Relationship between Fatigue and Physical Activity in a Polish Cohort of Multiple Sclerosis Patients


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Fatigue—General Results
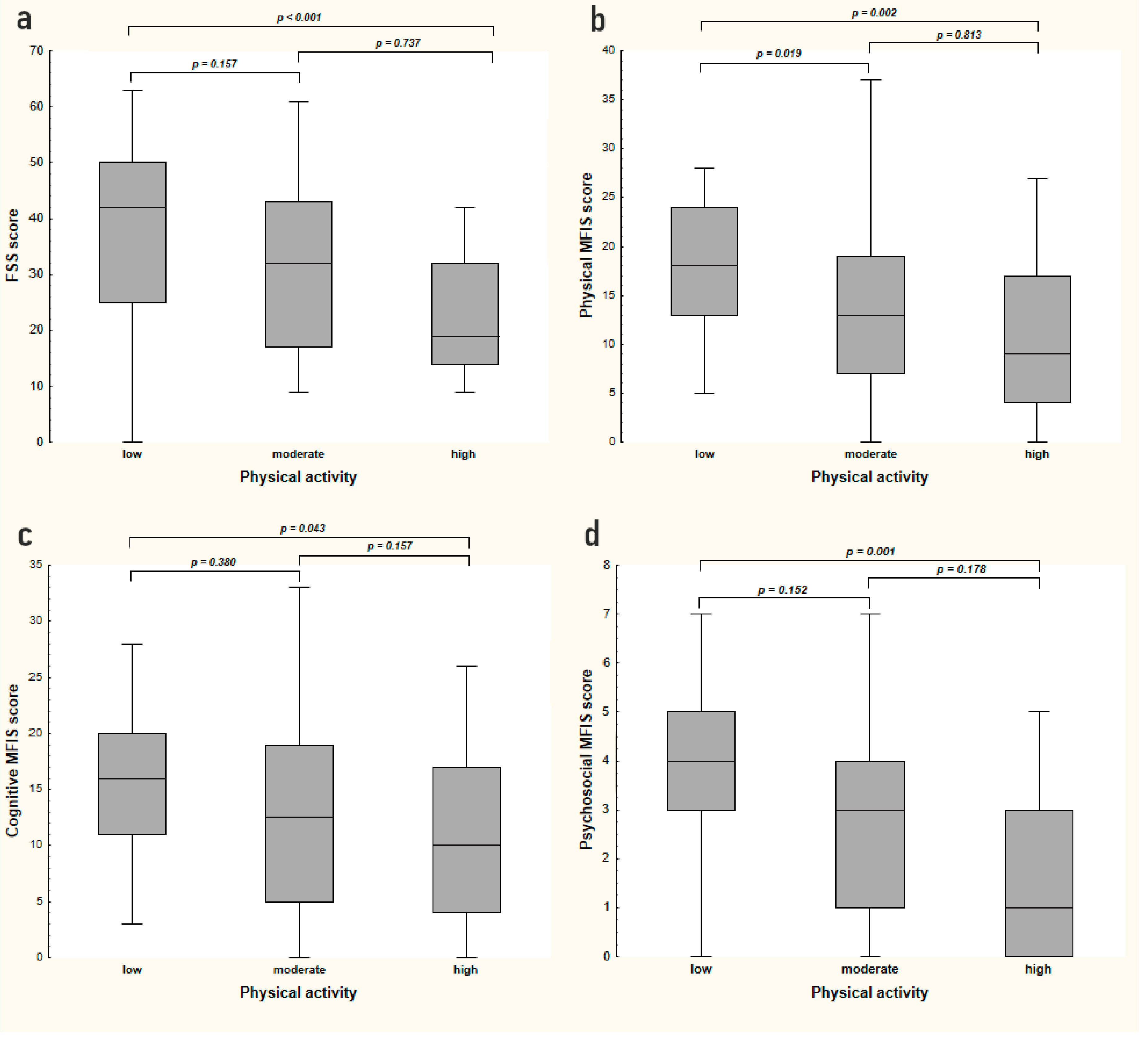
3.2. Fatigue and Physical Activity
3.3. Fatigue and Disability
3.4. Fatigue and Disease Duration
3.5. Fatigue and Professional Status
3.6. Fatigue and Gender, Place of Residence, or Smoking
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Atlas of MS 2013: Mapping Multiple Sclerosis around the World. London: Multiple Sclerosis International Federation. 2013. Available online: http://www.msif.org/about-ms/publications-and-resources/ (accessed on 19 July 2020).
