Prevention of Pathological Fracture of the Proximal Femur: A Systematic Review of Surgical and Percutaneous Image-Guided Techniques Used in Interventional Oncology



Abstract
:1. Introduction
2. Materials and Methods
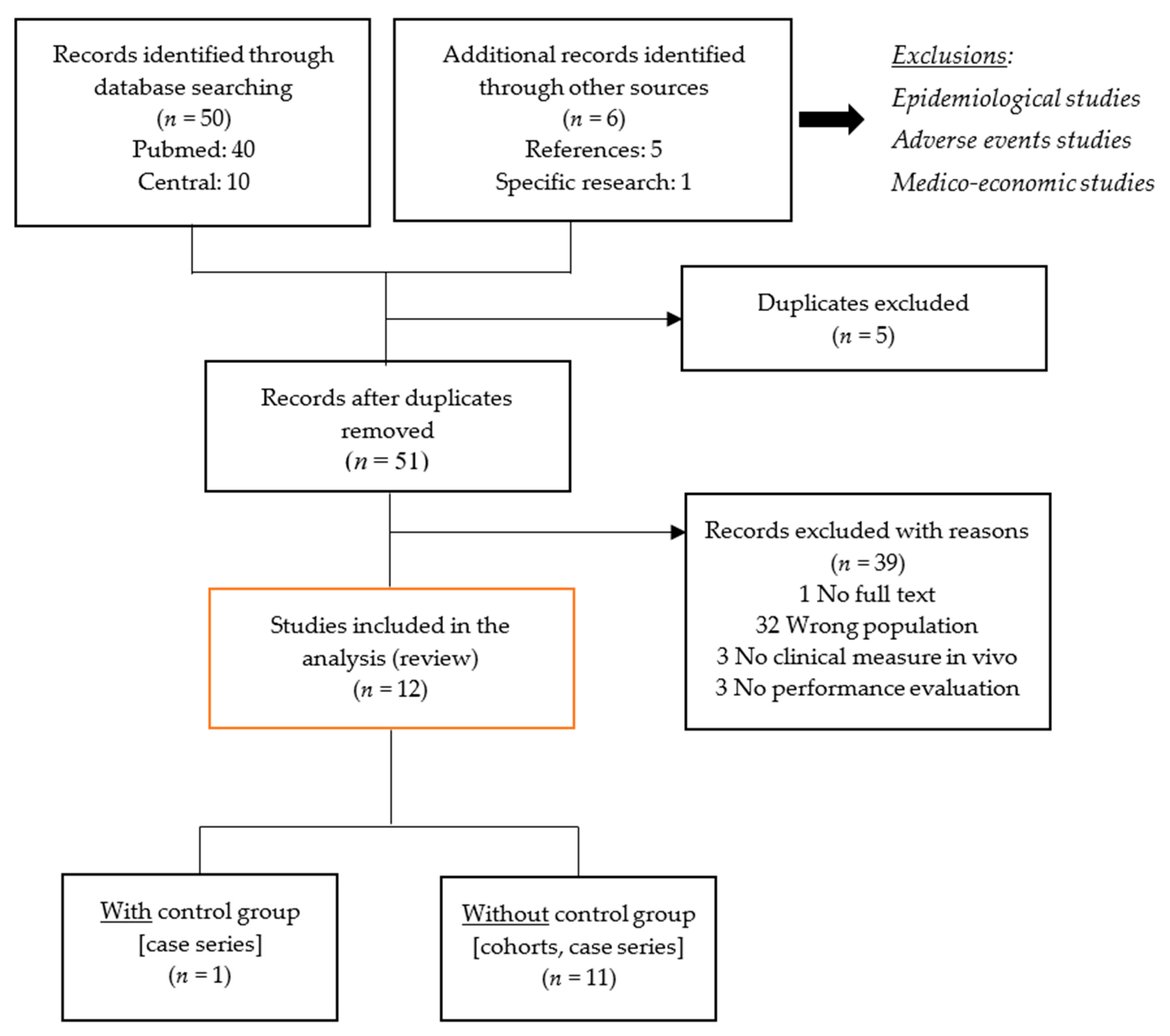
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
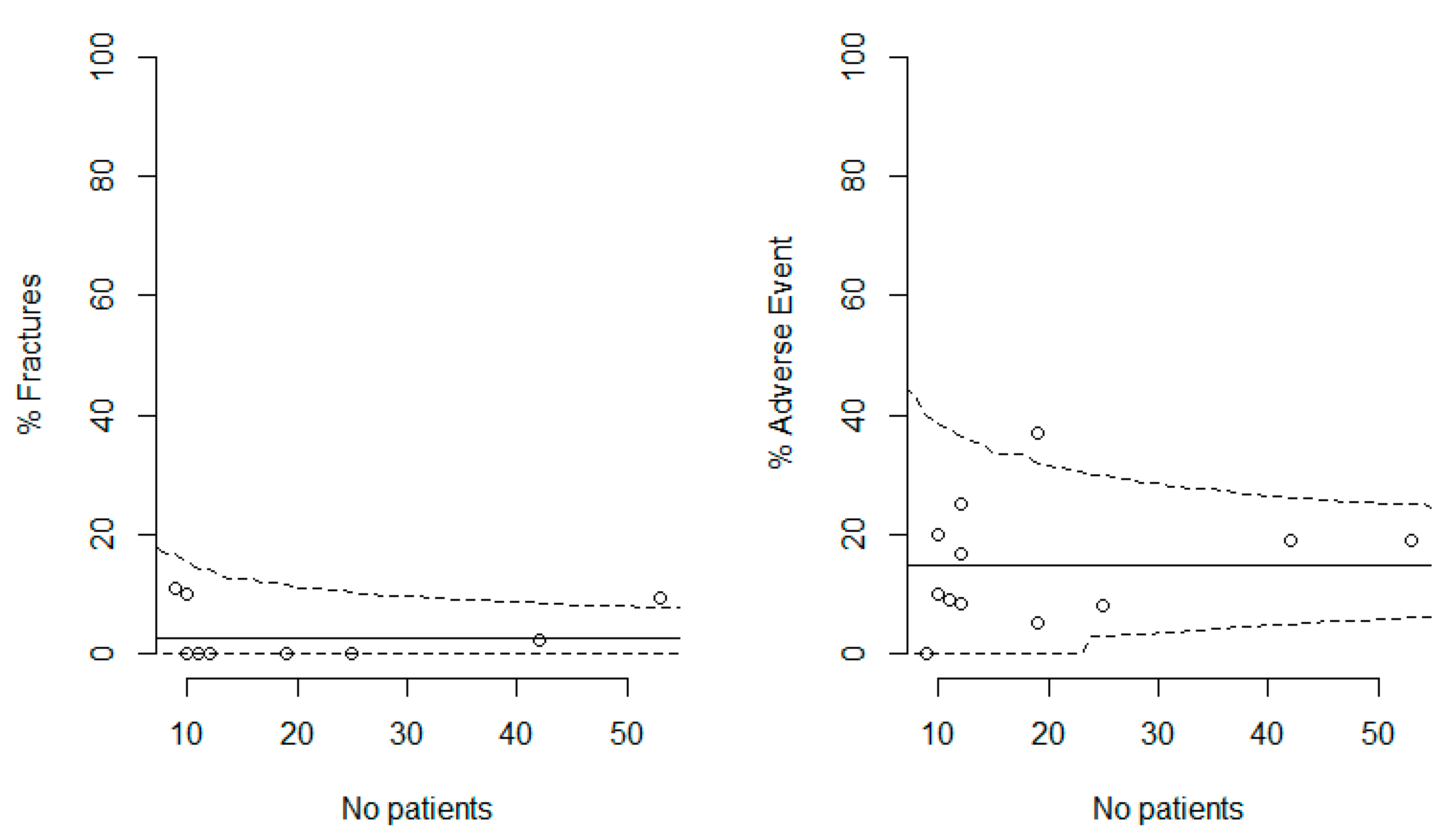
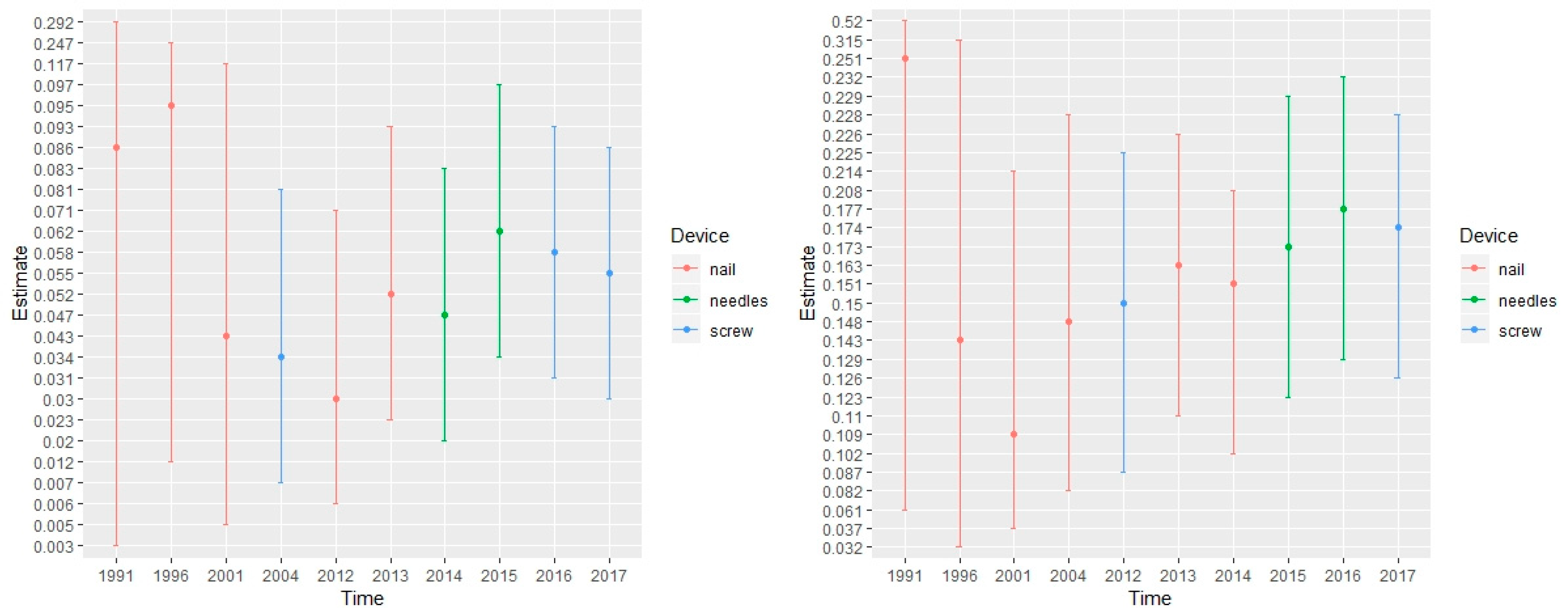
2.3. Systematic Review and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaneko, T.S.; Skinner, H.B.; Keyak, J.H. Lytic lesions in the femoral neck: Importance of location and evaluation of a novel minimally invasive repair technique. J. Orthop. Res. 2008, 26, 1127–1132. [Google Scholar] [CrossRef] [PubMed]
- Ashford, R.U.; Hanna, S.A.; Park, D.H.; Pollock, R.C.; Skinner, J.A.; Briggs, T.W.; Cannon, S.R. Proximal femoral replacements for metastatic bone disease: Financial implications for sarcoma units. Int. Orthop. 2010, 34, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Mundy, G.R. Metastasis to bone: Causes, consequences and therapeutic opportunities. Nat. Rev. Cancer 2002, 2, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Schneiderbauer, M.M.; Von Knoch, M.; Schleck, C.D.; Harmsen, W.S.; Sim, F.H.; Scully, S.P. Patient survival after hip arthroplasty for metastatic disease of the hip. J. Bone Jt. Surg. Am. Vol. 2004, 86, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Taylor, A.J.; Matthews, R.S.; Ray, M.N.; Becker, D.J.; Gary, L.C.; Kilgore, M.L.; Morrisey, M.A.; Saag, K.G.; Warriner, A.; et al. “Pathologic” fractures: Should these be included in epidemiologic studies of osteoporotic fractures? Osteoporos. Int. 2009, 20, 1969–1972. [Google Scholar] [CrossRef]
- Kelekis, A.; Filippiadis, D.; Anselmetti, G.; Brountzos, E.; Mavrogenis, A.; Papagelopoulos, P.; Kelekis, N.; Martin, J.B. Percutaneous Augmented Peripheral Osteoplasty in Long Bones of Oncologic Patients for Pain Reduction and Prevention of Impeding Pathologic Fracture: The Rebar Concept. Cardiovasc. Intervent. Radiol. 2016, 39, 90–96. [Google Scholar] [CrossRef]
- Parker, M.J.; Khan, A.Z.; Rowlands, T.K. Survival after Pathological Fractures of the Proximal Femur. HIP Int. 2011, 21, 526–530. [Google Scholar] [CrossRef]
- Mavrovi, E.; Pialat, J.-B.; Beji, H.; Kalenderian, A.-C.; Vaz, G.; Richioud, B. Percutaneous osteosynthesis and cementoplasty for stabilization of malignant pathologic fractures of the proximal femur. Diagn. Interv. Imaging 2017, 98, 483–489. [Google Scholar] [CrossRef]
- Jawad, M.U.; Scully, S.P. In Brief: Classifications in Brief: Mirels’ Classification: Metastatic Disease in Long Bones and Impending Pathologic Fracture. Clin. Orthop. Relat. Res. 2010, 468, 2825–2827. [Google Scholar] [CrossRef]
- Cornelis, F.H.; Deschamps, F. Augmented osteoplasty for proximal femur consolidation in cancer patients: Biomechanical considerations and techniques. Diagn. Interv. Imaging 2017, 98, 645–650. [Google Scholar] [CrossRef]
- Cazzato, R.L.; Garnon, J.; Tsoumakidou, G.; Koch, G.; Palussière, J.; Gangi, A.; Buy, X. Percutaneous image-guided screws meditated osteosynthesis of impeding and pathological/insufficiency fractures of the femoral neck in non-surgical cancer patients. Eur. J. Radiol. 2017, 90, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 4 June 2019).
