Clinical Value of Presepsin in Comparison to hsCRP as a Monitoring and Early Prognostic Marker for Sepsis in Critically Ill Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Specimen Collection and Processing
2.4. Specimen Examination
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Studied Patients
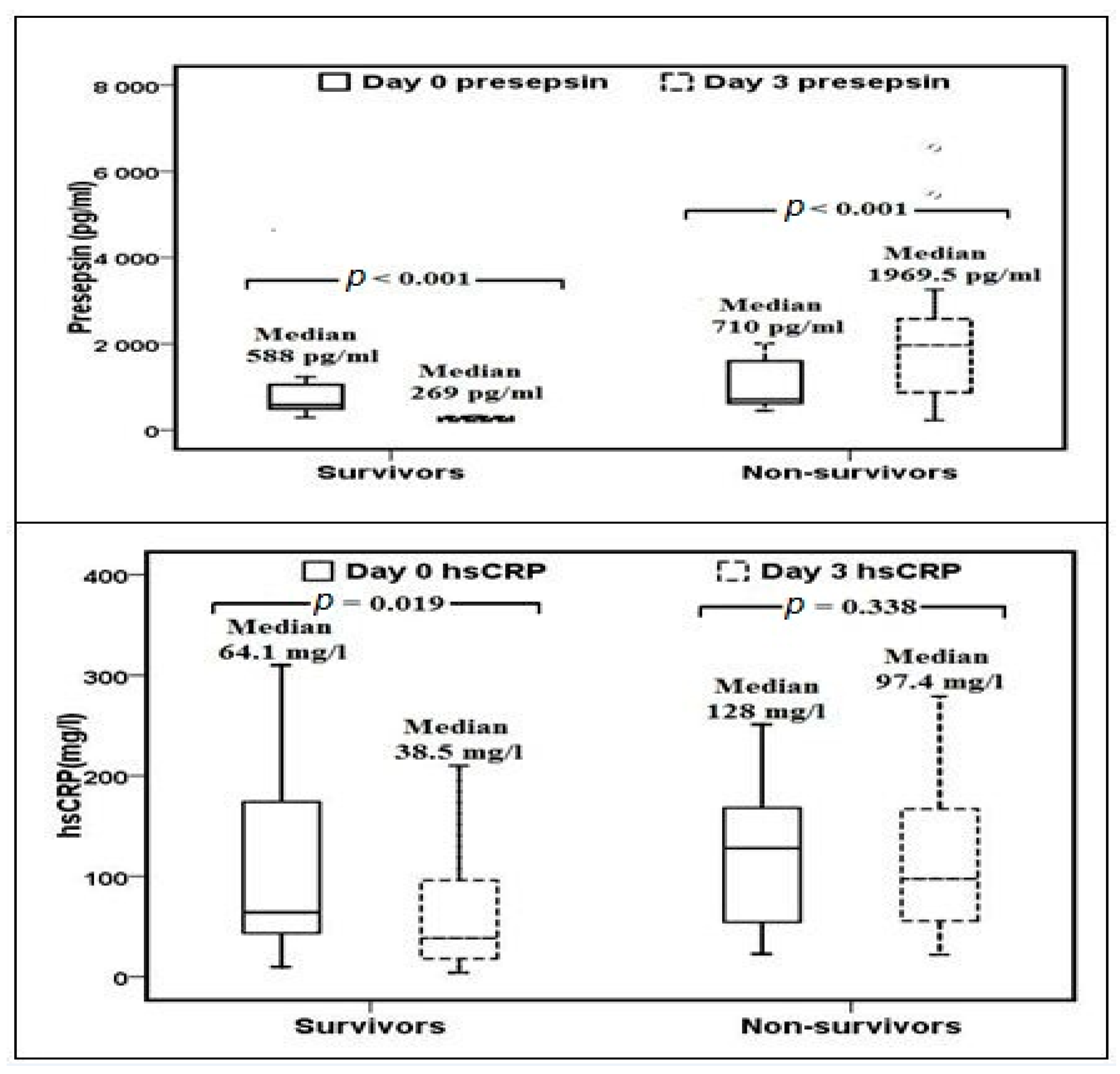
3.2. Assessment of Presepsin and hsCRP in Critically Ill Septic Patients
3.3. Determination of Risk Factors for Sepsis-Relatedin-Hospital Mortality
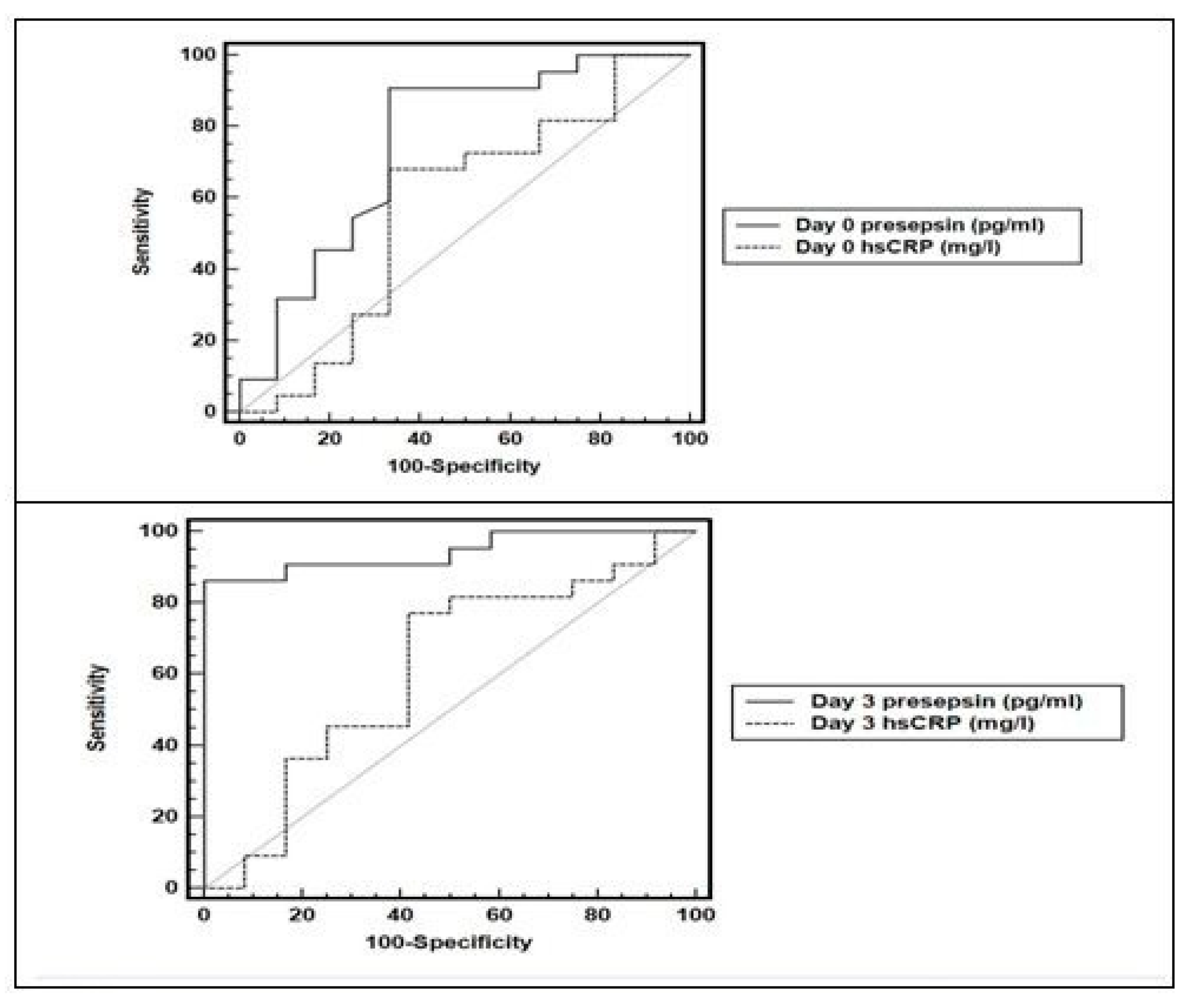
3.4. Comparison of Predictive Accuracy and Determination of the Best Cut-Off Value of Presepsin and hsCRP for Risk of Sepsis-Related in-Hospital Mortality
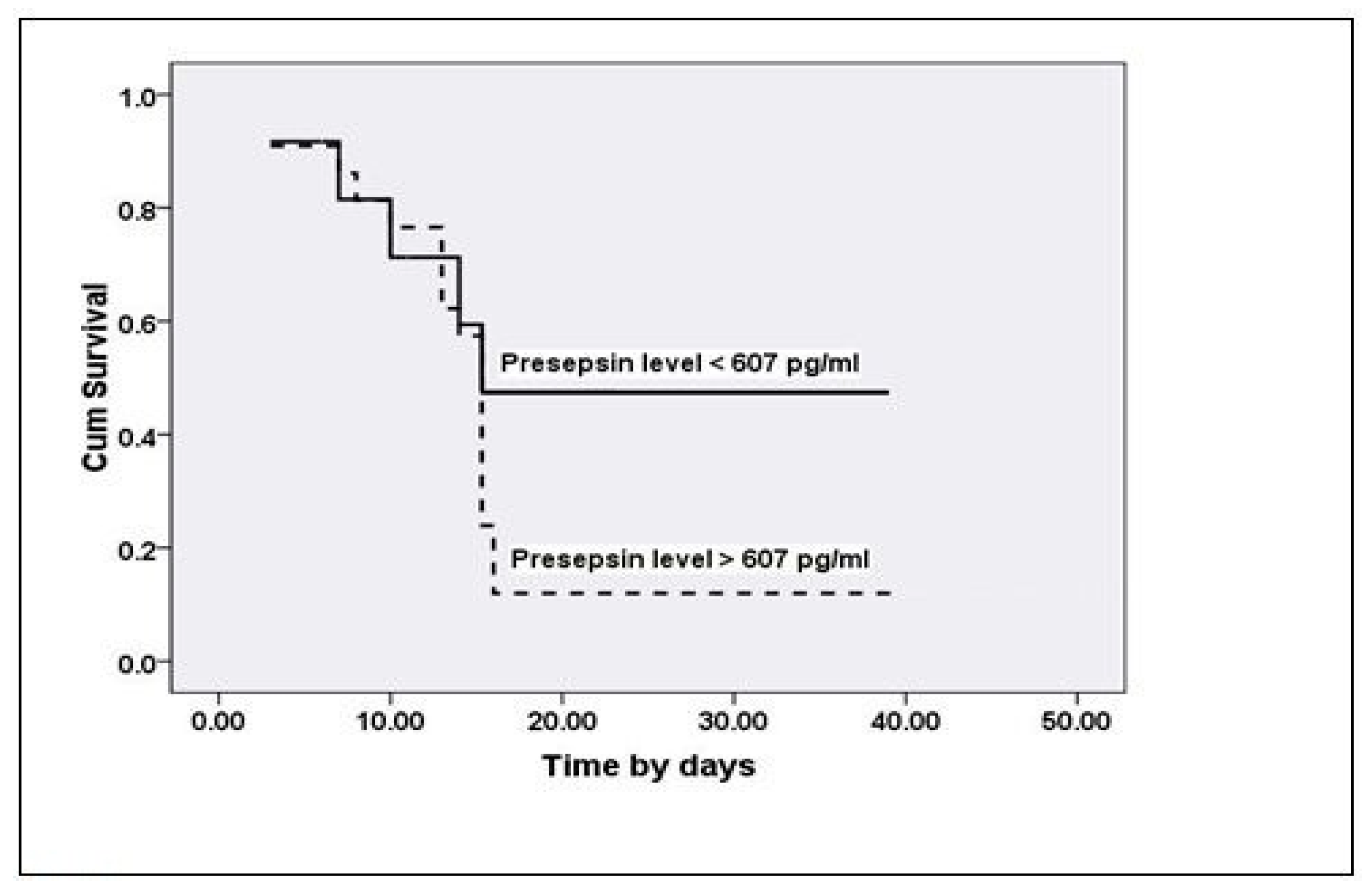
3.5. Determination of the Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Sirio, C.A.; Clermont, G.; Bion, J. International comparisons of critical care outcome and resource consumption. Crit. Care Clin. 1997, 13, 389–407. [Google Scholar] [CrossRef]
- Linde-Zwirble, W.T.; Angus, D.C. Severe sepsis epidemiology: Sampling, selection, and society. Crit. Care 2004, 8, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Kaukonen, K.M.; Bailey, M.; Suzuki, S.; Pilcher, D.; Bellomo, R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA 2014, 311, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Dombrovskiy, V.Y.; Martin, A.A.; Sunderram, J.; Paz, H.L. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: A trend analysis from 1993 to 2003. Crit. Care Med. 2007, 35, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Kumar, G.; Kumar, N.; Taneja, A.; Kaleekal, T.; Tarima, S.; McGinley, E.; Jimenez, E.; Mohan, A.; Khan, R.A.; Whittle, J.; et al. Nationwide trends of severe sepsis in the 21st century (2000–2007). Chest 2011, 140, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef]
