Evaluation of the Second Follicular Wave Phenomenon in Natural Cycle Assisted Reproduction: A Key Option for Poor Responders through Luteal Phase Oocyte Retrieval

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
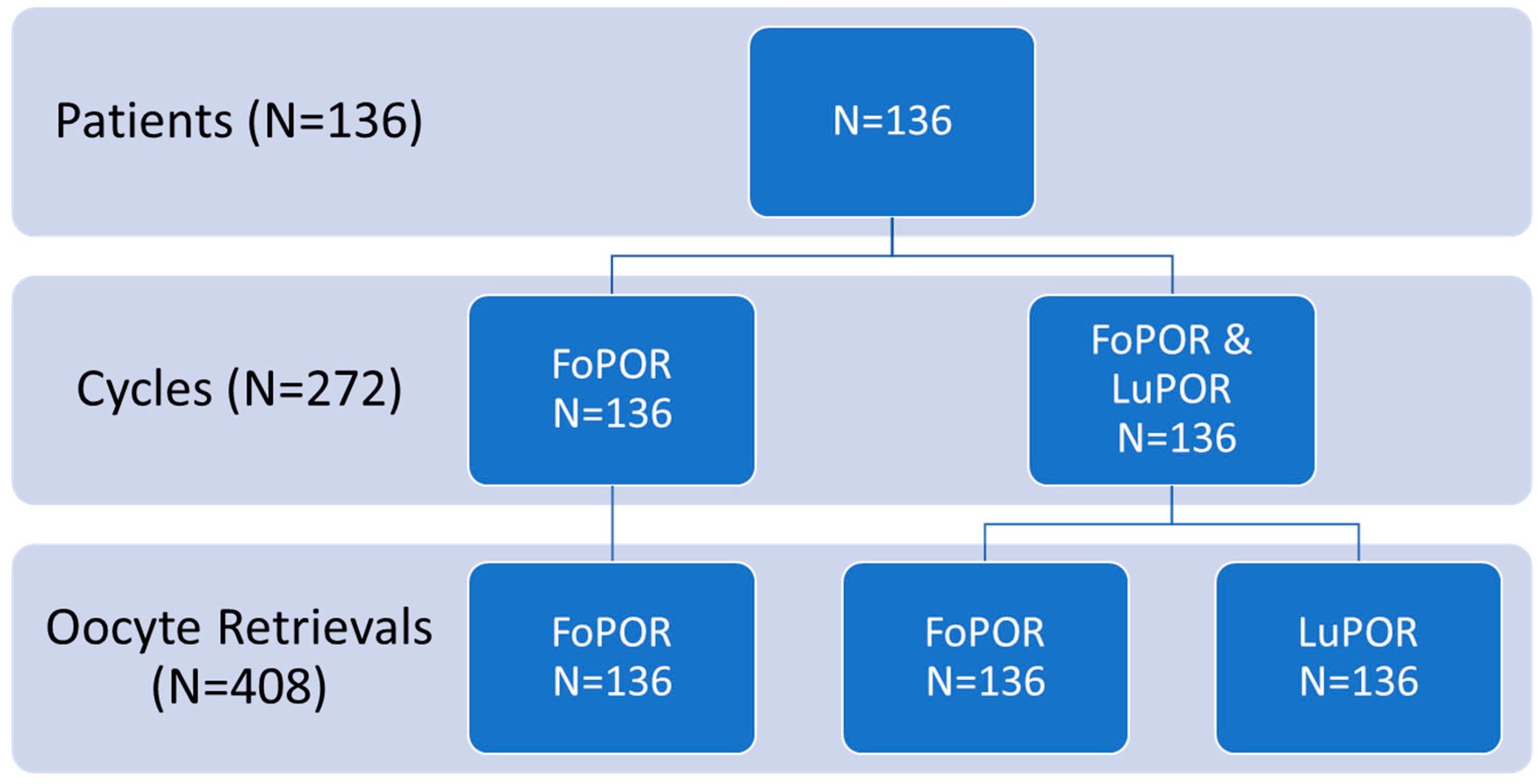
2.1. Study Population
2.2. Natural Cycle Protocol, Oocyte Retrieval and Fertilization
3. Statistical Analysis
4. Results
4.1. Patients’ Characteristics
4.2. Comparison of FoPORs and LuPORs during the Same Unstimulated Natural Menstrual Cycle
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Approval
References
- Block, E. Quantitative morphological investigations of the follicular system in women; variations at different ages. Acta Anat. 1952, 14, 108–123. [Google Scholar] [CrossRef]
- Pache, T.D.; Wladimiroff, J.W.; de Jong, F.H.; Hop, W.C.; Fauser, B.C.J.M. Growth patterns of nondominant ovarian follicles during the normal menstrual cycle. Fertil. Steril. 1990, 54, 638–642. [Google Scholar] [CrossRef]
- Baerwald, A.R.; Adams, G.P.; Pierson, R.A. A new model for ovarian follicular development during the human menstrual cycle. Fertil. Steril. 2003, 80, 116–122. [Google Scholar] [CrossRef]
- Mihm, M.; Crowe, M.; Knight, P.; Austin, E. Follicle Wave Growth in Cattle. Reprod. Domest. Anim. 2002, 37, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Chian, R.-C.; Chung, J.-T.; Downey, B.R.; Tan, S.L. Maturational and developmental competence of immature oocytes retrieved from bovine ovaries at different phases of folliculogenesis. Reprod. Biomed. Online 2002, 4, 127–132. [Google Scholar] [CrossRef]
- Baerwald, A.R.; Adams, G.P.; Pierson, R.A. Ovarian antral folliculogenesis during the human menstrual cycle: A review. Hum. Reprod. Update 2012, 18, 73–91. [Google Scholar] [CrossRef]
- Kuang, Y.; Chen, Q.; Hong, Q.; Lyu, Q.; Ai, A.; Fu, Y.; Shoham, Z. Double stimulations during the follicular and luteal phases of poor responders in IVF/ICSI programmes (Shanghai protocol). Reprod. Biomed. Online 2014, 29, 684–691. [Google Scholar] [CrossRef]
- Garcia, J.E.; Jones, G.S.; Acosta, A.A.; Wright, G. Human menopausal gonadotropin/human chorionic gonadotropin follicular maturation for oocyte aspiration: Phase II, 1981. Fertil. Steril. 1983, 39, 174–179. [Google Scholar] [CrossRef]
- Ferraretti, A.P.; La Marca, A.; Fauser, B.C.J.M.; Tarlatzis, B.; Nargund, G.; Gianaroli, L. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: The Bologna criteria. Hum. Reprod. 2011, 26, 1616–1624. [Google Scholar] [CrossRef]
- Surrey, E.S.; Schoolcraft, W.B. Evaluating strategies for improving ovarian response of the poor responder undergoing assisted reproductive techniques. Fertil. Steril. 2000, 73, 667–676. [Google Scholar] [CrossRef]
