The Lipid Paradox Among Acute Ischemic Stroke Patients-A Retrospective Study of Outcomes and Complications

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
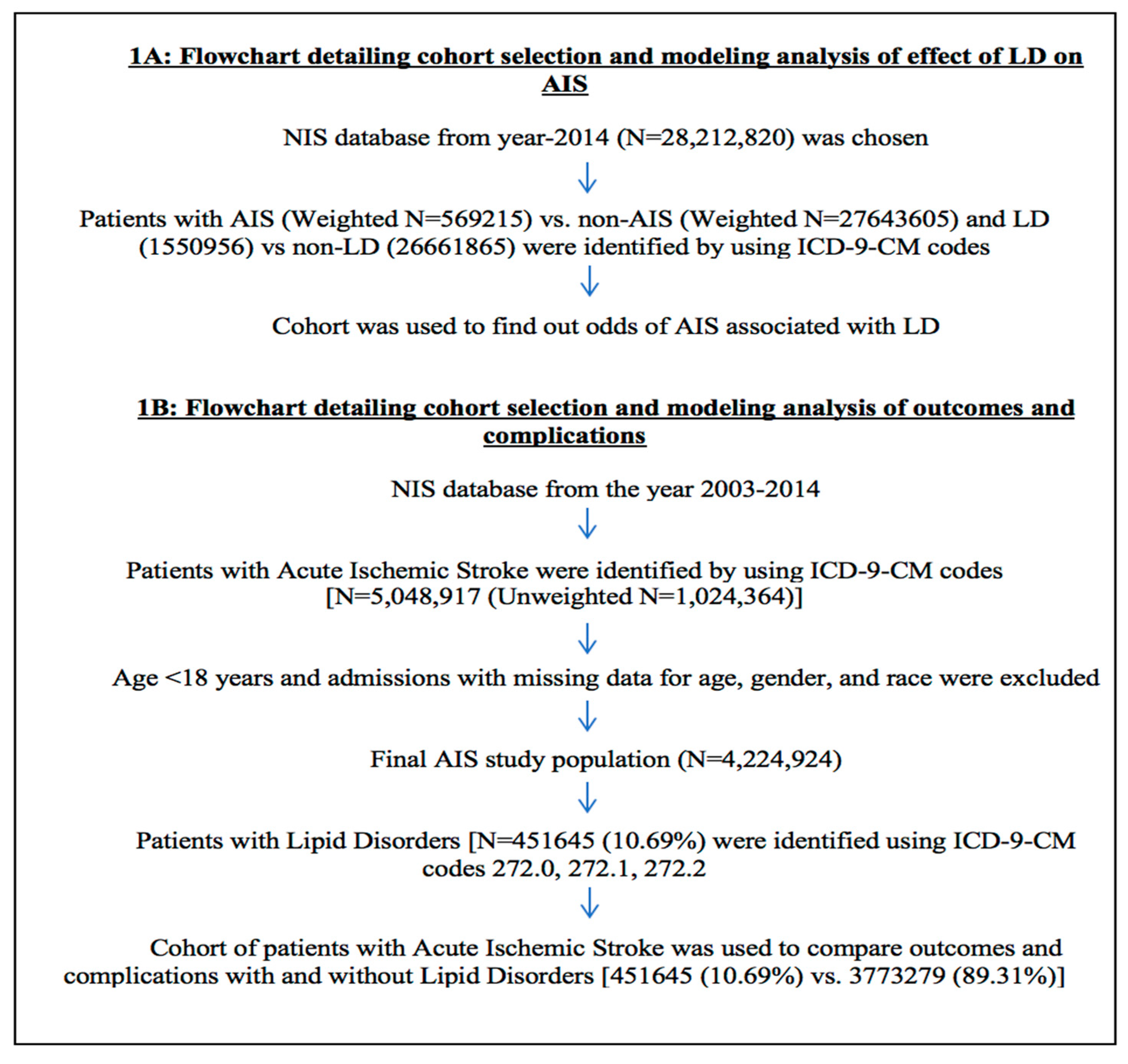
2.1. Study Population
2.2. Patient and Hospital Characteristics
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. LDs and AIS Amongst Year-2014 Hospitalizations
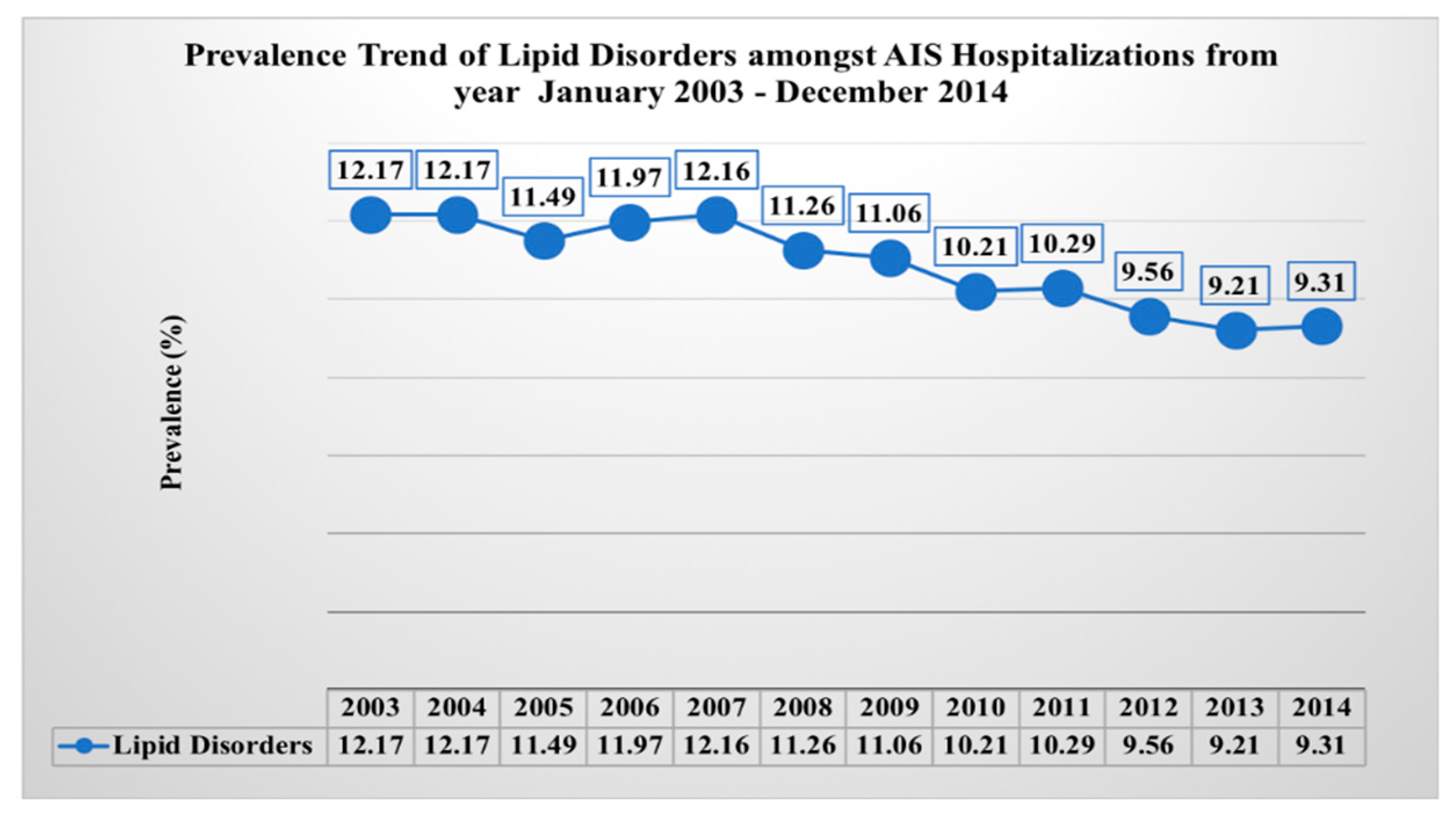
3.2. LDs and Post-AIS Outcomes Amongst AIS Population from Year 2003–2014
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Tong, X.; Schieb, L.; Vaughan, A.; Gillespie, C.; Wiltz, J.L.; King, S.C.; Odom, E.; Merritt, R.; Hong, Y.; et al. Vital Signs: Recent Trends in Stroke Death Rates—United States, 2000–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Klag, M.J.; Ford, D.E.; Mead, L.A.; He, J.; Whelton, P.K.; Liang, K.Y.; Levine, D.M. Serum cholesterol in young men and subsequent cardiovascular disease. N. Engl. J. Med. 1993, 328, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Castelli, W.P.; Anderson, K.; Wilson, P.W.; Levy, D. Lipids and risk of coronary heart disease. The Framingham Study. Ann. Epidemiol. 1992, 2, 23–28. [Google Scholar] [CrossRef]
- Hankey, G.J.; Warlow, C.P. Treatment and secondary prevention of stroke: Evidence, costs, and effects on individuals and populations. Lancet 1999, 354, 1457–1463. [Google Scholar] [CrossRef]
- Prospective Studies Collaboration. Cholesterol, diastolic blood pressure, and stroke: 13,000 strokes in 450,000 people in 45 prospective cohorts. Lancet 1995, 346, 1647–1653. [Google Scholar] [CrossRef]
- Landau, W.M. Is cholesterol a risk factor for stroke?: No. Arch. Neurol. 1999, 56, 1521–1524. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P. Hypercholesterolemia, lipid-lowering agents, and the risk for brain infarction. Neurology 2001, 57, S35–S44. [Google Scholar] [CrossRef] [PubMed]
- Wolf, P.A.; Kannel, W.B.; Verter, J. Current status of risk factors for stroke. Neurol. Clin. 1983, 1, 317–343. [Google Scholar] [CrossRef]
- Kagan, A.; Popper, J.S.; Rhoads, G.G. Factors related to stroke incidence in Hawaii Japanese men. The Honolulu Heart Study. Stroke 1980, 11, 14–21. [Google Scholar] [CrossRef]