- Levy, M.M.; Dellinger, R.P.; Townsend, S.R.; Linde-Zwirble, W.T.; Marshall, J.C.; Bion, J.; Schorr, C.; Artigas, A.; Ramsay, G.; Beale, R.; et al. The Surviving Sepsis Campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010, 36, 222–231. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Melot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef]
- Machado, F.R.; Assunção, M.S.; Cavalcanti, A.B.; Japiassú, A.M.; Azevedo, L.C.; Oliveira, M.C. Getting a consensus: Advantages and disadvantages of Sepsis 3 in the context of middle-income settings. Rev. Bras. Ter. Intensiva 2016, 28, 361–365. [Google Scholar] [CrossRef]
- Wacker, C.; Prkno, A.; Brunkhorst, F.M.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. Procalcitonin as a diagnostic marker for sepsis: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 426–435. [Google Scholar] [CrossRef]
- Kibe, S.; Adams, K.; Barlow, G. Diagnostic and prognostic biomarkers of sepsis in critical care. J. Antimicrob. Chemother. 2011, 66 (Suppl. 2), 33–40. [Google Scholar] [CrossRef]
- Au-Yong, A. Towards evidence-based emergency medicine: Best BETs from the Manchester Royal Infirmary. BET 2: C-reactive protein in the diagnosis of bacteraemia. Emerg. Med. J. 2012, 29, 423–424. [Google Scholar]
- Shozushima, T.; Takahashi, G.; Matsumoto, N.; Kojika, M.; Okamura, Y.; Endo, S. Usefulness of presepsin (sCD14-ST) measurements as a marker for the diagnosis and severity of sepsis that satisfied diagnostic criteria of systemic inflammatory response syndrome. J. Infect. Chemother. 2011, 17, 764–769. [Google Scholar] [CrossRef]
- Memar, M.Y.; Baghi, H.B. Presepsin: A promising biomarker for the detection of bacterial infections. Biomed. Pharmacother. 2019, 111, 649–656. [Google Scholar] [CrossRef]
