Arthroscopic Latarjet for Recurrent Shoulder Instability

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Clinical Assessment
2.3. Imaging Assessment
2.4. Surgical Technique
- Joint evaluation and exposure through a posterior portal and an anterior portal. The lateral side of the coracoids was analyzed, opening the rotator interval. The coracoacromial ligament was released.
- Subscapularis split through the anterolateral portal (parallel to the superior margin of the subscapularis tendon). In this stage, an inferior portal at the apex of the anterior axillary fold, an anteroinferior portal midway between the inferior and the anterolateral portal, and a medial portal were performed. The split area was identified through the posterior portal; the conjoint tendon and the brachial plexus were protected through the medial portal with a switching stick. A burr was used to expose and abrade the anterior wall of the glenoid neck.
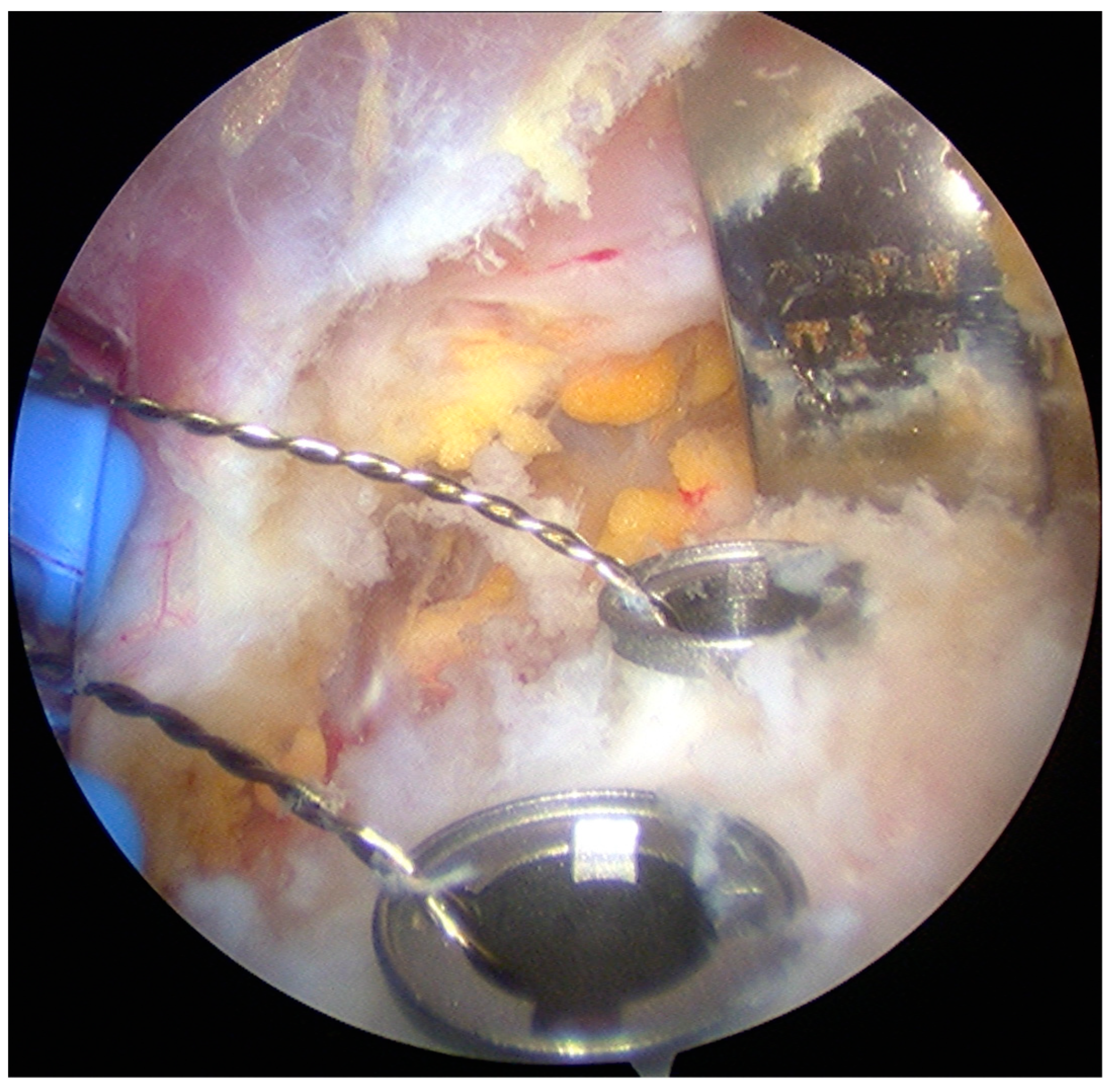
- The pectoralis minor was released, and a fresh portal was established with a needle over the coracoid, to insert the drill holes, at the junction of the lateral 2/3 and the medial 1/3. Two Kirschner wires through the coracoid were passed. The drill guide was removed. The holes were tapped, and the top hats were inserted into the fragment using a flexible Chia wire. The osteotomy was completed (Figure 2). The bone fragment was secured thought a coracoid screw passed over the Chia wire, using a double cannula.