- Kyrou, D.; Kolibianakis, E.M.; Venetis, C.A.; Papanikolaou, E.G.; Bontis, J.; Tarlatzis, B.C. How to improve the probability of pregnancy in poor responders undergoing in vitro fertilization: A systematic review and meta-analysis. Fertil. Steril. 2009, 91, 749–766. [Google Scholar] [CrossRef] [PubMed]
- Tarlatzis, B.C.; Zepiridis, L.; Grimbizis, G.; Bontis, J. Clinical management of low ovarian response to stimulation for IVF: A systematic review. Hum. Reprod. Update 2003, 9, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Loutradis, D.; Vomvolaki, E.; Drakakis, P. Poor responder protocols for in-vitro fertilization: Options and results. Curr. Opin. Obstet. Gynecol. 2008, 20, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Pandian, Z.; McTavish, A.R.; Aucott, L.; Hamilton, M.P.; Bhattacharya, S. Interventions for “poor responders” to controlled ovarian hyper stimulation (COH) in in-vitro fertilisation (IVF). Cochrane Database Syst. Rev. 2010, CD004379. [Google Scholar] [CrossRef]
- Penzias, A.S. Improving results with assisted reproductive technologies: Individualized patient-tailored strategies for ovulation induction. Reprod. Biomed. Online 2011, 22 (Suppl. 1), S83–S86. [Google Scholar] [CrossRef]
- Wyndham, N.; Marin Figueira, P.G.; Patrizio, P. A persistent misperception: Assisted reproductive technology can reverse the “aged biological clock”. Fertil. Steril. 2012, 97, 1044–1047. [Google Scholar] [CrossRef] [PubMed]
- Patrizio, P.; Vaiarelli, A.; Levi Setti, P.E.; Tobler, K.J.; Shoham, G.; Leong, M.; Shoham, Z. How to define, diagnose and treat poor responders? Responses from a worldwide survey of IVF clinics. Reprod. Biomed. Online 2015, 30, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Humaidan, P.; Alviggi, C.; Fischer, R.; Esteves, S.C. The novel POSEIDON stratification of ‘Low prognosis patients in Assisted Reproductive Technology’ and its proposed marker of successful outcome. F1000Research 2016, 5, 2911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pu, D.; Wu, J.; Liu, J. Comparisons of GnRH antagonist versus GnRH agonist protocol in poor ovarian responders undergoing IVF. Hum. Reprod. 2011, 26, 2742–2749. [Google Scholar] [CrossRef] [Green Version]
- Ferraretti, A.P.; Gianaroli, L.; Magli, M.C.; D’angelo, A.; Farfalli, V.; Montanaro, N. Exogenous luteinizing hormone in controlled ovarian hyperstimulation for assisted reproduction techniques. Fertil. Steril. 2004, 82, 1521–1526. [Google Scholar] [CrossRef]
- Ubaldi, F.M.; Rienzi, L.; Ferrero, S.; Baroni, E.; Sapienza, F.; Cobellis, L.; Greco, E. Management of poor responders in IVF. Reprod. Biomed. Online 2005, 10, 235–246. [Google Scholar] [CrossRef]