- Bone, R.; Balk, R.; Cerra, F.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM consensus conference committee. American college of chest physicians/society of critical care medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef]
- Chatterjee, S.; Bhattacharya, M.; Todi, S.K. Epidemiology of Adult-population Sepsis in India: A Single Center 5 Year Experience. Indian J. Crit. Care Med. 2017, 21, 573–577. [Google Scholar]
- Liu, B.; Chen, Y.X.; Yin, Q.; Zhao, Y.Z.; Li, C.S. Diagnostic value and prognostic evaluation of presepsin for sepsis in an emergency department. Crit. Care 2013, 17, R244. [Google Scholar] [CrossRef]
- Masson, S.; Caironi, P.; Fanizza, C.; Thomae, R.; Bernasconi, R.; Noto, A.; Oggioni, R.; Pasetti, G.S.; Romero, M.; Tognoni, G.; et al. Circulating presepsin (soluble CD14 subtype) as a marker of host response in patients with severe sepsis or septic shock: Data from the multicenter, randomized ALBIOS trial. Intensive Care Med. 2015, 41, 12–20. [Google Scholar] [CrossRef]
- Masson, S.; Caironi, P.; Spanuth, E.; Panigada, M.; Sangiorgi, G.; Fumagalli, R.; Mauri, T.; Isgrò, S.; Fanizza, C.; et al. Presepsin (soluble CD14 subtype) and procalcitonin levels for mortality prediction in sepsis: Data from the albumin Italian outcome sepsis trial. Crit. Care 2014, 18, R6. [Google Scholar] [CrossRef]
- Klouche, K.; Cristol, J.; Devin, J.; Gilles, V.; Kuster, N.; Larcher, R.; Amigues, L.; Corne, P.; Jonquet, O.; Dupuy, A.M. Diagnostic and prognostic value of soluble CD14 subtype (Presepsin) for sepsis and community acquired pneumonia in ICU patients. Ann. Intensive Care 2016, 6, 59. [Google Scholar] [CrossRef]
- Romualdo, L.G.; Torrella, P.E.; González, M.V.; Sánchez, R.J.; Holgado, A.H.; Freire, A.O.; Acebes, S.R.; Otón, M.D. Diagnostic accuracy of presepsin (soluble CD14 subtype) for prediction of bacteremia in patients with systemic inflammatory response syndrome in the Emergency Department. Clin. Biochem. 2014, 47, 505–508. [Google Scholar] [CrossRef]
