Critical Care Demand and Intensive Care Supply for Patients in Japan with COVID-19 at the Time of the State of Emergency Declaration in April 2020: A Descriptive Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Infectious Disease Data Source
2.3. Intensive Care Unit Capacity Data Source
2.4. Board-Certified Intensivists and Patient Numbers in ICUs in Seven Regions in Japan According to the JSICM and CRISIS
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| WHO | World Health Organization |
| ECMO | Extracorporeal membranous oxygenation |
| COVID-19 | Coronavirus induced disease 2019 |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| ICU | Intensive care unit |
| JSICM | The Japanese Society of Intensive Care Medicine |
| CRISIS | CRoss Icu Searchable Information System |
| IQR | Interquartile range |
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 30 September 2020).
- Cabinet Secretariat. Japan’s Response to the Novel Coronavirus Disease: Declaration of a State of Emergency. 2020. Available online: https://corona.go.jp/en/ (accessed on 30 September 2020).
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.-F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Hong, X.; Xiong, J.; Feng, Z.; Shi, Y. Extracorporeal membrane oxygenation (ECMO): Does it have a role in the treatment of severe COVID-19? Int. J. Infect. Dis. 2020, 94, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Firstenberg, M.S.; Stahel, P.F.; Hanna, J.; Kotaru, C.; Crossno, J., Jr.; Forrester, J. Successful COVID-19 rescue therapy by extra-corporeal membrane oxygenation (ECMO) for respiratory failure: A case report. Patient Saf. Surg. 2020, 14, 1–7. [Google Scholar] [CrossRef]
- Taniguchi, H.; Ogawa, F.; Honzawa, H.; Yamaguchi, K.; Niida, S.; Shinohara, M.; Takahashi, K.; Iwashita, M.; Abe, T.; Kubo, S.; et al. Veno-venous extracorporeal membrane oxygenation for severe pneumonia: COVID-19 case in Japan. Acute Med. Surg. 2020, 7, e509. [Google Scholar] [CrossRef] [Green Version]
- MacLaren, G.; Fisher, D.; Brodie, D. Preparing for the Most Critically Ill Patients With COVID-19. JAMA 2020, 323, 1245. [Google Scholar] [CrossRef]
- Hartman, M.E.; Hernandez, R.A.; Patel, K.; Wagner, T.E.; Trinh, T.; Lipke, A.B.; Yim, E.T.; Pulido, J.N.; Pagel, J.M.; Youssef, S.J.; et al. COVID-19 Respiratory Failure: Targeting Inflammation on VV-ECMO Support. ASAIO J. 2020, 66, 603–606. [Google Scholar] [CrossRef]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.-C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients With Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [Green Version]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lu, F.; Zhou, M.; Qi, Z.; Chen, Z. Tracheal intubation in patients with severe and critical COVID-19: Analysis of 18 cases. J. South. Med. Univ. 2020, 40, 337–341. [Google Scholar] [CrossRef]
- Sun, P.; Qie, S.; Liu, Z.; Ren, J.; Li, K.; Xi, J. Clinical characteristics of hospitalized patients with SARS-CoV-2 infection: A single arm meta-analysis. J. Med. Virol. 2020, 92, 612–617. [Google Scholar] [CrossRef] [Green Version]
- Qiu, H.; China Critical Care Clinical Trials Group (CCCCTG); Tong, Z.; Ma, P.; Hu, M.; Peng, Z.; Wu, W.; Du, B. Intensive care during the coronavirus epidemic. Intensiv. Care Med. 2020, 46, 576–578. [Google Scholar] [CrossRef] [Green Version]
- Devereaux, A.; Christian, M.D.; Dichter, J.R.; Geiling, J.A.; Rubinson, L. Summary of Suggestions from the Task Force for Mass Critical Care Summit, January 26–27, 2007. Chest 2008, 133, 1S–7S. [Google Scholar] [CrossRef]
- Rubinson, L.; Hick, J.L.; Curtis, J.R.; Branson, R.D.; Burns, S.; Christian, M.D.; Devereaux, A.V.; Dichter, J.R.; Talmor, D.; Erstad, B.; et al. Definitive Care for the Critically Ill During a Disaster: Medical Resources for Surge Capacity. Chest 2008, 133, 32S–50S. [Google Scholar] [CrossRef]
- Li, R.; Rivers, C.; Tan, Q.; Murray, M.B.; Toner, E.; Lipsitch, M. Estimated Demand for US Hospital Inpatient and Intensive Care Unit Beds for Patients with COVID-19 Based on Comparisons With Wuhan and Guangzhou, China. JAMA Netw. Open 2020, 3, e208297. [Google Scholar] [CrossRef]
- Japan ECMOnet for COVID-19; Shime, N. Save the ICU and save lives during the COVID-19 pandemic. J. Intensiv. Care 2020, 8, 1–3. [Google Scholar] [CrossRef]
- Worldometer. Japan Coronavirus. Available online: https://www.worldometers.info/coronavirus/country/japan/ (accessed on 30 September 2020).