- Bosdou, J.K.; Venetis, C.A.; Kolibianakis, E.M.; Toulis, K.A.; Goulis, D.G.; Zepiridis, L.; Tarlatzis, B.C. The use of androgens or androgen-modulating agents in poor responders undergoing in vitro fertilization: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 127–145. [Google Scholar] [CrossRef]
- D’Amato, G.; Caroppo, E.; Pasquadibisceglie, A.; Carone, D.; Vitti, A.; Vizziello, G.M. A novel protocol of ovulation induction with delayed gonadotropin-releasing hormone antagonist administration combined with high-dose recombinant follicle-stimulating hormone and clomiphene citrate for poor responders and women over 35 years. Fertil. Steril. 2004, 81, 1572–1577. [Google Scholar] [CrossRef]
- Chern, C.-U.; Tsui, K.-H.; Vitale, S.G.; Chen, S.-N.; Wang, P.-H.; Cianci, A.; Tsai, H.-W.; Wen, Z.-H.; Lin, L.-T. Dehydroepiandrosterone (DHEA) supplementation improves in vitro fertilization outcomes of poor ovarian responders, especially in women with low serum concentration of DHEA-S: A retrospective cohort study. Reprod. Biol. Endocrinol. 2018, 16, 90. [Google Scholar] [CrossRef]
- Unfer, V.; Raffone, E.; Rizzo, P.; Buffo, S. Effect of a supplementation with myo-inositol plus melatonin on oocyte quality in women who failed to conceive in previous in vitro fertilization cycles for poor oocyte quality: A prospective, longitudinal, cohort study. Gynecol. Endocrinol. 2011, 27, 857–861. [Google Scholar] [CrossRef]
- Vitale, S.G.; Rossetti, P.; Corrado, F.; Rapisarda, A.M.C.; La Vignera, S.; Condorelli, R.A.; Valenti, G.; Sapia, F.; Laganà, A.S.; Buscema, M. How to Achieve High-Quality Oocytes? The Key Role of Myo-Inositol and Melatonin. Int. J. Endocrinol. 2016, 2016, 4987436. [Google Scholar] [CrossRef]
- Waldenström, U.; Hellberg, D.; Nilsson, S. Low-dose aspirin in a short regimen as standard treatment in in vitro fertilization: A randomized, prospective study. Fertil. Steril. 2004, 81, 1560–1564. [Google Scholar] [CrossRef]
- Filicori, M.; Cognigni, G.E.; Gamberini, E.; Parmegiani, L.; Troilo, E.; Roset, B. Efficacy of low-dose human chorionic gonadotropin alone to complete controlled ovarian stimulation. Fertil. Steril. 2005, 84, 394–401. [Google Scholar] [CrossRef]
- Patrono, C.; García Rodríguez, L.A.; Landolfi, R.; Baigent, C. Low-dose aspirin for the prevention of atherothrombosis. N. Engl. J. Med. 2005, 353, 2373–2383. [Google Scholar] [CrossRef]
- Berkkanoglu, M.; Isikoglu, M.; Aydin, D.; Ozgur, K. Clinical effects of ovulation induction with recombinant follicle-stimulating hormone supplemented with recombinant luteinizing hormone or low-dose recombinant human chorionic gonadotropin in the midfollicular phase in microdose cycles in poor responders. Fertil. Steril. 2007, 88, 665–669. [Google Scholar] [CrossRef]