- Iso, H.; Jacobs, D.R., Jr.; Wentworth, D.; Neaton, J.D.; Cohen, J.D. Serum cholesterol levels and six-year mortality from stroke in 350,977 men screened for the multiple risk factor intervention trial. N. Engl. J. Med. 1989, 320, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Benfante, R.; Yano, K.; Hwang, L.J.; Curb, J.D.; Kagan, A.; Ross, W. Elevated serum cholesterol is a risk factor for both coronary heart disease and thromboembolic stroke in Hawaiian Japanese men. Implications of shared risk. Stroke 1994, 25, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Schulz, U.G.; Rothwell, P.M. Differences in vascular risk factors between etiological subtypes of ischemic stroke: Importance of population-based studies. Stroke 2003, 34, 2050–2059. [Google Scholar] [CrossRef] [PubMed]
- Tirschwell, D.L.; Smith, N.L.; Heckbert, S.R.; Lemaitre, R.N.; Longstreth, W.T., Jr.; Psaty, B.M. Association of cholesterol with stroke risk varies in stroke subtypes and patient subgroups. Neurology 2004, 63, 1868–1875. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P.; Labreuche, J.; Elbaz, A.; Touboul, P.J.; Driss, F.; Jaillard, A.; Bruckert, E. Blood lipids in brain infarction subtypes. Cereb. Dis. 2006, 22, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Eastern Stroke and Coronary Heart Disease Collaborative Research Group. Blood pressure, cholesterol, and stroke in eastern Asia. Lancet 1998, 352, 1801–1807. [Google Scholar] [CrossRef]
- Dyker, A.G.; Weir, C.J.; Lees, K.R. Influence of cholesterol on survival after stroke: Retrospective study. BMJ 1997, 314, 1584–1588. [Google Scholar] [CrossRef] [PubMed]
- Vauthey, C.; de Freitas, G.R.; van Melle, G.; Devuyst, G.; Bogousslavsky, J. Better outcome after stroke with higher serum cholesterol levels. Neurology 2000, 54, 1944–1949. [Google Scholar] [CrossRef]
- Zuliani, G.; Cherubini, A.; Atti, A.R.; Ble, A.; Vavalle, C.; Di Todaro, F.; Benedetti, C.; Volpato, S.; Marinescu, M.G.; Senin, U.; et al. Low cholesterol levels are associated with short-term mortality in older patients with ischemic stroke. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 293–297. [Google Scholar] [CrossRef]
- Ni Chroinin, D.; Callaly, E.L.; Duggan, J.; Merwick, A.; Hannon, N.; Sheehan, O.; Marnane, M.; Horgan, G.; Williams, E.B.; Harris, D.; et al. Association between acute statin therapy, survival, and improved functional outcome after ischemic stroke: The North Dublin Population Stroke Study. Stroke 2011, 42, 1021–1029. [Google Scholar] [CrossRef]