- Lad, S.P.; Chapman, C.H.; Vaninetti, M.; Steinman, L.; Green, A.; Boakye, M. Socioeconomic trends in hospitalization for multiple sclerosis. Neuroepidemiology 2010, 35, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Compston, A.; Coles, A. Multiple sclerosis. Lancet 2008, 372, 1502–1517. [Google Scholar] [CrossRef]
- Guzik, A.; Kwolek, A. The prevalence and distribution of Multiple Sclerosis in Poland and around the world. Przegląd Med. Uniw. Rzesz. Nar. Inst. Leków Warszawie 2015, 1, 55–62. [Google Scholar]
- Garczyński, W. Obraz Kliniczny Chorych na Stwardnienie Rozsiane w Kontekście Rehabilitacji Opartej na Objawach. In Horyzonty Współczesnej Fizjoterapii; Wydawnictwo WSEiT: Poznań, Poland, 2016; pp. 129–143. [Google Scholar]
- Krajewski, S.; Dobek, A.; Zawadka-Kunikowska, M.; Kowalewski, M.; Jakimiec, R.; Kunikowski, K. Zespół przewlekłego zmęczenia problem osób chorych na stwardnienie rozsiane, Hygeia Public Health 2014, 49, 519–525. Hygeia Public Health 2014, 49, 519–525. [Google Scholar]
- Łabuz-Roszak, B.; Kubicka-Baczyk, K.; Pierzchała, K.; Machowska-Majchrzak, A.; Skrzypek, M. Fatigue and its association with sleep disorders, depressive symptoms and anxiety in patients with multiple sclerosis. Neurol. Neurochir. Pol. 2012, 46, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Brola, W.; Fudala, M. Current opinions of pathogenesis and treatment of fatigue syndrome in multiple sclerosis. Aktualności Neurol. 2011, 11, 23–28. [Google Scholar]
- Losy, J. Zmęczenie w stwardnieniu rozsianym. Farm. Psychiatry Neurol. 2005, 3, 279–282. [Google Scholar]
- Ziemssen, T. Multiple sclerosis beyond EDSS: Depression and fatigue. J. Neurol. Sci. 2009, 77 (Suppl. 1), 37–41. [Google Scholar] [CrossRef]
- Brenner, P.; Piehl, F. Fatigue and depression in multiple sclerosis: Pharmacological and non-pharmacological interventions. Acta Neurol. Scand. 2016, 134 (Suppl. 200), 47–54. [Google Scholar] [CrossRef]
- Lerdal, A.; Celius, E.G.; Krupp, L.; Dahl, A.A. A prospective study of patterns of fatigue in multiple sclerosis. Eur. J. Neurol. 2007, 14, 1338–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Gruszczak, A.; Bartosik-Psujek, H.; Pocińska, K.; Stelmasiak, Z. Validation analysis of selected psychometric features of Polish version of Modified Fatigue Impact Scale--preliminary findings. Neurol. Neurochir. Pol. 2009, 43, 148–154. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-country reliability and validity. Med. Sci Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Benedict, R.H.; Fishman, I.; McClellan, M.M.; Bakshi, R.; Weinstock-Guttman, B. Validity of the Beck Depression Inventory-Fast Screen in multiple sclerosis. Mult. Scler. 2003, 9, 393–396. [Google Scholar] [CrossRef]
- Pasiut, S.; Juda, K.; Mirek, E.; Szymura, J. Wpływ rehabilitacji na poziom odczuwanego zmȩczenia u pacjentów ze stwardnieniem rozsianym. Fizjoterapia 2015, 23, 3–10. [Google Scholar] [CrossRef]