- Frattarelli, J.L.; McWilliams, G.D.E.; Hill, M.J.; Miller, K.A.; Scott, R.T. Low-dose aspirin use does not improve in vitro fertilization outcomes in poor responders. Fertil. Steril. 2008, 89, 1113–1117. [Google Scholar] [CrossRef]
- Nardo, L.G.; Granne, I.; Stewart, J. Policy & Practice Committee of the British Fertility Society. Medical adjuncts in IVF: Evidence for clinical practice. Hum. Fertil. 2009, 12, 1–13. [Google Scholar] [CrossRef]
- Papathanasiou, A.; Searle, B.J.; King, N.M.A.; Bhattacharya, S. Trends in “poor responder” research: Lessons learned from RCTs in assisted conception. Hum. Reprod. Update 2016, 22. [Google Scholar] [CrossRef]
- Morgia, F.; Sbracia, M.; Schimberni, M.; Giallonardo, A.; Piscitelli, C.; Giannini, P.; Aragona, C. A controlled trial of natural cycle versus microdose gonadotropin-releasing hormone analog flare cycles in poor responders undergoing in vitro fertilization. Fertil. Steril. 2004, 81, 1542–1547. [Google Scholar] [CrossRef]
- Schimberni, M.; Morgia, F.; Colabianchi, J.; Giallonardo, A.; Piscitelli, C.; Giannini, P.; Montigiani, M.; Sbracia, M. Natural-cycle in vitro fertilization in poor responder patients: A survey of 500 consecutive cycles. Fertil. Steril. 2009, 92, 1297–1301. [Google Scholar] [CrossRef]
- Orris, J.J.; Taylor, T.H.; Gilchrist, J.W.; Hallowell, S.V.; Glassner, M.J.; Wininger, J.D. The utility of embryo banking in order to increase the number of embryos available for preimplantation genetic screening in advanced maternal age patients. J. Assist. Reprod. Genet. 2010, 27, 729–733. [Google Scholar] [CrossRef] [Green Version]
- Kushnir, V.A.; Barad, D.H.; Albertini, D.F.; Darmon, S.K.; Gleicher, N. Effect of Embryo Banking on U.S. National Assisted Reproductive Technology Live Birth Rates. PLoS ONE 2016, 11, e0154620. [Google Scholar] [CrossRef]
- Gleicher, N.; Kushnir, V.A.; Albertini, D.F.; Barad, D.H. Improvements in IVF in women of advanced age. J. Endocrinol. 2016, 230, F1–F6. [Google Scholar] [CrossRef] [Green Version]
- Ubaldi, F.M.; Capalbo, A.; Vaiarelli, A.; Cimadomo, D.; Colamaria, S.; Alviggi, C.; Trabucco, E.; Venturella, R.; Vajta, G.; Rienzi, L. Follicular versus luteal phase ovarian stimulation during the same menstrual cycle (DuoStim) in a reduced ovarian reserve population results in a similar euploid blastocyst formation rate: New insight in ovarian reserve exploitation. Fertil. Steril. 2016, 105, 1488–1495.e1. [Google Scholar] [CrossRef]
- Vaiarelli, A.; Venturella, R.; Vizziello, D.; Bulletti, F.; Ubaldi, F.M. Dual ovarian stimulation and random start in assisted reproductive technologies: From ovarian biology to clinical application. Curr. Opin. Obstet. Gynecol. 2017, 29, 153. [Google Scholar] [CrossRef]
