Effects of Boxing Matches on Metabolic, Hormonal, and Inflammatory Parameters in Male Elite Boxers

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Blood Collection and Analysis
2.4. Statistical Analysis
3. Results
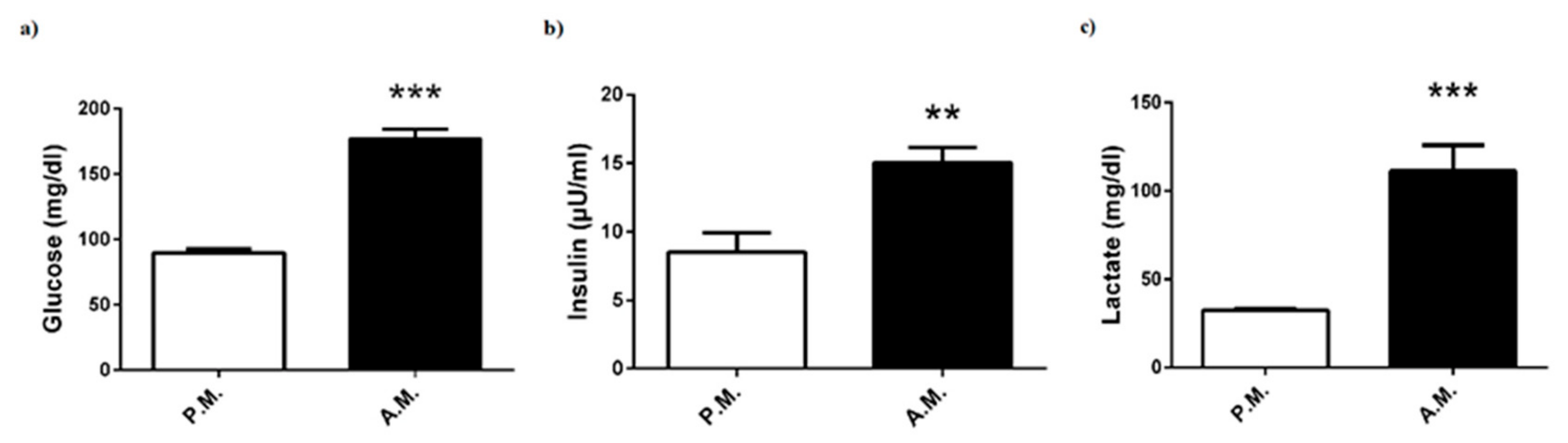
3.1. Metabolic Parameters
3.2. Hormonal Status
3.3. Inflammatory Parameters
3.4. Redox Status
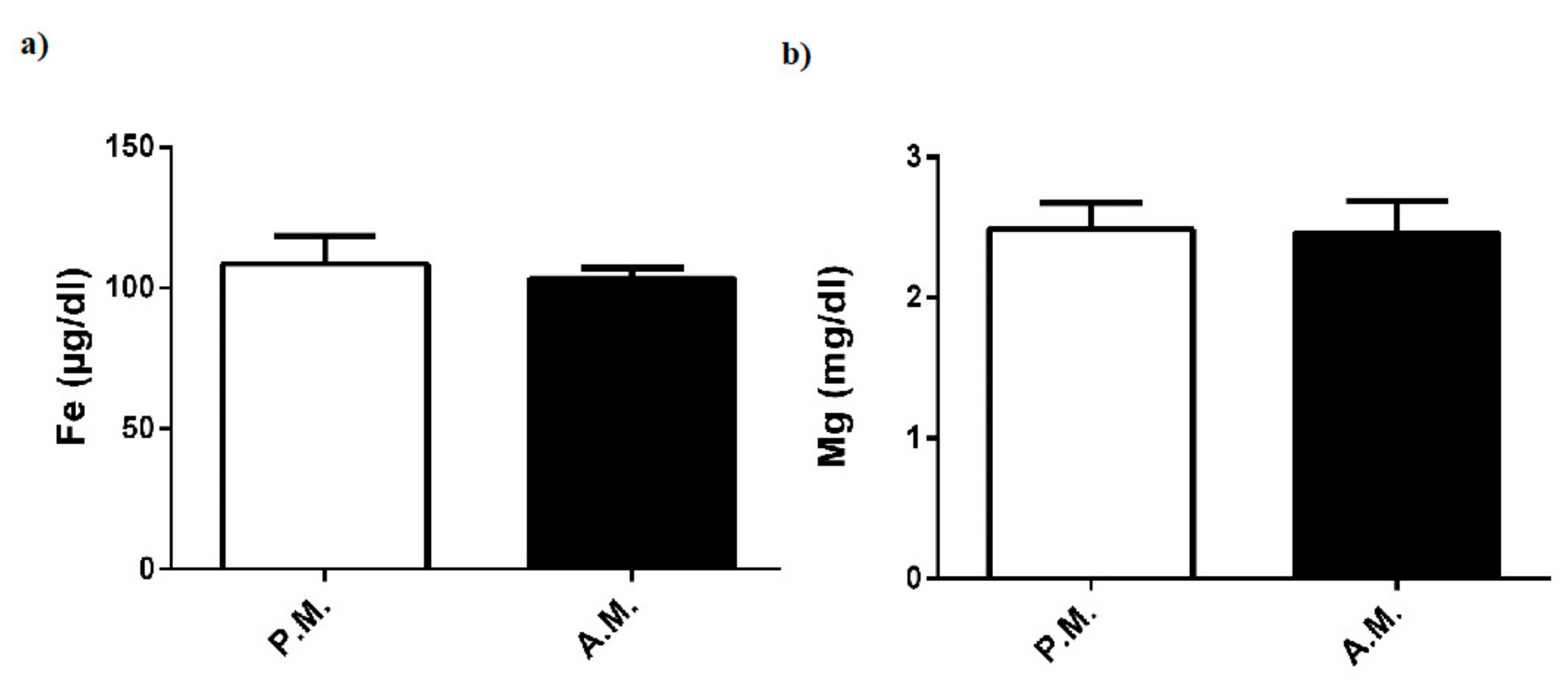
3.5. Fe and Mg levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Davis, P.; Wittekind, A.; Beneke, R. Amateur boxing: Activity profile of winners and losers. Int. J. Sports Physiol. Perform. 2013, 8, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Chaabene, H.; Tabben, M.; Mkaouer, B.; Franchini, E.; Negra, Y.; Hammami, M.; Amara, S.; Chaabene, R.B.; Hachana, Y. Amateur boxing: Physical and physiological attributes. Sports Med. 2015, 45, 337–352. [Google Scholar] [CrossRef] [PubMed]
- Saengsirisuwan, V.; Phadungkij, S.; Pholpramool, C. Renal and liver functions and muscle injuries during training and after competition in Thai boxers. Br. J. Sports Med. 1998, 32, 304–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilz-Burstein, R.; Ashkenazi, Y.; Yaakobovitz, Y.; Cohen, Y.; Zigel, L.; Nemet, D.; Shamash, N.; Eliakim, A. Hormonal response to Taekwondo fighting simulation in elite adolescent athletes. Eur. J. Appl. Physiol. 2010, 110, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.K. Heart Rate: Oxygen consumption and blood lactate responses during specific training in amateur boxing. IJASS 2010, 22, 1–12. [Google Scholar]
- Moreira, A.; Arsati, F.; Lima-Arsati, Y.B.; Franchini, E.; De Araújo, V.C. Effect of a kickboxing match on salivary cortisol and immunoglobulin A. Percept. Mot. Skills 2010, 111, 158–166. [Google Scholar] [CrossRef]
- Pesce, M.; Fratta, I.L.; Ialenti, V.; Patruno, A.; Ferrone, A.; Franceschelli, S.; Rizzuto, A.; Tatangelo, R.; Campagna, G.; Speranza, L.; et al. Emotions, immunity and sport: Winner and loser athlete’s profile of fighting sport. Brain Behav. Immun. 2015, 46, 261–269. [Google Scholar] [CrossRef]
