Comparison of 30-Day MACE between Immediate versus Staged Complete Revascularization in Acute Myocardial Infarction with Multivessel Disease, and the Effect of Coronary Lesion Complexity

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
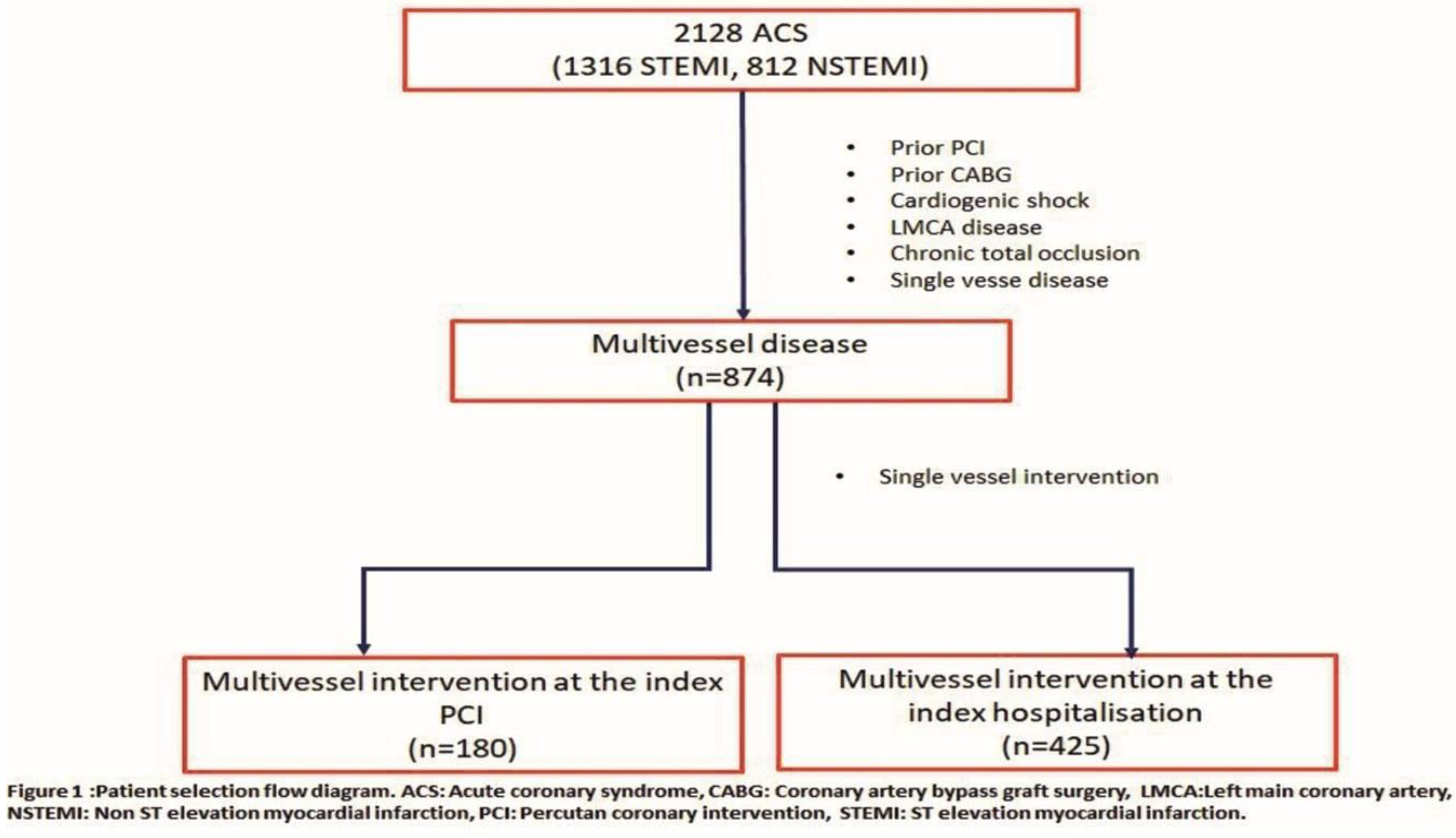
2.1. Study Population
2.2. Definitions
2.3. Sx Score
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ibrahim, H.; Sharma, P.K.; Cohen, D.J.; Fonarow, G.C.; Kaltenbach, L.A.; Effron, M.B.; Zettler, M.E.; Peterson, E.D.; Wang, T.Y. Multivessel Versus Culprit Vessel-Only Percutaneous Coronary Intervention among Patients with Acute Myocardial Infarction: Insights from the TRANSLATE-ACS Observational Study. J. Am. Heart Assoc. 2017, 6, e006343. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.; Zeymer, U.; Hochadel, M.; Möllmann, H.; Weidinger, F.; Zahn, R.; Nef, H.M.; Hamm, C.W.; Marco, J.; Gitt, A.K. Prima-vista multi-vessel percutaneous coronary intervention in haemodynamically stable patients with acute coronary syndromes: Analysis of over 4.400 patients in the EHS-PCI registry. Int. J. Cardiol. 2013, 166, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Sorajja, P.; Gersh, B.J.; Cox, D.A.; McLaughlin, M.G.; Zimetbaum, P.; Costantini, C.; Stuckey, T.; Tcheng, J.E.; Mehran, R.; Lansky, A.J. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur. Heart J. 2007, 28, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, A.; Wallentin, L.; Simoons, M.; Gitt, A.K.; Behar, S.; Battler, A.; Hasdai, D. Age, clinical presentation, and outcome of acute coronary syndromes in the Euroheart acute coronary syndrome survey. Eur. Heart J. 2006, 27, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Morris, J.K.; Wald, N.J.; Chase, A.J.; Edwards, R.J.; Hughes, L.O.; Berry, C.; Oldroyd, K.G.; PRAMI Investigators. Randomized trial of preventive angioplasty in myocardial infarction. N. Engl. J. Med. 2013, 369, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Gershlick, A.H.; Khan, J.N.; Kelly, D.J.; Greenwood, J.P.; Sasikaran, T.; Curzen, N.; Blackman, D.J.; Dalby, M.; Fairbrother, K.L.; Banya, W. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: The CvLPRIT trial. J. Am. Coll. Cardiol. 2015, 65, 963–972. [Google Scholar] [CrossRef]
- Engstrøm, T.; Kelbæk, H.; Helqvist, S.; Høfsten, D.E.; Kløvgaard, L.; Holmvang, L.; Jørgensen, E.; Pedersen, F.; Saunamäki, K.; Clemmensen, P. Complete revascularization versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3—PRIMULTI): An open-label, randomised controlled trial. Lancet 2015, 386, 665–671. [Google Scholar] [CrossRef]