- Spanuth, E.; Ebelt, H.; Ivandic, B.T.; Werdan, K. Diagnostic and prognostic value of presepsin (soluble CD14 subtype) in emergency patients with early sepsis using the new assay PATHFAST Presepsin. In Advances in Clinical Chemistry and Laboratory Medicine; Renz, H., Tauber, R., Eds.; De Gruyter: Berlin, Germany, 2012; pp. 129–133. [Google Scholar]
- Limongi, D.; D’Agostini, C.; Ciotti, M. New sepsis biomarkers. Asian Pac. J. Trop. Biomed. 2016, 6, 516–519. [Google Scholar] [CrossRef]
- Nakamura, Y.; Hoshino, K.; Kiyomi, F.; Kawano, Y.; Mizunuma, M.; Tanaka, J.; Nishida, T.; Ishikura, H. Comparison of accuracy of presepsin and procalcitonin concentrations in diagnosing sepsis in patients with and without acute kidney injury. Clin. Chim. Acta 2018. [Google Scholar] [CrossRef]
- Behnes, M.; Bertsch, T.; Lepiorz, D.; Trinkmann, F.; Brueckmann, M.; Borggrefe, M.; Hoffmann, U. Diagnostic and prognostic utility of soluble CD14 subtype (presepsin) for severe sepsis and septic shock during the first week of intensive care treatment. Crit. Care 2014, 18, 507. [Google Scholar] [CrossRef]
- Ishikura, H.; Nishida, T.; Murai, A.; Nakamura, Y.; Irie, Y.; Tanaka, J.; Umemura, T. New diagnostic strategy for sepsis-induced disseminated intravascular coagulation: A prospective single-center observational study. Crit. Care 2014, 18, R19. [Google Scholar] [CrossRef]
- Ho, K.M.; Lee, K.Y.; Dobb, G.J.; Webb, S.A. C-reactive protein concentration as a predictor of in-hospital mortality after ICU discharge: A prospective cohort study. Intensive Care Med. 2008, 34, 481–487. [Google Scholar] [CrossRef]