- Maman, E.; Meirow, D.; Brengauz, M.; Raanani, H.; Dor, J.; Hourvitz, A. Luteal phase oocyte retrieval and in vitro maturation is an optional procedure for urgent fertility preservation. Fertil. Steril. 2011, 95, 64–67. [Google Scholar] [CrossRef]
- Martinez, F.; Clua, E.; Devesa, M.; Rodriguez, I.; Arroyo, G.; Gonzalez, C.; Sole, M.; Tur, R.; Coroleu, B.; Barri, P.N. Comparison of starting ovarian stimulation on day 2 versus day 15 of the menstrual cycle in the same oocyte donor and pregnancy rates among the corresponding recipients of vitrified oocytes. Fertil. Steril. 2014, 102, 1307–1311. [Google Scholar] [CrossRef]
- Von Wolff, M.; Thaler, C.J.; Frambach, T.; Zeeb, C.; Lawrenz, B.; Popovici, R.M.; Strowitzki, T. Ovarian stimulation to cryopreserve fertilized oocytes in cancer patients can be started in the luteal phase. Fertil. Steril. 2009, 92, 1360–1365. [Google Scholar] [CrossRef]
- Xu, B.; Li, Y. Flexible ovarian stimulation in a poor responder: A case report and literature review. Reprod. Biomed. Online 2013, 26, 378–383. [Google Scholar] [CrossRef]
- Kuang, Y.; Hong, Q.; Chen, Q.; Lyu, Q.; Ai, A.; Fu, Y.; Shoham, Z. Luteal-phase ovarian stimulation is feasible for producing competent oocytes in women undergoing in vitro fertilization/intracytoplasmic sperm injection treatment, with optimal pregnancy outcomes in frozen-thawed embryo transfer cycles. Fertil. Steril. 2014, 101, 105–111. [Google Scholar] [CrossRef]
- Cardoso, M.C.A.; Evangelista, A.; Sartorio, C.; Vaz, G.; Werneck, C.L.V.; Guimaraes, F.M.; Sa, P.G.; Erthal, M.C. Can ovarian double-stimulation in the same menstrual cycle improve IVF outcomes? JBRA Assist. Reprod. 2017, 21, 217–221. [Google Scholar] [CrossRef]
- Liu, C.; Jiang, H.; Zhang, W.; Yin, H. Double ovarian stimulation during the follicular and luteal phase in women >/=38 years: A retrospective case-control study. Reprod. Biomed. Online 2017, 35, 678–684. [Google Scholar] [CrossRef]
- Ubaldi, F.M.; Vaiarelli, A.; Alviggi, C.; Trabucco, E.; Zullo, F.; Capalbo, A.; Cimadomo, D.; Rienzi, L. Double stimulation in a single menstrual cycle increases the number of oocytes retrieved in poor prognosis patients undergoing IVF treatment. Prospective study with historical control. Fertil. Steril. 2015, 104, e322. [Google Scholar] [CrossRef]
- Zhang, J. Luteal phase ovarian stimulation following oocyte retrieval: Is it helpful for poor responders? Reprod. Biol. Endocrinol. RB&E 2015, 13, 76. [Google Scholar] [CrossRef]
