Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies


1
Department of Pharmacy, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City 23142, Taiwan
2
School of Pharmacy, College of Pharmacy, Taipei Medical University, Taipei City 11031, Taiwan
3
School of Medicine, Tzu Chi University, Hualien 97004, Taiwan
4
Department of Internal Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City 23142, Taiwan
*
Author to whom correspondence should be addressed.
Medicina 2020, 56(10), 513; https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100513
Submission received: 10 August 2020
/
Revised: 24 September 2020
/
Accepted: 29 September 2020
/
Published: 1 October 2020
(This article belongs to the Special Issue Meta-Research in the Medico-Scientific Field)
Abstract
:Background and objectives: The association between hypnotic drugs and risk of cancer remains controversial. Therefore, we performed a meta-analysis to investigate this association. Materials and Methods: Pubmed and Embase were searched systematically to identify publications up to April 2020. The Newcastle-Ottawa scale for observational studies was used to assess the quality of studies. All included studies were evaluated by two reviewers independently; any discrepancies were resolved through discussion. Results: Twenty-eight studies including 22 case-control studies and 6 cohort studies with 340,614 hypnotics users and 1,828,057 non-users were included in the final analyses. Hypnotics (benzodiazepines and Z-drugs) use was significantly associated with an increased risk of cancer (odds ratio [OR] or relative risk [RR] 1.17; 95% confidence interval 1.09–1.26) in a random-effects meta-analysis of all studies. Subgroup meta-analysis by anxiolytics/sedatives effect (anxiolytics benzodiazepines vs. sedatives group (include sedatives benzodiazepines and Z-drugs)) revealed that a significant association in sedatives group (pooled OR/RR 1.26, 95% CI, 1.10–1.45), whereas no significant relationship was observed in anxiolytics benzodiazepines (pooled OR/RR 1.09, 95% CI, 0.95–1.26). Moreover, a significant dose–response relationship was observed between the use of hypnotics and the risk of cancer. Conclusions: This meta-analysis revealed association between use of hypnotics drugs and risk of cancer. However, the use of lower dose hypnotics and shorter duration exposed to hypnotics seemed to be not associated with an increased risk of cancer. Moreover, the use of anxiolytics effect benzodiazepines seemed to be lower risk than sedatives benzodiazepines. A high heterogeneity was observed among identified studies, and results were inconsistent in some subgroups. Randomized control trials are needed to confirm the findings in the future.
1. Introduction
Hypnotics (benzodiazepines and Z-drugs) are medications used to improve sleeping quality and to reduce wakefulness [1]. Benzodiazepines and Z-drugs (zolpidem and zopiclone) are common medications prescribed for sleep disorder. Moreover, benzodiazepines are prescribed in treating diseases such as seizures, anxiety, insomnia, and depression. Benzodiazepines derivatives have been distinguished into anxiolytics (i.e., diazepam, oxazepam, bromazepam, alprazepam, fludiazepam) and sedatives (i.e., flurazepam, flunitrazepam, estazolam, triazolam, temazepam, midazolam) by their effect. Z-drugs are non-benzodiazepines sedative-hypnotic medications commonly used to treat insomnia. The prevalence of benzodiazepine uses ranges from 10% to 43% worldwide among the aged population [2].
Meanwhile, most common adverse effects associated with hypnotics are residual daytime sedation, drowsiness, cognitive impairment, motor incoordination, dependence [3,4,5,6], and even tremor, which imply the possible neurotoxicity in long-term or high dose use of hypnotics. Several previous laboratory or animal studies had demonstrated that uses of benzodiazepine drugs or Z-drugs are risk factors for cancer [7].
Cancer is the second leading cause of death globally and leads to economic burden for health systems or costs for patients. Previous studies have assessed the relation between benzodiazepines or Z-drugs use and cancer risk. However, the results are still controversial. In addition, the quantitative meta-analysis has separately examined the benzodiazepines or Z-drugs and cancer risk. Until now, no published quantitative meta-analysis discussed benzodiazepines and Z-drugs long-term use conjunction with cancers. Recently, several observational studies with a larger population indicated conflicting inconsistent results. Combining the results of these studies in a meta-analysis may strengthen their statistical power. In this study, we updated the hypnotic drug correlation between use and the risk of cancer by using a meta-analysis of observational studies both case-control studies and prospective cohort studies.
2. Methods
2.1. Literature Search Strategy
PubMed and EMBASE were searched, by using selected keywords linked with benzodiazepine and non-benzodiazepine hypnotics and the risk of cancer up to April 2020. Keywords were as follows: benzodiazepine or zolpidem or zopiclone or diazepam or alprazolam or clonazepam or temazepam or oxazepam and cancer or tumor or carcinoma or neoplasm and case-control or cohort. Moreover, we reviewed the bibliographies of relevant articles to locate additional studies. The search was limited to human patients and articles in English. The detailed information on the search strategy for eligible studies is given in the flowchart provided by Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
2.2. Selection Relevant Studies and Criteria
The studies we included meet all the following criteria: (1) case-control or cohort study, (2) investigated the associations between the use of benzodiazepines or Z-drugs and the risk of cancer, (3) outcome measures with adjusted odds ratios (OR) or relative risks (RR) and 95% confidence intervals (CI). If data were duplicated or shared in more than one study, the longest-term follow-up studies were included in the analysis. We excluded non-published studies.
2.3. Data Extraction
We used a standardized data extraction form that included study year, study location, study population, participant characteristics, cancer types and crude or adjusted effect sizes and their 95% confidence intervals (CIs).
2.4. Risk of Bias of Included Studies
Newcastle-Ottawa Scale (NOS) was used to assess the methodological quality of included case-controls and cohort studies [8]. The quality score can range from 0 to 9. A study is classified in each domain as at high or low risk according to prespecified criteria (see Table 1). All included studies were evaluated by two pharmacists (T.W.W.) and (T.R.P.) independently; any discrepancies were resolved through discussion.
2.5. Statistical Analyses
We conducted meta-analyses on the association of hypnotics use and the risk of cancer by observational studies. The random-effects model (DerSimonian–Laird method) was used to calculate the pooled OR or RR [9]. The Cochran Q test and I2 statistics were used to assess statistical heterogeneity and inconsistency. Statistical significance was set at p < 0.10 for Cochrane Q tests. Heterogeneity was considered low, moderate, or high, if the I2 values was < 25%, 25–50%, and > 50%, respectively. Results were considered as statistically significant when the p value was less than 0.05. Publication bias was examined by using funnel plots, and Egger’s and Begg’s test was used to analyze the publication bias in our studies. A p-value > 0.05 based on the Egger’s and Begg’s test indicated the absence of publication bias. Statistical analysis was performed according to the Cochrane Handbook for Statistical Review of Interventions (version 5.4) [10]. The meta-analysis was performed by using RevMan software (The Cochrane Collaboration, Oxford, UK) and STATA version 15.0 (StataCorp, College Station, TX, USA).
