. Validation of Outcome Comparison between Two Groups
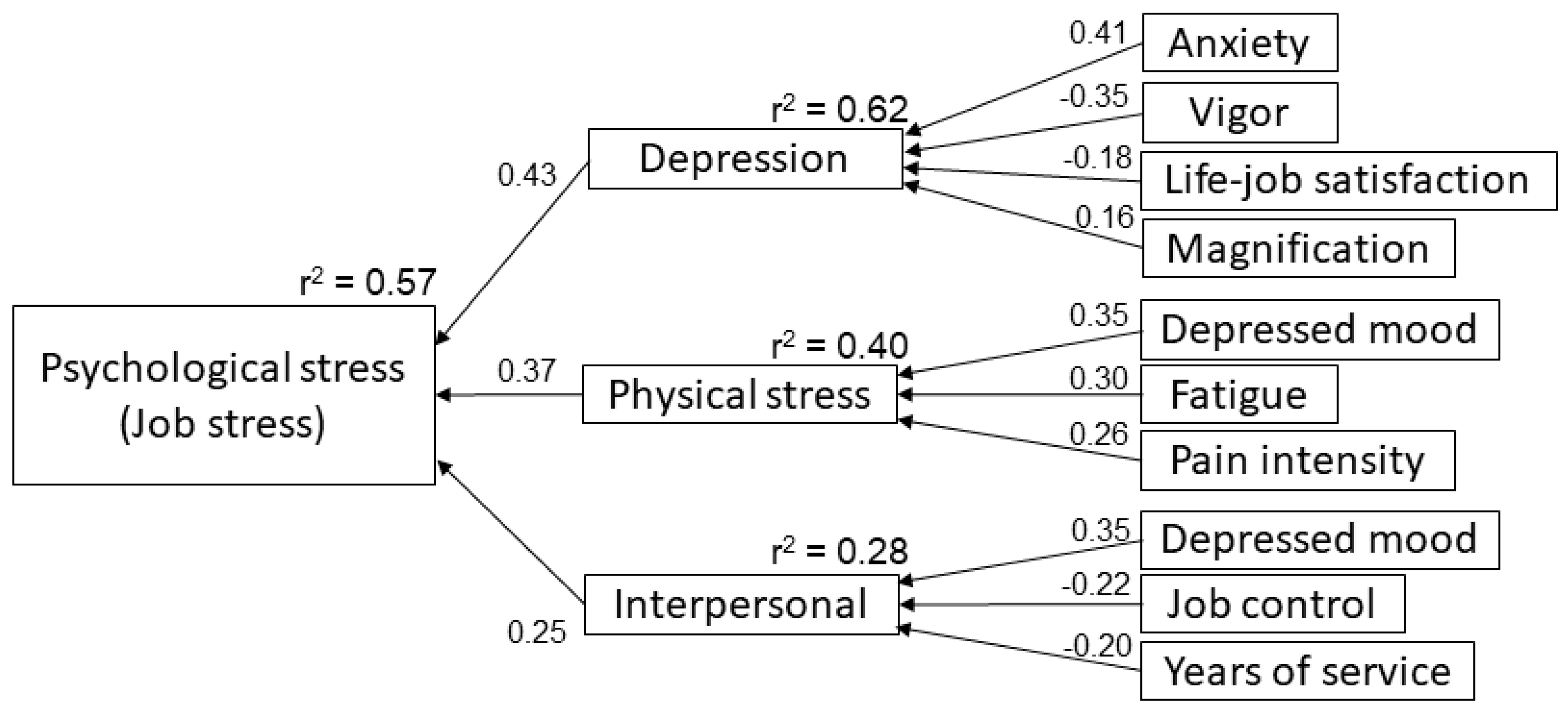
4.3. Validation of Structure Model by Multiple Regression Analysis
4.4. Highlight of This Study
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Meltem, I.Y. Economic and Social Consequences of Population Aging the Dilemmas and Opportunities in the Twenty-First Century. Appl. Res. Qual. Life 2015, 10, 735–752. [Google Scholar]
- Statistics Bureau Portal Site of Official Statistics of Japan, 2015 Population Census. Available online: http://www.stat.go.jp/english/data/kokusei/index.html (accessed on 11 June 2019).