- Lin, L.-T.; Vitale, S.G.; Chen, S.-N.; Wen, Z.-H.; Tsai, H.-W.; Chern, C.-U.; Tsui, K.-H. Luteal Phase Ovarian Stimulation May Improve Oocyte Retrieval and Oocyte Quality in Poor Ovarian Responders Undergoing In Vitro Fertilization: Preliminary Results from a Single-Center Prospective Pilot Study. Adv. Ther. 2018, 35, 847–856. [Google Scholar] [CrossRef]
- Wu, Y.; Zhao, F.C.; Sun, Y.; Liu, P.S. Luteal-phase protocol in poor ovarian response: A comparative study with an antagonist protocol. J. Int. Med. Res. 2017, 45, 1731–1738. [Google Scholar] [CrossRef]
- Baart, E.B.; Martini, E.; Eijkemans, M.J.; Van Opstal, D.; Beckers, N.G.M.; Verhoeff, A.; Macklon, N.S.; Fauser, B.C.J.M. Milder ovarian stimulation for in-vitro fertilization reduces aneuploidy in the human preimplantation embryo: A randomized controlled trial. Hum. Reprod. 2007, 22, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Baker, V.L.; Brown, M.B.; Luke, B.; Conrad, K.P. Association between oocyte number retrieved with live birth rate and birth weight: An analysis of 231,815 cycles of in vitro fertilization. Fertil. Steril. 2015, 103, 931–938.e2. [Google Scholar] [CrossRef]
- Kamath, M.S.; Kirubakaran, R.; Mascarenhas, M.; Sunkara, S.K. Perinatal outcomes after stimulated versus natural cycle IVF: A systematic review and meta-analysis. Reprod. Biomed. Online 2018, 36, 94–101. [Google Scholar] [CrossRef] [PubMed]
- De Klerk, C.; Macklon, N.S.; Heijnen, E.M.E.W.; Eijkemans, M.J.C.; Fauser, B.C.J.M.; Passchier, J.; Hunfeld, J.a.M. The psychological impact of IVF failure after two or more cycles of IVF with a mild versus standard treatment strategy. Hum. Reprod. 2007, 22, 2554–2558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ubaldi, F.; Vaiarelli, A.; D’Anna, R.; Rienzi, L. Management of Poor Responders in IVF: Is There Anything New? BioMed Res. Int. 2014. [Google Scholar] [CrossRef]
- Baerwald, A.R.; Adams, G.P.; Pierson, R.A. Characterization of ovarian follicular wave dynamics in women. Biol. Reprod. 2003, 69, 1023–1031. [Google Scholar] [CrossRef]
- Child, T.; Leonard, S.A.; Evans, J.S.; Lass, A. Systematic review of the clinical efficacy of vaginal progesterone for luteal phase support in assisted reproductive technology cycles. Reprod. Biomed. Online 2018. [CrossRef]
- Herman, A.; Ron-El, R.; Golan, A.; Nahum, H.; Soffer, Y.; Caspi, E. Follicle cysts after menstrual versus midluteal administration of gonadotropin-releasing hormone analog in in vitro fertilization. Fertil. Steril. 1990, 53, 854–858. [Google Scholar] [CrossRef]
- Ben-Rafael, Z.; Bider, D.; Menashe, Y.; Maymon, R.; Zolti, M.; Mashiach, S. Follicular and luteal cysts after treatment with gonadotropin-releasing hormone analog for in vitro fertilization**Presented in part at the VIth World Congress of In Vitro Fertilization and Assisted Reproductive Technologies, Jerusalem, Israel, April 2 to 7, 1989. Fertil. Steril. 1990, 53, 1091–1094. [Google Scholar] [CrossRef]