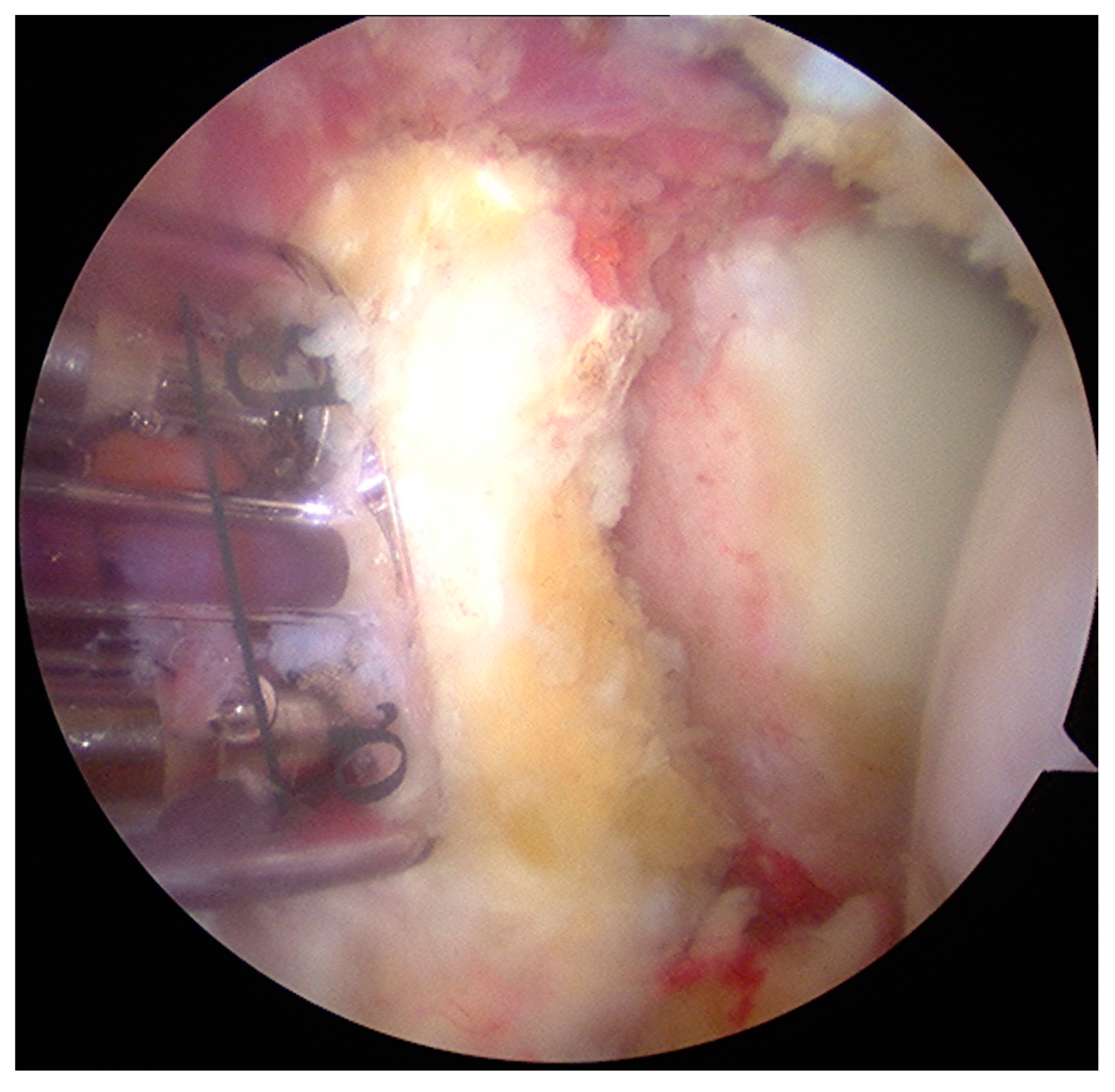
- The graft was positioned on the anterior glenoid neck with the switching stick through the posterior portal (Figure 3).