3. Results
3.1. Study Characteristics
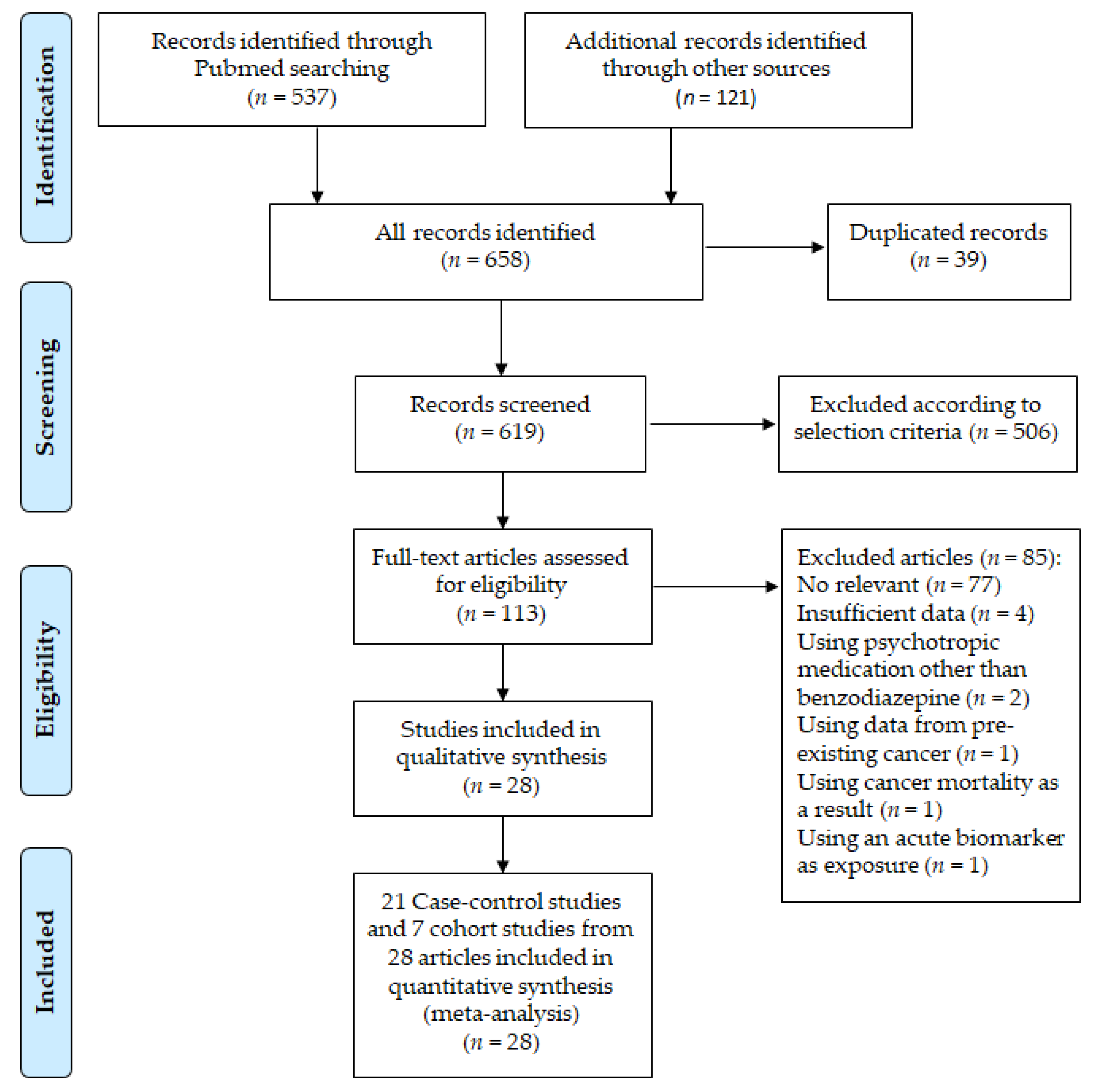
A total of 658 records were screened, and 113 full-text articles were assessed for eligibility. Twenty-eight articles were selected for qualitative review, including 22 case-control studies and 6 cohort studies (Figure 1). The characteristics of the 28 included studies are summarized in Table 2. The studies involved 2,168,671 participants (340,614 hypnotics users and 1,828,057 non-users).
3.2. Quality Assessment
We performed the methodological quality of studies based on NOS scales. The results of the methodological quality of studies are summarized in Table 2. The NOS range from 5–8; average NOS score was 6.9 and 7.1 for case-control studies and cohort studies, respectively; In case-control studies, 3 high-quality studies are included [25,29,33] (score of 8); in cohort studies, 6 high-quality studies are included [26,28,30,31,32,35] (score of 7).
3.3. Meta-Analysis and Subgroup Analysis
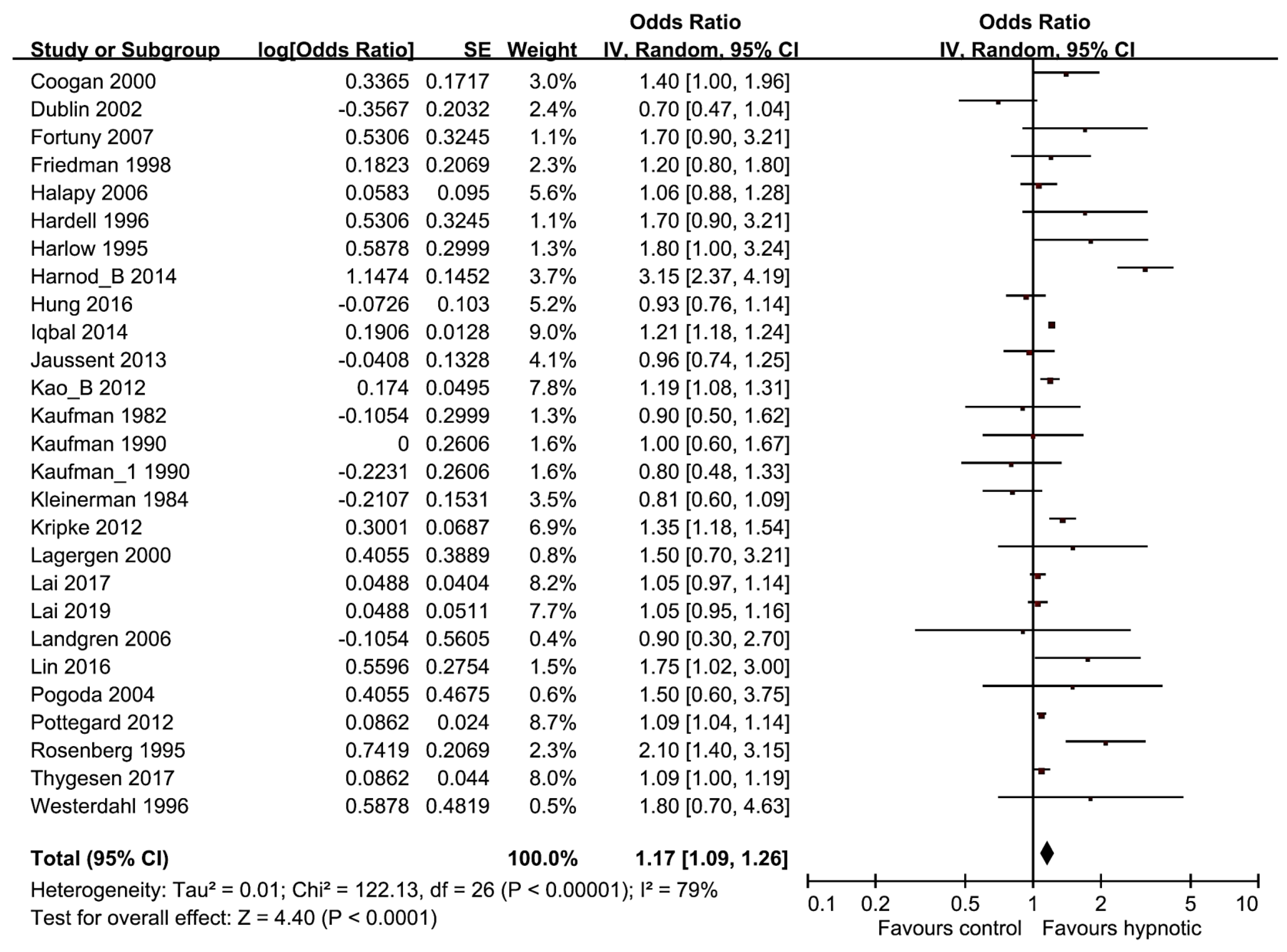
Overall, the risk of cancer was greater in hypnotics user than nonusers in the random-effects meta-analysis of all 27 studies (pooled OR/RR, 1.17; 95% CI, 1.09–1.26, p < 0.001, I2 = 79%) (Figure 2).