- Ouergui, I.; Davis, P.; Houcine, N.; Marzouki, H.; Zaouali, M.; Franchini, E.; Gmada, N.; Bouhlel, E. Hormonal, physiological, and physical performance during simulated kickboxing combat: Differences between winners and losers. Int. J. Sports Physiol. Perform. 2016, 11, 425–431. [Google Scholar] [CrossRef]
- Peake, J.M.; Tan, S.J.; Markworth, J.F.; Broadbent, J.A.; Skinner, T.L.; Cameron-Smith, D. Metabolic and hormonal responses to isoenergetic high-intensity interval exercise and continuous moderate-intensity exercise. Am. J. Physiol. Endocrinol. Metab. 2014, 307, 539–552. [Google Scholar] [CrossRef]
- Cartee, G.D. Mechanisms for greater insulin-stimulated glucose uptake in normal and insulin-resistant skeletal muscle after acute exercise. Am. J. Physiol. Endocrinol. Metab. 2015, 309, 949–959. [Google Scholar] [CrossRef]
- Adams, O.P. The impact of brief high-intensity exercise on blood glucose levels. Diabetes Metab. Syndr. Obes. 2013, 6, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, M.M.; Rajasekaran, S.; Thomsen, T.W.; Peterson, A.R. Lactate: Friend or foe. PMR 2016, 8, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, R.J.; Madgwick, Z.; Whyte, G.P. The exercise-induced growth hormone response in athletes. Sports Med. 2003, 33, 599–613. [Google Scholar] [CrossRef] [PubMed]
- Pomerants, T.; Tillmann, V.; Karelson, K.; Jürimäe, J.; Jürimäe, T. Impact of acute exercise on bone turnover and growth hormone/insulin-like growth factor axis in boys. J. Sports Med. Phys. Fit. 2008, 48, 266–271. [Google Scholar]
- Frystyk, J. Exercise and the growth hormone–insulin-like growth factor axis. Med. Sci Sports Exerc. 2010, 42, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Eliakim, A.; Nemet, D. The endocrine response to exercise and training in young athletes. Pediatr. Exerc. Sci. 2013, 25, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Mastorakos, G.; Pavlatou, M.; Diamanti-Kandarakis, E.; Chrousos, G.P. Exercise and the stress system. Hormones (Athens) 2005, 4, 73–89. [Google Scholar]
- Anderson, T.; Wideman, L. Exercise and the cortisol awakening response: A systematic review. Sports Med. Open 2017, 3, 37. [Google Scholar] [CrossRef]