- Hlinomaz, O.; Groch, L.; Polokova, K.; Lehar, F.; Vekov, T.; Petkov, R.; Stoynev, M.; Griva, M.; Sitar, J.; Rezek, M. Multivessel coronary disease diagnosed at the time of primary PCI for STEMI: Complete revascularization versus conservative strategy. In Proceedings of the Summit of the European Association of Percutaneous Cardiovascular Interventions, Paris, France, 19 May 2015. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2015, 37, 267–315. [Google Scholar]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M. 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2015, 67, 1235–1250. [Google Scholar] [PubMed]
- Garg, S.; Sarno, G.; Serruys, P.W.; Rodriguez, A.E.; Bolognese, L.; Anselmi, M.; De Cesare, N.; Colangelo, S.; Moreno, R.; Gambetti, S. Prediction of 1-year clinical outcomes using the SYNTAX score in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: A substudy of the STRATEGY (Single High-Dose Bolus Tirofiban and Sirolimus-Eluting Stent Versus Abciximab and Bare-Metal Stent in Acute Myocardial Infarction) and MULTISTRATEGY (Multicenter Evaluation of Single High-Dose Bolus Tirofiban Versus Abciximab with Sirolimus-Eluting Stent or Bare-Metal Stent in Acute Myocardial Infarction Study) trials. JACC Cardiovasc. Interv. 2011, 4, 66–75. [Google Scholar] [PubMed]
- Palmerini, T.; Genereux, P.; Caixeta, A.; Cristea, E.; Lansky, A.; Mehran, R.; Dangas, G.; Lazar, D.; Sanchez, R.; Fahy, M.; et al. Prognostic value of the SYNTAX score in patients with acute coronary syndromes undergoing percutaneous coronary intervention: Analysis from the ACUITY (Acute Catheterization and Urgent Intervention Triage StrategY) trial. J. Am. Coll. Cardiol. 2011, 57, 2389–2397. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Park, K.W.; Han, J.K.; Yang, H.M.; Kang, H.J.; Koo, B.K.; Kim, H.S. Usefulness of the Baseline Syntax Score to Predict 3-Year Outcome after Complete Revascularization by Percutaneous Coronary Intervention. Am. J. Cardiol. 2016, 118, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute Dialysis Quality Initiative workgroup. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004. [Google Scholar] [CrossRef]
- Magro, M.; Nauta, S.; Simsek, C.; Onuma, Y.; Garg, S.; van der Heide, E.; van der Giessen, W.J.; Boersma, E.; van Domburg, R.T.; van Geuns, R.J. Value of the SYNTAX score in patients treated by primary percutaneous coronary intervention for acute ST-elevation myocardial infarction: The MISYNTAX score study. Am. Heart J. 2011, 161, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Park, D.W.; Clare, R.M.; Schulte, P.J.; Pieper, K.S.; Shaw, L.K.; Califf, R.M.; Ohman, E.M.; Van de Werf, F.; Hirji, S.; Harrington, R.A. Extent, location, and clinical significance of non-infarct-related coronary artery disease among patients with ST-elevation myocardial infarction. JAMA 2014, 312, 2019–2027. [Google Scholar] [CrossRef]
- Chin, C.T.; L’Allier, P.; Neumann, F.J.; Engstrøm, T.; Jüni, P.; Olivecrona, G.K. The Compare-Acute trial of fractional flow reserve-guided multivessel angioplasty in myocardial infarction. EuroIntervention 2017, 13, 613–616. [Google Scholar] [CrossRef]
