Three-Dimensional Volumetric Changes and Clinical Outcomes after Decompression with DIAM™ Implantation in Patients with Degenerative Lumbar Spine Diseases


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Surgical Technique
2.3. Clinical Outcomes and Radiographic Parameters
2.4. 3D MRI for Volume Assessmentt
2.5. Statistical Analysis
3. Results
3.1. Clinical Outcomes
3.2. Radiographic Outcome
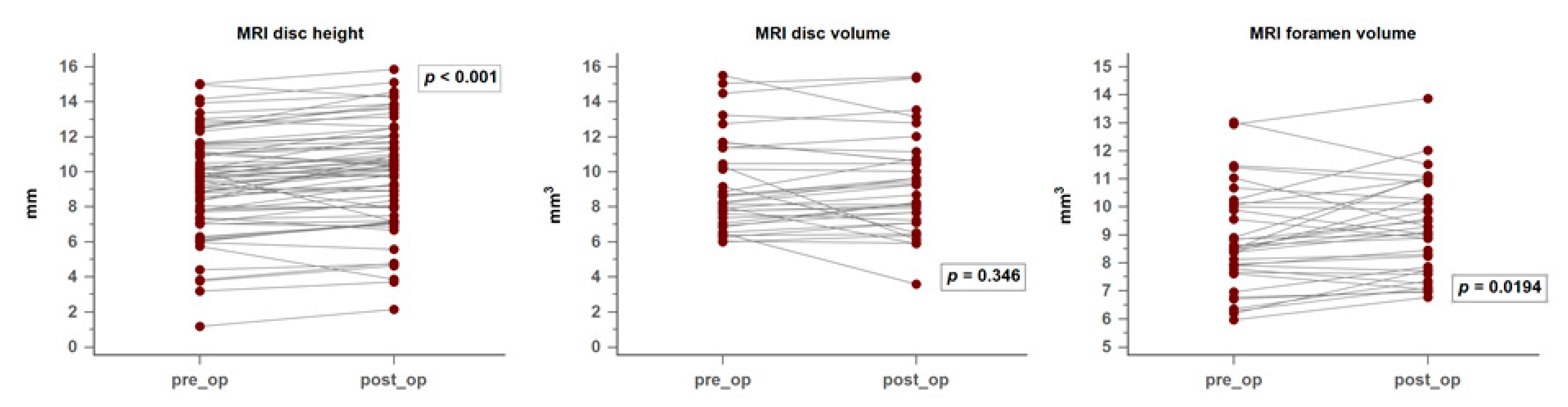
3.3. MRI and 3D Volumetric Outcomes
3.4. Correlation between Clinical Symptoms and Image Findings
3.5. Illustrative Case
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ravindra, V.M.; Senglaub, S.S.; Rattani, A.; Dewan, M.C.; Hartl, R.; Bisson, E.; Park, K.B.; Shrime, M.G. Degenerative Lumbar Spine Disease: Estimating Global Incidence and Worldwide Volume. Glob. Spine J. 2018, 8, 784–794. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.; Luo, J.; Huang, J.; Lian, C.; Zhou, H.; Yao, H.; Su, P. Interspinous spacers versus posterior lumbar interbody fusion for degenerative lumbar spinal diseases: A meta-analysis of prospective studies. Int. Orthop. 2016, 40, 1135–1142. [Google Scholar] [CrossRef]
- Segura-Trepichio, M.; Martin-Benlloch, A.; Manuel Montoza-Nunez, J.; Candela-Zaplana, D.; Nolasco, A. Lumbar disc herniation surgery with microdiscectomy plus interspinous stabilization: Good clinical results, but failure to lower the incidence of re-operation. J. Clin. Neurosci. 2018, 51, 29–34. [Google Scholar] [CrossRef]
- Fabrizi, A.P.; Maina, R.; Schiabello, L. Interspinous spacers in the treatment of degenerative lumbar spinal disease: Our experience with DIAM and Aperius devices. Eur. Spine J. 2011, 20, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Pintauro, M.; Duffy, A.; Vahedi, P.; Rymarczuk, G.; Heller, J. Interspinous implants: Are the new implants better than the last generation? A review. Curr. Rev. Musculoskelet. Med. 2017, 10, 189–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo, Z.; Li, D.; Zhang, R.; Chang, M.; Yang, B.; Tang, S. Comparative effectiveness and safety of posterior lumbar interbody fusion, Coflex, Wallis, and X-stop for lumbar degenerative diseases: A systematic review and network meta-analysis. Clin. Neurol. Neurosurg. 2018, 172, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.; Liliang, P.C.; Wang, H.K.; Liang, C.L.; Chen, J.S.; Chen, T.B.; Wang, K.-W.; Chen, H.-J. Reduction in adjacent-segment degeneration after multilevel posterior lumbar interbody fusion with proximal DIAM implantation. J. Neurosurgery: Spine 2015, 23, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, H.; Fogel, G.R.; Zhu, J.; Liao, Z.; Liu, W. Biomechanical Analysis of Different Lumbar Interspinous Process Devices: A Finite Element Study. World Neurosurg. 2019, 127, e1112–e1119. [Google Scholar] [CrossRef]
- Phan, K.; Rao, P.J.; Ball, J.R.; Mobbs, R.J. Interspinous process spacers versus traditional decompression for lumbar spinal stenosis: Systematic review and meta-analysis. J. Spine Surg. 2016, 2, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Gazzeri, R.; Galarza, M.; Neroni, M.; Fiore, C.; Faiola, A.; Puzzilli, F.; Callovini, G.M.; Alfieri, A. Failure rates and complications of interspinous process decompression devices: A European multicenter study. Neurosurg. Focus 2015, 39, E14. [Google Scholar] [CrossRef] [Green Version]