- Japan ECMOnet for COVID-19. Status of Severe COVID-19 Patients. Available online: https://crisis.ecmonet.jp/ (accessed on 30 September 2020).
- Osamu, N. 2020. Available online: https://www.covid19-jma-medical-expert-meeting.jp/topic/1121 (accessed on 30 September 2020). (In Japanese).
- Japanese Society of Intensive Care Medicine; Society of Respiratory Care Medicine; Japan Association for Clinical Engineer. Estimate of the Number of Ventilator, Etc, in Japanese Hospitals. Available online: https://www.jsicm.org/news/news200514.html (accessed on 30 September 2020).
- Setti, L.; Passarini, F.; De Gennaro, G.; Barbieri, P.; Perrone, M.G.; Borelli, M.; Palmisani, J.; Di Gilio, A.; Piscitelli, P.; Miani, A. Airborne Transmission Route of COVID-19: Why 2 Meters/6 Feet of Inter-Personal Distance Could Not Be Enough. Int. J. Environ. Res. Public Health 2020, 17, 2932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, E.L.; Turnham, P.; Griffin, J.R.; Clarke, C.C. Consideration of the Aerosol Transmission for COVID-19 and Public Health. Risk Anal. 2020, 40, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.; Norton, A.; Young, F.P.; Collins, D.W. Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: A narrative review. Anaesthesia 2020. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nat. Cell Biol. 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Wang, J.; Feng, H.; Zhang, S.; Ni, Z.; Ni, L.; Chen, Y.; Zhuo, L.; Zhong, Z.; Qu, T. SARS-CoV-2 RNA detection of hospital isolation wards hygiene monitoring during the Coronavirus Disease 2019 outbreak in a Chinese hospital. Int. J. Infect. Dis. 2020, 94, 103–106. [Google Scholar] [CrossRef]
- Wax, R.S.; Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can. J. Anesth. 2020, 67, 568–576. [Google Scholar] [CrossRef] [Green Version]
- Ferioli, M.; Cisternino, C.; Leo, V.; Pisani, L.; Palange, P.; Nava, S. Protecting healthcare workers from SARS-CoV-2 infection: Practical indications. Eur. Respir. Rev. 2020, 29, 200068. [Google Scholar] [CrossRef]
- Chigurupati, R.; Panchal, N.; Henry, A.M.; Batal, H.; Sethi, A.; D’Innocenzo, R.; Mehra, P.; Krishnan, D.G.; Roser, S.M. Considerations for Oral and Maxillofacial Surgeons in COVID-19 Era: Can We Sustain the Solutions to Keep Our Patients and Healthcare Personnel Safe? J. Oral Maxillofac. Surg. 2020, 78, 1241–1256. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour, and Welfare. Status of Designation of Class II Designated Medical Institutions for Infectious Diseases. 2019. Available online: https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou15/02-02-01.html (accessed on 30 September 2020).