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health--a meta-analytic review. Scand. J. Work. Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef] [PubMed]
- Grimani, A.; Bergström, G.; Casallas, M.I.R.; Aboagye, E.; Jensen, I.; Lohela-Karlsson, M. Economic Evaluation of Occupational Safety and Health Interventions from the Employer Perspective: A Systematic Review. J. Occup. Environ. Med. 2018, 60, 147–166. [Google Scholar] [CrossRef] [PubMed]
- Ravesteijn, B.; van Kippersluis, H.; van Doorslaer, E. The wear and tear on health: What is the role of occupation? Health Econ. 2018, 27, e69–e86. [Google Scholar] [CrossRef] [PubMed]
- Seidler, A.; Thinschmidt, M.; Deckert, S.; Then, F.; Hegewald, J.; Nieuwenhuijsen, K.; Riedel-Heller, S.G. The role of psychosocial working conditions on burnout and its core component emotional exhaustion—A systematic review. J. Occup. Med. Toxicol. 2014, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Avey, J.B.; Luthans, F.; Jensen, S.M. Psychological capital: A positive resource for combating employee stress and turnover. Hum. Resour. Manag. 2009, 48, 677–693. [Google Scholar] [CrossRef]
- Darr, W.; Johns, G. Work strain, health, and absenteeism: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 293–318. [Google Scholar] [CrossRef]
- Bubonya, M.; Cobb-Clark, D.A.; Wooden, M. Mental Health and Productivity at Work: Does What You Do Matter? Labour Econ. 2017, 46, 150–165. [Google Scholar] [CrossRef]
- Kawakami, N.; Tsutsumi, A. The Stress Check Program: A new national policy for monitoring and screening psychosocial stress in the workplace in Japan. J. Occup. Health 2016, 58, 1–6. [Google Scholar] [CrossRef]
- Gaskin, D.J.; Richard, P. The Economic Costs of Pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef]
- Wideman, T.H.; Asmundson, G.G.; Smeets, R.J.; Zautra, A.J.; Simmonds, M.J.; Sullivan, M.J.; Haythornthwaite, J.A.; Edwards, R.R. Re-Thinking the Fear Avoidance Model: Toward a Multi-Dimensional Framework of Pain-Related Disability. Pain 2013, 154, 2262–2265. [Google Scholar] [CrossRef] [PubMed]
- Hoogendoorn, W.E.; Van Poppel, M.N.M.; Bongers, P.M.; Koes, B.W.; Bouter, L.M. Systematic Review of Psychosocial Factors at Work and Private Life as Risk Factors for Back Pain. Spine 2000, 25, 2114–2125. [Google Scholar] [CrossRef] [PubMed]
- Fanavoll, R.; Nilsen, T.I.; Holtermann, A.; Mork, P.J. Psychosocial work stress, leisure time physical exercise and the risk of chronic pain in the neck/shoulders: Longitudinal data from the Norwegian HUNT Study. Int. J. Occup. Med. Environ. Health 2016, 29, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Matsudaira, K.; Imano, H.; Kitamura, A.; Iso, H. Influence of work-related psychosocial factors on the prevalence of chronic pain and quality of life in patients with chronic pain. BMJ Open 2016, 6, 010356. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, Y.; Amari, T.; Shimo, S. The relationship between pain psychological factors and job stress in rehabilitation workers with or without chronic pain. Work 2018, 61, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.H.; Andersen, L.L.; Gram, B.; Pedersen, M.T.; Mortensen, O.S.; Zebis, M.K.; Sjøgaard, G. Influence of frequency and duration of strength training for effective management of neck and shoulder pain: A randomised controlled trial. Br. J. Sports Med. 2012, 46, 1004–1010. [Google Scholar] [CrossRef]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [Green Version]
- Fillingim, R.B.; Loeser, J.D.; Baron, R.; Edwards, R.R. Assessment of Chronic Pain: Domains, Methods, and Mechanisms. J. Pain 2016, 17, T10–T20. [Google Scholar] [CrossRef] [Green Version]
- Tsutsumi, A.; Shimazu, A.; Eguchi, H.; Inoue, A.; Kawakami, N. A Japanese Stress Check Program screening tool predicts employee long-term sickness absence: A prospective study. J. Occup. Health 2018, 60, 55–63. [Google Scholar] [CrossRef]
- Hirsh, A.T.; George, S.Z.; Bialosky, J.E.; Robinson, M.E. Fear of pain, pain catastrophizing, and acute pain perception: Relative prediction and timing of assessment. J. Pain 2008, 9, 806–812. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Matsuoka, H.; Sakano, Y. Assessment of cognitive aspect of pain: Development, reliability, and validation of Japanese version of pain catastrophizing scale. Jpn. J. Psychosom. Med. 2007, 47, 95–102. (In Japanese) [Google Scholar]
- Meyers, L.S.; Gamst, G.; Guarino, A. Applied Multivariate Research: Design and Interpretation; SAGE Publishing: Thousand Oaks, CA, USA, 2006; pp. 594–595. [Google Scholar]
- Patrick, D. Analysis of Multiple Dependent Variables; Oxford Scholarship Online, Oxford University Press: Oxford, UK, 2013. [Google Scholar] [CrossRef]
- Collins, S.L.; Moore, R.A.; McQuay, H.J. The visual analogue pain intensity scale: What is moderate pain in millimeters? Pain 1997, 72, 95–97. [Google Scholar] [CrossRef]
- Kliger, M.; Stahl, S.; Haddad, M.; Suzan, E.; Adler, R.; Eisenberg, E. Measuring the Intensity of Chronic Pain: Are the Visual Analogue Scale and the Verbal Rating Scale Interchangeable? Pain Pract. 2015, 15, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Nishiwaki, Y.; Ushida, T.; Toyama, Y. Prevalence and characteristics of chronic musculoskeletal pain in Japan. J. Orthop. Sci. 2011, 16, 424–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.K.; Harris, K.; Hadi, S.; Chow, E. What Should be the Optimal Cut Points for Mild, Moderate, and Severe Pain? J. Palliat. Med. 2007, 10, 1338–1346. [Google Scholar] [CrossRef] [PubMed]
- Kapstad, H.; Hanestad, B.R.; Langeland, N.; Rustøen, T.; Stavem, K. Cutpoints for mild, moderate and severe pain in patients with osteoarthritis of the hip or knee ready for joint replacement surgery. BMC Musculoskelet. Disord. 2008, 9, 55. [Google Scholar] [CrossRef] [PubMed]
