Transjejunal Laparoscopic Assisted ERCP in a Patient with Roux-en-Y Hepaticojejunostomy

 ,
,
Abstract
:1. Introduction
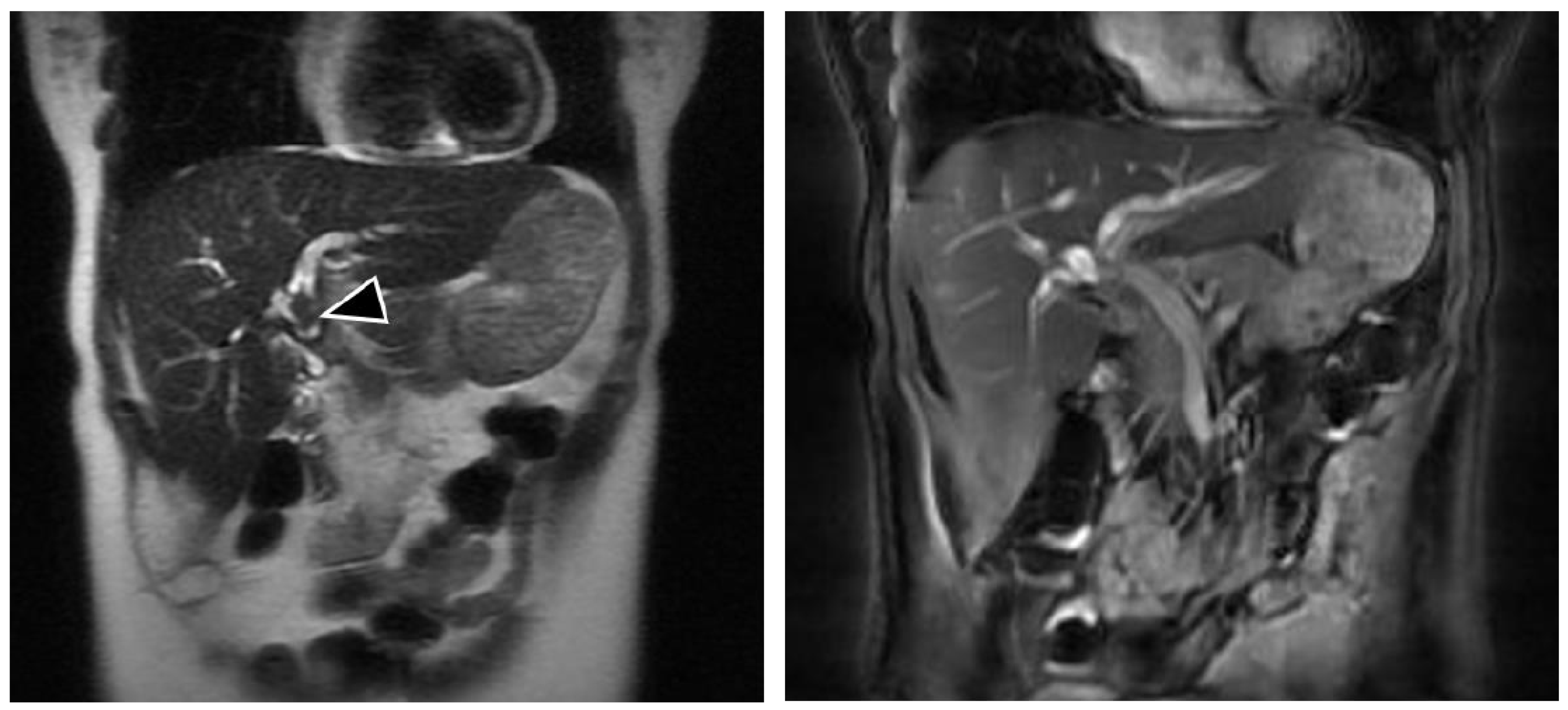
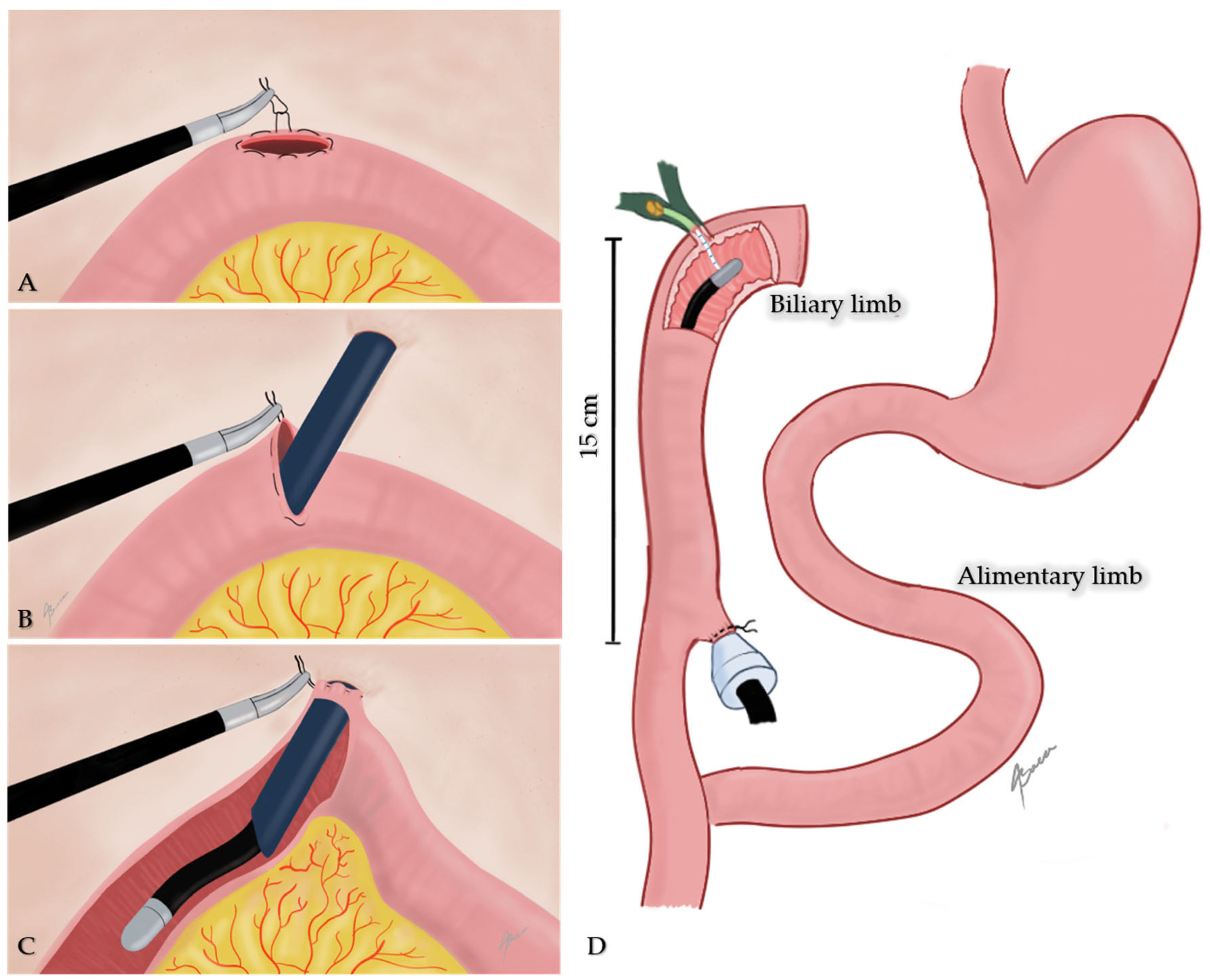
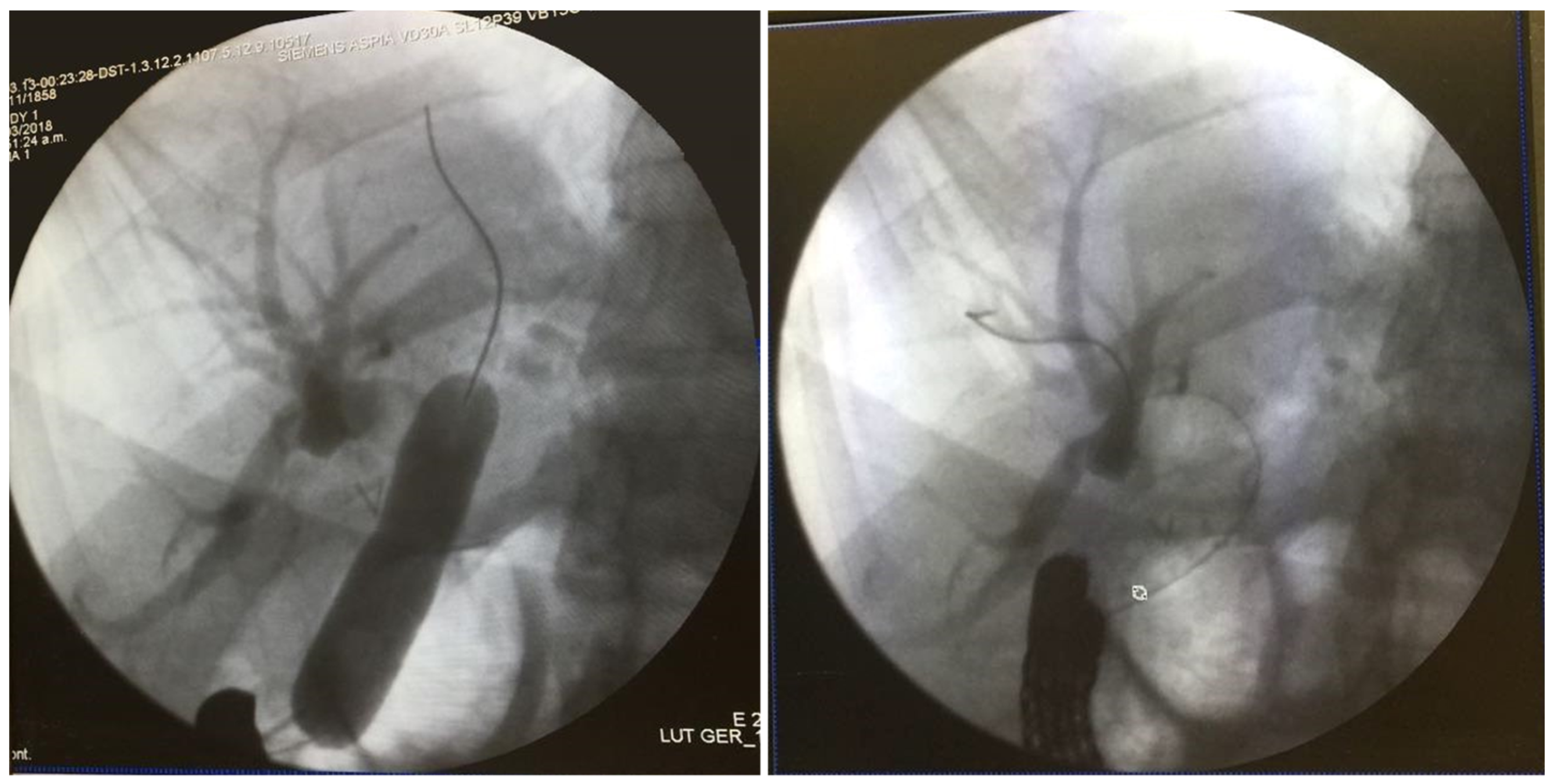
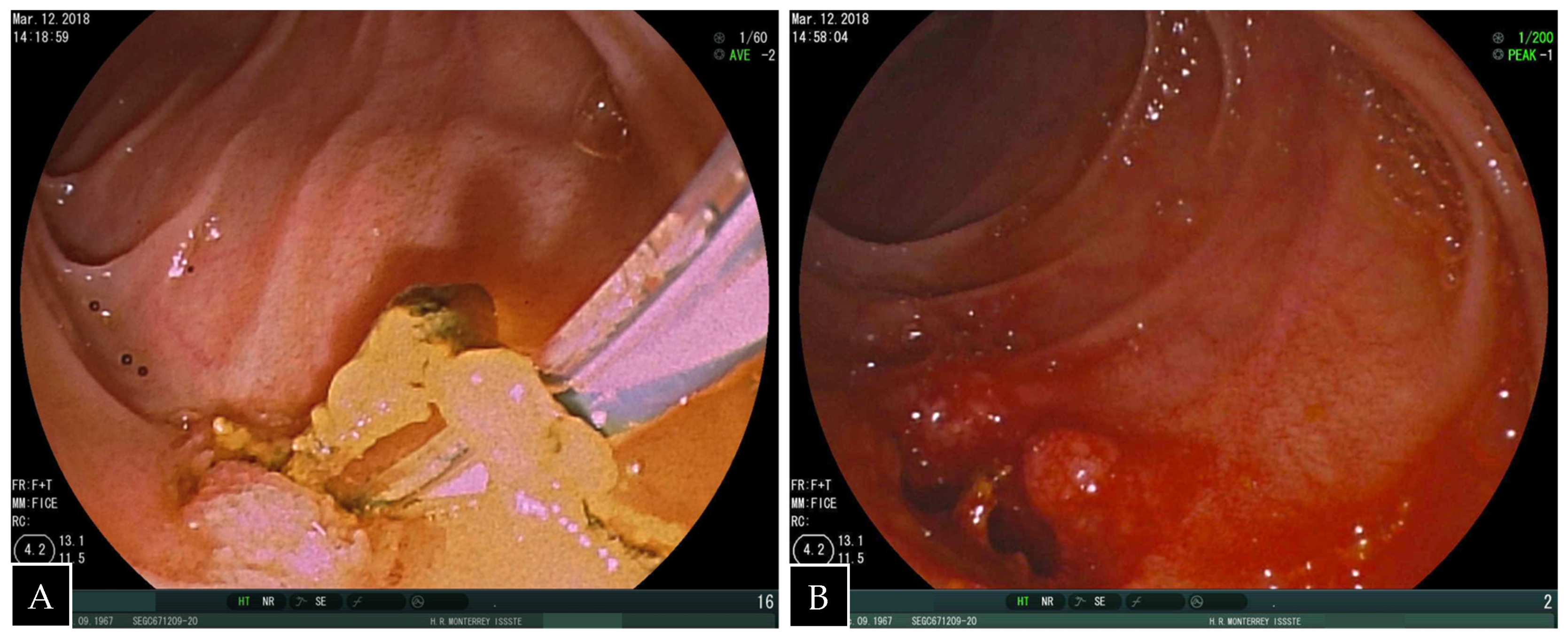
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sultan, A.M.; Elshobary, M.M.; Askar, W.; El Nakeeb, A.; Abdelrafee, A.; Atef, E.; Ezzat, H.; Fathy, O.; Abdel Wahab, M. Risk Factors and Predictors of Poor Outcome Following Hepaticojejunostomy for Postcholecystecomy Bile Duct Injury. Indian J. Surg. 2019. [Google Scholar] [CrossRef]
- Abbas, A.M.; Strong, A.T.; Diehl, D.L.; Brauer, B.C.; Lee, I.H.; Burbridge, R.; Zivny, J.; Higa, J.T.; Falcão, M.; El Hajj, I.I.; et al. Multicenter evaluation of the clinical utility of laparoscopy-assisted ERCP in patients with Roux-en-Y gastric bypass. Gastrointest. Endosc. 2018, 87, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Mita, M.; Dalmonte, G.; Gnocchi, A.; Marchesi, F. Transjejunal laparoscopic-assisted ERCP in Roux-en-Y patient: The new right path. Ann. R. Coll. Surg. Engl. 2018, 101, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Dalmonte, G.; Valente, M.; Bosi, S.; Gnocchi, A.; Marchesi, F. Transjejunal Laparoscopic-Assisted ERCP: A Technique to Deal with Choledocholithiasis After Roux-En-Y Reconstruction. Obes. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, J.C.D.; Noda, R.; Haida, V.M.; Medeiros, R.C.D.L.; Sadowski, S.; Galvão Neto, M.; Marchesini, J.B.; Campos, J.M. Transenteric ERCP for treatment of choledocholithiasis after duodenal switch. Surg. Laparosc. Endosc. Percutan. Tech. 2017, 27, e28–e30. [Google Scholar] [CrossRef] [PubMed]
- Surdeanu, I.; El Moussaoui, I.; Dika, M.; Des Marez, B.; Closset, J.; Mehdi, A. Laparoscopy-assisted transjejunal ERCP in a patient with roux-en-Y gastric bypass. Acta. Chir. Belg. 2016, 12, 1–7. [Google Scholar] [CrossRef]
- Lopes, T.L.; Clements, R.H.; Wilcox, C.M. Laparoscopy-Assisted Transjejunal ERCP in a Patient with Roux-en-Y Reconstruction Following Partial Gastrectomy. J. Laparoendosc. Adv. Surg. Tech. 2010, 20, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Saleem, A.; Sawyer, M.D.; Baron, T.H. Laparoscopy assisted transjejunal ERCP for treatment of pancreaticopleural fistula. J. Pancreas. 2010, 11, 69–71. [Google Scholar]