- Haeck, J.D.; Dongelmans, D.A.; Schultz, M.J. ECMO Centers and Mortality From Influenza A(H1N1). JAMA 2012, 307. [Google Scholar] [CrossRef] [PubMed]
- Brodie, D.; Bacchetta, M. Extracorporeal Membrane Oxygenation for ARDS in Adults. N. Engl. J. Med. 2011, 365, 1905–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Society of Respiratory Care Medicine. ECMO Project. Available online: http://square.umin.ac.jp/jrcm/contents/ecmo/index.html (accessed on 30 September 2020).
- Statistics Bureau of Japan. Population Statistics on 2019. Available online: https://www.stat.go.jp/data/jinsui/2019np/index.html (accessed on 30 September 2020).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Lois, M. The shortage of critical care physicians: Is there a solution? J. Crit. Care 2014, 29, 1121–1122. [Google Scholar] [CrossRef] [PubMed]
- Gutsche, J.T.; Kohl, B.A. Who should care for intensive care unit patients? Crit. Care Med. 2007, 35, S18–S23. [Google Scholar] [CrossRef]
- Hokkaido Government. Declarations a State of Emergency in Hokkaido. 2020. Available online: http://www.pref.hokkaido.lg.jp/ss/tkk/koronasengen.htm (accessed on 30 September 2020).
- Takeda, S.; Kotani, T.; Nakagawa, S.; Ichiba, S.; Aokage, T.; Ochiai, R.; Taenaka, N.; Kawamae, K.; Nishimura, M.; Ujike, Y.; et al. Extracorporeal membrane oxygenation for 2009 influenza A(H1N1) severe respiratory failure in Japan. J. Anesthesia 2012, 26, 650–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Checkley, W. Extracorporeal Membrane Oxygenation as a First-Line Treatment Strategy for ARDS. JAMA 2011, 306, 1703–1704. [Google Scholar] [CrossRef]