- Coghe, G.; Corona, F.; Marongiu, E.; Fenu, G.; Frau, J.; Lorefice, L.; Crisafulli, A.; Galli, M.; Concu, A.; Marrosu, M.G.; et al. Fatigue, as measured using the Modified Fatigue Impact Scale, is a predictor of processing speed improvement induced by exercise in patients with multiple sclerosis: Data from a randomized controlled trial. J. Neurol. 2018, 265, 1328–1333. [Google Scholar] [CrossRef]
- Brola, W.; Fudala, M. Problem zmęczenia w stwardnieniu rozsianym. Przegląd Med. Uniw. Rzesz. 2010, 2, 237–243. [Google Scholar]
- Téllez, N.; Río, J.; Tintoré, M.; Nos, C.; Galán, I.; Montalban, X. Does the Modified Fatigue Impact Scale offer a more comprehensive assessment of fatigue in MS? Mult. Scler. 2005, 11, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Biernat, E.; Stupnicki, R.; Gajewski, A.K. Międzynarodowy Kwestionariusz Aktywności Fizycznej (IPAQ)—Wersja polska. Wych. Fiz. Sport. 2007, 51, 47–54. [Google Scholar]
- Mendes, M.A.; da Silva, I.; Ramires, V.; Reichert, F.; Martins, R.; Ferreira, R.; Tomasi, E. Metabolic equivalent of task (METs) thresholds as an indicator of physical activity intensity. PLoS ONE 2018, 13, e0200701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagaraj, K.; Taly, A.B.; Gupta, A.; Prasad, C.; Christopher, R. Depression and sleep disturbances in patients with multiple sclerosis and correlation with associated fatigue. J. Neurosci. Rural. Pract. 2013, 4, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanisz, A. Accessible Statistics Course Using Statistica PL Examples from Medicine; StatSoft Polska: Kraków, Poland, 2006. [Google Scholar]
- Lobentanz, I.S.; Asenbaum, S.; Vass, K.; Sauter, C.; Klösch, G.; Kollegger, H.; Kristoferitsch, W.; Zeitlhofer, J. Factors influencing quality of life in multiple sclerosis patients: Disability, depressive mood, fatigue and sleep quality. Acta Neurol. Scand. 2004, 110, 6–13. [Google Scholar] [CrossRef]
- Nagaraj, K.; Taly, A.B.; Gupta, A.; Prasad, C.; Christopher, R. Prevalence of fatigue in patients with multiple sclerosis and its effect on the quality of life. J. Neurosci. Rural. Pract. 2013, 4, 278–282. [Google Scholar] [CrossRef]
- Janardhan, V.; Bakshi, R. Quality of life in patients with multiple sclerosis: The impact of fatigue and depression. J. Neurol. Sci. 2002, 205, 51–58. [Google Scholar] [CrossRef]
- Göksel Karatepe, A.; Kaya, T.; Günaydn, R.; Demirhan, A.; Ce, P.; Gedizlioğlu, M. Quality of life in patients with multiple sclerosis: The impact of depression, fatigue, and disability. Int. J. Rehabil. Res. 2011, 34, 290–298. [Google Scholar] [CrossRef]
- Łabuz-Roszak, B.; Kubicka-Baczyk, K.; Pierzchała, K.; Horyniecki, M.; Machowska-Majchrzak, A.; Augustyńska-Mutryn, D.; Kosałka, K.; Michalski, K.; Pyszak, D.; Wach, J. Quality of life in multiple sclerosis—Association with clinical. Psychiatr. Pol. 2013, 3, 433–442. [Google Scholar]