- Biau, D.J.; Boulezaz, S.; Casabianca, L.; Hamadouche, M.; Anract, P.; Chevret, S. Using Bayesian statistics to estimate the likelihood a new trial will demonstrate the efficacy of a new treatment. BMC Med. Res. Methodol. 2017, 17, 128. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, F.H.; Tselikas, L.; Carteret, T.; Lapuyade, B.; De Baere, T.; Cabane, V.; Rodrigues, L.; Maas, C.; Deschamps, F. A Novel Implant for the Prophylactic Treatment of Impending Pathological Fractures of the Proximal Femur: Results from a Prospective, First-in-Man Study. Cardiovasc. Interv. Radiol. 2017, 40, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Shemesh, S.; Kosashvili, Y.; Sidon, E.; Yaari, L.; Cohen, N.; Velkes, S. Intramedullary nailing without curettage and cement augmentation for the treatment of impending and complete pathological fractures of the proximal or midshaft femur. Acta Orthop. Belg. 2014, 80, 144–150. [Google Scholar]
- Alvi, H.M.; Damron, T.A. Prophylactic stabilization for bone metastases, myeloma, or lymphoma: Do we need to protect the entire bone? Clin. Orthop. Relat. Res. 2013, 47, 706–714. [Google Scholar] [CrossRef]
- Moholkar, K.; Mohan, R.; Grigoris, P. The Long Gamma Nail for stabilisation of existing and impending pathological fractures of the femur: An analysis of 48 cases. Acta Orthop. Belg. 2004, 70, 429–434. [Google Scholar]
- Edwards, S.; Pandit, H.; Clarke, H.; Pandit, H. The treatment of impending and existing pathological femoral fractures using the long gamma nail. Injury 2001, 32, 299–306. [Google Scholar] [CrossRef]
- Voggenreiter, G.; Assenmacher, S.; Klaes, W.; Schmit-Neuerburg, K.-P. Pathological fractures of the proximal femur with impending shaft fractures treated by THR and cemented intramedullary nailing. J. Bone Jt. Surg. Br. Vol. 1996, 78, 400–403. [Google Scholar] [CrossRef]
- Weikert, D.; Schwartz, H. Intramedullary nailing for impending pathological subtrochanteric fractures. J. Bone Jt. Surg. Br. Vol. 1991, 73, 668–670. [Google Scholar] [CrossRef]
- Deschamps, F.; Farouil, G.; Hakime, A.; Teriitehau, C.; Barah, A.; de Baere, T. Percutaneous stabilization of impending pathological fracture of the proximal femur. Cardiovasc. Intervent. Radiol. 2012, 35, 1428–1432. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.-H.; He, C.-J.; Wu, C.-G.; Li, Y.-D.; Gu, Y.-F.; Wang, T.; Xiao, Q.-P.; Li, M.-H. Comparison of Percutaneous Cementoplasty with and Without Interventional Internal Fixation for Impending Malignant Pathological Fracture of the Proximal Femur. Cardiovasc. Interv. Radiol. 2015, 39, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Pons-Tostivint, E.; Latouche, A.; Vaflard, P.; Ricci, F.; Loirat, D.; Hescot, S.; Sablin, M.-P.; Rouzier, R.; Kamal, M.; Morel, C.; et al. Comparative Analysis of Durable Responses on Immune Checkpoint Inhibitors Versus Other Systemic Therapies: A Pooled Analysis of Phase III Trials. JCO Precis. Oncol. 2019, 3, 1–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Ref | Study | NOS stars (out of 9) | Medical Device | Cement | Number of Patients | % Man | Mean Age | Mean Follow-up | % Fracture | % AEs | % SAEs |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [15] | Cornelis 2017 | 6 | Implant | Yes | 10 | 67 | 62 | 0.65 | 10 | 10 | NK |