- Mutignani, M.; Marchese, M.; Tringali, A.; Tacchino, R.M.; Matera, D.; Foco, M.; Greco, F.; Costamagna, G. Laparoscopy-assisted ERCP after biliopancreatic diversion. Obes. Surg. 2007, 17, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Mansor, S.M.; Abdalla, S.I.; Bendardaf, R.S. Laparoscopy assisted transjejunal endoscopic retrograde cholangiography for treatment of intrahepatic duct stones in a post Roux-en-y patient. Saudi. Med. J. 2015, 36, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Tsutsumi, K.; Kato, H.; Akimoto, Y.; Uchida, D.; Tomoda, T.; Yamamoto, N.; Noma, Y.; Horiguchi, S.; Okada, H.; et al. Effectiveness of peroral direct cholangioscopy using an ultraslim endoscope for the treatment of hepatolithiasis in patients with hepaticojejunostomy (with video). Surg. Endosc. 2016, 30, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.J.; Jiang, Y.; Wang, X.; Tian, F.Z.; Lv, L.Z. Comparatively lower postoperative hepatolithiasis risk with hepaticocholedochostomy versus hepaticojejunostomy. Hepatobiliary Pancreat. Dis. Int. 2010, 9, 38–43. [Google Scholar] [PubMed]
- Inamdar, S.; Slattery, E.; Sejpal, D.V.; Miller, L.S.; Pleskow, D.K.; Berzin, T.M.; Trindade, A.J. Systematic review and meta-analysis of single-balloon enteroscopy-assisted ERCP in patients with surgically altered GI anatomy. Gastrointest. Endosc. 2015, 82, 9–19. [Google Scholar] [CrossRef] [PubMed]
- da Ponte-Neto, A.M.; Bernardo, W.M.; de A Coutinho, L.M.; Josino, I.R.; Brunaldi, V.O.; Moura, D.T.H.; Sakai, P.; Kuga, R.; de Moura, E.G.H. Comparison between Enteroscopy-Based and Laparoscopy-Assisted for Accessing the Biliary Tree in Patients with Roux-en-Y Gastric Bypass: Systematic Review and Meta-analysis. Obes Surg. 2018, 28, 4064–4076. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, K.; Kato, H.; Yabe, S.; Mizukawa, S.; Seki, H.; Akimoto, Y.; Uchida, D.; Matsumoto, K.; Tomoda, T.; Yamamoto, N.; et al. A comparative evaluation of treatment methods for bile duct stones after hepaticojejunostomy between percutaneous transhepatic cholangioscopy and peroral, short double-balloon enteroscopy. Therap. Adv. Gastroenterol. 2017, 10, 54–67. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Age | Gender | GI Surgery | Bypass Time (months) | Diagnostic Studies | Diagnosis | LOS (Days) | Follow up | Concomitant CCE | Endoscope Type | Notes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dalmonte 2019 | NM | Female | RYGBP | 24 | CT, MRCP | CBD stones | 4 | 3m | yes | Colonoscope | Biliary limb extracted through mini laparotomy |