- Nassib, S.; Moalla, W.; Hammoudi-Nassib, S.; Chtara, M.; Hachana, Y.; Tabka, Z.; Chamari, K.; Elloumi, M. The IGF-1/cortisol ratio as a useful marker for monitoring training in young boxers. Biol. Sport 2016, 33, 15–22. [Google Scholar] [CrossRef]
- DeRijk, R.; Michelson, D.; Karp, B.; Petrides, J.; Galliven, E.; Deuster, P.; Paciotti, G.; Gold, P.W.; Sternberg, E.M. Exercise and circadian rhythm-induced variations in plasma cortisol differentially regulate interleukin-1 beta (IL-1 beta), IL-6, and tumor necrosis factor-alpha (TNF alpha) production in humans: High sensitivity of TNF alpha and resistance of IL-6. J. Clin. Endocrinol. Metab. 1997, 82, 2182–2191. [Google Scholar] [CrossRef]
- Ostrowski, K.; Hermann, C.; Bangash, A.; Schjerling, P.; Nielsen, J.N.; Pedersen, B.K. A trauma-like elevation of plasma cytokines in humans in response to treadmill running. J. Physiol. 1998, 513, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Ostrowski, K.; Rohde, T.; Asp, S.; Schjerling, P.; Pedersen, B.K. Pro- and anti-inflammatory cytokine balance in strenuous exercise in humans. J. Physiol. 1999, 515, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Konishi, M.; Takahashi, M.; Tabata, H.; Endo, N.; Numao, S.; Lee, S.K.; Kim, Y.H.; Suzuki, K.; Sakamoto, S. Effects of acute endurance exercise performed in the morning and evening on inflammatory cytokine and metabolic hormone response. PLoS ONE 2015, 10, e0137567. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Steensberg, A.; Fischer, C.; Keller, C.; Ostrowski, K.; Schjerling, P. Exercise and cytokines with particular focus on muscle-derived IL-6. Exerc. Immunol. Rev. 2001, 7, 18–31. [Google Scholar] [PubMed]
- Suzuki, K. Cytokine response to exercise and its modulation. Antioxidants (Basel) 2018, 7, 17. [Google Scholar] [CrossRef]
- Fisher-Wellman, K.; Bloomer, R.J. Acute exercise and oxidative stress: A 30 year history. Dyn Med. 2009, 8, 1. [Google Scholar] [CrossRef]
- Rahal, A.; Kumar, A.; Singh, V.; Yadav, B.; Tiwari, R.; Chakraborty, S.; Dhama, K. Oxidative stress, prooxidants, and antioxidants: The interplay. Biomed Res. Int. 2014, 2014, 761264. [Google Scholar] [CrossRef]