- Thiem, U.; Niklaus, D.; Sehlhoff, B.; Stückle, C.; Heppner, H.J.; Endres, H.G.; Pientka, L. C-reactive protein, severity of pneumonia and mortality in elderly, hospitalised patients with community-acquired pneumonia. Age Ageing 2009, 38, 693–697. [Google Scholar] [CrossRef] [Green Version]
- Endo, S.; Suzuki, Y.; Takahashi, G.; Shozushima, T.; Ishikura, H.; Murai, A.; Nishida, T.; Irie, Y.; Miura, M.; Iguchi, H.; et al. Presepsin as a powerful monitoring tool for the prognosis and treatment of sepsis: A multicenter prospective study. J. Infect. Chemother. 2014, 20, 30–34. [Google Scholar] [CrossRef]
- Silvestre, J.; Povoa, P.; Coelho, L.; Almeida, E.; Moreira, P.; Fernandes, A.; Mealha, R.; Sabino, H. Is C-reactive protein a good prognostic marker in septic patients? Intensive Care Med. 2009, 35, 909–913. [Google Scholar] [CrossRef]
- Hogarth, M.B.; Gallimore, R.; Savage, P.; Palmer, A.J.; Starr, J.M.; Bulpitt, C.J.; Pepys, M.B. Acute phase proteins, C-reactive protein and serum amyloid A protein, as prognostic markers in the elderly inpatient. Age Ageing 1997, 26, 153–158. [Google Scholar] [CrossRef] [Green Version]
- El-Shafiea, M.E.; Taemaa, K.M.; El-Hallaga, M.M.; Kandeel, A.M.A. Role of presepsin compared to C-reactive protein in sepsis diagnosis and prognostication. Egypt. J. Crit. Care Med. 2017, 5, 1–12. [Google Scholar] [CrossRef]
- Lobo, S.M.; Lobo, F.R.; Bota, D.P.; Lopes-Ferreira, F.; Soliman, H.M.; Mélot, C.; Vincent, J.L. C-reactive protein levels correlate with mortality and organ failure in critically ill patients. Chest 2003, 123, 2043–2049. [Google Scholar] [CrossRef]
- Castelli, G.P.; Pognani, C.; Meisner, M.; Stuani, A.; Bellomi, D.; Sgarbi, L. Procalcitonin and C-reactive protein during systemic inflammatory response syndrome, sepsis and organ dysfunction. Crit. Care 2004, 8, R234–R242. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 68) | Survivors (n = 24) | Non-Survivor (n = 44) | p | |