| Mita 2018 | 79 | Female | RYGBP | 48 | CT, MRCP | CBD stones, CCL | 6 | NM | yes | Colonoscope | Biliary limb extracted through mini laparotomy |
| Marchesini 2017 | 60 | Male | BPD | 24 | MRCP | CBD stones, CCL | NM | NM | yes | Duodenoscope | Rendezvous cannulation through gallbladder, bowel drawn up to abdominal wall. |
| Marchesini 2017 | 52 | Female | BPD | 36 | US, MRCP | CBD stones, CCL | NM | NM | yes | Duodenoscope | |
| Surdeanu 2016 | 50 | Male | RYGBP | 48 | US, IOC | CBD stones, CCL | 7 | NM | yes | Endoscope (?) | Jejuno-jejunal anastomosis exteriorization |
| Mansor 2015 | 17 | Female | Roux-en-Y hepaticojejunostomy | 156 | MRCP | Ascending cholangitis due to intrahepatic gallstones | 5 | 12m | No (previously done) | Gastroscope | Bowel drawn up to abdominal wall through optic port incision |
| Lopes 2010 | 18 | Female | RYGB (partial gastrectomy) | 24 | CT, MRCP | Sphincter of Oddi dysfunction | NM | 3m | No (previously done) | Duodenoscope | No exteriorization |