- Noah, A.M.; Peek, G.J.; Finney, S.J.; Griffiths, M.J.; Harrison, D.; Grieve, R.; Sadique, Z.; Sekhon, J.S.; McAuley, D.F.; Firmin, R.K.; et al. Referral to an Extracorporeal Membrane Oxygenation Center and Mortality Among Patients With Severe 2009 Influenza A(H1N1). JAMA 2011, 306, 1659–1668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laudi, S.; Busch, T.; Kaisers, U. Extracorporeal membrane oxygenation for ARDS due to 2009 influenza A(H1N1). JAMA 2010, 303, 941. [Google Scholar] [CrossRef] [PubMed]
- Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA 2009, 302, 1888–1895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Japan ECMOnet for COVID-19. Japan ECMOnet for COVID-19: Telephone consultations for cases with severe respiratory failure caused by COVID-19. J. Intensiv. Care 2020, 8, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Japan ECMOnet for COVID-19. Nationwide system to centralize decisions around ECMO use for severe COVID-19 pneumonia in Japan (Special Correspondence). J. Intensiv. Care 2020, 8, 1–2. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hokkaido | Tohoku | Kanto- Koshinetsu | Tokai- Hokuriku | Kansai | Chugoku- Shikoku | Kyusyu- Okinawa | Japan | |
|---|---|---|---|---|---|---|---|---|
| Prefecture | 1 | 6 | 10 | 7 | 6 | 9 | 8 | 47 |
| Population (105 adults) | 468.5 | 769.8 | 4287 | 1565.3 | 1805.4 | 966.6 | 1233.4 | 11,075.4 |