|---|---|---|---|---|
| Age (years; Mean ± SD) | 35.7 ± 15.1 | 34.7 ± 15.3 | 36.3 ± 15.2 | 0.771 |
| Sex (M/F) | 48/20 (70.6/29.4%) | 20/4 (83.3/16.7%) | 28/16 (63.6/36.4%) | 0.228 |
| SOFA score | 7.6 ± 3.1 | 6.3 ± 3.2 | 8.9 ± 2.9 | 0.015 |
| Type of organisms (Gram+/−ve) | 22/46 (32.4/67.6%) | 0/24 (0/100%) | 22/22 (50/50%) | 0.05 |
| Glucose (mmol/L; mean ± SD) | 6.9 ± 2 | 7.2 ± 2.2 | 6.8 ± 1.9 | 0.581 |
| Urea (mmol/L; median, range) | 6.1 (1.3–30.4) | 8.2 (4.2–16.1) | 5.8 (1.3–30.4) | 0.118 |
| Creatinine (µmol/L; median, range) | 84.5 (35.9–663.8) | 103.5 (35.9–296) | 378.8 (37–663.8) | 0.03 |
| Albumin (g/dL; mean ± SD) | 2.6 ± 0.7 | 2.7 ± 0.7 | 2.6 ± 0.7 | 0.556 |
| Total bilirubin (µmol/L; median, range) | 10.7 (3–85) | 9.4 (3–33.5) | 21.4 (8.5–85) | 0.04 |
| AST (U/L; median, range) | 102 (19–989) | 122.5 (31–597) | 84.5 (19–989) | 0.261 |
| ALT (U/L; median, range) | 58.5 (14–298) | 111.5 (16–298) | 49.5 (14–194) | 0.094 |
| INR | 1.6 ± 0.2 | 1.2 ± 0.2 | 1.8 ± 0.2 | 0.400 |
| Hemoglobin (g/dL; mean ± SD) | 10 ± 2.3 | 10.2 ± 1.6 | 9.9 ± 2.5 | 0.736 |
| Platelets (×109/L; median, range) | 193 (20–625) | 196.5 (53–625) | 187 (20–275) | 0.548 |
| WBC (×109/L; mean ± SD) | 12.9 ± 5.6 | 10.8 ± 4.7 | 15 ± 6.4 | 0.03 |
| WBC at follow-up (×109/L; mean ± SD) | 11 ± 4.9 | 10.2 ± 3.9 | 11.5 ± 5.4 | 0.462 |
| hsCRP (mg/L; median, range) | 101.5 (9.8–384) | 64.1 (9.8–384) | 128 (22.8–380) | 0.488 |
| hsCRP at follow-up (mg/L; median, range) | 66 (4–279) | 38.5 (4–210) | 97.4 (22–279) | 0.015 |
| Presepsin (pg/mL; median, range) | 690 (294–4965) | 588 (294–4965) | 810.5 (453–4879) | 0.03 |
| Presepsin at follow-up (pg/mL; median, range) | 721 (210–6540) | 269 (210–323) | 1969.5 (232–6540) | <0.001 |