- Runia, T.F.; Jafari, N.; Siepman, D.A.; Hintzen, R.Q. Fatigue at time of CIS is an independent predictor of a subsequent diagnosis of multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2015, 86, 543–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, S., Jr.; Tan, H.; Otahal, P.; Taylor, B.; Ponsonby, A.L.; Lucas, R.M.; Blizzard, L.; Valery, P.C.; Lechner-Scott, J.; Shaw, C.; et al. Anxiety, depression and fatigue at 5-year review following CNS demyelination. Acta Neurol. Scand. 2016, 134, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Kister, I.; Bacon, T.E.; Chamot, E.; Salter, A.R.; Cutter, G.R.; Kalina, J.T.; Herbert, J. Natural history of multiple sclerosis symptoms. Int. J. MS Care 2013, 15, 146–158. [Google Scholar] [CrossRef] [Green Version]
- Patejdl, R.; Penner, I.K.; Noack, T.K.; Zettl, U.K. Multiple sclerosis and fatigue: A review on the contribution of inflammation and immune-mediated neurodegeneration. Autoimmun. Rev. 2016, 15, 210–220. [Google Scholar] [CrossRef]
- Patrick, E.; Christodoulou, C.; Krupp, L.B. New York State MS Consortium. Longitudinal correlates of fatigue in multiple sclerosis. Mult. Scler. 2009, 15, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Braga, D.M.; Prado, G.F.; Bichueti, D.B.; Oliveira, E.M. Positive correlation between functional disability, excessive daytime sleepiness, and fatigue in relapsing-remitting multiple sclerosis. Arq. Neuropsiquiatr. 2016, 74, 433–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pittion-Vouyovitch, S.; Debouverie, M.; Guillemin, F.; Vandenberghe, N.; Anxionnat, R.; Vespignani, H. Fatigue in multiple sclerosis is related to disability, depression and quality of life. J. Neurol. Sci. 2006, 243, 39–45. [Google Scholar] [CrossRef]
- Colosimo, C.; Millefiorini, E.; Grasso, M.G.; Vinci, F.; Fiorelli, M.; Koudriavtseva, T.; Pozzilli, C. Fatigue in MS is associated with specific clinical features. Acta Neurol. Scand. 1995, 92, 353–355. [Google Scholar] [CrossRef]
- Iriarte, J.; Carreño, M.; Castro, P. Fatigue and functional system involvement in multiple sclerosis. Neurologia 1996, 11, 210–215. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: http://apps.who.int/iris/bitstream/10665/44399/1/9789241599979_eng.pdf (accessed on 26 November 2020).
- Langeskov-Christensen, M.; Bisson, E.J.; Finlayson, M.L.; Dalgas, U. Potential pathophysiological pathways that can explain the positive effects of exercise on fatigue in multiple sclerosis: A scoping review. J. Neurol. Sci. 2017, 373, 307–320. [Google Scholar] [CrossRef]
- Andreasen, A.K.; Stenager, E.; Dalgas, U. The effect of exercise therapy on fatigue in multiple sclerosis. Mult. Scler. 2011, 17, 1041–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petajan, J.H.; Gappmaier, E.; White, A.T.; Spencer, M.K.; Mino, L.; Hicks, R.W. Impact of aerobic training on fitness and quality of life in multiple sclerosis. Ann. Neurol. 1996, 39, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Pilutti, L.A.; Greenlee, T.A.; Motl, R.W.; Nickrent, M.S.; Petruzzello, S.J. Effects of exercise training on fatigue in multiple sclerosis: A meta-analysis. Psychosom. Med. 2013, 75, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Mostert, S.; Kesselring, J. Effects of a short-term exercise training program on aerobic fitness, fatigue, health perception and activity level of subjects with multiple sclerosis. Mult. Scler. 2002, 8, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Bansi, J.; Bloch, W.; Gamper, U.; Riedel, S.; Kesselring, J. Endurance training in MS: Short-term immune responses and their relation to cardiorespiratory fitness, health-related quality of life, and fatigue. J. Neurol. 2013, 260, 2993–3001. [Google Scholar] [CrossRef]