| Category II beds | 92 (0.02) | 171 (0.022) | 531 (0.012) | 220 (0.014) | 238 (0.013) | 206 (0.021) | 300 0.024) | 1758 (0.016) |
| Category II and TB beds | 153 (0.033) | 261 (0.034) | 937 (0.022) | 513 (0.033) | 616 (0.034) | 397 (0.041) | 625 (0.051) | 3502 (0.032) |
| Intensivist | 75 (0.016) | 95 (0.012) | 727 (0.017) | 233 (0.015) | 368 (0.02) | 228 (0.024) | 231 (0.019) | 1957 (0.018) |
| Category II institution | 24 (0.005) | 40 (0.005) | 91 (0.002) | 46 (0.003) | 39 (0.002) | 42 (0.004) | 69 (0.006) | 351 (0.003) |
| ECMO project hospital * | 4 (0.0085) | 8 (0.0104) | 35 (0.0082) | 11 (0.007) | 24 (0.0133) | 6 (0.0062) | 12 (0.0097) | 100 (0.009) |
| Hokkaido | Tohoku | Kanto- Koshinetsu | Tokai- Hokuriku | Kansai | Chugoku- Shikoku | Kyusyu- Okinawa | Japan | |
|---|---|---|---|---|---|---|---|---|
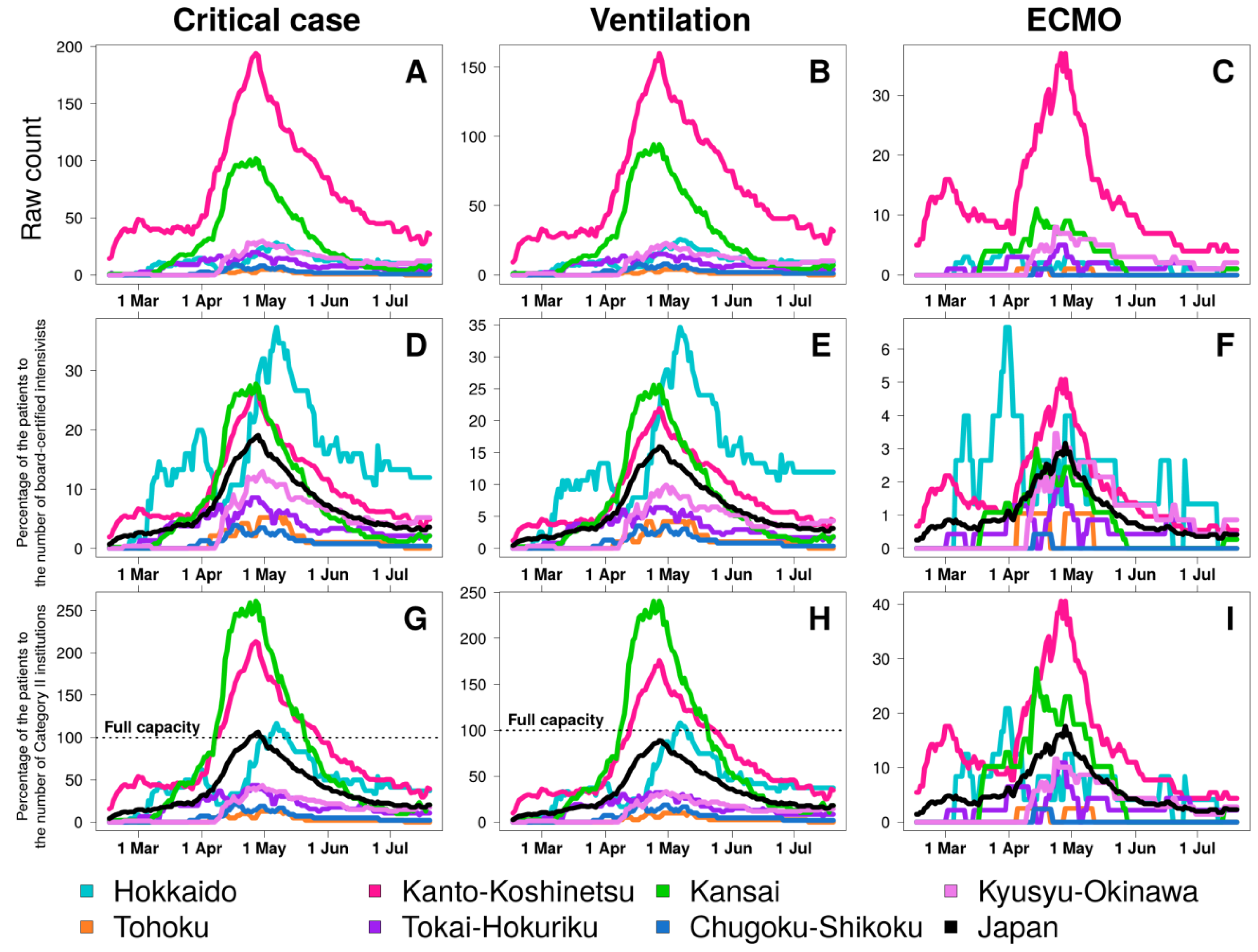
| critical case | 1766 [8, 10, 13] | 200 [0, 1, 2] | 11,805 [40, 51, 106] | 1318 [5, 8, 12] | 4587 [6, 17, 48] | 367 [0, 2, 3] | 1662 [1, 10, 17] | 21,705 [68, 96, 197] |
| ventilation | 1547 [7, 9, 12] | 170 [0, 1, 1] | 9820 [30, 44, 93] | 1102 [4, 7, 10] | 4188 [6, 14, 44] | 358 [0, 2, 3] | 1310 [1, 9, 14] | 18,495 [58, 83, 174] |
| ECMO | 219 [1, 1, 2] | 30 [0, 0, 0] | 1985 [7, 10, 16] | 216 [1, 1, 2] | 399 [0, 0, 4] | 9 [0, 0, 0] | 352 [0, 2, 3] | 3210 [11, 15, 27] |
| Hokkaido | Tohoku | Kanto- Koshinetsu | Tokai- Hokuriku | Kansai | Chugoku- Shikoku | Kyusyu- Okinawa | Japan | |
|---|---|---|---|---|---|---|---|---|