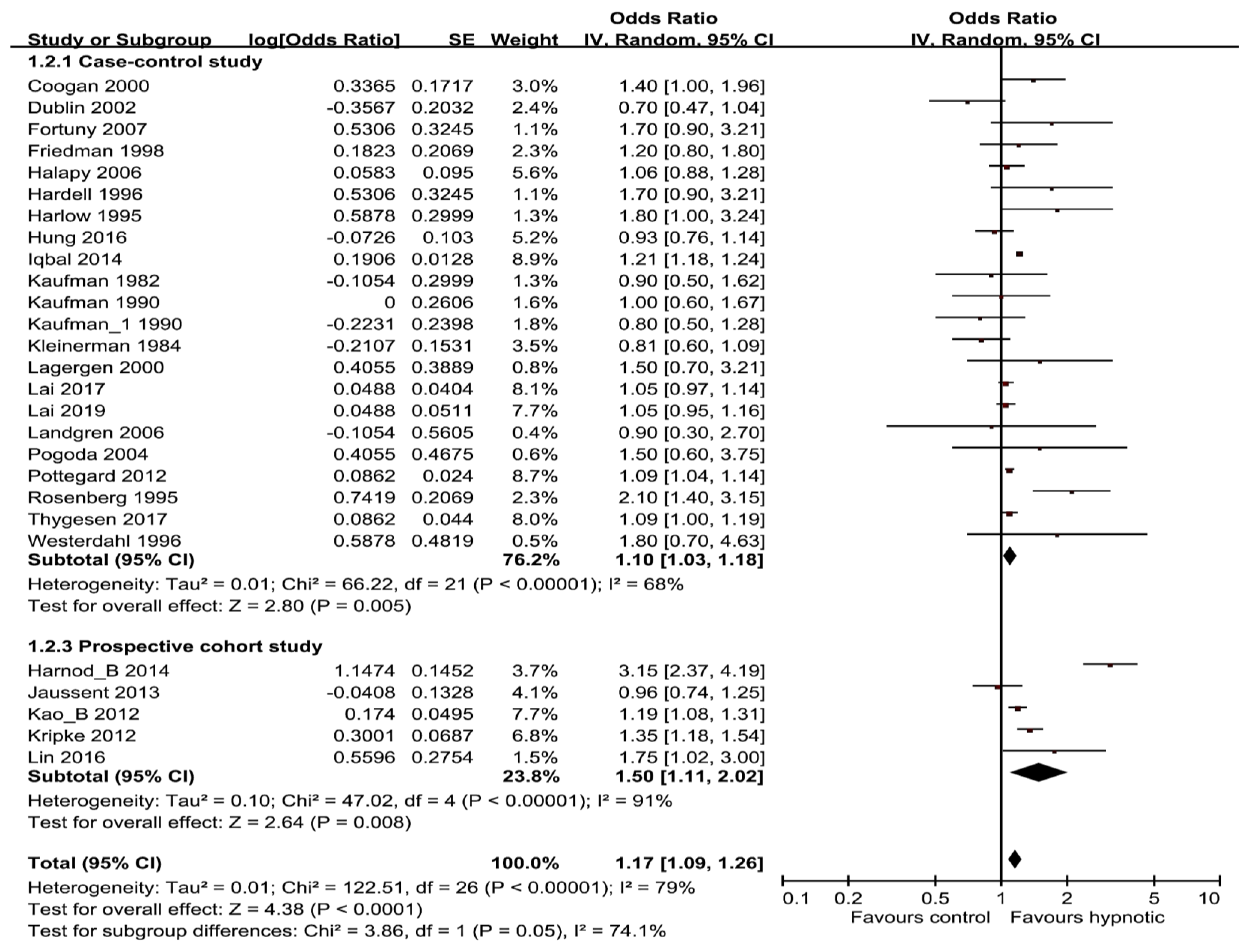
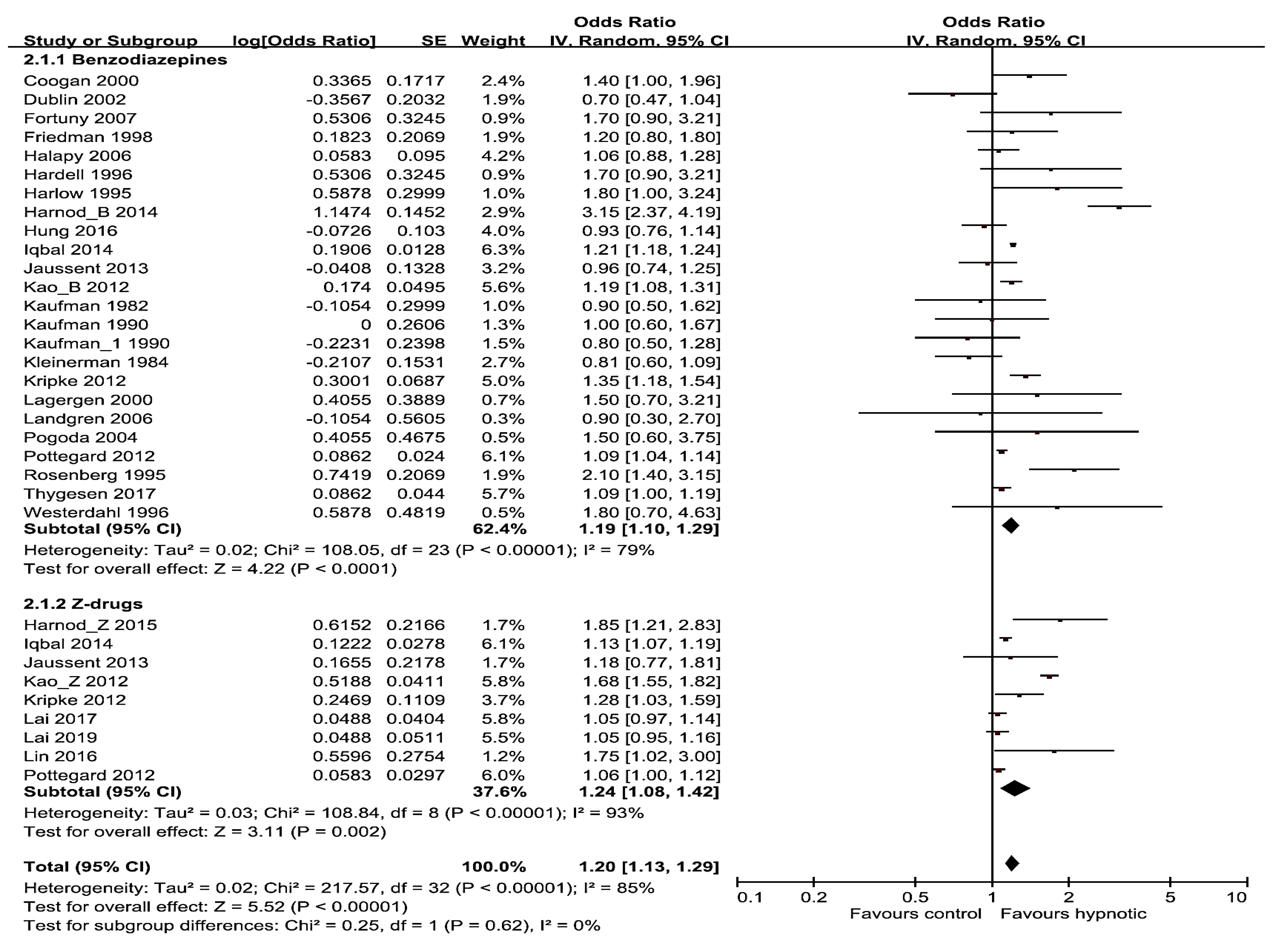
Subgroup analyses were carried out by research methods design (cohort or case-control study) and hypnotics categories (benzodiazepines, Z-drugs). In the subgroup analyses aligned with study design, hypnotics showed significant positive correlation with risk of cancer, both in case-control and cohort studies subgroup (pooled OR/RR was 1.10; 95% CI, 1.03–1.18 for 22 case-control studies and 1.50; 95% CI, 1.11–2.02 for 5 cohort studies) (Figure 3). In the subgroup analyses of hypnotics categories (benzodiazepines vs. Z-drugs), 24 studies are included in benzodiazepines group, the pooled OR/RR was 1.19 (95% CI, 1.10–1.29), and 8 studies are included in Z-drugs group and the pooled OR/RR was 1.24 (95% CI, 1.08–1.42) (Figure 4). Z-drugs group showed higher OR/RR than benzodiazepines group.