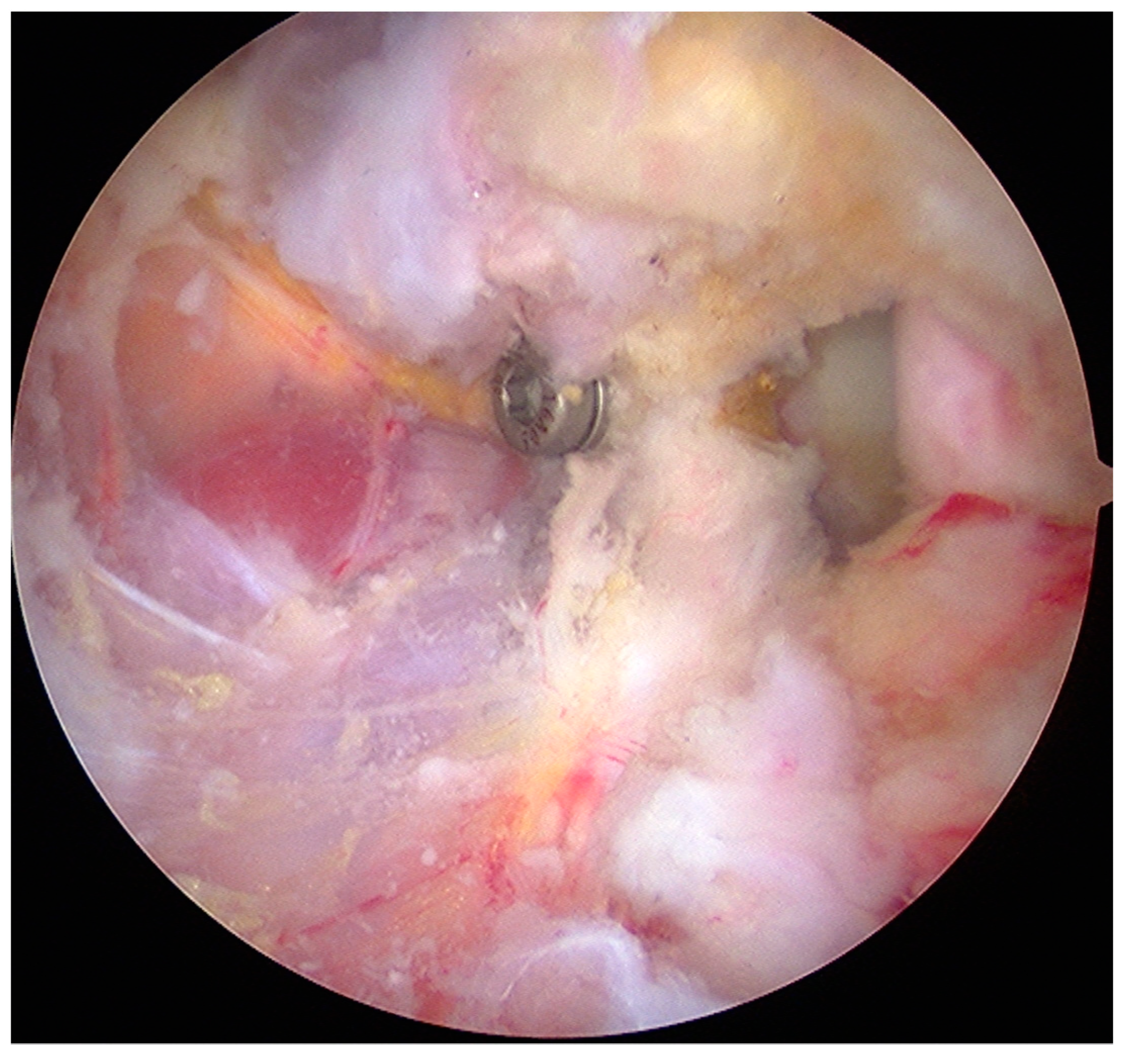
- The graft was fixed. Two holes were made through the coracoid and the glenoid using the double cannula. Graft trimming was performed with the burr (Figure 4).