- Ozkul, C.; Guclu-Gunduz, A.; Irkec, C.; Fidan, I.; Aydin, Y.; Ozkan, T.; Yazici, G. Effect of combined exercise training on serum brain-derived neurotrophic factor, suppressors of cytokine signaling 1 and 3 in patients with multiple sclerosis. J. Neuroimmunol. 2018, 316, 121–129. [Google Scholar] [CrossRef]
- Edwards, T.; Pilutti, L.A. The effect of exercise training in adults with multiple sclerosis with severe mobility disability: A systematic review and future research directions. Mult. Scler. Relat. Disord. 2017, 16, 31–39. [Google Scholar] [CrossRef]
- Opara, J.; Szwejkowski, W.; Brola, W. Aktualne kierunki rehabilitacji w stwardnieniu rozsianym. Aktual. Neurol. 2009, 9, 140–146. [Google Scholar]
- Latimer-Cheung, A.E.; Pilutti, L.A.; Hicks, A.L.; Martin Ginis, K.A.; Fenuta, A.M.; MacKibbon, K.A.; Motl, R.W. Effects of exercise training on fitness, mobility, fatigue, and health-related quality of life among adults with multiple sclerosis: A systematic review to inform guideline development. Arch. Phys. Med. Rehabil. 2013, 94, 1800–1828.e3. [Google Scholar] [CrossRef]
- Heine, M.; Verschuren, O.; Hoogervorst, E.L.; van Munster, E.; Hacking, H.G.; Visser-Meily, A.; Twisk, J.W.; Beckerman, H.; de Groot, V.; Kwakkel, G.; et al. Does aerobic training alleviate fatigue and improve societal participation in patients with multiple sclerosis? A randomized controlled trial. Mult. Scler. 2017, 23, 1517–1526. [Google Scholar] [CrossRef] [Green Version]
- Blair, S.N.; Morris, J.N. Healthy hearts--and the universal benefits of being physically active: Physical activity and health. Ann. Epidemiol. 2009, 19, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Fulcher, K.Y.; White, P.D. Randomised controlled trial of graded exercise in patients with the chronic fatigue syndrome. BMJ 1997, 314, 1647–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, L.V.; White, P.D. The role of deconditioning and therapeutic exercise in chronic fatigue syndrome (CFS). J. Ment. Health 2005, 14, 237–252. [Google Scholar] [CrossRef]
- Kim, D.Y.; Lee, J.S.; Park, S.Y.; Kim, S.J.; Son, C.G. Systematic review of randomized controlled trials for chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J. Transl. Med. 2020, 18, 7. [Google Scholar] [CrossRef] [Green Version]
- Avellaneda Fernández, A.; Pérez Martín, A.; Izquierdo Martínez, M.; Arruti Bustillo, M.; Barbado Hernández, F.J.; de la Cruz Labrado, J.; Díaz-Delgado Peñas, R.; Gutiérrez Rivas, E.; Palacín Delgado, C.; Rivera Redondo, J.; et al. Chronic fatigue syndrome: Aetiology, diagnosis and treatment. BMC Psychiatry 2009, 9 (Suppl. 1), S1. [Google Scholar] [CrossRef] [Green Version]