3.4. Subgroup Meta-Analyses by Different Factors
The results of subgroup meta-analyses by different factors were showed in Table 3. The use of hypnotics was associated with an increased risk of cancer in the subgroup meta-analyses by duration of hypnotics use, cumulative yearly dose, and sedatives benzodiazepines and Z-drugs. Subgroup meta-analysis by gender showed that a significant association in both gender with 19 studies (pooled OR/RR 1.22, 95% CI, 1.13–1.32; I2 = 42%), whereas no significant relationship was observed in female with nine studies (pooled OR/RR 1.01, 95% CI, 0.89–1.14; I2 = 83%). However, there was no significant relationship observed in four studies with only elderly subjects (pooled OR/RR 1.16, 95% CI, 0.92–1.47). Subgroup meta-analysis by anxiolytics/sedatives effect (anxiolytics benzodiazepines vs. sedatives group (include sedatives benzodiazepines and Z-drugs)) revealed a significant association in sedatives group (pooled OR/RR 1.26, 95% CI, 1.10–1.45), whereas no significant relationship was observed in anxiolytics benzodiazepines (pooled OR/RR 1.09, 95% CI, 0.95–1.26). Regarding the type of hypnotics, short-acting hypnotics (midazolam, oxazepam, alprazolam, triazolam, and zolpidem) showed a significantly increased risk. Hypnotics use increased the risk of brain cancer, esophagus cancer, liver cancer, lung cancer, stomach cancer, pancreatic cancer, colon cancer, renal cancer, and prostate cancer. However, no significant association was observed in malignant melanoma, breast cancer, and ovarian cancer. When compared with nonusers of hypnotics, the pooled OR/RR for the risk of cancer was 1.03 (95% CI, 1.01–1.05) in a low dose, 1.30 (95% CI, 0.97–1.75) in a medium dose, and 2.03 (95% CI, 1.19–3.46) in a high dose (Table 3).
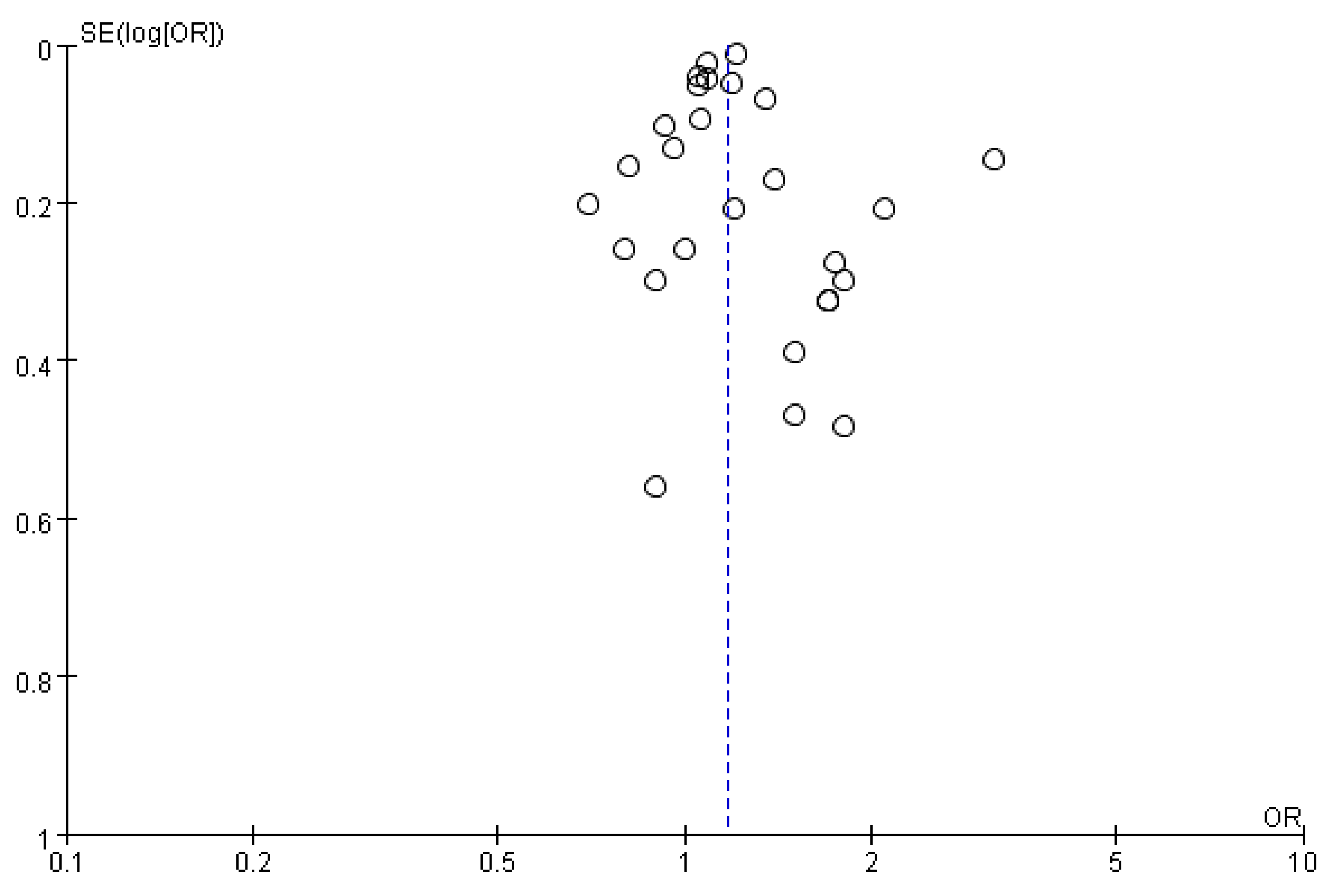
3.5. Publication Bias
A visual inspection of the funnel plot of OR/RR from these studies revealed asymmetry (Figure 5). However, both the Egger’s and Begg’s test suggested no statistical evidence of publication bias, with p value of 0.541 and 0.420, respectively.
4. Discussion
In our updated meta-analysis studies, the use of hypnotics was associated with an increased risk of cancer. Subgroup meta-analyses by different factors also showed similar results. However, this meta-analysis revealed that the cancer risk is related to dose–response, sedatives benzodiazepines and Z-drugs (pooled OR/RR 1.26, 95% CI, 1.10–1.45), and duration of hypnotics use (long term use: pooled OR/RR 1.11, 95% CI, 1.02–1.21). In recent years, several literatures have reported a tentative link between benzodiazepines and/or Z-drugs exposure with adverse outcomes such as respiratory disease exacerbation, infections, inflammation, dementia, pancreatitis, and cancer [39]. These kinds of adverse outcome, especially hypnotics, may relate to inflammation, infection, or cancer patients suffering from psychiatric and leading to more benzodiazepines exposure might reflect sharp of cancer diagnosed.
