Use of Plasmapheresis and Immunosuppressants to Treat Diffuse Alveolar Hemorrhage in a Patient with Granulomatosis with Polyangiitis



Abstract
:1. Introduction
2. Case Presentation
- (A)
- Microscopic polyangiitis—this was difficult to differentiate on the basis of the clinical background, but a negative myeloperoxidase titer helped us to rule this out.
- (B)
- Eosinophilic granulomatosis with polyangiitis—this was difficult to differentiate on the basis of the clinical presentation, but this was ruled out considering the negative myeloperoxidase findings and a normal eosinophil count.
- (C)
- Drug-induced vasculitis—although this can have a similar presentation, a thorough history-taking ruled out this disease.
3. Discussion
- Nasal or oral inflammation (e.g., painful or painless oral ulcers or purulent or bloody nasal discharge).
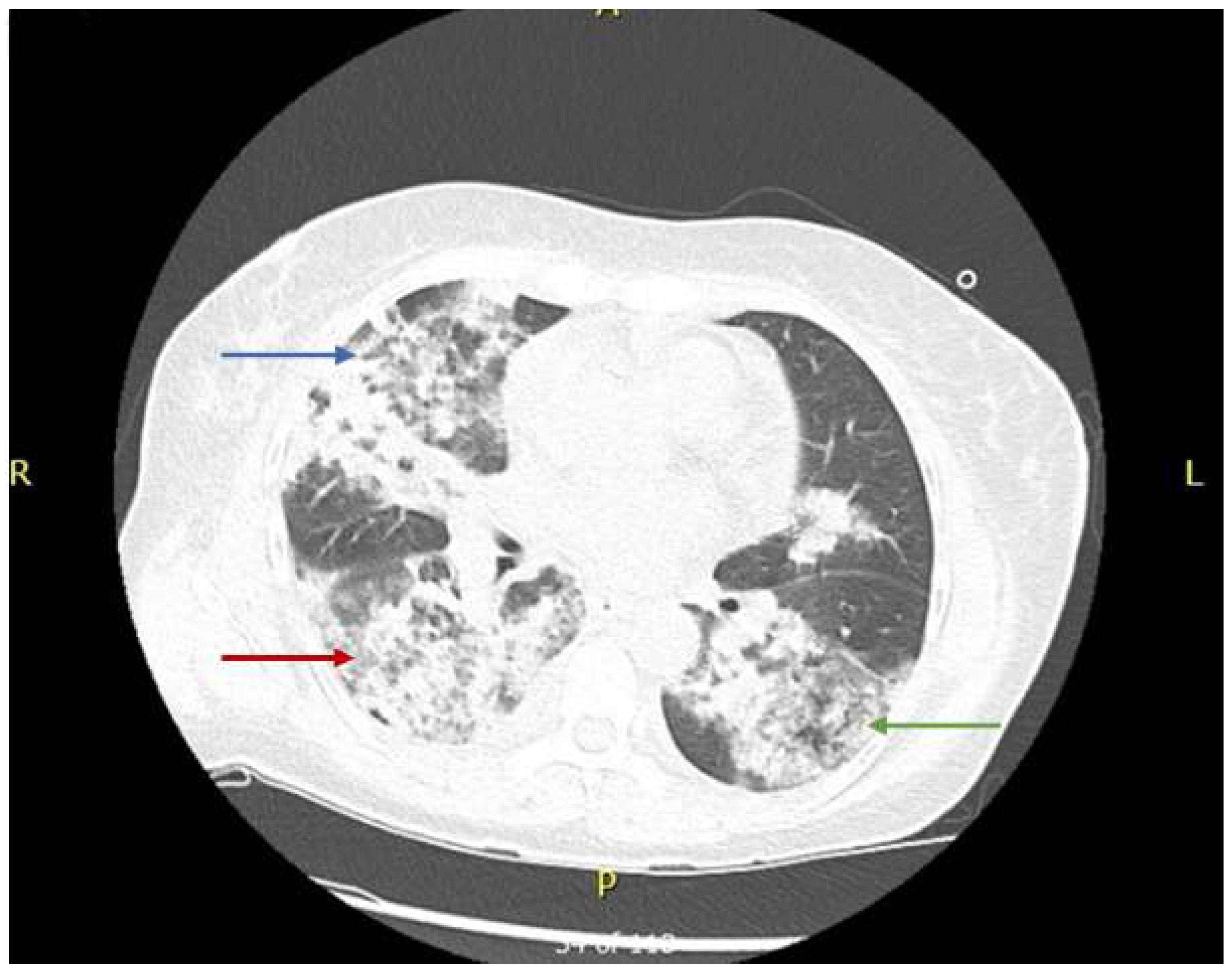
- Abnormal chest radiography scans showing nodules, fixed infiltrates, or cavities.