2.5. Postoperative Rehabilitation
2.6. Data Collection and Statistical Analysis
3. Results
3.1. Demographics
3.2. Clinical Outcomes
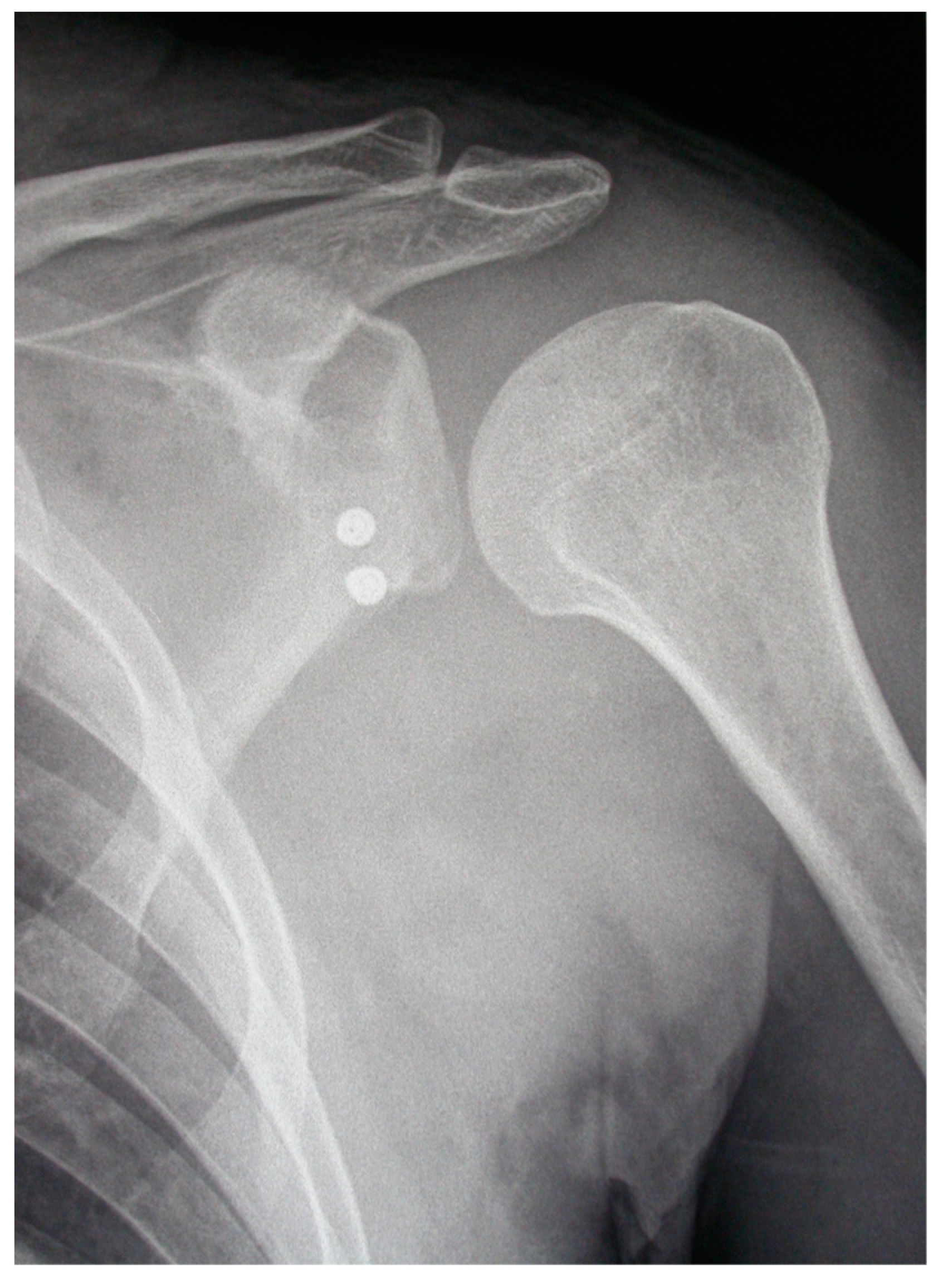
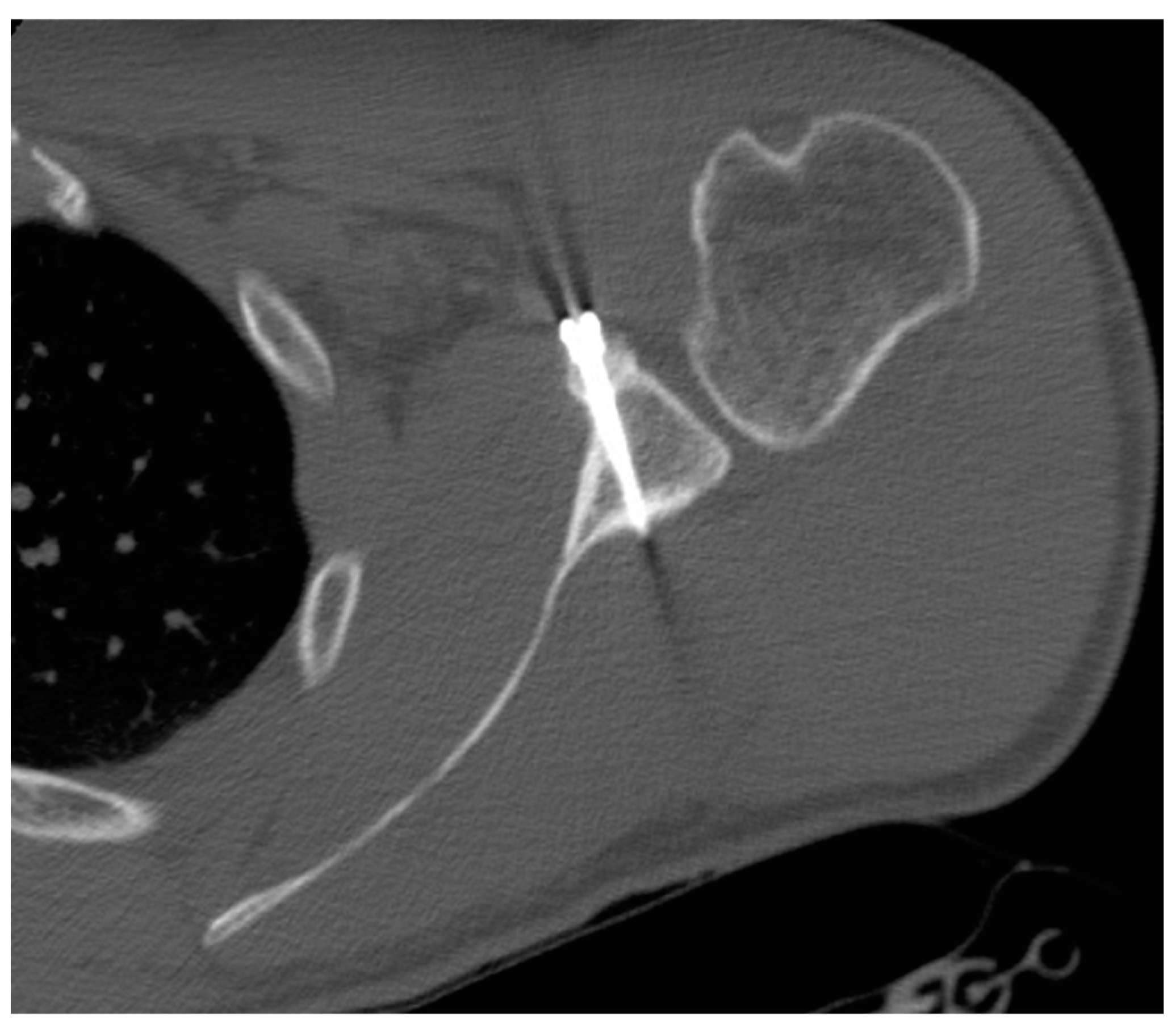
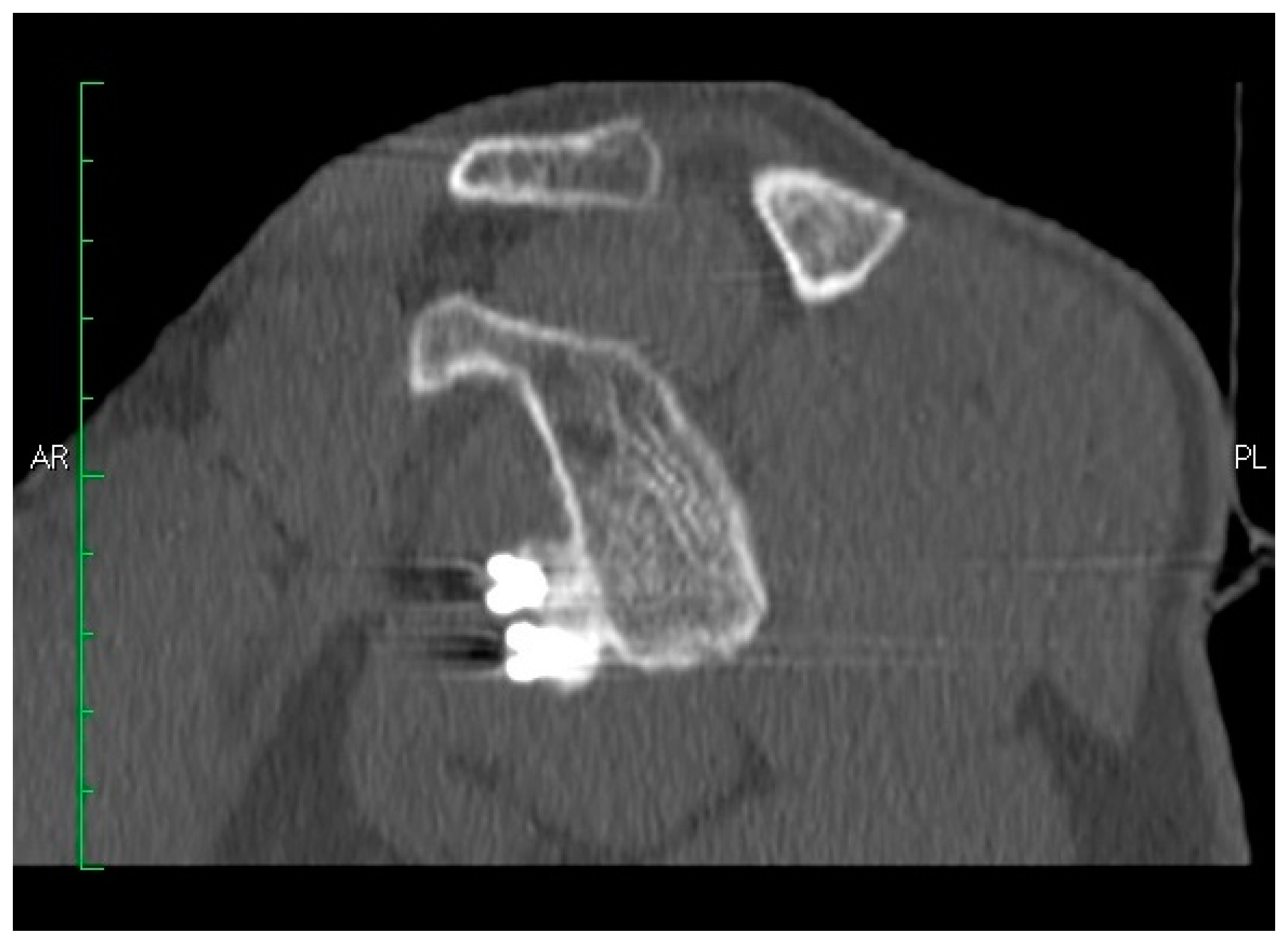
3.3. Imaging Outcomes
3.3.1. Coracoid Graft Healing
3.3.2. Coracoid Graft Positioning
3.3.3. Screws Angle
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Longo, U.G.; Loppini, M.; Rizzello, G.; Ciuffreda, M.; Maffulli, N.; Denaro, V. Management of primary acute anterior shoulder dislocation: Systematic review and quantitative synthesis of the literature. Arthrosc. J. Arthrosc. Relat. Surg. 2014, 30, 506–522. [Google Scholar] [CrossRef] [PubMed]
- Kartus, C.; Matis, N.; Forstner, R.; Resch, H. Long-term independent evaluation after arthroscopic extra-articular bankart repair with absorbable tacks: A clinical and radiographic study with a seven to ten-year follow-up. J. Bone Jt. Surgery-American Vol. 2007, 89, 1442. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Rizzello, G.; Ciuffreda, M.; Maffulli, N.; Denaro, V. Latarjet, Bristow, and Eden-Hybinette procedures for anterior shoulder dislocation: Systematic review and quantitative synthesis of the literature. Arthrosc. J. Arthrosc. Relat. Surg. 2014, 30, 1184–1211. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Rizzello, G.; Loppini, M.; Locher, J.; Buchmann, S.; Maffulli, N.; Denaro, V. Multidirectional instability of the shoulder: A systematic review. Arthroscopy 2015, 31, 2431–2443. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; van der Linde, J.A.; Loppini, M.; Coco, V.; Poolman, R.W.; Denaro, V. Surgical versus nonoperative treatment in patients up to 18 years old with traumatic shoulder instability: A systematic review and quantitative synthesis of the literature. Arthroscopy 2016, 32, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Locher, J.; Wilken, F.; Beitzel, K.; Buchmann, S.; Longo, U.G.; Denaro, V.; Imhoff, A.B. Hill-Sachs off-track lesions as risk factor for recurrence of instability after arthroscopic Bankart repair. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 1993–1999. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Rizzello, G.; Locher, J.; Salvatore, G.; Florio, P.; Maffulli, N.; Denaro, V. Bone loss in patients with posterior gleno-humeral instability: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Rizzello, G.; Ciuffreda, M.; Berton, A.; Maffulli, N.; Denaro, V. Remplissage, humeral osteochondral grafts, weber osteotomy, and shoulder arthroplasty for the management of humeral bone defects in shoulder instability: Systematic review and quantitative synthesis of the literature. Arthrosc. J. Arthrosc. Relat. Surg. 2014, 30, 1650–1666. [Google Scholar] [CrossRef] [PubMed]
- Latarjet, M. Treatment of recurrent dislocation of the shoulder. Lyon Chir. 1954, 49, 994–997. [Google Scholar] [PubMed]
- Latarjet, M. Technic of coracoid preglenoid arthroereisis in the treatment of recurrent dislocation of the shoulder. Lyon Chir. 1958, 54, 604–607. [Google Scholar] [PubMed]
- Beranger, J.S.; Klouche, S.; Bauer, T.; Demoures, T.; Hardy, P. Anterior shoulder stabilization by Bristow–Latarjet procedure in athletes: return-to-sport and functional outcomes at minimum 2-year follow-up. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Ruci, V.; Duni, A.; Cake, A.; Ruci, D.; Ruci, J. Bristow-Latarjet technique: Still a very successful surgery for anterior glenohumeral instability - A forty year one clinic experience. Open Access Maced. J. Med Sci. 2015, 3, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Paulino Pereira, N.R.; van der Linde, J.A.; Alkaduhimi, H.; Longo, U.G.; van den Bekerom, M.P.J. Are collision athletes at a higher risk of re-dislocation after an open Bristow-Latarjet procedure? A systematic review and meta-analysis. Shoulder Elbow 2018, 10, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Van der Linde, J.A.; van Wijngaarden, R.; Somford, M.P.; van Deurzen, D.F.; van den Bekerom, M.P. The Bristow-Latarjet procedure, a historical note on a technique in comeback. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Boileau, P.; Mercier, N.; Old, J. Arthroscopic Bankart-Bristow-Latarjet (2B3) procedure: How to do it and tricks to make it easier and safe. Orthop. Clin. North Am. 2010, 41, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Boileau, P.; Mercier, N.; Roussanne, Y.; Thélu, C.-É.; Old, J. Arthroscopic Bankart-Bristow-Latarjet procedure: The development and early results of a safe and reproducible technique. Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 1434–1450. [Google Scholar] [CrossRef] [PubMed]