- Linton, S.J.; Nicholas, M.K.; MacDonald, S.; Boersma, K.; Bergbom, S.; Maher, C.; Refshauge, K. The role of depression and catastrophizing in musculoskeletal pain. Eur. J. Pain 2011, 15, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Lerman, S.F.; Rudich, Z.; Brill, S.; Shalev, H.; Shahar, G. Longitudinal Associations Between Depression, Anxiety, Pain, and Pain-Related Disability in Chronic Pain Patients. Psychosom. Med. 2015, 77, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.F. The Hospital Anxiety and Depression Scale. Occup. Med. 2014, 64, 393–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfonso, S.P.; Andres Avelino, S.P. Well-Being at Work: A Cross-National Analysis of the Levels and Determinants of Job Satisfaction. J. Socio-Econ. 2000, 29, 517–538. [Google Scholar] [CrossRef]
- Faragher, E.B.; Cass, M.; Cooper, C.L. The relationship between job satisfaction and health: A meta-analysis. Occup. Environ. Med. 2005, 62, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Masselin-Dubois, A.; Attal, N.; Fletcher, D.; Jayr, C.; Albi, A.; Fermanian, J.; Bouhassira, D.; Baudic, S. Are Psychological Predictors of Chronic Postsurgical Pain Dependent on the Surgical Model? A Comparison of Total Knee Arthroplasty and Breast Surgery for Cancer. J. Pain 2013, 14, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Bergsten, E.L.; Mathiassen, S.E.; Vingård, E. Psychosocial Work Factors and Musculoskeletal Pain: A Cross-Sectional Study among Swedish Flight Baggage Handlers. BioMed Res. Int. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halonen, J.I.; Virtanen, M.; Leineweber, C.; Rod, N.H.; Westerlund, H.; Magnusson Hanson, L.L. Associations between onset of effort-reward imbalance at work and onset of musculoskeletal pain: Analyzing observational longitudinal data as pseudo-trials. Pain 2018, 159, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Foppa, I.; Noack, R.H. The relation of self-reported back pain to psychosocial, behavioral, and health-related factors in a working population in Switzerland. Soc. Sci. Med. 1996, 43, 1119–1126. [Google Scholar] [CrossRef]
- Barro, D.; Olinto, M.T.A.; Macagnan, J.B.A.; Henn, R.L.; Pattussi, M.P.; Faoro, M.W.; Garcez, A.D.S.; Paniz, V.M.V. Job characteristics and musculoskeletal pain among shift workers of a poultry processing plant in Southern Brazil. J. Occup. Health 2015, 57, 448–456. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Chronic Pain Group | No Pain Group | |||||
|---|---|---|---|---|---|---|
| n = 97 | n = 68 | p-Value | ||||
| Age | Median (LQ–HQ) years | 34 | (29.5–41) | 34 | (27–37) | 0.11 |
| Gender | Female (%) | 74 | (76) | 43 | (63) | 0.083 |
| Years of service | Median (LQ–HQ) years | 6 | (3–11) | 6 | (3–9) | 0.26 |
| Office Position | None (%) | 81 | (84) | 57 | (84) | 1 |
| Labor contract | Regular workers (%) | 87 | (89) | 61 | (90) | 1 |
| License | Nurse (%) | 46 | (47) | 25 | (37) | |
| None (%) | 12 | (12) | 12 | (17) | ||
| Physical therapist (%) | 9 | (9) | 4 | (6) | ||
| Medical Social worker (%) | 6 | (6) | 2 | (3) | ||
| Pharmacist (%) | 5 | (5) | 5 | (7) | ||