- Fransen, P. Long-term results with percutaneous interspinous process devices in the treatment of neurogenic intermittent claudication. J. Spine Surg. 2017, 3, 620–623. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, D.P.; Swanson, K.E.; Fuchs, P.; Hsu, K.Y.; Zucherman, J.F.; Yerby, S.A. The effects of an interspinous implant on the kinematics of the instrumented and adjacent levels in the lumbar spine. Spine 2003, 28, 2192–2197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, F.M.; Voronov, L.I.; Gaitanis, I.N.; Carandang, G.; Havey, R.M.; Patwardhan, A.G. Biomechanics of posterior dynamic stabilizing device (DIAM) after facetectomy and discectomy. Spine J. 2006, 6, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Vanti, C.; Prosperi, D.; Boschi, M. The Prolo Scale: History, evolution and psychometric properties. J. Orthop. Traumatol. 2013, 14, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.H.; Choi, W.G.; Hwang, B.W.; Tsang, Y.S.; Chung, E.R.; Lee, H.C.; Lee, S.-J. Microscopic anterior foraminal decompression combined with anterior lumbar interbody fusion. Spine J. 2013, 13, 1190–1199. [Google Scholar] [CrossRef]
- Rao, P.J.; Maharaj, M.M.; Phan, K.; Lakshan Abeygunasekara, M.; Mobbs, R.J. Indirect foraminal decompression after anterior lumbar interbody fusion: A prospective radiographic study using a new pedicle-to-pedicle technique. Spine J. 2015, 15, 817–824. [Google Scholar] [CrossRef]
- Richards, J.C.; Majumdar, S.; Lindsey, D.P.; Beaupre, G.S.; Yerby, S.A. The treatment mechanism of an interspinous process implant for lumbar neurogenic intermittent claudication. Spine 2005, 30, 744–749. [Google Scholar] [CrossRef]
- Caserta, S.; La Maida, G.A.; Misaggi, B.; Peroni, D.; Pietrabissa, R.; Raimondi, M.T.; Redaelli, A. Elastic stabilization alone or combined with rigid fusion in spinal surgery: A biomechanical study and clinical experience based on 82 cases. Eur. Spine J. 2002, 11, S192–S197. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.M.; Zhou, Y.; Li, Q.L.; Wu, X.L.; Jin, Y.L.; Luo, P.; Chi, Y.-L.; Wang, X.-Y. Interspinous spacer versus traditional decompressive surgery for lumbar spinal stenosis: A systematic review and meta-analysis. PLoS ONE 2014, 9, e97142. [Google Scholar] [CrossRef] [Green Version]
- Tamburrelli, F.C.; Proietti, L.; Logroscino, C.A. Critical analysis of lumbar interspinous devices failures: A retrospective study. Eur. Spine J. 2011, 20, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Chung, K.J.; Hwang, Y.S.; Koh, S.H. Stress fracture of bilateral posterior facet after insertion of interspinous implant. Spine 2009, 34, E380–E383. [Google Scholar] [CrossRef] [PubMed]
- Moojen, W.A.; Arts, M.P.; Jacobs, W.C.; van Zwet, E.W.; van den Akker-van Marle, M.E.; Koes, B.W.; Vleggeert-Lankamp, C.; Peul, W.; for the Leiden-The Hague Spine Intervention Prognostic Study Group (SIPS). Interspinous process device versus standard conventional surgical decompression for lumbar spinal stenosis: Randomized controlled trial. BMJ 2013, 347, f6415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqui, M.; Karadimas, E.; Nicol, M.; Smith, F.W.; Wardlaw, D. Effects of X-STOP device on sagittal lumbar spine kinematics in spinal stenosis. J. Spinal Disord. Tech. 2006, 19, 328–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buric, J.; Pulidori, M. Long-term reduction in pain and disability after surgery with the interspinous device for intervertebral assisted motion (DIAM) spinal stabilization system in patients with low back pain: 4-year follow-up from a longitudinal prospective case series. Eur. Spine J. 2011, 20, 1304–1311. [Google Scholar] [CrossRef] [Green Version]
- Lu, K.; Liliang, P.C.; Wang, H.K.; Chen, J.S.; Chen, T.Y.; Huang, R.; Chen, H.-J. Clinical outcome following DIAM implantation for symptomatic lumbar internal disk disruption: A 3-year retrospective analysis. J. Pain Res. 2016, 9, 917–924. [Google Scholar] [CrossRef] [Green Version]