- Boileau, P.; Thélu, C.-É.; Mercier, N.; Ohl, X.; Houghton-Clemmey, R.; Carlès, M.; Trojani, C. Arthroscopic Bristow-Latarjet Combined With Bankart Repair Restores Shoulder Stability in Patients With Glenoid Bone Loss. Clin. Orthop. Relat. Res. 2014, 472, 2413–2424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lafosse, L.; Boyle, S. Arthroscopic Latarjet procedure. J. Shoulder Elbow Surg. 2010, 19, 2–12. [Google Scholar] [CrossRef]
- Lafosse, L.; Boyle, S.; Gutierrez-Aramberri, M.; Shah, A.; Meller, R. Arthroscopic latarjet procedure. Orthop. Clin. North Am. 2010, 41, 393–405. [Google Scholar] [CrossRef]
- Hovelius, L.K.; Sandström, B.C.; Rösmark, D.L.; Saebö, M.; Sundgren, K.H.; Malmqvist, B.G. Long-term results with the Bankart and Bristow-Latarjet procedures: Recurrent shoulder instability and arthropathy. J. Shoulder Elbow Surg. 2001, 10, 445–452. [Google Scholar] [CrossRef]
- Hovelius, L.; Sandström, B.; Olofsson, A.; Svensson, O.; Rahme, H. The effect of capsular repair, bone block healing, and position on the results of the Bristow-Latarjet procedure (study III): Long-term follow-up in 319 shoulders. J. Shoulder Elbow Surg. 2012, 21, 647–660. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Saris, D.; Poolman, R.W.; Berton, A.; Denaro, V. Instruments to assess patients with rotator cuff pathology: A systematic review of measurement properties. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Ellman, H.; Hanker, G.; Bayer, M. Repair of the rotator cuff. End-result study of factors influencing reconstruction. J. Bone Jt. Surgery-American Vol. 1986, 68, 1136–1144. [Google Scholar] [CrossRef]
- Lafosse, L.; Lejeune, E.; Bouchard, A.; Kakuda, C.; Gobezie, R.; Kochhar, T. The Arthroscopic Latarjet Procedure for the Treatment of Anterior Shoulder Instability. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 1242-e1–1242-e5. [Google Scholar] [CrossRef] [PubMed]