- Tuttolomondo, A.; Di Raimondo, D.; Di Sciacca, R.; Pedone, C.; La Placa, S.; Arnao, V.; Pinto, A.; Licata, G. Effects of clinical and laboratory variables at admission and of in-hospital treatment with cardiovascular drugs on short term prognosis of ischemic stroke. The GIFA study. Nutr. Metab. Cardiovasc. Dis. NMCD 2013, 23, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.S.; Christensen, R.H.; Kammersgaard, L.P.; Andersen, K.K. Higher total serum cholesterol levels are associated with less severe strokes and lower all-cause mortality: Ten-year follow-up of ischemic strokes in the Copenhagen Stroke Study. Stroke 2007, 38, 2646–2651. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, H.S.; Nakayama, H.; Reith, J.; Raaschou, H.O.; Olsen, T.S. Acute stroke with atrial fibrillation. The Copenhagen Stroke Study. Stroke 1996, 27, 1765–1769. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.J.; Wolf, P.A.; Kelly-Hayes, M.; Beiser, A.S.; Kase, C.S.; Benjamin, E.J.; D’Agostino, R.B. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996, 27, 1760–1764. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Leveille, S.G.; Corti, M.C.; Harris, T.B.; Guralnik, J.M. The value of serum albumin and high-density lipoprotein cholesterol in defining mortality risk in older persons with low serum cholesterol. J. Am. Geriatr. Soc. 2001, 49, 1142–1147. [Google Scholar] [CrossRef] [PubMed]
- Birman-Deych, E.; Waterman, A.D.; Yan, Y.; Nilasena, D.S.; Radford, M.J.; Gage, B.F. Accuracy of ICD-9-CM codes for identifying cardiovascular and stroke risk factors. Med. Care 2005, 43, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Oake, J.; Aref-Eshghi, E.; Godwin, M.; Collins, K.; Aubrey-Bassler, K.; Duke, P.; Mahdavian, M.; Asghari, S. Using Electronic Medical Record to Identify Patients With Dyslipidemia in Primary Care Settings: International Classification of Disease Code Matters From One Region to a National Database. Biomed. Inform. Insights 2017, 9, 1178222616685880. [Google Scholar] [CrossRef]
- Markaki, I.; Nilsson, U.; Kostulas, K.; Sjostrand, C. High cholesterol levels are associated with improved long-term survival after acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 2014, 23, e47–e53. [Google Scholar] [CrossRef] [PubMed]