- Abnormal urine analysis (microscopic hematuria with or without red cell casts).
- Granulomatosis inflammation upon biopsy of an artery or perivascular area.
- Large-vessel vasculitis includes Takayasu and Giant cell arteritis.
- Medium-vessel vasculitis includes polyarteritis nodosa and Kawasaki disease.
- Small-vessel vasculitis includes AAV, MPA, GPA, EGPA, immune complex vasculitis, anti-glomerular basement membrane disease, cryoglobulinemic vasculitis, IgA vasculitis, and hypocomplementemia urticarial vasculitis.
- Variable-vessel vasculitis includes Behcet’s syndrome and Cogan’s syndrome.
- Single-organ vasculitis includes vasculitis in only one organ with no systemic manifestation.
- Vasculitis associated with systemic disease includes vasculitis secondary to systemic disease, comprising rheumatoid arthritis, lupus vasculitis, etc.
- Vasculitis associated with probable etiology, including hepatitis B, hepatitis C, and hydralazine.
- The absence of immune complex deposits, differentiating small vessel vasculitis from GPA, MPA, and EGPA.
- The presence of necrotizing vasculitis without granuloma, distinguishing MPA from EGPA and GPA.
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Comarmond, C.; Cacoub, P. Granulomatosis with Polyangiitis (Wegener): Clinical Aspects and Treatment. Autoimmun. Rev. 2014, 13, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Kubaisi, B.; Samra, A.K.; Foster, S.C. Granulomatosis with Polyangiitis (Wegener’s Disease): An Updated Review of Ocular Disease Manifestations. Intractable Rare Dis. Res. 2016, 5, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Ning, S.; Zhang, X.; Xu, C.; Dang, X.; Cheng, H.; Zhu, K.; Han, Y. Methylprednisolone and Plasmapheresis Are Effective for Life-Threatening Diffuse Alveolar Hemorrhage and Gastrointestinal Hemorrhage in Granulomatosis with Polyangiitis: A Case Report and Literature Review. Medicine (Baltimore). 2018, 97, e0592. [Google Scholar] [CrossRef] [PubMed]
- Yates, M.; Watts, R. ANCA-Associated Vasculitis. Clin. Med. (Lond.) 2017, 17, 60–64. [Google Scholar] [CrossRef] [PubMed]
- West, S.; Arulkumaran, N.; Ind, P.W.; Pusey, C.D. Diffuse Alveolar Haemorrhage in Anca-Associated Vasculitis. Intern Med. 2013, 52, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Kaya, H.; Yilmaz, S.; Sezgi, C.; Abakay, O.; Taylan, M.; Sen, H.; Demir, M.; Akkurt, M.Z.; Senyigit, M. Two Cases of Extrapulmonary Onset Granulomatosis with Polyangiitis Which Caused Diffuse Alveolar Haemorrhage. Respir. Med. Case Rep. 2014, 13, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Suresh, E. Diagnostic Approach to Patients with Suspected Vasculitis. Postgrad. Med. J. 2006, 82, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Specks, U. Diffuse Alveolar Hemorrhage Syndromes. Curr. Opin. Rheumatol. 2001, 13, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Vanoli, J.; Riva, M.; Vergnano, B.; D’Andrea, G.; L’Imperio, V.; Pozzi, M.R.; Grassi, G. Granulomatosis with Polyangiitis Presenting with Diffuse Alveolar Hemorrhage Requiring Extracorporeal Membrane Oxygenation with Rapid Multiorgan Relapse: A Case Report. Medicine (Baltimore). 2017, 96, e6024. [Google Scholar] [CrossRef] [PubMed]