- Wallman, K.E.; Morton, A.R.; Goodman, C.; Grove, R. Exercise prescription for individuals with chronic fatigue syndrome. Med. J. Aust. 2005, 183, 142–143. [Google Scholar] [CrossRef]
- Rowe, P.C.; Underhill, R.A.; Friedman, K.J.; Gurwitt, A.; Medow, M.S.; Schwartz, M.S.; Speight, N.; Stewart, J.M.; Vallings, R.; Rowe, K.S. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Diagnosis and Management in Young People: A Primer. Front. Pediatrics 2017, 5, 121. [Google Scholar] [CrossRef] [Green Version]
- Larun, L.; Brurberg, K.G.; Odgaard-Jensen, J.; Price, J.R. Exercise therapy for chronic fatigue syndrome. Cochrane Database Syst. Rev. 2019, 10, CD003200. [Google Scholar] [CrossRef]
- Bjørkum, T.; Wang, C.E.; Waterloo, K. Patients’ experience with treatment of chronic fatigue syndrome. Tidsskr. Nor. Laegeforen. 2009, 129, 1214–1216. [Google Scholar] [CrossRef]
- Twisk, F.N.; Maes, M. A review on cognitive behavorial therapy (CBT) and graded exercise therapy (GET) in myalgic encephalomyelitis (ME)/chronic fatigue syndrome (CFS): CBT/GET is not only ineffective and not evidence-based, but also potentially harmful for many patients with ME/CFS. Neuro. Endocrinol. Lett. 2009, 30, 284–299. [Google Scholar]
- Twisk, F.N. Objective Evidence of Post-exertional “Malaise” in Myalgic Encephalomyelitis and Chronic Fatigue Syndrome. J. Sports Med. Doping Stud. 2015, 5, 159. [Google Scholar] [CrossRef]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jason, L.A.; Ohanian, D.; Brown, A.; Sunnquist, M.; McManimen, S.; Klebek, L.; Fox, P.; Sorenson, M. Differentiating Multiple Sclerosis from Myalgic Encephalomyelitis and Chronic Fatigue Syndrome. Insights Biomed. 2017, 2, 11. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.M.; Arnett, P.A. Factors related to employment status changes in individuals with multiple sclerosis. Mult. Scler. 2005, 11, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B. Fatigue in multiple sclerosis: Definition, pathophysiology and treatment. CNS Drugs 2003, 17, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.F.; Quaal, C.; Reeves, M.A. Effects of multiple sclerosis on occupational and career patterns. Axone 1991, 13, 16–22. [Google Scholar]
- Mills, R.J.; Young, C.A.; Pallant, J.F.; Tennant, A. Development of a patient reported outcome scale for fatigue in multiple sclerosis: The Neurological Fatigue Index (NFI-MS). Health Qual. Life Outcomes 2010, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Flachenecker, P.; Kümpfel, T.; Kallmann, B.; Gottschalk, M.; Grauer, O.; Rieckmann, P.; Trenkwalder, C.; Toyka, K.V. Fatigue in multiple sclerosis: A comparison of different rating scales and correlation to clinical parameters. Mult. Scler. 2002, 8, 523–526. [Google Scholar] [CrossRef]
- Iriarte, J.; Subirá, M.L.; Castro, P. Modalities of fatigue in multiple sclerosis: Correlation with clinical and biological factors. Mult. Scler. 2000, 6, 124–130. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Whole Group (n = 100) | Fatigued (n = 42) | Non-Fatigued (n = 58) | p |
|---|---|---|---|---|
| Gender n (%) | ||||
| Women | 78 (78%) | 85.7% | 72.4% | 0.110 * |
| Men | 22 (22%) | 14.2% | 27.6% | |