- Koton, S.; Molshatzki, N.; Bornstein, N.M.; Tanne, D. Low cholesterol, statins and outcomes in patients with first-ever acute ischemic stroke. Cerebrovasc. Dis. 2012, 34, 213–220. [Google Scholar] [CrossRef] [PubMed]
- McCormick, P.J.; Lin, H.M.; Deiner, S.G.; Levin, M.A. Validation of the All Patient Refined Diagnosis Related Group (APR-DRG) Risk of Mortality and Severity of Illness Modifiers as a Measure of Perioperative Risk. J. Med. Syst. 2018, 42, 81. [Google Scholar] [CrossRef] [PubMed]
- Baram, D.; Daroowalla, F.; Garcia, R.; Zhang, G.; Chen, J.J.; Healy, E.; Riaz, S.A.; Richman, P. Use of the All Patient Refined-Diagnosis Related Group (APR-DRG) Risk of Mortality Score as a Severity Adjustor in the Medical ICU. Clin. Med. Circ. Respir. Pul. Med. 2008, 2, 19–25. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| LD | No LD | Total | p Value | |
|---|---|---|---|---|
| AIS | 50,005 (3.22%) | 519,210 (1.95%) | 569,215 | <0.0001 |
| No AIS | 1,500,951 (96.78%) | 26,142,654 (98.05%) | 27,643,605 | |
| 1,550,956 | 26,661,864 | 28,212,820 |
| OR | 95% Confidence Limits | p Value | ||
|---|---|---|---|---|
| LL | UL | |||
| No Lipid Disorders | Reference | |||
| Lipid Disorders | 1.18 | 1.15 | 1.20 | <0.0001 |
| Demographics of Patients | ||||
| Age (Years) | 1.02 | 1.02 | 1.02 | <0.0001 |
| Gender | ||||
| Female | Reference | |||
| Male | 1.00 | 0.99 | 1.01 | 0.8272 |
| Race | ||||
| White | Reference | |||
| African American | 1.17 | 1.15 | 1.19 | <0.0001 |
| Hispanic | 0.90 | 0.88 | 0.93 | <0.0001 |
| Asian or Pacific Islander | 1.12 | 1.07 | 1.16 | <0.0001 |
| Native American | 0.92 | 0.84 | 1.01 | 0.0793 |
| Characteristics of Patients | ||||
| Median Household Income Category for patient’s Zip code * | ||||
| 0–25th percentile | Reference | |||
| 26–50th percentile | 1.03 | 1.01 | 1.04 | 0.0038 |
| 51–75th percentile | 1.02 | 1.01 | 1.04 | 0.0127 |
| 76–100th percentile | 1.01 | 0.99 | 1.03 | 0.2592 |
| Primary Payer | ||||
| Medicare | Reference | |||
| Medicaid | 1.04 | 1.01 | 1.07 | 0.0025 |
| Private Insurance | 1.30 | 1.27 | 1.32 | <0.0001 |
| Other/Self-pay/No charge | 1.46 | 1.42 | 1.51 | <0.0001 |
| Admission type | ||||
| Non-elective | Reference | |||
| Elective | 0.29 | 0.28 | 0.30 | <0.0001 |
| Admission day | ||||
| Weekday | Reference | |||