- Castricini, R.; De Benedetto, M.; Orlando, N.; Rocchi, M.; Zini, R.; Pirani, P. Arthroscopic Latarjet procedure: analysis of the learning curve. Musculoskelet. Surg. 2013, 97, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Forriol, F.; Loppini, M.; Lanotte, A.; Salvatore, G.; Maffulli, N.; Denaro, V. The safe zone for avoiding suprascapular nerve injury in bone block procedures for shoulder instability. A cadaveric study. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1506–1510. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Delaney, R.; Petkin, K.; Lafosse, L. Complications of the Latarjet procedure. Curr. Rev. Musculoskelet. Med. 2015, 8, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griesser, M.J.; Harris, J.D.; McCoy, B.W.; Hussain, W.M.; Jones, M.H.; Bishop, J.Y.; Miniaci, A. Complications and re-operations after Bristow-Latarjet shoulder stabilization: a systematic review. J. Shoulder Elb. Surg. 2013, 22, 286–292. [Google Scholar] [CrossRef]
- Walch, G.; Agostini, J.Y.; Levigne, C.; Nové-Josserand, L. [Recurrent anterior and multidirectional instability of the shoulder]. Revue de Chirurgie Orthopédique et Réparatrice de l’Appareil Moteur 1995, 81, 682–690. [Google Scholar]
- Hovelius, L.; Albrektsson, B.; Berg, E.; Körner, L.; Lundberg, B.; Wredmark, T.; Åkermark, C. Bristow-Latarjet Procedure for Recurrent Anterior Dislocation of the Shoulder: A 2-5 Year Follow-up Study on the Results of 112 Cases. Acta Orthop. Scand. 1983, 54, 284–290. [Google Scholar] [CrossRef]
- Goutallier, D.; Glorion, C.; Allain, J. Long-Term Results of the Latarjet Procedure for the Treatment of Anterior Instability of the Shoulder*. J. Bone Jt. Surgery-American Vol. 1998, 80, 841–852. [Google Scholar]
- Young, D.C.; Rockwood, C.A. Complications of a failed Bristow procedure and their management. J. Bone Jt. Surgery-American Vol. 1991, 73, 969–981. [Google Scholar] [CrossRef]
- Longo, U.G.; Rizzello, G.; Ciuffreda, M.; Locher, J.; Berton, A.; Salvatore, G.; Denaro, V. Humeral avulsion of the glenohumeral ligaments: A systematic review. Arthroscopy 2016, 32, 1868–1876. [Google Scholar] [CrossRef] [PubMed]