| Odds Ratio (95% CI) | p | |
|---|---|---|
| Type of organisms (Gram+/−ve) | 0.9 (0.8–1.03) | 0.342 |
| SOFA score | 1.3 (0.8–2) | 0.03 |
| Serum creatinine | 1 (0.8–1.4) | 0.499 |
| Serum total bilirubin | 1.1 (0.9–1.9) | 0.549 |
| WBCs | 0.7 (0.4–1.1) | 0.683 |
| hsCRP | 1.03 (1–1.1) | 0.092 |
| Presepsin | 1 (0.9–1.02) | 0.04 |
| AUC 95% CI | SEN (%) | SPE (%) | PPV (%) | NPV (%) | +LR | −LR | Accuracy (%) | |
|---|---|---|---|---|---|---|---|---|
| Day 0 Presepsin (>607 pg/mL) | 0.824 (0.775–0.955) | 86.4 | 89.6 | 93.8 | 78.2 | 8.3 | 0.2 | 87.5 |
| Day 3 Presepsin (>1323 pg/mL) | 0.943 (0.806–0.992) | 90.1 | 100 | 100 | 89.8 | 0.1 | 93.6 | |
| Day 0 hsCRP (>58 mg/L) | 0.576 (0.395–0.743) | 72.7 | 50 | 72.7 | 50 | 1.5 | 0.5 | 64.7 |
| Day 3 hsCRP (>67 mg/L) | 0.737 (0.558–0.872) | 54.6 | 75 | 80 | 47.4 | 2.2 | 0.6 | 61.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassan, E.A.; Abdel Rehim, A.S.; Ahmed, A.O.; Abdullahtif, H.; Attia, A. Clinical Value of Presepsin in Comparison to hsCRP as a Monitoring and Early Prognostic Marker for Sepsis in Critically Ill Patients. Medicina 2019, 55, 36. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020036
Hassan EA, Abdel Rehim AS, Ahmed AO, Abdullahtif H, Attia A. Clinical Value of Presepsin in Comparison to hsCRP as a Monitoring and Early Prognostic Marker for Sepsis in Critically Ill Patients. Medicina. 2019; 55(2):36. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020036
Chicago/Turabian StyleHassan, Elham A., Abeer S. Abdel Rehim, Asmaa O. Ahmed, Hanan Abdullahtif, and Alaa Attia. 2019. "Clinical Value of Presepsin in Comparison to hsCRP as a Monitoring and Early Prognostic Marker for Sepsis in Critically Ill Patients" Medicina 55, no. 2: 36. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020036