| Weekend | 1.13 | 1.11 | 1.15 | <0.0001 |
| Characteristics of Hospitals | ||||
| Bed-size of hospital † | ||||
| Small | Reference | |||
| Medium | 1.11 | 1.09 | 1.13 | <0.0001 |
| Large | 1.15 | 1.13 | 1.17 | <0.0001 |
| Hospital Location & Teaching Status | ||||
| Rural | Reference | |||
| Urban Non-teaching | 1.04 | 1.02 | 1.07 | 0.0019 |
| Urban Teaching | 1.14 | 1.12 | 1.17 | <0.0001 |
| Hospital Region | ||||
| Northeast | Reference | |||
| Midwest | 1.14 | 1.12 | 1.17 | <0.0001 |
| South | 1.23 | 1.21 | 1.26 | <0.0001 |
| West | 1.26 | 1.24 | 1.29 | <0.0001 |
| Comorbidities of Patients | ||||
| Diabetes Mellites | 0.49 | 0.49 | 0.50 | <0.0001 |
| Hypertension | 1.73 | 1.70 | 1.76 | <0.0001 |
| Obesity | 0.83 | 0.81 | 0.84 | <0.0001 |
| Drug Abuse/Dependence | 1.03 | 0.99 | 1.07 | 0.1261 |
| Current Alcohol Dependence | 0.91 | 0.88 | 0.94 | <0.0001 |
| Past History of Alcohol | 0.83 | 0.70 | 0.98 | 0.0265 |
| Current Smoker | 1.30 | 1.27 | 1.32 | <0.0001 |
| Past History of Smoking | 0.73 | 0.72 | 0.75 | <0.0001 |
| Acquired immune deficiency syndrome | 0.12 | 0.10 | 0.13 | <0.0001 |
| Renal Failure | 0.27 | 0.27 | 0.28 | <0.0001 |
| Atrial Fibrillation | 1.13 | 1.11 | 1.14 | <0.0001 |
| Hemorrhagic Stroke | 2.49 | 2.39 | 2.60 | <0.0001 |
| History of TIA/Stroke | 1.56 | 1.53 | 1.59 | <0.0001 |
| Deyo’s Charlson Comorbidity Index (CCI) | ||||
| 1 | Reference | |||
| 2 | 1.86 | 1.83 | 1.89 | <0.0001 |
| 3 | 4.39 | 4.30 | 4.48 | <0.0001 |
| 4 | 7.39 | 7.22 | 7.57 | <0.0001 |
| ≥5 | 9.38 | 9.18 | 9.58 | <0.0001 |
| Area under the ROC curve/c-index | 0.882 | |||
| LDs | Non-LDs | Total | p Value | |
|---|---|---|---|---|
| AIS (%) | 451,645 (10.69) | 3,773,279 (89.31) | 446,446 (100) | <0.0001 |
| Demographics of Patients | ||||
| Mean Age ± Standard Error (Years) | 70 ± 0.04 | 71 ± 0.01 | <0.0001 | |
| Gender (%) | <0.0001 | |||
| Female | 222,900 (49.35) | 1,767,703 (46.85) | 1,990,602 (47.12) | |
| Male | 228,746 (50.65) | 2,005,507 (53.15) | 2,234,253 (52.88) | |
| Race (%) | <0.0001 | |||
| White | 318,230 (72.36) | 2,667,898 (72.54) | 2,986,128 (72.53) | |
| African American | 70,736 (16.08) | 620,354 (16.87) | 691,090 (16.78) | |
| Hispanic | 35,048 (7.97) | 276,724 (7.52) | 311,772 (7.57) | |
| Asian or Pacific Islander | 13,944 (3.17) | 94,600 (2.57) | 108,544 (2.64) | |