| Age (years) (mean ± SD) | 38.8 ± 9.8 | 41.0 ± 9.4 | 37.3 ± 9.9 | 0.071 † |
| Marital status n (%) | ||||
| Single | 40 (40%) | 33.3% | 44.8% | 0.247 * |
| In relationship | 60 (60%) | 55.2% | 44.8% | |
| Place of residence n (%) | ||||
| Rural areas | 12 (12%) | 14.3% | 10.3% | |
| Town (population): | ||||
| up to 50,000 | 18 (18%) | 14.3% | 20.7% | 0.616 * |
| 50,000–99,999 | 18 (18%) | 14.3% | 20.7% | |
| 100,000 and more | 52 (52%) | 57.1% | 48.3% | |
| Smoking n (%) | ||||
| Yes | 12 (12%) | 4.8% | 17.2% | 0.058 * |
| No | 88 (88%) | 95.2% | 82.8% | |
| Education n (%) | ||||
| Vocational | 12 (12%) | 19.0% | 6.9% | |
| Secondary | 32 (32%) | 42.9% | 24.1% | 0.007 * |
| Higher | 56 (56%) | 38.1% | 69.0% | |
| Duration of the disease (years) (mean ± SD) | 8.19 ± 6.34 | 9.6 ± 5.2 | 7.1 ± 6.9 | 0.003 ‡ |
| EDSS (mean ± SD) | 2.5 ± 1.5 | 3.0 ± 1.6 | 2.2 ± 1.4 | 0.002 ‡ |
| MET (mean ± SD) | 2234 ± 2865 | 1294 ± 2317 | 2860 ± 3038 | <0.001 ‡ |
| MFIS total score (mean ± SD) | 30.0 ± 17.0 | 42.4 ± 13.0 | 21.2 ± 13.7 | <0.001 † |
| MFIS physical score (mean ± SD) | 14.1 ± 8.4 | 19.9 ± 6.4 | 10.0 ± 7.1 | <0.001 ‡ |
| MFIS cognitive score (mean ± SD) | 13.2 ± 8.0 | 18.6 ± 7.0 | 9.4 ± 6.3 | <0.001 † |
| MFIS psychosocial score (mean ± SD) | 2.8 ± 2.0 | 4.1 ± 1.4 | 1.8 ± 1.7 | <0.001 ‡ |
| Characteristics | FSS Score | MFIS Total Score | MFIS Physical Score | MFIS Psychosocial Score | MFIS Cognitive Score | |
|---|---|---|---|---|---|---|
| Age | R | 0.17 * | 0.27 † | 0.32 * | 0.38 * | 0.18 † |
| p | 0.09 | 0.00 | 0.00 | 0.00 | 0.09 | |
| Place of residence | R | 0.00 * | 0.02 * | −0.02 * | 0.02 * | 0.03 * |
| p | 0.97 | 0.84 | 0.88 | 0.86 | 0.76 | |
| Smoking | R | −0.04 * | −0.02 * | 0.01 * | 0.02 * | −0.11 * |
| p | 0.70 | 0.86 | 0.95 | 0.83 | 0.28 | |
| Education | R | −0.21 * | −0.23 * | −0.21 * | −0.28 * | −0.21 * |
| p | 0.04 | 0.02 | 0.03 | 0.01 | 0.03 | |
| Duration of the disease | R | 0.30 * | 0.27 * | 0.37 * | 0.37 * | 0.29 * |
| p | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | |
| IPAQ (MET) | R | −0.38 * | −0.33 * | −0.36 * | −0.36 * | −0.25 * |
| p | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | |
| EDSS | R | 0.36 * | 0.45 * | 0.49 * | 0.54 * | 0.29 * |
| p | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzepka, M.; Toś, M.; Boroń, M.; Gibas, K.; Krzystanek, E. Relationship between Fatigue and Physical Activity in a Polish Cohort of Multiple Sclerosis Patients. Medicina 2020, 56, 726. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120726
Rzepka M, Toś M, Boroń M, Gibas K, Krzystanek E. Relationship between Fatigue and Physical Activity in a Polish Cohort of Multiple Sclerosis Patients. Medicina. 2020; 56(12):726. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120726
Chicago/Turabian StyleRzepka, Michalina, Mateusz Toś, Michał Boroń, Katarzyna Gibas, and Ewa Krzystanek. 2020. "Relationship between Fatigue and Physical Activity in a Polish Cohort of Multiple Sclerosis Patients" Medicina 56, no. 12: 726. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120726