- Creux, H.; Monnier, P.; Son, W.Y.; Tulandi, T.; Buckett, W. Immature oocyte retrieval and in vitro oocyte maturation at different phases of the menstrual cycle in women with cancer who require urgent gonadotoxic treatment. Fertil. Steril. 2017, 107, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.H.; Ma, W.H.; Tang, N.; Wei, J.H. Luteal-phase ovarian stimulation is a feasible method for poor ovarian responders undergoing in vitro fertilization/intracytoplasmic sperm injection-embryo transfer treatment compared to a GnRH antagonist protocol: A retrospective study. Taiwan J. Obstet. Gynecol. 2016, 55, 50–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grynberg, M.; Poulain, M.; le Parco, S.; Sifer, C.; Fanchin, R.; Frydman, N. Similar in vitro maturation rates of oocytes retrieved during the follicular or luteal phase offer flexible options for urgent fertility preservation in breast cancer patients. Hum. Reprod. 2016, 31, 623–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiser, A.; Son, W.-Y.; Shalom-Paz, E.; Reinblatt, S.L.; Tulandi, T.; Holzer, H. How old is too old for in vitro maturation (IVM) treatment? Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Garel, M.; Blondel, B.; Karpel, L.; Blanchet, V.; Breart, G.; Frydman, R.; Olivennes, F. Women’s views on Friendly IVF: A qualitative preliminary study. J. Psychosom. Obstet. Gynaecol. 2009, 30, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, S.; Boivin, J.; Peronace, L.; Verhaak, C.M. Why do patients discontinue fertility treatment? A systematic review of reasons and predictors of discontinuation in fertility treatment. Hum. Reprod. Update 2012, 18, 652–669. [Google Scholar] [CrossRef] [Green Version]
- Wang, N.; Wang, Y.; Chen, Q.; Dong, J.; Tian, H.; Fu, Y.; Ai, A.; Lyu, Q.; Kuang, Y. Luteal-phase ovarian stimulation vs. conventional ovarian stimulation in patients with normal ovarian reserve treated for IVF: A large retrospective cohort study. Clin. Endocrinol. 2016, 84, 720–728. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean ± SD | |
|---|---|
| Age | 44.08 ± 2.24 |
| AMH (ng/mL) | 0.88 ± 0.98 |
| FSH (mIU/mL) | 17.15 ± 4.86 |
| LH (mIU/mL) | 7.11 ± 4.77 |
| E2 (pg/mL) | 64.09 ± 41.54 |
| Progesterone (ng/mL) | 2.38 ± 1.83 |
| FoPORs | LuPORs | p | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Range | Mean ± SD | Median | Range | ||||
| Min | Max | Min | Max | ||||||
| Oocytes Received a | 1.22 ± 0.48 | 1 | 1 | 3 | 1.29 ± 0.55 | 1 | 1 | 4 | 0.30 |
| MII a | 0.91 ± 0.45 | 1 | 0 | 2 | 1.01 ± 0.48 | 1 | 0 | 3 | 0.08 |