| Native American | 1832 (0.42) | 18,001 (0.49) | 19,833 (0.48) | |
| Characteristics of Patients | ||||
| Median Household Income Category for patient’s Zip code (%) * | <0.0001 | |||
| 0–25th percentile | 116,887 (26.40) | 1,125,147 (30.48) | 1,242,034 (30.04) | |
| 26–50th percentile | 105,237 (23.77) | 959,992 (26) | 1,065,230 (25.76) | |
| 51–75th percentile | 108,373 (24.48) | 855,077 (23.16) | 963,450 (23.30) | |
| 76–100th percentile | 112,216 (25.35) | 751,704 (20.36) | 863,920 (20.89) | |
| Primary Payer (%) | <0.0001 | |||
| Medicare | 290,927 (64.49) | 2,532,866 (67.25) | 2,823,793 (66.95) | |
| Medicaid | 28,514 (6.32) | 257,590 (6.84) | 286,104 (6.78) | |
| Private Insurance | 101,488 (22.50) | 697,741 (18.53) | 799,229 (18.95) | |
| Other/Self-pay/No charge | 30,179 (6.69) | 278,274 (7.39) | 308,453 (7.31) | |
| Admission type (%) | 0.0002 | |||
| Non-elective | 433,571 (96.20) | 3,589,986 (95.35) | 4,023,557 (95.44) | |
| Elective | 17,130 (3.80) | 175,254 (4.65) | 192,384 (4.56) | |
| Admission day (%) | 0.0026 | |||
| Weekday | 337,044 (74.63) | 2,808,044 (74.42) | 3,145,089 (74.44) | |
| Weekend | 114,601 (25.37) | 965,234 (25.58) | 1,079,835 (25.56) | |
| Characteristics of Hospitals | ||||
| Bed-size of hospital (%) † | <0.0001 | |||
| Small | 50,403 (11.19) | 448,170 (11.93) | 498,573 (11.85) | |
| Medium | 115,506 (25.63) | 963,139 (25.64) | 1,078,644 (25.64) | |
| Large | 284,703 (63.18) | 2,345,109 (62.43) | 2,629,813 (62.51) | |
| Hospital Location & Teaching Status (%) | <0.0001 | |||
| Rural | 41,205 (9.14) | 453,884 (12.08) | 495,089 (11.77) | |
| Urban Non-teaching | 200,443 (44.48) | 1,582,234 (42.12) | 1,782,676 (42.37) | |
| Urban Teaching | 208,964 (46.37) | 1,720,301 (45.80) | 1,929,265 (45.86) | |
| Hospital Region (%) | <0.0001 | |||
| Northeast | 117,433 (26) | 778,923 (20.64) | 896,356 (21.22) | |
| Midwest | 74,569 (16.51) | 655,617 (17.38) | 730,186 (17.28) | |
| South | 179,036 (39.64) | 1,631,363 (43.23) | 1,810,399 (42.85) | |
| West | 80,608 (17.85) | 707,375 (18.75) | 787,983 (18.65) | |
| Comorbidities of Patients (%) | <0.0001 | |||
| Diabetes | 179,812 (40.02) | 1,258,315 (33.50) | 1,438,128 (34.20) | |
| Drug abuse | 6735 (1.50) | 82,624 (2.20) | 89,359 (2.12) | |
| Obesity | 44,246 (9.85) | 286,635 (7.63) | 330,881 (7.81) | |