- Sardella, G.; Lucisano, L.; Garbo, R.; Pennacchi, M.; Cavallo, E.; Stio, R.E.; Calcagno, S.; Ugo, F.; Boccuzzi, G.; Fedele, F. Single-Staged Compared with Multi-Staged PCI in Multivessel NSTEMI Patients: The SMILE Trial. J. Am. Coll. Cardiol. 2016, 67, 264–272. [Google Scholar] [CrossRef]
- Qiao, Y.; Li, W.; Mohamed, S.; Nie, S.; Du, X.; Zhang, Y.; Jia, C.; Wang, X.; Liu, X.; Ma, C.A. A comparison of multivessel and culprit vessel percutaneous coronary intervention in non-ST-segment elevation acute coronary syndrome patients with multivessel disease: A meta-analysis. EuroIntervention 2015, 11, 525–532. [Google Scholar] [CrossRef]
- Marenzi, G.; Assanelli, E.; Campodonico, J.; Lauri, G.; Marana, I.; De Metrio, M.; Moltrasio, M.; Grazi, M.; Rubino, M.; Veglia, F. Contrast volume during primary percutaneous coronary intervention and subsequent contrast-induced nephropathy and mortality. Ann. Intern. Med. 2009, 150, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G.; Kleinbongard, P.; Böse, D.; Levkau, B.; Haude, M.; Schulz, R.; Erbel, R. Coronary microembolization: From bedside to bench and back to bedside. Circulation 2009, 120, 1822–1836. [Google Scholar] [CrossRef] [PubMed]
- Hanratty, C.G.; Koyama, Y.; Rasmussen, H.H.; Nelson, G.I.; Hansen, P.S.; Ward, M.R. Exaggeration of nonculprit stenosis severity during acute myocardial infarction: Implications for immediate multivessel revascularization. J. Am. Coll. Cardiol. 2002, 40, 911–916. [Google Scholar] [CrossRef]
- Welty, F.K.; Mittleman, M.A.; Lewis, S.M.; Healy, R.W.; Shubrooks, S.J., Jr.; Muller, J.E. Significance of location (anterior versus inferior) and type (Q-wave versus non-Q-wave) of acute myocardial infarction in patients undergoing percutaneous transluminal coronary angioplasty for postinfarction ischemia. Am. J. Cardiol. 1995, 76, 431–435. [Google Scholar] [CrossRef]
- Califf, R.M.; Tomabechi, Y.; Lee, K.L.; Phillips, H.; Pryor, D.B.; Harrell, F.E., Jr.; Harris, P.J.; Peter, R.H.; Behar, V.S.; Kong, Y. Outcome in one-vessel coronary artery disease. Circulation 1983, 67, 283–290. [Google Scholar] [CrossRef]
- El-Menyar, A.; Zubaid, M.; AlMahmeed, W.; Sulaiman, K.; AlNabti, A.; Singh, R.; Al Suwaidi, J. Killip classification in patients with acute coronary syndrome: Insight from a multicenter registry. Am. J. Emerg. Med. 2012, 30, 97–103. [Google Scholar] [CrossRef]
- Iqbal, M.B.; Nadra, I.J.; Ding, L.; Fung, A.; Aymong, E.; Chan, A.W.; Hodge, S.; Della Siega, A.; Robinson, S.D.; British Columbia Cardiac Registry Investigators. Culprit Vessel Versus Multivessel Versus In-Hospital Staged Intervention for Patients With ST-Segment Elevation Myocardial Infarction and Multivessel Disease: Stratified Analyses in High-Risk Patient Groups and Anatomic Subsets of Nonculprit Disease. JACC Cardiovasc. Interv. 2017, 10, 11–23. [Google Scholar] [CrossRef]