| Saleem 2010 | 47 | female | ST gastrectomy with RY gastrojejunostomy | NM | NM | Pancreaticopleural fistula | 5 | 2m | NM | Duodenoscope | Biliopancreatic limb drawn up to abdominal wall through right subcostal port |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baca-Arzaga, A.A.; Navarro-Chavez, H.; Galindo-Jimenez, J.; Santibanez-Juarez, J.; Cardosa-Gonzalez, C.; Flores-Villalba, E. Transjejunal Laparoscopic Assisted ERCP in a Patient with Roux-en-Y Hepaticojejunostomy. Medicina 2019, 55, 483. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080483
Baca-Arzaga AA, Navarro-Chavez H, Galindo-Jimenez J, Santibanez-Juarez J, Cardosa-Gonzalez C, Flores-Villalba E. Transjejunal Laparoscopic Assisted ERCP in a Patient with Roux-en-Y Hepaticojejunostomy. Medicina. 2019; 55(8):483. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080483
Chicago/Turabian StyleBaca-Arzaga, Adrian A., Hector Navarro-Chavez, Jesus Galindo-Jimenez, Jose Santibanez-Juarez, Claudia Cardosa-Gonzalez, and Eduardo Flores-Villalba. 2019. "Transjejunal Laparoscopic Assisted ERCP in a Patient with Roux-en-Y Hepaticojejunostomy" Medicina 55, no. 8: 483. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080483