| Occupational therapist (%) | 4 | (4) | 8 | (12) | ||
| Radiologist (%) | 4 | (4) | 1 | (6) | ||
| Other (%) | 12 | (13) | 11 | (12) | ||
| Evaluation Item | Measured Value | |
|---|---|---|
| Visual analog scale | median (LQ–HQ) mm | 48 (30.5–63.5) |
| Brief pain inventory-life | median (LQ–HQ) | 3 (1–5) |
| Brief pain inventory-job | median (LQ–HQ) | 3 (1–5) |
| Pain catastrophizing scale | median (LQ–HQ) | 20 (8.5–27) |
| Rumination | median (LQ–HQ) | 10 (6–13) |
| Helplessness | median (LQ–HQ) | 5 (2–9) |
| Magnification | median (LQ–HQ) | 4 (1–6) |
| Duration of pain | median (LQ–HQ) week | 208 (91–520) |
| Recalled trigger A | not reported (%) | 51 (55) |
| Pain persistence B | always (%) | 21 (22) |
| often (%) | 44 (47) | |
| sometimes (%) | 21 (22) | |
| Consultation history | reported (%) | 51 (53) |
| Surgical history | not reported (%) | 92 (95) |
| Influence at work | reported (%) | 41 (58) |
| Absenteeism | not reported (%) | 84 (87) |
| Pain site C | low back (%) | 59 (61) |
| shoulder (%) | 53 (55) | |
| neck (%) | 29 (30) | |
| head (%) | 11 (11) | |
| knee (%) | 10 (10) | |
| groin (%) | 9 (9) | |
| other (%) | 18 (19) | |
| Chronic Pain Group | No Pain Group | p-Value | |||
|---|---|---|---|---|---|
| Median (LQ–HQ) | Median (LQ–HQ) | ||||
| BJSQ | |||||
| Psychological stress | 40 | (34–47) | 38 | (32–42) | 0.039 A |
| Physical stress | 22 | (18–25) | 16 | (13–19.8) | p < 0.0001 |
| Job stressors | 64 | (56–68) | 63 | (57–67) | 0.83 |
| Support | 26 | (23–30) | 26 | (23–28) | 0.39 |
| Job-life satisfaction | 6 | (5–6) | 6 | (5–7) | 0.043 A |
| HADS | |||||
| Anxiety | 7 | (4–9) | 5 | (3–8) | 0.054 |
| Depression | 6 | (3.5–9) | 4.5 | (2–8) | 0.037 A |
| Dependent Variable | Independent Variable | r2 | Adj-r2 | RMSE | F-Value | B | SE | 95% CI | β | T Value | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||||||
| Psychological stress | 0.57 | 0.56 | 6.78 | 41.7 | p < 0.0001 | |||||||
| 1 Depression | 1.24 | 0.22 | 0.81 | 1.68 | 0.43 | 5.64 | p < 0.0001 | |||||
| 2 Physical stress | 0.74 | 0.15 | 0.45 | 1.04 | 0.37 | 5.01 | p < 0.0001 | |||||
| 3 Interpersonal | 1.34 | 0.37 | 0.60 | 2.08 | 0.25 | 3.58 | 0.0005 | |||||
| 1 Depression | 0.62 | 0.61 | 2.20 | 38.3 | p < 0.0001 | |||||||
| Anxiety | 0.39 | 0.081 | 0.25 | 0.54 | 0.41 | 5.26 | p < 0.0001 | |||||
| Vigor | −0.56 | 0.11 | −0.78 | −0.34 | −0.35 | −4.97 | p < 0.0001 | |||||
| Job-life satisfaction | −0.50 | 0.20 | −0.90 | −0.01 | −0.18 | −2.42 | 0.017 | |||||
| Magnification | 0.17 | 0.08 | 0.01 | 0.34 | 0.16 | 2.14 | 0.035 | |||||
| 2 Physical stress | 0.40 | 0.38 | 4.00 | 20.3 | p < 0.0001 | |||||||
| Depressed mood | 0.43 | 0.11 | 0.20 | 0.65 | 0.35 | 3.76 | 0.0003 | |||||
| Fatigue | 0.59 | 0.18 | 0.23 | 0.96 | 0.30 | 3.25 | 0.0016 | |||||
| Pain intensity (VAS) | 0.06 | 0.02 | 0.02 | 0.10 | 0.26 | 3.17 | 0.002 | |||||
| 3 Interpersonal | 0.28 | 0.26 | 1.65 | 12.0 | p < 0.0001 | |||||||
| Depressed mood | 0.16 | 0.04 | 0.08 | 0.25 | 0.35 | 3.77 | 0.0003 | |||||