- Vlaar, P.J.; Mahmoud, K.D.; Holmes, D.R., Jr.; van Valkenhoef, G.; Hillege, H.L.; van der Horst, I.C.; Zijlstra, F.; de Smet, B.J. Culpritvessel only versus multivessel and staged percutaneous coronary intervention for multivessel disease in patients presenting with ST-segment elevation myocardial infarction: A pairwise and network meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 692–703. [Google Scholar] [CrossRef]
- Li, Z.; Zhou, Y.; Xu, Q.; Chen, X. Staged versus One-Time Complete Revascularization with Percutaneous Coronary Intervention in STEMI Patients with Multivessel Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169406. [Google Scholar] [CrossRef]
- Bainey, K.; Mehta, S.; Lai, T.; Welsh, R. Complete vs culprit-only revascularization for patients with multivessel disease undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: A systematic review and meta-analysis. Am. Heart J. 2014, 167, 1–14. [Google Scholar] [CrossRef]
- Tarantini, G.; D’Amico, G.; Brener, S.J.; Tellaroli, P.; Basile, M.; Schiavo, A.; Mojoli, M.; Fraccaro, C.; Marchese, A.; Musumeci, G. Survival After Varying Revascularization Strategies in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease: A Pairwise and Network Meta-Analysis. JACC Cardiovasc. Interv. 2016, 9, 1765–1776. [Google Scholar] [CrossRef] [PubMed]
- Ayça, B.; Akın, F.; Celik, O.; Cetin, S.; Sahin, I.; Gülşen, K.; Kalyoncuoğlu, M.; Katkat, F.; Okuyan, E.; Dinçkal, M.H. Does SYNTAX score predict in-hospital outcomes in patients with ST elevation myocardial infarction undergoing primary percutaneous coronary intervention? Kardiol. Polska 2014, 72, 806–813. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | MVI-S (n = 425) | MVI-I (n = 180) | p Value |
|---|---|---|---|
| Age, median (interquartile range (IQR)), years | 58 (51–66) | 59 (50–67) | 0.815 |
| Male, n (%) | 335 (78.8) | 152 (84.4) | 0.111 |
| Diabetes mellitus, n (%) | 108 (25.4) | 49 (27.2) | 0.642 |
| Hypertension, n (%) | 334 (78.6) | 146 (81) | 0.483 |
| Smoking, n (%) | 184 (43.3) | 84 (46.7) | 0.615 |
| Hyperlipidemia n (%) | 269 (63.3) | 120 (66.7) | 0.429 |
| Ejection fraction, median (IQR), % | 50 (45–60) | 50 (40–55) | 0.333 |
| Creatinine, median (IQR), mg/dL | 0.8 (0.7–1.0) | 0.9 (0.7–1.0) | 0.024 |
| STEMI, n (%) | 260 (61.2) | 91 (50.6) | 0.016 |
| Non-STEMI, n (%) | 165 (38.8) | 89 (49.4) | |
| STEMI type, n (%) | 0.044 | ||
| Anterior | 99 (37.9) | 48 (52.7) | |
| Inferior | 136 (52.1) | 35 (38.5) | |
| Others | 26 (10.0) | 8 (8.8) | |
| Culprit Lesion, n (%) | 0.016 | ||
| LAD | 153 (36.0) | 86 (47.8) | |
| RCA | 162 (38.1) | 46 (25.6) | |
| CX | 91 (21.4) | 40 (22.2) | |
| Other | 19 (4.5) | 8 (4.4) | |