According to a review by Brambilla et al., the fact that the mechanisms of benzodiazepines- and Z-drugs-induced tumorigenesis remains tentative and unclear [40]. A study has reported evidence that use of hypnotics may lead to decline in immune function. Several animal studies have revealed that benzodiazepines disrupted the processes of phagocytes spreading and macrophages oxidative bursting [41,42]. These may be reduced release of the proinflammatory cytokines interleukin-6 and interleukin-13 in blood cells because of the activation of their benzodiazepine receptors [43]. Hypnotics use showed the strongest association with the risk of brain cancer in this meta-analysis (Table 3). These findings were consistent with results of Kim et al. (2017) and Zhang et al. (2017) [2,44]. The possible mechanism is that hypnotics enhance the neurotransmitter of gamma-aminobutyric acid (GABA) by interacting with the chlorine ion channel that binds to GABA receptors. The gamma-aminobutyric acid has an inhibitory neurotransmitter effect but also can regulate cell proliferation and differentiation of brain and peripheral at various stages and may participate benign tumor growth [45,46]. However, these potential mechanisms are still unproven.
Currently, there is still a lack of conclusive experimental data, but alarm signals for cancer risk have been raised by researchers for hypnotic drugs based on observational study findings [26,27,28,33]. A previous meta-analysis of 22 observational studies (18 case-control and 4 cohort studies) concluded there is an overall estimate of 19% increased cancer risk, with a significant dose–response trend, among benzodiazepines users over non-users [47]. A meta-analysis performed by Kim et al. (2017) included 6 observational epidemiological studies (3 case-control and 3 cohort studies) [44]. In a meta-analysis, compared with non-use of hypnotics, the OR for overall hypnotics (zopiclone or zolpidem) use was 1.29 for various cancers (95% confidence interval, 1.08–1.53). Our meta-analysis reported an overall estimate of 17% increased cancer risk with benzodiazepines- and Z-drugs use. Z-drugs group showed higher OR/RR (1.24, 95% CI, 1.08–1.42) than benzodiazepines group (1.19, 95% CI, 1.10–1.29). Our meta-analysis showed that hypnotics use was associated with the increased risk of cancer by duration of hypnotics, highest cumulative dose, and short acting hypnotics. According to the Bradford Hill criteria, the biological gradient (dose–response) is one of the important criteria confirming a causal relationship [48]. As shown, the dose of hypnotic is related to cancer risk, but it can also increase the causal relationship. The elderly is usually defined as individuals aged 65 years and older [49]. Insomnia is problematic for older adults. Two-fold increase was found in the intake of hypnotics among the elderly [50]. Current available hypnotic drugs all have significant risks for the elderly, such as increased risk for falls and cognitive function decline. However, we found that hypnotics use among the elderly showed a trend towards increased risk of cancer but not significantly (OR/RR, 1.16; 95% CI, 0.92–1.47; I2 = 84%). It may be associated with the small sample size (4 trials). Iqbal et al.’s (2014) study uses the Taiwanese National Health Insurance system to gather information about benzodiazepines use and cancer risk. They found that clonazepam, lorazepam, alprazolam, bromazepam, zolpidem, and zopiclone have a high risk of cancer [33]. However, we found that sedatives benzodiazepines and Z-drugs have higher cancer risk (pooled OR/RR 1.26, 95% CI, 1.10–1.45). Moreover, Z-drugs (zolpidem and zopiclone) have higher cancer risk than benzodiazepines (24% vs. 19%).
In addition, the most common risk factors for cancer including aging, smoking, alcohol consumption, family history, and exposure to chemicals or other substances [51]. The studies included in this meta-analysis, all of them, adjusted age as a confounding factor; fourteen studies adjusted alcohol drinking as a confounding factors; nine studies adjusted tobacco smoking as a confounding factor; nine studies adjusted family cancer history as a confounding factor, and only six studies adjusted medical use as a confounding factor. Thus, our studies are not excluding some important confounding factors such as alcohol drinking, tobacco smoking, family cancer history, and medical use that association between the hypnotics use and cancer risk. Nevertheless, there are still many factors that contribute to the risk factors of cancer, which have not been corrected. Therefore, the results should not be over-interpreted.
This study has some limitations. First, a portion of the included studies in our analysis did not adjust tobacco smoking, alcohol drinking, family cancer history, and medical use factors, which are known as important factors related to cancer. Second, this study only included cohort studies and case-control studies because there are no randomized controlled trials published on this topic. However, cohort studies and case-control studies have a lower level of evidence than randomized controlled trials.
5. Conclusions
The present meta-analysis found that hypnotics use was associated with an increased risk of cancer. However, the use of lower dose hypnotics and shorter duration exposed to hypnotics seemed to be not associated with an increased risk of cancer. Moreover, the use of anxiolytic effect benzodiazepines seemed to be lower risk than sedative benzodiazepines. Further large randomized controlled trials providing a higher level of evidence should be conducted to confirm our findings.
Author Contributions
Conceptualization, T.-R.P. and T.-W.W.; methodology, T.-R.P.; software, T.-R.P.; validation, T.-R.P., L.-J.Y., and T.-W.W.; formal analysis, T.-R.P. and L.-J.Y.; investigation, T.-W.W.; data curation, L.-J.Y.; writing—original draft preparation, T.-R.P.; writing—review and editing, T.-W.W. and Y.-C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by grants from the Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (TCRD-TPE-109-18).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Deoras, K.; Moul, D. Hypnotics. In Encyclopedia of the Neurological Sciences, 2nd ed.; Academic Press: Cambridge, MA, USA, 2014; pp. 646–649. [Google Scholar]
- Zhang, T.; Yang, X.; Zhou, J.; Liu, P.; Wang, H.; Li, A.; Zhou, Y. Benzodiazepine drug use and cancer risk: A dose-response meta analysis of prospective cohort studies. Oncotarget 2017, 8, 102381–102391. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. National Institutes of Health State of the Science Conference statement on Manifestations and Management of Chronic Insomnia in Adults. Sleep 2005, 28, 1049. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, N.; Vandermeer, B.; Friesen, C.; Bialy, L.; Tubman, M.; Ospina, M.; Klassen, T.P.; Witmans, M. The efficacy and safety of drug treatments for chronic insomnia in adults: A meta-analysis of RCTs. J. Gen Intern Med. 2007, 22, 1335. [Google Scholar] [CrossRef]