| Intensivist | ||||||||
| critical case | 37.3 | 5.3 | 26.7 | 8.6 | 27.7 | 3.9 | 13 | 19.1 |
| ventilation | 34.7 | 4.2 | 22 | 6.4 | 25.5 | 3.5 | 10 | 15.9 |
| ECMO | 6.7 | 1.1 | 5.1 | 2.1 | 3 | 0.4 | 3.5 | 3.2 |
| Category II institution | ||||||||
| critical case | 116.7 | 12.5 | 213.2 | 43.5 | 261.5 | 21.4 | 43.5 | 106.3 |
| Ventilation | 108.3 | 10 | 175.8 | 32.6 | 241 | 19 | 33.3 | 88.9 |
| ECMO | 20.8 | 2.5 | 40.7 | 10.9 | 28.2 | 2.4 | 11.6 | 17.7 |
| ECMO project | ||||||||
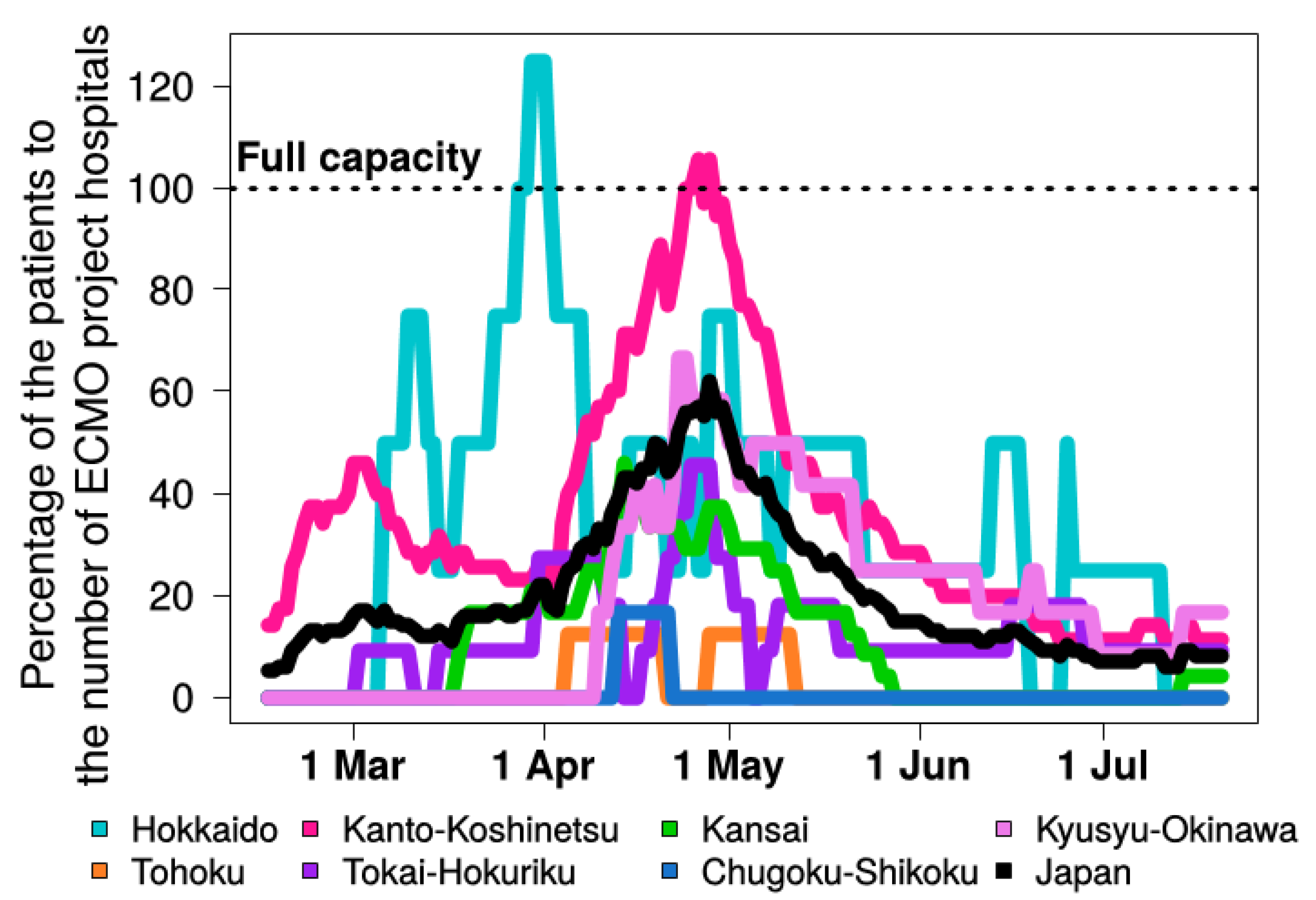
| ECMO | 125 | 12.5 | 105.7 | 45.5 | 45.8 | 16.7 | 66.7 | 62 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujii, Y.; Hirota, K. Critical Care Demand and Intensive Care Supply for Patients in Japan with COVID-19 at the Time of the State of Emergency Declaration in April 2020: A Descriptive Analysis. Medicina 2020, 56, 530. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100530
Fujii Y, Hirota K. Critical Care Demand and Intensive Care Supply for Patients in Japan with COVID-19 at the Time of the State of Emergency Declaration in April 2020: A Descriptive Analysis. Medicina. 2020; 56(10):530. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100530
Chicago/Turabian StyleFujii, Yosuke, and Kiichi Hirota. 2020. "Critical Care Demand and Intensive Care Supply for Patients in Japan with COVID-19 at the Time of the State of Emergency Declaration in April 2020: A Descriptive Analysis" Medicina 56, no. 10: 530. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100530