| Syntax Score, median (IQR) | 14 (12-19) | 14 (11–28) | 0.623 |
| 0–22, % | 85.4 | 89.4 | 0.001 |
| 23–32, % | 13.6 | 9.4 | |
| >32, % | 0.9 | 1.1 | |
| KILLIP, n (%) | |||
| 1 | 420 (98.8) | 169 (93.9) | |
| 2 | 5 (1.1) | 11 (6.1) | |
| Procedural characteristics | |||
| CV DES, n (%) | 393 (92.2) | 165 (91.7) | 0.766 |
| CV TIMI III, n (%) | 366 (86.1) | 169 (93.8) | 0.891 |
| CV GPIIb-IIIa inhibitor, n (%) | 44 (11.7) | 15 (8.4) | 0.231 |
| CV Stent diameter, median (IQR) | 2.75 (2.5–3.0) | 2.75 (2.5–3.0) | 0.559 |
| Thrombectomy, n (%) | 33 (8.8) | 9 (5.1) | 0.123 |
| Medications, n (%) | |||
| ASA | 425 (100) | 180 (100) | 1.000 |
| P2Y12 inhibitor | 422 (99.8) | 179 (99.4) | 0.822 |
| Beta blocker | 412 (98.3) | 176 (98.9) | 0.616 |
| ACEI | 399 (95.2) | 164 (92.1) | 0.136 |
| Statin | 408 (97.4) | 177 (99.4) | 0.100 |
| Odds Ratios (95% Confidence Interval) | ||||||
|---|---|---|---|---|---|---|
| MVI-I n (%) | MVI-S n (%) | Unadjusted | PS Adjusted MV Model | IPW | Covariate Adjusted | |
| MACE | 20(11.2) | 21 (5.0) | 3.02 (1.516.02) | 2.46 (1.19–5.07) | 2.11 (1.28–3.47) | 2.06 (1.02–4.18) |
| 30 Day CV mortality | 16 (8.9) | 9 (2.1) | 4.51 (1.96–10.4) | |||
| Nonfatal MI | 3 (1.7) | 7 (1.7) | 1.01 (0.26–3.96) | |||
| Ischemia driven revascularization | 3 (1.7) | 10 (2.4) | 0.70 (0.19–2.59) | |||
| Acute heart failure | 16 (8.9) | 15 (3.5) | 2.67 (1.29–5.52) | |||
| Nonfatal Stroke | 2 (1.1) | 1 (0.2) | 2.37 (0.15–38.1) | |||
| Acute renal failure | 9 (5.0) | 15 (3.5) | 1.44 (0.62–3.35) | |||
| Bleeding | 4 (2.2) | 11 (2.6) | 0.85 (0.27–2.72) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doğan, C.; Bayram, Z.; Çap, M.; Özkalaycı, F.; Unkun, T.; Erdoğan, E.; Uslu, A.; Acar, R.D.; Guvendi, B.; Akbal, Ö.Y.; et al. Comparison of 30-Day MACE between Immediate versus Staged Complete Revascularization in Acute Myocardial Infarction with Multivessel Disease, and the Effect of Coronary Lesion Complexity. Medicina 2019, 55, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020051
Doğan C, Bayram Z, Çap M, Özkalaycı F, Unkun T, Erdoğan E, Uslu A, Acar RD, Guvendi B, Akbal ÖY, et al. Comparison of 30-Day MACE between Immediate versus Staged Complete Revascularization in Acute Myocardial Infarction with Multivessel Disease, and the Effect of Coronary Lesion Complexity. Medicina. 2019; 55(2):51. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020051
Chicago/Turabian StyleDoğan, Cem, Zübeyde Bayram, Murat Çap, Flora Özkalaycı, Tuba Unkun, Emrah Erdoğan, Abdulkadir Uslu, Rezzan Deniz Acar, Busra Guvendi, Özgur Yaşar Akbal, and et al. 2019. "Comparison of 30-Day MACE between Immediate versus Staged Complete Revascularization in Acute Myocardial Infarction with Multivessel Disease, and the Effect of Coronary Lesion Complexity" Medicina 55, no. 2: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020051