- Southgate, D.F.; Bokor, D.J.; Longo, U.G.; Wallace, A.L.; Bull, A.M. The effect of humeral avulsion of the glenohumeral ligaments and humeral repair site on joint laxity: A biomechanical study. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Denaro, V.; Huijsmans, P.E.; Maffulli, N.; De Beer, J.F.; Beer, J.F. Video analysis of the mechanisms of shoulder dislocation in four elite rugby players. J. Orthop. Sci. 2011, 16, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Lazarides, A.L.; Duchman, K.R.; Ledbetter, L.; Riboh, J.C.; Garrigues, G.E. Arthroscopic remplissage for anterior shoulder instability: A systematic review of clinical and biomechanical studies. Arthroscopy 2019, 35, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Funakoshi, T.; Hartzler, R.; Stewien, E.; Burkhart, S. Remplissage using interconnected knotless anchors: Superior biomechanical properties to a knotted technique? Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 2954–2959. [Google Scholar] [CrossRef]
- Hartzler, R.U.; Bui, C.N.; Jeong, W.K.; Akeda, M.; Peterson, A.; McGarry, M.; Denard, P.J.; Burkhart, S.S.; Lee, T.Q. Remplissage of an off-track hill-sachs lesion is necessary to restore biomechanical glenohumeral joint stability in a bipolar bone loss model. J. Shoulder Elb. Surg. 2016, 25, e325–e326. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Complications | Number of Patients (%) | Management |
|---|---|---|
| Coracoid graft rupture | 3 (7%) | Surgery: screws removal |
| Screws intolerance | 2 (5%) | Surgery: screws removal |
| Hematoma | 1 (2%) | Conservative management |
| Recurrent instability | 1 (2%) | Surgery (other Hospital) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castricini, R.; Longo, U.G.; Petrillo, S.; Candela, V.; De Benedetto, M.; Maffulli, N.; Denaro, V. Arthroscopic Latarjet for Recurrent Shoulder Instability. Medicina 2019, 55, 582. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090582
Castricini R, Longo UG, Petrillo S, Candela V, De Benedetto M, Maffulli N, Denaro V. Arthroscopic Latarjet for Recurrent Shoulder Instability. Medicina. 2019; 55(9):582. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090582
Chicago/Turabian StyleCastricini, Roberto, Umile Giuseppe Longo, Stefano Petrillo, Vincenzo Candela, Massimo De Benedetto, Nicola Maffulli, and Vincenzo Denaro. 2019. "Arthroscopic Latarjet for Recurrent Shoulder Instability" Medicina 55, no. 9: 582. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090582