| Hypertension | 388,411 (86.44) | 2,954,771 (78.66) | 3,343,182 (79.50) | |
| Renal failure | 45,347 (10.09) | 445,605 (11.86) | 490,952 (11.67) | |
| Acquired immune deficiency syndrome | 457 (0.10) | 7606 (0.20) | 8063 (0.19) | |
| Deyo’s Charlson Comorbidity Index (CCI) | <0.0001 | |||
| 1 | 126,878 (28.09) | 1,059,432 (28.08) | 1,186,309 (28.08) | |
| 2 | 110,148 (24.39) | 831,212 (22.03) | 941,360 (22.38) | |
| 3 | 93,546 (20.71) | 816,642 (21.64) | 910,188 (21.54) | |
| 4 | 65,014 (14.39) | 537,270 (14.24) | 602,284 (14.26) | |
| ≥5 | 56,061 (12.41) | 528,722 (14.01) | 584,783 (13.84) | |
| LDs | No-LDs | Total | p Value | |
|---|---|---|---|---|
| Post-AIS Outcomes | ||||
| All Cause in Hospital Mortality (%) | 13,218 (2.93) | 206,346 (5.48) | 219,564 (5.21) | <0.0001 |
| Discharge Disposition (%) | <0.0001 | |||
| Routine/Home | 187,568 (43.14) | 1,299,013 (36.81) | 1,486,581 (37.50) | |
| Transfer to Short-term Hospital | 12,474 (2.87) | 114,476 (3.24) | 126,950 (3.20) | |
| Transfer to SNF/ICF/Another Type of Facility | 175,573 (40.38) | 1,639,408 (46.45) | 1,814,981 (45.79) | |
| Home Health Care | 59,159 (13.61) | 476,296 (13.50) | 535,455 (13.51) | |
| Discharge other than Home (%) | 247,206 (56.86) | 2,230,180 (63.19) | 2,477,386 (62.50) | <0.0001 |
| APR-DRG Severity/Loss of Function (%) | <0.0001 | |||
| Minor loss of function | 58,647 (13.47) | 401,109 (11.32) | 459,756 (11.55) | |
| Moderate loss of function | 246,559 (56.61) | 1,805,199 (50.93) | 2,051,758 (51.55) | |
| Major loss of function | 114,404 (26.27) | 1,106,595 (31.22) | 1,220,999 (30.68) | |
| Severe loss of function | 15,899 (3.65) | 231,623 (6.53) | 247,522 (6.22) | |
| Major/Severe Loss of Function/Severity (%) | 130,303 (29.92) | 1,338,218 (37.75) | 1,468,521 (36.9) | |
| APR-DRG Likelihood of Death (%) | <0.0001 | |||
| Minor likelihood of death | 171,426 (39.36) | 1,124,229 (31.72) | 1,295,655 (32.55) | |
| Moderate likelihood of death | 195,248 (44.83) | 1,644,501 (46.40) | 1,839,749 (46.22) | |
| Major likelihood of death | 54,708 (12.56) | 579,523 (16.35) | 634,231 (15.94) | |
| Severe likelihood of death | 14,128 (3.24) | 196,272 (5.54) | 210,401 (5.29) | |
| Major/Extreme likelihood of death (%) | 68,836 (15.8) | 775,795 (21.89) | 844,632 (21.23) | |
| Post-AIS Complications | ||||