| [16] | Shemesh 2014 | 6 | Nail | No | 19 | 38.1 | 62 | 0.8 | 0 | 5.3 | NK |
| [17] | Alvi 2013 | 6 | Nail | No | 53 | 42 | 60 | 0.9 | 9.4 | 18.9 | 9.4 |
| [18] | Moholkar 2004 | 6 | Nail | No | 42 | 28.6 | 66 | 1.1 | 2.4 | 19 | 9.5 |
| [19] | Edwards 2001 | 6 | Nail | No | 25 | 44 | 68 | 1.5 | 0 | 8 | 8 |
| [20] | Voggenreiter 1996 | 6 | Nail | Yes | 9 | 22 | 59 | 0.7 | 11.1 | 0 | 22.2 |
| [21] | Weikert 1991 | 6 | Nail | No | 10 | NK | 67 | 0.7 | 0 | 20 | NK |
| [11] | Cazzato 2017 | 5 | Screw | Yes | 11 | 54.5 | 63.7 | 0.17 | 0 | 9.1 | 0 |
| [22] | Deschamps 2012 | 6 | Screw | Yes | 12 | 25 | 55 | 0.64 | 0 | 16.7 | 0 |
| [6] | Kelekis 2016 | 6 | Needles | Yes | 12 | 83 | NK | 1.35 | 0 | 25 | 0 |
| [23] | Tian 2015 | 8 | Needles | Yes | 19 | 47.4 | 58.5 | 0.75 | 0 | 17.5 | 12.5 |
| [8] | Mavrovi 2017 | 6 | Screw | Yes | 12 | 75 | 56 | 1.05 | 0 | 8.3 | 0 |
| Endpoints | OR * (95% CI) | p Value |
|---|---|---|
| Fracture | ||
| % male | 0.96 (0.89;1.04) | 0.32 |
| Mean Age | 1.02 (0.76;1.37) | 0.91 |
| Nail | 1.67 (0.15;18.9) | 0.68 |
| Cement | 0.60 (0.05;6.79) | 0.68 |
| Nb patients | 1.08 (0.97;1.21) | 0.16 |
| Adverse Event | ||
| % male | 0.98 (0.92;1.05) | 0.59 |
| Mean Age | 1.12 (0.83;1.52) | 0.46 |
| Nail | 5.33 (0.38;75.8) | 0.22 |
| Cement | 0.19 (0.01;2.66) | 0.22 |
| Nb patients | 1.17 (0.90;1.55) | 0.24 |
| Severe Adverse Event | ||
| % male | 0.93 (0.85;1.02) | 0.13 |
| Mean Age | 1.08 (0.81;1.45) | 0.59 |
| Nail | 3.75 (0.33;42.5) | 0.29 |
| Cement | 0.27 (0.02;3.02) | 0.29 |
| Nb patients | 1.25 (0.93;1.69) | 0.14 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, L.; Cornelis, F.H.; Reina, N.; Chevret, S. Prevention of Pathological Fracture of the Proximal Femur: A Systematic Review of Surgical and Percutaneous Image-Guided Techniques Used in Interventional Oncology. Medicina 2019, 55, 755. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55120755
Rodrigues L, Cornelis FH, Reina N, Chevret S. Prevention of Pathological Fracture of the Proximal Femur: A Systematic Review of Surgical and Percutaneous Image-Guided Techniques Used in Interventional Oncology. Medicina. 2019; 55(12):755. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55120755
Chicago/Turabian StyleRodrigues, Laëtitia, François H. Cornelis, Nicolas Reina, and Sylvie Chevret. 2019. "Prevention of Pathological Fracture of the Proximal Femur: A Systematic Review of Surgical and Percutaneous Image-Guided Techniques Used in Interventional Oncology" Medicina 55, no. 12: 755. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55120755