- Radak, Z.; Zhao, Z.; Koltai, E.; Ohno, H.; Atalay, M. Oxygen consumption and usage during physical exercise: The balance between oxidative stress and ROS-dependent adaptive signaling. Antioxid. Redox Signal. 2013, 18, 1208–1246. [Google Scholar] [CrossRef]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical markers of muscular damage. Clin. Chem. Lab. Med. 2010, 48, 757–767. [Google Scholar] [CrossRef]
- Ramos, D.; Martins, E.G.; Viana-Gomes, D.; Casimiro-Lopes, G.; Salerno, V.P. Biomarkers of oxidative stress and tissue damage released by muscle and liver after a single bout of swimming exercise. Appl. Physiol. Nutr. Metab. 2013, 38, 507–511. [Google Scholar] [CrossRef]
- Karakukcu, C.; Polat, Y.; Torun, Y.A.; Pac, A.K. The effects of acute and regular exercise on calcium, phosphorus and trace elements in young amateur boxers. Clin. Lab. 2013, 59, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Baygutalp, N.K.; Ozturk, N.; Bakan, E.; Kurt, N.; Gul, M.A.; Dorman, E.; Kiyici, F.; Kaynar, O.; Yazici, A.G. Acute effects of training on some biochemical analytes in professional boxers. Int. J. Med. Pharm. 2016, 4, 39–52. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Mean ± SD |
|---|---|
| Age (years) | 25.88 ± 3.27 |
| Weight (kg) | 69.88 ± 15.14 |
| Height (cm) | 174.5 ± 9.71 |
| BMI (kg/m2) | 22.68 ± 2.70 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kılıc, Y.; Cetin, H.N.; Sumlu, E.; Pektas, M.B.; Koca, H.B.; Akar, F. Effects of Boxing Matches on Metabolic, Hormonal, and Inflammatory Parameters in Male Elite Boxers. Medicina 2019, 55, 288. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060288
Kılıc Y, Cetin HN, Sumlu E, Pektas MB, Koca HB, Akar F. Effects of Boxing Matches on Metabolic, Hormonal, and Inflammatory Parameters in Male Elite Boxers. Medicina. 2019; 55(6):288. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060288
Chicago/Turabian StyleKılıc, Yakup, Hasan N. Cetin, Esra Sumlu, Mehmet B. Pektas, Halit B. Koca, and Fatma Akar. 2019. "Effects of Boxing Matches on Metabolic, Hormonal, and Inflammatory Parameters in Male Elite Boxers" Medicina 55, no. 6: 288. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060288