| Post-stroke early epilepsy | 21,149 (4.68) | 231,487 (6.13) | 252,636 (5.98) | <0.0001 |
| Stroke associated pneumonia | 9616 (2.13) | 139,553 (3.70) | 149,169 (3.53) | <0.0001 |
| Hemorrhagic Transformation | 5642 (1.25) | 64,576 (1.71) | 70,218 (1.66) | <0.0001 |
| Upper gastro-intestinal bleeding | 1477 (0.33) | 17,152 (0.45) | 18,629 (0.44) | <0.0001 |
| Length of Stay ± SE (Days) | 4.83 ± 0.02 | 5.43 ± 0.01 | <0.0001 | |
| Cost of Hospitalization ± SE ($) | 34,604 ± 154 | 38,547 ± 62.04 | <0.0001 | |
| Odds Ratio | 95% Confidence Interval | p Value | Area under the ROC Curve/c-Index | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| Model 1: All cause in-hospital Mortality | ||||
| 0.66 | 0.62 | 0.69 | <0.0001 | 0.76 |
| Model 2: Discharge Disposition (Home vs. no-Home) | ||||
| 0.83 | 0.82 | 0.85 | <0.0001 | 0.76 |
| Model 3: APR-DRG loss of function (major/severe vs. minor/moderate) | ||||
| 0.80 | 0.79 | 0.82 | <0.0001 | 0.82 |
| Model 4: APR-DRG risk of death (major/severe likelihood vs. minor/moderate likelihood) | ||||
| 0.77 | 0.75 | 0.79 | <0.0001 | 0.81 |
| Model 5: Post Stroke Early Epilepsy | ||||
| 0.89 | 0.8 | 0.86 | <0.0001 | 0.65 |
| Model 6: Stroke Associated Pneumonia | ||||
| 0.75 | 0.71 | 0.80 | <0.0001 | 0.8 |
| Model 7: Upper GI Bleeding | ||||
| 0.85 | 0.73 | 0.99 | <0.0001 | 0.69 |
| Model 8: Hemorrhagic Transformation | ||||
| 0.82 | 0.75 | 0.89 | <0.0001 | 0.78 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, U.; Malik, P.; Dave, M.; DeMasi, M.S.; Lunagariya, A.; Jani, V.B.; Dhamoon, M.S. The Lipid Paradox Among Acute Ischemic Stroke Patients-A Retrospective Study of Outcomes and Complications. Medicina 2019, 55, 475. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080475
Patel U, Malik P, Dave M, DeMasi MS, Lunagariya A, Jani VB, Dhamoon MS. The Lipid Paradox Among Acute Ischemic Stroke Patients-A Retrospective Study of Outcomes and Complications. Medicina. 2019; 55(8):475. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080475
Chicago/Turabian StylePatel, Urvish, Preeti Malik, Mihir Dave, Matthew S. DeMasi, Abhishek Lunagariya, Vishal B. Jani, and Mandip S. Dhamoon. 2019. "The Lipid Paradox Among Acute Ischemic Stroke Patients-A Retrospective Study of Outcomes and Complications" Medicina 55, no. 8: 475. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080475