- Frasca, G.M.; Zoumparidis, N.G.; Borgnino, L.G.; Neri, L.; Vangelista, A.; Bonomini, V. Plasma Exchange Treatment in Rapidly Progressive Glomerulonephritis Associated with Anti-Neutrophil Cytoplasmic Autoantibodies. Int. J. Artif. Organs. 1992, 15, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Cartin-Ceba, R.; Diaz-Caballero, L.; Al-Qadi, M.O.; Tryfon, S.; Fervenza, F.C.; Ytterberg, S.R.; Specks, U. Diffuse Alveolar Hemorrhage Secondary to Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: Predictors of Respiratory Failure and Clinical Outcomes. Arthritis Rheumatol. 2016, 68, 1467–1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, M.; Merkel, P.A.; Peh, C.A.; Szpirt, W.; Guillevin, L.; Pusey, C.D.; De Zoysa, J.; Ives, N.; Clark, W.F.; Quillen, K.; et al. Plasma Exchange and Glucocorticoid Dosing in the Treatment of Anti-Neutrophil Cytoplasm Antibody Associated Vasculitis (Pexivas): Protocol for a Randomized Controlled Trial. Trials 2013, 14, 73. [Google Scholar] [CrossRef] [PubMed]
- Buturovic-Ponikvar, J.; Pernat, A.M.; Ponikvar, R. Citrate Anticoagulation During Plasma Exchange in a Patient with Thrombotic Thrombocytopenic Purpura: Short Heparin-Free Hemodialysis Helps to Attenuate Citrate Load. Ther. Apher. Dial. 2005, 9, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Uechi, E.; Okada, M.; Fushimi, K. Effect of Plasma Exchange on in-Hospital Mortality in Patients with Pulmonary Hemorrhage Secondary to Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Propensity-Matched Analysis Using a Nationwide Administrative Database. PLoS ONE 2018, 13, e0196009. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Analyte | Baseline | Reference Range |
|---|---|---|
| Hematology | ||
| WBC | 21.8 K/mcL | 4.5–11.0 K/mcL |
| Hemoglobin | 5.8 gm/dL | 12.0–16.0 gm/dL |
| RBC | 2.10 M/mcL | 4.00–5.20 M/mcL |
| Platelet count | 356 K/uL | 550 K/uL |
| Neutrophils | 90.5% | 43.0–77.0% |
| Lymphocytes | 3.8% | 13.0–44.0% |
| Monocyte | 6.2% | 2.0–14.0% |
| Eosinophil | 0.1% | 0.0–6.0% |
| Basophil | 0.5% | 0.0–2.0% |
| MCV | 90.1 fl | 80.0–100.0 fl |
| MCH | 27.8 pg | 27.0–34.0 pg |
| MCHC | 30.8 gm/dL | 32.0–36.0 gm/dL |
| RDW | 17.4% | 10.3–14.5% |
| PT | 13.0 seconds | 10.0–13.0 seconds |
| aPTT | 27.4 seconds | 27.0–36.0 seconds |
| Metabolic panel | ||
| ALT | 7 U/L | 7–35 U/L |
| AST | 11 U/L | 10–35 U/L |
| Total Bilirubin | 0.3 mg/dL | 0.1–1.2 mg/dL |
| BNP | 616 pg/mL | 1–100 pg/mL |
| C-reactive protein | 178.3 mg/L | 0.0–1.0 mg/L |
| ESR | 116 mm/hr | 0–20 mm/hr |
| Creatinine | 8.83 mg/dL | 0.40–1.60 mg/dL |
| BUN | 70 mg/dL | 8–22 mg/dL |
| e-GFR | 5 ml/min/1.73 m2 | 90–120 ml/min/1.73 m2 |
| Phosphorus | 7.4 mg/dL | 2.5–4.9 mg/dL |
| Calcium | 8.3 | 8.5–10.5 mg/dL |
| Sodium | 136 mEq/L | 136–146 mEq/L |
| Vitamin D 25- Hydroxy | 22.6 ng/mL | 30.0–100.0 ng/mL |
| PTH | 160.5 pg/mL | 10.0–65.0 pg/mL |
| Arterial Blood Gases | ||
| pH | 7.46 | 7.320–7.420 |
| pCO2 | 31.2 mmHg | 38.0–50.0 mmHg |
| HCO3 | 23.6 mmol/L | 22.0–28.0 mmol/L |
| Anion gap | 17 mmol/L | 2–11 mmol/L |