| MI b | 0.11 ± 0.31 | 0 | 0 | 1 | 0.10 ± 0.33 | 0 | 0 | 1 | 0.7 |
| GV b | 0.11 ± 0.34 | 0 | 0 | 1 | 0.12 ± 0.34 | 0 | 0 | 1 | 0.84 |
| Abnormal b | 0.09 ± 0.28 | 0 | 0 | 1 | 0.07 ± 0.26 | 0 | 0 | 1 | 0.66 |
| 2PN a | 0.64 ± 0.56 | 1 | 0 | 2 | 0.67 ± 0.54 | 1 | 0 | 2 | 0.61 |
| Unfertilized b | 0.11 ± 0.31 | 0 | 0 | 1 | 0.10 ± 0.34 | 0 | 0 | 1 | 0.57 |
| 3PN b | 0.03 ± 0.19 | 0 | 0 | 1 | 0.06 ± 0.23 | 0 | 0 | 1 | 0.4 |
| Lysed b | 0.07 ± 0.25 | 0 | 0 | 1 | 0.08 ± 0.27 | 0 | 0 | 1 | 0.64 |
| Natural FoPORs Only | Natural FoPORs + LuPORs | p | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Range | Mean ± SD | Median | Range | ||||
| Min | Max | Min | Max | ||||||
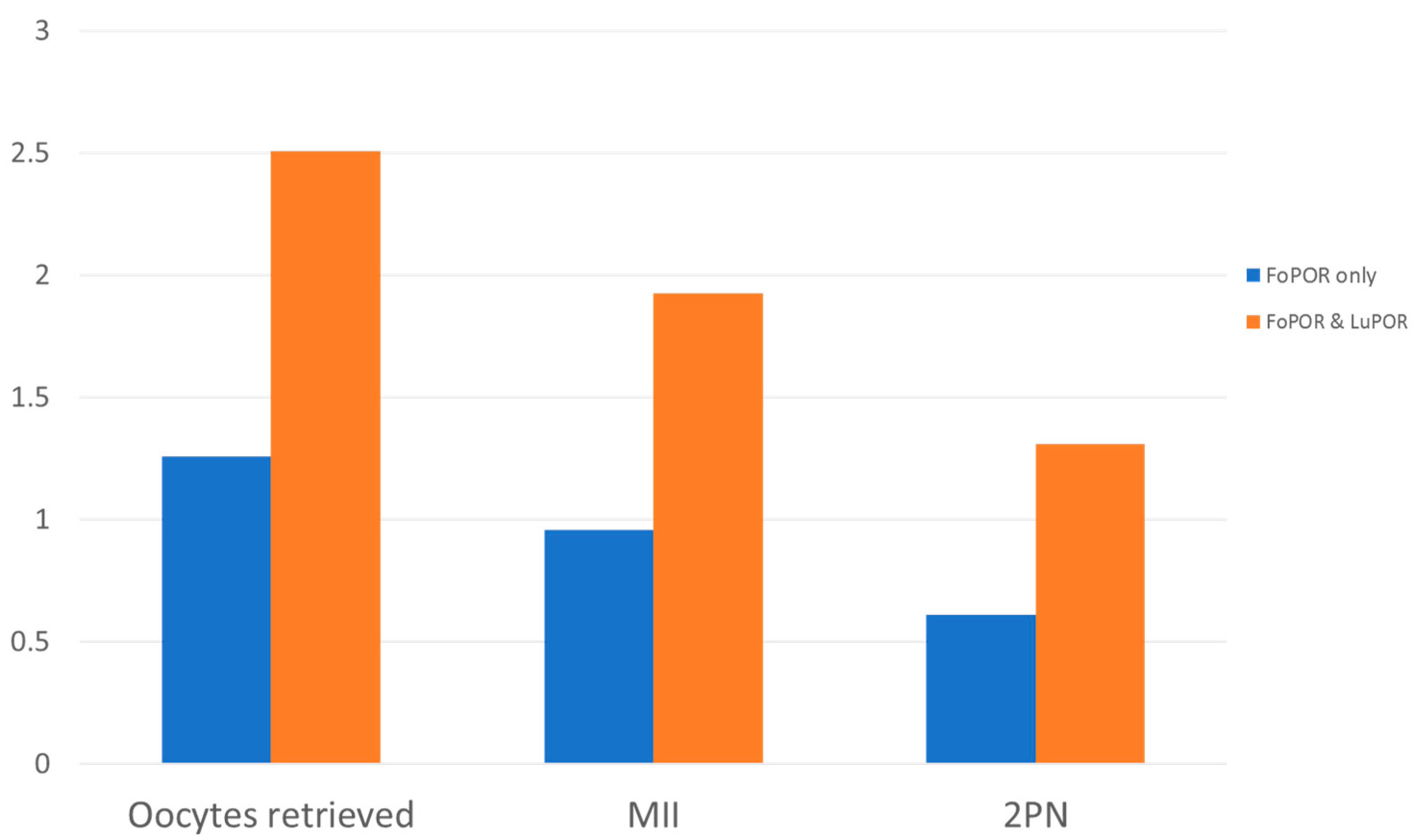
| Oocytes Received a | 1.25 ± 0.53 | 1 | 1 | 4 | 2.50 ± 0.78 | 3 | 2 | 6 | <0.001 * |
| MII a | 0.95 ± 0.59 | 1 | 0 | 3 | 1.93 ± 0.69 | 2 | 0 | 5 | <0.001 * |
| MI b | 0.11 ± 0.31 | 0 | 0 | 2 | 0.21 ± 0.49 | 0 | 0 | 2 | 0.08 |
| GV b | 0.13 ± 0.33 | 0 | 0 | 1 | 0.23 ± 0.50 | 0 | 0 | 2 | 0.09 |
| Abnormal b | 0.08 ± 0.27 | 0 | 0 | 1 | 0.16 ± 0.41 | 0 | 0 | 2 | 0.08 |
| 2PN a | 0.61 ± 0.60 | 1 | 0 | 2 | 1.31 ± 0.87 | 2 | 0 | 4 | <0.001 * |
| Unfertilized b | 0.15 ± 0.36 | 0 | 0 | 1 | 0.21 ± 0.48 | 0 | 0 | 2 | 0.45 |
| 3PN b | 0.05 ± 0.22 | 0 | 0 | 1 | 0.10 ± 0.29 | 0 | 0 | 1 | 0.33 |
| Lysed b | 0.07 ± 0.26 | 0 | 0 | 1 | 0.14 ± 0.35 | 0 | 0 | 1 | 0.05 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sfakianoudis, K.; Simopoulou, M.; Maziotis, E.; Giannelou, P.; Tsioulou, P.; Rapani, A.; Pantou, A.; Petroutsou, K.; Angeli, I.; Deligeoroglou, E.; et al. Evaluation of the Second Follicular Wave Phenomenon in Natural Cycle Assisted Reproduction: A Key Option for Poor Responders through Luteal Phase Oocyte Retrieval. Medicina 2019, 55, 68. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55030068
Sfakianoudis K, Simopoulou M, Maziotis E, Giannelou P, Tsioulou P, Rapani A, Pantou A, Petroutsou K, Angeli I, Deligeoroglou E, et al. Evaluation of the Second Follicular Wave Phenomenon in Natural Cycle Assisted Reproduction: A Key Option for Poor Responders through Luteal Phase Oocyte Retrieval. Medicina. 2019; 55(3):68. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55030068
Chicago/Turabian StyleSfakianoudis, Konstantinos, Mara Simopoulou, Evangelos Maziotis, Polina Giannelou, Petroula Tsioulou, Anna Rapani, Agni Pantou, Konstantina Petroutsou, Irene Angeli, Efthymios Deligeoroglou, and et al. 2019. "Evaluation of the Second Follicular Wave Phenomenon in Natural Cycle Assisted Reproduction: A Key Option for Poor Responders through Luteal Phase Oocyte Retrieval" Medicina 55, no. 3: 68. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55030068