- Holbrook, A.M.; Crowther, R.; Lotter, A.; Cheng, C.; King, D. Meta-analysis of benzodiazepine use in the treatment of insomnia. CMAJ 2000, 162, 225. [Google Scholar]
- Nowell, P.D.; Mazumdar, S.; Buysse, D.J.; Dew, M.A.; Reynolds, C.F.; Kupfer, D.J. Benzodiazepines and zolpidem for chronic insomnia: A meta-analysis of treatment efficacy. JAMA 1997, 278, 2170. [Google Scholar] [CrossRef]
- Kunert-Radek, J.; Stepien, H.; Pawlikowski, M. Inhibition of rat pituitary tumor cell proliferation by benzodiazepines in vitro. Neuroendocrinology 1994, 59, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.; Deeks, J.J.; Altman, D.G. Special Topics in Statistics. Cochrane Handbook for Systematic Reviews of Interventions. In Cochrane Book Series; Wiley & Sons: London, UK, 2008; pp. 48–529. [Google Scholar]
- Kaufman, D.W.; Shapiro, S.; Slone, D.; Rosenberg, L.; Helmrich, S.P.; Miettinen, O.S.; Stolley, P.D.; Levy, M.; Schottenfeld, D. Diazepam and the risk of breast cancer. Lancet 1982, 6, 537–539. [Google Scholar] [CrossRef]
- Kleinerman, R.A.; Brinton, L.A.; Hoover, R.; Fraumeni, J.F. Diazepam use and progression of breast cancer. Cancer Res. 1984, 44, 1223–1225. [Google Scholar]
- Kaufman, D.W.; Werler, M.M.; Palmer, J.R.; Rosenberg, L.; Stolley, P.D.; Shapiro, S.; Warshauer, M.E.; Clarke, E.A.; Miller, D.R. Diazepam use in relation to breast cancer: Results from two case-control studies. Am. J. Epidemiol. 1990, 131, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Harlow, B.L.; Cramer, D.W. Self-reported use of antidepressants or benzodiazepine tranquilizers and risk of epithelial ovarian cancer: Evidence from two combined case-control studies (Massachusetts, United States). Cancer Causes Control 1995, 6, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L.; Palmer, J.R.; Zauber, A.G.; Warshauer, M.A.; Strom, B.L.; Hariap, S.; Shapiro, S. Relation of benzodiazepine use to the risk of selected cancers: Breast, large bowel, malignant melanoma, lung, endometrium, ovary, non-Hodgkin’s lymphoma, testis, Hodgkin’s disease, thyroid, and liver. Am. J. Epidemiol. 1995, 141, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Hardell, L.; Fredrikson, M.; Axelson, O. Case-control study on colon cancer regarding previous diseases and drug intake. Int. J. Oncol. 1996, 8, 439–444. [Google Scholar] [CrossRef]
- Westerdahl, J.; Olsson, H.; Måskback, A.; Ingvar, C.; Jonsson, N. Risk of malignant melanoma in relation to drug intake, alcohol, smoking and hormonal factors. Br. J. Cancer 1996, 73, 1126–1131. [Google Scholar] [CrossRef]
- Friedman, G.D.; Coates, A.O.; Potter, J.D.; Slattery, M.L. Drugs and colon cancer. Pharmacoepidemiol. Drug Saf. 1998, 7, 99–106. [Google Scholar] [CrossRef]
- Coogan, P.F.; Rosenberg, L.; Palmer, J.R.; Strom, B.L.; Stolley, P.D.; Zauber, A.G.; Shapiro, S. Risk of ovarian cancer according to use of antidepressants, phenothiazines, and benzodiazepines (United States). Cancer Causes Control 2000, 11, 839–845. [Google Scholar] [CrossRef]
- Lagergren, J.; Bergstrom, R.; Adami, H.O.; Nyrén, O. Association between medications that relax the lower esophageal sphincter and risk for esophageal adenocarcinoma. Ann. Intern. Med. 2000, 133, 165–175. [Google Scholar] [CrossRef]
- Dublin, S.; Rossing, M.A.; Heckbert, S.R.; Goff, B.A.; Weiss, N.S. Risk of epithelial ovarian cancer in relation to use of antidepressants, benzodiazepines, and other centrally acting medications. Cancer Causes Control 2002, 13, 35–45. [Google Scholar] [CrossRef]
- Pogoda, J.M.; Katz, J.; McKean-Cowdin, R.; Nichols, P.W.; Ross, R.K.; Preston-Martin, S. Prescription drug use and risk of acute myeloid leukemia by French-American-British subtype: Results from a Los Angeles County case-control study. Int. J. Cancer 2005, 114, 634–638. [Google Scholar] [CrossRef]
- Halapy, E.; Kreiger, N.; Cotterchio, M.; Sloan, M. Benzodiazepines and risk for breast cancer. Ann. Epidemiol. 2006, 16, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Zhang, Y.; Zahm, S.H.; Inskip, P.; Zheng, T.; Baris, D. Risk of multiple myeloma following medication use and medical conditions: A case-control study in Connecticut women. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2342–2347. [Google Scholar] [CrossRef] [PubMed]
- Fortuny, J.; Johnson, C.C.; Bohlke, K.; Chow, W.-H.; Hart, G.; Kucera, G.; Mujumdar, U.; Ownby, D.; Wells, K.; Engel, L.S.; et al. Use of anti-inflammatory drugs and lower esophageal sphincter-relaxing drugs and risk of esophageal and gastric cancers. Clin. Gastroenterol. Hepatol. 2007, 5, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Kripke, D.F.; Langer, R.D.; Kline, L.E. Hypnotics’ association with mortality or cancer: A matched cohort study. BMJ Open 2012, 2, e000850. [Google Scholar] [CrossRef]
- Kao, C.H.; Sun, L.M.; Su, K.P.; Chang, S.N.; Sung, F.C.; Muo, C.H.; Liang, J.A. Benzodiazepine use possibly increases cancer risk: A population-based retrospective cohort study in Taiwan. J. Clin. Psychiatr. 2012, 73, e555–e560. [Google Scholar] [CrossRef]
- Kao, C.H.; Sun, L.M.; Liang, J.A.; Chang, S.N.; Sung, F.C.; Muo, C.H. Relationship of zolpidem and cancer risk: A Taiwanese population-based cohort study. Mayo Clin. Proc. 2012, 87, 430–436. [Google Scholar] [CrossRef]
- Pottegård, A.; Friis, S.; Andersen, M.; Hallas, J. Use of benzodiazepines or benzodiazepine related drugs and the risk of cancer: A population-based case control study. Br. J. Clin. Pharmacol. 2013, 75, 1356–1364. [Google Scholar] [CrossRef]
- Jaussent, I.; Ancelin, M.L.; Berr, C.; Pérès, K.; Scali, J.; Besset, A.; Ritchie, K.; Dauvilliers, Y. Hypnotics and mortality in an elderly general population: A 12-year prospective study. BMC Med. 2013, 11, 212. [Google Scholar] [CrossRef]
- Harnod, T.; Lin, C.L.; Sung, F.C.; Kao, C.H. An association between benzodiazepine use and occurrence of benign brain tumors. J. Neurol. Sci. 2014, 336, 8–12. [Google Scholar] [CrossRef]
- Harnod, T.; Li, Y.F.; Lin, C.L.; Chang, S.N.; Sung, F.C.; Kao, C.H. Higher-dose uses of zolpidem will increase the subsequent risk of developing benign brain tumors. J. Neuropsychiatr. Clin. Neurosci. 2015, 27, e107–e111. [Google Scholar] [CrossRef]
- Iqbal, U.; Nguyen, P.A.; Syed-Abdul, S.; Yang, H.-S.; Huang, C.-H.; Jian, W.-E.; Hsu, M.-I.; Yen, Y.; Li, Y.-C. Is longterm use of benzodiazepine a risk for cancer? Medicine 2015, 94, e483. [Google Scholar] [CrossRef] [PubMed]
- Hung, D.Z.; Lin, C.L.; Li, Y.W. Association between antiepileptic drugs and hepatocellular carcinoma in patients with epilepsy: A population-based case-control study. Brain Behav. 2016, 6, e00554. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.C.; Su, Y.C.; Huang, Y.S.; Lee, C.C. Zolpidem increased cancer risk in patients with sleep disorder: A 3-year follow-up study. J. Med. Sci. 2016, 36, 68–74. [Google Scholar]
- Lai, S.W.; Lin, C.L.; Liao, K.F. Zolpidem administration and risk of hepatocellular carcinoma: A case-control study in Taiwan. Front. Pharmacol. 2017, 8, 767. [Google Scholar] [CrossRef]