| Lactate | 1.0 mmol/L | 0.0–2.2 mmol/L |
| Culture and sensitivity | ||
| Sputum AFB | Negative in three samples | Negative |
| Stool culture | Negative | Negative |
| Urine culture | Negative | Negative |
| Blood culture | Negative | Negative |
| Analyte | Results |
|---|---|
| Appearance | Cloudy (Reference: clear) |
| Color | Yellow (Reference: yellow) |
| Urine pH | 6.0 (Reference: 5.0–7.5) |
| Specific gravity | 1.016 (Reference: 1.005–1.030) |
| Bilirubin | Negative (Reference: negative) |
| Ketones | Negative (Reference: negative) |
| Glucose | Negative (Reference: negative) |
| Blood | Large (Reference: negative) |
| Protein | 1000 mg/dL (Reference: negative mg/dL) |
| Urobilinogen | 1.0 (Reference: 0.2–1.0) |
| Nitrite | Negative (Reference: negative) |
| Leukocyte esterase | Negative (Reference: negative) |
| White blood cells urine | >50 HPF (Reference: 0–4 HPF) |
| Red blood cells urine | <50 HPF (Reference: 0–3 HPF) |
| Urine bacteria | Negative (Reference: negative) |
| Squamous epithelial cells | 0–4 HPF (Reference: 0–4 HPF) |
| Casts | None (Reference: no cast) |
| Analyte | Result | Reference |
|---|---|---|
| ANA antibody | 1:160 | 1:180 |
| ANA pattern | Homogenous | |
| Anti-GBM antibodies | Negative (<0.2 U) | Negative: <1.0 U Positive: >1.0 U |
| C-ANCA | Positive (1:320 titer) | |
| Proteinase-3 antibody | Positive (>150.0 units) | Negative: <20 units Diffusely positive: 21.0–30.0 units Positive: >30 units |
| Myeloperoxidase antibody | Negative (5.1 units) | Negative: <20 units Diffusely positive: 21.0–30.0 units Positive: >30.0 units |
| Anti-U1RNP Antibody | Negative (0.4 AI) | Negative: <1.0 AI Positive: ≥1.0 AI |
| Anti SCL-70 | Negative (<0.2 AI) | Positive: ≥1.0 AI |
| ASO | Negative | |
| Anti-DsDNA | Negative (<12 IU/mL) | Positive: >75 IU/mL |
| Hepatitis C Antibody | Non-reactive | |
| Hepatitis B Antibody | Non-reactive (<10 mIU/mL) | Reactive: ≥10 mIU/mL |
| C3 | 113 mg/dL | 81–157 mg/dL |
| C4 | 25 mg/dL | 13–39 mg/dL |
| Rheumatoid factor | 22 IU/mL | 0–13 IU/mL |
| Anti-SS-A-AB(RO) | Negative; <0.2 AI | Negative: <1.0 AI Positive: >1.0 AI |
| Cyclic Citrullinated C-Peptide Ab | <8 U | Negative: ≤39 U Positive: >40 U |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sattar, Y.; Susheela, A.T.; Ullah, W.; Usman, N.; Zafrullah, F. Use of Plasmapheresis and Immunosuppressants to Treat Diffuse Alveolar Hemorrhage in a Patient with Granulomatosis with Polyangiitis. Medicina 2019, 55, 378. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55070378
Sattar Y, Susheela AT, Ullah W, Usman N, Zafrullah F. Use of Plasmapheresis and Immunosuppressants to Treat Diffuse Alveolar Hemorrhage in a Patient with Granulomatosis with Polyangiitis. Medicina. 2019; 55(7):378. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55070378
Chicago/Turabian StyleSattar, Yasar, Ammu Thampi Susheela, Waqas Ullah, Norina Usman, and Fnu Zafrullah. 2019. "Use of Plasmapheresis and Immunosuppressants to Treat Diffuse Alveolar Hemorrhage in a Patient with Granulomatosis with Polyangiitis" Medicina 55, no. 7: 378. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55070378