| Job control | −0.28 | 0.12 | −0.52 | −0.04 | −0.22 | −2.36 | 0.020 | |||||
| Years of service | −0.06 | 0.03 | −0.11 | −0.01 | −0.20 | −2.23 | 0.028 | |||||
| Dependent Variable | Independent Variable | r2 | Adj-r2 | RMSE | F-Value | B | SE | 95% CI | β | T Value | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||||||
| Psychological stress | 0.63 | 0.60 | 5.90 | 26.3 | p < 0.0001 | |||||||
| 1 Physical stress | 0.75 | 0.14 | 0.48 | 1.03 | 0.45 | 5.45 | p < 0.0001 | |||||
| 2 Anxiety | 0.94 | 0.24 | 0.46 | 1.43 | 0.34 | 3.90 | 0.0002 | |||||
| 3 Quality of work | 1.26 | 0.24 | 0.45 | 2.07 | 0.25 | 3.10 | 0.0029 | |||||
| 4 Job fit | −3.19 | 1.21 | −5.61 | −0.77 | −0.21 | −2.64 | 0.0104 | |||||
| 1 Physical stress | 0.41 | 0.38 | 4.41 | 15.0 | p < 0.0001 | |||||||
| Depressed mood | 0.59 | 0.14 | 0.31 | 0.86 | 0.43 | 4.24 | p < 0.0001 | |||||
| Irritability | 0.78 | 0.29 | 0.21 | 1.36 | 0.28 | 2.72 | 0.0085 | |||||
| Support from coworkers | −0.65 | 0.30 | −1.25 | −0.04 | −0.21 | −2.14 | 0.036 | |||||
| 2 Anxiety | 0.63 | 0.60 | 2.09 | 26.5 | p < 0.0001 | |||||||
| Depression | 0.31 | 0.08 | 0.16 | 0.46 | 0.37 | 4.18 | p < 0.0001 | |||||
| Feelings of anxiety | 0.53 | 0.14 | 0.25 | 0.82 | 0.33 | 3.75 | 0.0004 | |||||
| Vigor | −0.43 | 0.14 | −0.72 | −0.14 | −0.28 | −2.98 | 0.0041 | |||||
| Work environment | 0.92 | 0.37 | 0.19 | 1.65 | 0.19 | 2.51 | 0.015 | |||||
| 3 Quality of work | 0.51 | 0.47 | 1.36 | 16.1 | p < 0.0001 | |||||||
| Quantity of work | 0.32 | 0.10 | 0.12 | 0.52 | 0.34 | 3.20 | 0.0022 | |||||
| Feelings of anxiety | 0.27 | 0.09 | 0.09 | 0.44 | 0.30 | 3.02 | 0.0036 | |||||
| Physical burden | 0.59 | 0.21 | 0.17 | 1.00 | 0.28 | 2.83 | 0.0063 | |||||
| Support from family and friends | 0.18 | 0.09 | 0.004 | 0.36 | 0.19 | 2.05 | 0.044 | |||||
| 4 Job fit | 0.52 | 0.50 | 0.43 | 35.1 | p < 0.0001 | |||||||
| Job value | 0.71 | 0.10 | 0.51 | 0.91 | 0.62 | 7.15 | p < 0.0001 | |||||
| Job-life satisfaction | 0.17 | 0.05 | 0.07 | 0.26 | 0.29 | 3.38 | 0.0012 | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakamoto, Y.; Oka, T.; Amari, T.; Shimo, S. Factors Affecting Psychological Stress in Healthcare Workers with and without Chronic Pain: A Cross-Sectional Study Using Multiple Regression Analysis. Medicina 2019, 55, 652. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100652
Sakamoto Y, Oka T, Amari T, Shimo S. Factors Affecting Psychological Stress in Healthcare Workers with and without Chronic Pain: A Cross-Sectional Study Using Multiple Regression Analysis. Medicina. 2019; 55(10):652. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100652
Chicago/Turabian StyleSakamoto, Yuta, Takeru Oka, Takashi Amari, and Satoshi Shimo. 2019. "Factors Affecting Psychological Stress in Healthcare Workers with and without Chronic Pain: A Cross-Sectional Study Using Multiple Regression Analysis" Medicina 55, no. 10: 652. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100652