- Thygesen, L.C.; Pottegård, A.; Ersbøll, A.K.; Friis, S.; Stürmer, T.; Hallas, J. External adjustment of unmeasured confounders in a case-control study of benzodiazepine use and cancer risk. Br. J. Clin. Pharmacol. 2017, 83, 2517–2527. [Google Scholar] [CrossRef]
- Lai, S.W.; Lin, C.L.; Liao, K.F. Association between colorectal cancer and zolpidem use in a case-control study. Medicine 2019, 98, e18127. [Google Scholar] [CrossRef]
- Brandt, J.; Leong, C. Benzodiazepines and Z-drugs: An updated review of major adverse outcomes reported on in epidemiologic research. Drugs R D. 2017, 17, 493–507. [Google Scholar] [CrossRef]
- Brambilla, G.; Carrozzino, R.; Martelli, A. Genotoxicity and carcinogenicity studies of benzodiazepines. Pharmacol. Res. 2007, 56, 443–458. [Google Scholar] [CrossRef]
- Massoco, C.; Palermo-Neto, J. Effects of midazolam on equine innate immune response: A flow cytometric study. Vet. Immunol. Immunopathol. 2003, 95, 11–19. [Google Scholar] [CrossRef]
- Massoco, C.O.; Palermo-Neto, J. Diazepam effects of peritoneal macrophage activity and corticosterone serum levels in Balb/C mice. Life Sci. 1999, 65, 2157–2165. [Google Scholar] [CrossRef]
- Torres, S.R.; Frode, T.S.; Nardi, G.M.; Vita, N.; Reeb, R.; Ferrara, P.; Farges, R.C.; Ribeiro-do-Valle, R.M. Anti-inflammatory effects of peripheral benzodiazepine receptor ligands in two mouse models of inflammation. Eur. J. Pharmacol. 2000, 408, 199–211. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, H.B.; Kim, Y.H.; Kim, J.Y. Use of Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Korean J. Fam. Med. 2018, 39, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Enna, S.J. Role of gamma-aminobutyric acid in anxiety. Psychopathology 1984, 17, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Jezewska, E.; Scinska, A.; Kukwa, W.; Sobolewska, A.; Turzynska, D.; Samochowiec, J.; Bienkowski, P. Gamma-aminobutyric acid concentrations in benign parotid tumours and unstimulated parotid saliva. J. Laryngol. Otol. 2011, 125, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.B.; Myung, S.K.; Park, Y.C.; Park, B. Use of benzodiazepine and risk of cancer: A meta-analysis of observational studies. Int. J. Cancer 2017, 140, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.B. The Environment and Disease: Association or Causation? Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef]
- Schutte-Rodin, S.; Broch, L.; Buysse, D.; Dorsey, C.; Sateya, M. Clinical guideline for the evaluation and chronic management of chronic insomnia in adults. J. Clin. Sleep Med. 2008, 4, 487–504. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Caulet, M.; Priest, R.G.; Guilleminault, C. Psychotropic medication consumption patterns in the UK general population. J. Clin. Epidemiol. 1998, 51, 273–283. [Google Scholar] [CrossRef]
- White, M.C.; Holman, D.M.; Boehm, J.E.; Peipins, L.A.; Grossman, M.; Henley, S.J. Age and cancer risk: A potentially modifiable relationship. Am. J. Prev. Med. 2014, 46, S7–S15. [Google Scholar] [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 flow diagram.
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 flow diagram.

Figure 2.
Forest plot of benzodiazepines/Z-drugs use and the risk of cancer.

Figure 3.
Forest plot of benzodiazepine/Z-drugs use and the risk of cancer by type of study design.

Figure 4.
Forest plot of use of benzodiazepines vs. Z-drugs and the risk of cancer.

Figure 5.
Publication bias funnel plots for use of benzodiazepines/Z-drugs and the risk of cancer.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Methodological quality of the studies included in the final analysis (n = 28).
| Case-Control Studies (n= 21) | Selection | Comparability Control for Important Factor or Additional Factor | Exposure | Total | |||||
| Adequate Definition of Cases | Representativeness of Cases | Selection of Controls | Definition of Controls | Ascertainment of Exposure | Same Method of Ascertainment for Participants | Nonresponse Rate | |||
| Kaufman (1982) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 |
| Kleinerman (1984) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Kaufman (1990) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Harlow (1995) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Rosenberg (1995) | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 7 |
| Hardell (1996) | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 5 |
| Westerdahl (1996) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Friedman (1998) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Coogan (2000) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 |
| Lagergen (2000) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Dublin (2002) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Pogoda (2004) | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
| Halapy (2006) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Landgren (2006) | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
| Fortuny (2007) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| Pottegard (2012) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Iqbal (2014) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Hung (2016) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Lai (2017) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Thygesen (2017) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Lai (2019) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Cohort Studies (n= 7) | Selection | Comparability Control for Important Factor or Additional Factor | Outcome | Total | |||||
| Representativeness of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Outcome of Interest Was Not Present at Start of Study | Assessment of Outcome | Follow-up Long Enough for Outcomes to Occur | Adequacy of Follow-up of Cohorts | |||
| Kripke (2012) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Kao_B (2012) | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 6 |
| Jaussent (2013) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Harnod_B (2014) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Kao_Z (2012) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Harnod (2015) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Lin (2016) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
Table 2.
Characteristics of included studies.
| Author (year) | Study type | Country | Years Enrolled | Population (Hypnotic /Control) | Cancer Type | Definition of Hypnotic use | OR/RR (95% CI) |
|---|---|---|---|---|---|---|---|
| Kaufman (1982) [11] | Case-control | Canada, United States and Israel | 1976–1980 | 1236/728 | Breast | Diazepam ≥ 6 month vs. never-use | 0.9 (0.5–1.6) |
| Kleinerman (1984) [12] | Case-control | United States | 1973–1977 | 1075/1146 | Breast | Diazepam ≥ 6 month vs. never-use | 0.81 (0.6–1.1) |
| Kaufman (1990) [13] | Case-control | United States | 1981–1987 | 3078/1931 | Breast | Diazepam ≥ 6 month vs. never-use | 1.0 (0.6–1.7) |