- Sobottke, R.; Schluter-Brust, K.; Kaulhausen, T.; Rollinghoff, M.; Joswig, B.; Stutzer, H.; Eysel, P.; Simons, P.; Kuchta, J. Interspinous implants (X Stop, Wallis, Diam) for the treatment of LSS: Is there a correlation between radiological parameters and clinical outcome? Eur. Spine J. 2009, 18, 1494–1503. [Google Scholar] [CrossRef] [Green Version]
- Minns, R.J.; Walsh, W.K. Preliminary design and experimental studies of a novel soft implant for correcting sagittal plane instability in the lumbar spine. Spine 1997, 22, 1819–1825. [Google Scholar] [CrossRef]
- Tsai, K.J.; Murakami, H.; Lowery, G.L.; Hutton, W.C. A biomechanical evaluation of an interspinous device (Coflex) used to stabilize the lumbar spine. J. Surg. Orthop. Adv. 2006, 15, 167–172. [Google Scholar]
- Schulte, T.L.; Hurschler, C.; Haversath, M.; Liljenqvist, U.; Bullmann, V.; Filler, T.J.; Osada, N.; Fallenberg, E.-M.; Hackenberg, L. The effect of dynamic, semi-rigid implants on the range of motion of lumbar motion segments after decompression. Eur. Spine J. 2008, 17, 1057–1065. [Google Scholar] [CrossRef] [Green Version]
- Bellini, C.M.; Galbusera, F.; Raimondi, M.T.; Mineo, G.V.; Brayda-Bruno, M. Biomechanics of the lumbar spine after dynamic stabilization. J. Spinal Disord. Tech. 2007, 20, 423–429. [Google Scholar] [CrossRef]
- Siddiqui, M.; Smith, F.W.; Wardlaw, D. One-year results of X Stop interspinous implant for the treatment of lumbar spinal stenosis. Spine 2007, 32, 1345–1348. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, A.; An, H.S.; Lim, T.H.; Haughton, V.M. Morphologic changes in the lumbar intervertebral foramen due to flexion-extension, lateral bending, and axial rotation: An in vitro anatomic and biomechanical study. Spine 2001, 26, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Lee, S.G.; Park, C.W.; Son, S.; Kim, W.K. Long-term Follow-up (Minimum 5 Years) Study of Single-level Posterior Dynamic Stabilization in Lumbar Degenerative Disease; ‘Interspinous U’ & ‘DIAM’. Korean J. Spine 2012, 9, 102–107. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | 50 |
|---|---|
| Age (years old) | 62.1 |
| Gender M/F | 13/37 |
| Radiographic diagnosis | |
| Stenosis | 38 |
| Spondylolisthesis | 29 (all grade I listhesis) |
| Herniated disc | 15 |
| Levels of operation | |
| L2–3 | 4 |
| L3–4 | 2 |
| L4–5 | 24 |
| L2–3 and L3–4 | 3 |
| L3–4 and L4–5 | 15 |
| L2–3, L3–4 and L4–5 | 2 |
| Preoperatively | Postoperatively | Improvement Rate | |
|---|---|---|---|
| Low back pain | 44/50 (88%) | 11/50 (22%) | 75% * |
| Leg pain +/− NIC | 43/50 (86%) | 4/50 (8%) | 90.7% * |
| Soreness | 14 (28%) | 13 (26%) | 7% |
| VAS (mean ± SE) | 3.9 ± 1.7 | 0.9 ± 1.8 | p < 0.05 |
| The Prolo Scale (mean ± SE) | 6.3 ± 0.9 | 8.3 ± 1.4 | p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.-Y.; Chen, M.-Y.; Chang, C.-N.; Yan, J.-L. Three-Dimensional Volumetric Changes and Clinical Outcomes after Decompression with DIAM™ Implantation in Patients with Degenerative Lumbar Spine Diseases. Medicina 2020, 56, 723. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120723
Li C-Y, Chen M-Y, Chang C-N, Yan J-L. Three-Dimensional Volumetric Changes and Clinical Outcomes after Decompression with DIAM™ Implantation in Patients with Degenerative Lumbar Spine Diseases. Medicina. 2020; 56(12):723. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120723
Chicago/Turabian StyleLi, Cheng-Yu, Mao-Yu Chen, Chen-Nen Chang, and Jiun-Lin Yan. 2020. "Three-Dimensional Volumetric Changes and Clinical Outcomes after Decompression with DIAM™ Implantation in Patients with Degenerative Lumbar Spine Diseases" Medicina 56, no. 12: 723. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120723