| Kaufman_1 (1990) [13] | Case-control | Canada | 1982–1986 | 607/1214 | Breast | Diazepam ≥ 6 month vs. never-use | 0.8 (0.5–1.3) |
| Harlow (1995) [14] | Case-control | United States | 1978–1987 | 450/454 | Ovarian | Benzodiazepine vs. never-use | 1.8 (1.0–3.1) |
| Rosenberg (1995) [15] | Case-control | United States | 1977–1991 | 382/5695 | Non-Hodgkin’s lymphoma | Benzodiazepine ≥ 1 month vs. never- use | 2.1 (1.4–3.3) |
| Hardell (1996) [16] | Case-control | Sweden | 1984–1986 | 329/658 | Colon | Benzodiazepine vs. never-use | 1.7 (0.9-3.3) |
| Westerdahl (1996) [17] | Case-control | Sweden | 1988–1990 | 400/640 | Malignant melanoma | Benzodiazepine vs. never-use | 1.8 (0.7–4.4) |
| Friedman (1998) [18] | Case-control | United States | 1991–1994 | 1993/2410 | Colon | Diazepam ≥ 12 month vs. never-use | 1.2 (0.8–1.8) |
| Coogan (2000) [19] | Case-control | United States | 1976–1998 | 748/2992 | Ovarian | Benzodiazepine < 12 month vs. never-use | 1.4 (1.0–2.1) |
| Lagergen (2000) [20] | Case-control | Sweden | 1995–1997 | 189/820 | Esophageal | Benzodiazepine vs. never-use | 1.5 (0.7–2.9) |
| Dublin (2002) [21] | Case-control | United States | 1981–1997 | 314/790 | Ovarian | Benzodiazepine < 6 month vs. never-use | 0.70 (0.47–1.0) |
| Pogoda (2004) [22] | Case-control | United States | 1987–1994 | 412/412 | Acute myeloid leukemia | Benzodiazepine ≥ 6 month vs. never-use | 1.5 (0.6–3.7) |
| Halapy (2006) [23] | Case-control | Canada | 1996–1998 | 3133/3062 | Breast | Benzodiazepine vs. never-use | 1.06 (0.88–1.27) |
| Landgren (2006) [24] | Case-control | United States | 1997–2002 | 179/691 | Multiple myeloma | Benzodiazepine ≥ 6 month vs. never-use | 0.9 (0.3–2.6) |
| Fortuny (2007) [25] | Case-control | United States | 1980–2002 | 114/3996 | Esophageal | Benzodiazepine vs. never-use | 1.7 (0.9–3.1) |
| Kripke (2012) [26] | Prospective cohort | United States | 2002–2007 | 2076 cases among 25,750 | All cancers | Any hypnotic > 132 pill/year vs. non-users | 1.35 (1.18–1.55) |
| Kao_B (2012) [27] | Prospective cohort | Taiwan | 1996–2000 | 3520 cases among 119,239 | All cancers | Benzodiazepine ≥ 2 month vs. non-users | 1.19 (1.08–1.32) |
| Kao_Z (2012) [28] | Prospective cohort | Taiwan | 1998–2000 | 1047/2924 | All cancers | Zolpidem vs. never-use | 1.68 (1.55–1.82) |
| Pottegard (2012) [29] | Case-control | Denmark | 2002–2009 | 149360/1194729 | All cancers | All benzodiazepine any related drugs (cumulative amount ≥ 500 defined daily dose) vs. never use | 1.09 (1.04–1.14) |
| Jaussent (2013) [30] | Prospective cohort | France | 1999–2011 | 1454 cases among 6696 | All cancers | Hypnotic vs. never-use | 0.96 (0.74–1.23) |
| Harnod_B (2014) [31] | Prospective cohort | Taiwan | 2000–2009 | 274 cases among 62,050 | Brain cancer | Benzodiazepine ≥ 2 month vs. never-use | 3.15 (2.37–4.20) |
| Harnod_Z (2015) [32] | Prospective cohort | Taiwan | 2000–2009 | 37810/37810 | Brain cancer | Zolpidem ≥ 520 mg/year vs. never-use | 1.85 (1.21–2.82) |
| Iqbal (2014) [33] | Case-control | Taiwan | 1998–2009 | 42500/255000 | All cancers | Benzodiazepine ≥ 2 month vs. never-use | 1.21 (1.18–1.24) |
| Hung (2016) [34] | Case-control | Taiwan | 2006–2011 | 1454/1448 | Hepatocellular carcinoma | Clonazepam vs. never-use | 0.93 (0.76–1.13) |
| Lin (2016) [35] | Prospective cohort | Taiwan | 2002–2004 | 1728 cases among 6924 | All cancers | Zolpidem vs. never-use | 1.75 (1.02–3.0) |
| Lai (2017) [36] | Case-control | Taiwan | 2011–2012 | 77986/77986 | Hepatocellular carcinoma | Benzodiazepine vs. never-use | 1.5 (1.45–2.44) |
| Thygesen (2017) [37] | Case-control | Danish | 2002–2009 | 1854/4950 | All cancers | Benzodiazepine > 500 DDD (1–5 years) vs. never-use | 1.09 (1.00–1.19) |
| Lai (2019) [38] | Case-control | Taiwan | 2000–2013 | 4912/4912 | Colorectal | Zolpidem vs. never-use | 1.05 (0.95–1.15) |
Abbreviation: OR, odds ratio; RR, relative risk; CI, confidence interval; DDD, defined daily dose.
Table 3.
Benzodiazepines/Z-drugs use and the risk of cancer in the subgroup meta-analysis by different factors.
Table 3.
Benzodiazepines/Z-drugs use and the risk of cancer in the subgroup meta-analysis by different factors.
| Factors | Study Number | Summary OR or RR (95% CI) | Heterogeneity I2 (%) | Random/Fixed Effects |
|---|---|---|---|---|
| All | 27 | 1.17 (1.09–1.26) | 79% | Random |
| Region | ||||
| America | 14 | 1.15 (0.95–1.36) | 62% | Random |
| Europe | 6 | 1.09 (1.05–1.14) | 0% | Random |
| Asia | 7 | 1.24 (1.09–1.42) | 91% | Random |
| Type of cancer | ||||
| Brain cancer | 5 | 1.93 (1.29–2.88) | 82% | Random |
| Malignant melanoma | 4 | 1.01 (0.78–1.31) | 0% | Fixed |
| Esophagus cancer | 6 | 1.56 (1.32–1.84) | 0% | Fixed |
| Breast cancer | 10 | 1.08 (0.96–1.22) | 61% | Random |
| Liver cancer | 7 | 1.38 (1.17–1.63) | 89% | Random |
| Lung cancer | 5 | 1.24 (1.04–1.48) | 80% | Random |
| Stomach cancer | 3 | 1.18 (1.05–1.34) | 4% | Fixed |
| Pancreatic cancer | 2 | 1.38 (1.20–1.58) | 0% | Fixed |
| Colon cancer | 7 | 1.11 (1.01–1.23) | 59% | Random |
| Ovarian cancer | 7 | 1.07 (0.86–1.33) | 50% | Random |
| Renal cancer | 4 | 1.51 (1.18–1.94) | 60% | Random |
| Prostate cancer | 4 | 1.29 (1.07–1.55) | 70% | Random |
| Gender | ||||
| Female | 9 | 1.01 (0.89–1.14) | 42% | Fixed |
| Male and Female | 19 | 1.22 (1.13–1.32) | 83% | Random |
| Elderly ≥ 65 | 4 | 1.16 (0.92–1.47) | 84% | Random |
| Anxiolytics/ Sedatives | ||||
| Anxiolytics benzodiazepines | 9 | 1.09 (0.95–1.26) | 30% | Random |
| Sedatives benzodiazepines and Z-drugs | 10 | 1.26 (1.10–1.45) | 93% | Random |
| Duration of hypnotics use | ||||
| <6 months | 12 | 1.03 (1.02–1.04) | 35% | Fixed |
| ≥6 months | 13 | 1.05 (1.02–1.08) | 0% | Fixed |
| ≥5 years | 9 | 1.11 (1.02–1.21) | 0% | Fixed |
| Cumulative yearly dose | ||||
| Lower | 5 | 1.03 (1.01–1.05) | 10% | Fixed |
| Moderate | 6 | 1.30 (0.97–1.75) | 95% | Random |
| Highest | 6 | 2.03 (1.19–3.46) | 97% | Random |
| Type of hypnotics | ||||
| Long-acting (Diazepam) | 8 | 0.97 (0.93–1.01) | 37% | Fixed |
| Intermediate-acting | 4 | 1.21 (0.93–1.57) | 88% | Random |
| Short-acting | 9 | 1.29 (1.12–1.48) | 92% | Random |
| Methodological quality | ||||
| High quality | 19 | 1.14 (1.04–1.25) | 92% | Random |
| Low quality | 10 | 1.59 (1.27–1.98) | 85% | Random |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Peng, T.-R.; Yang, L.-J.; Wu, T.-W.; Chao, Y.-C. Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Medicina 2020, 56, 513. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100513
AMA Style
Peng T-R, Yang L-J, Wu T-W, Chao Y-C. Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Medicina. 2020; 56(10):513. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100513
Chicago/Turabian StylePeng, Tzu-Rong, Li-Jou Yang, Ta-Wei Wu, and You-Chen Chao. 2020. "Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies" Medicina 56, no. 10: 513. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100513