The Role of Blood Biomarkers for Magnetic Resonance Imaging Diagnosis of Traumatic Brain Injury

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
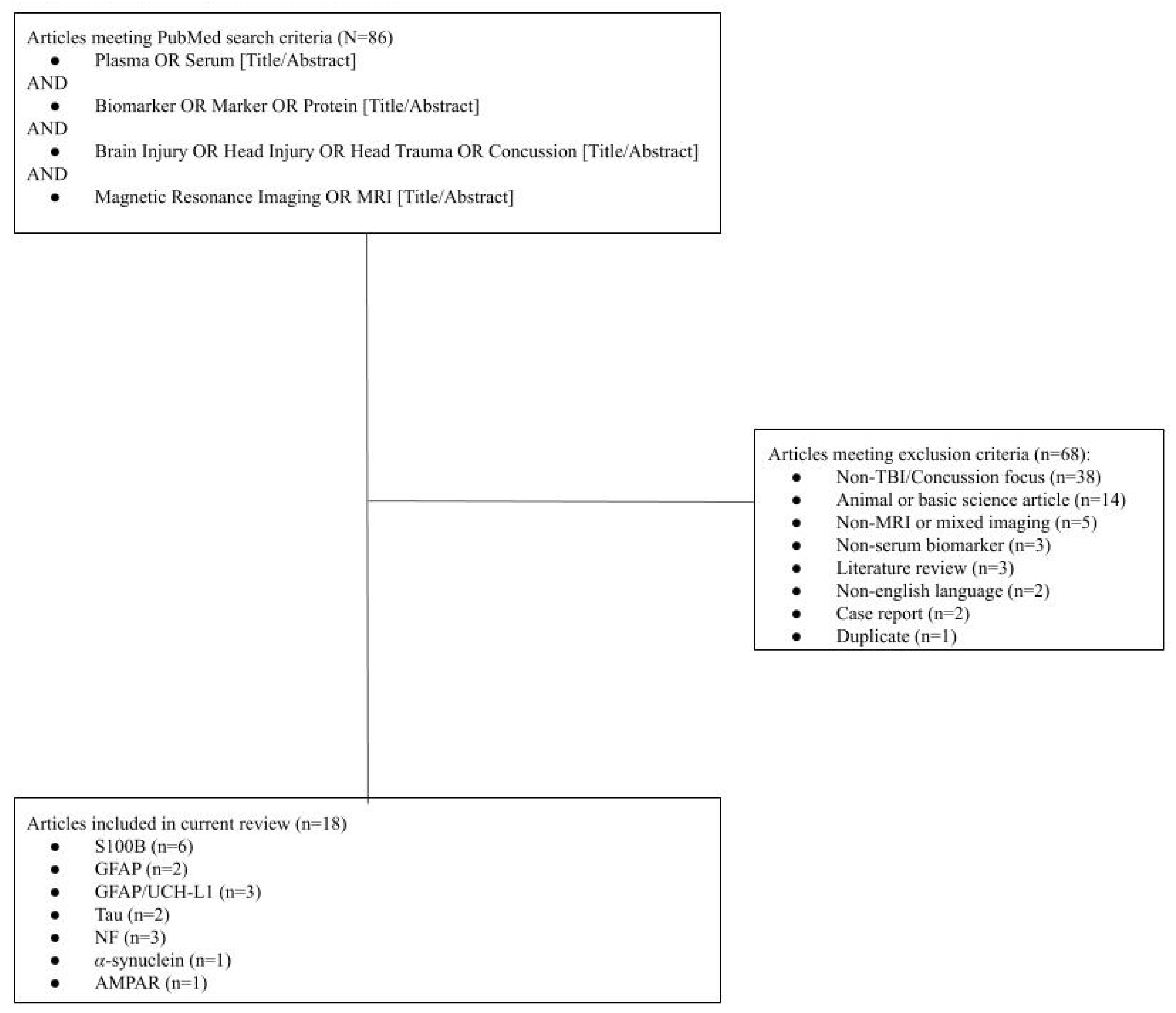
2.1. Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Article Summary
3. Results
3.1. S100 Calcium-Binding Protein B (S100B; 6 Studies)
3.2. Glial Fibrillary Acidic Protein (GFAP; 5 Studies)
3.3. Ubiquitin Carboxy-Terminal Hydrolase L1 (UCH-L1; 2 Studies)
3.4. Neurofilament Proteins (NF-L; 3 Studies)
3.5. Tau Protein (2 Studies)
3.6. Alpha-Synuclein (α-Synuclein; 1 Study)
3.7. Alpha-Amino-3-Hydroxy-5-Methyl-4-Isoxazolepropionic Acid Receptor Peptide (AMPAR; 1 Study)
4. Discussion
4.1. Relevance of MRI-Based TBI Diagnosis and Rationale for Serum Biomarker Use
4.2. GFAP Has High Diagnostic Potential for MRI
4.3. Tau Has Possible Diagnostic Potential for MRI
4.4. Biomarkers in Need of Further Research for Diagnostic Potential on MRI
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Taylor, C.A.; Bell, J.M.; Breiding, M.J.; Xu, L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths - United States, 2007 and 2013. MMWR Surveill. Summ. 2017, 66, 1–16. [Google Scholar] [CrossRef]
- Faul, M.; Coronado, V. Epidemiology of Traumatic Brain Injury. Handb. Clin. Neurol. 2015, 127, 3–13. [Google Scholar] [PubMed]
- Papa, L.; Edwards, D.; Ramia, M. Exploring serum biomarkers for mild traumatic brain injury. In Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects; Kobeissy, F.H., Ed.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2015; ISBN 9781466565982. [Google Scholar]
- Rabinowitz, A.R.; Levin, H.S. Cognitive sequelae of traumatic brain injury. Psychiatr. Clin. N. Am. 2014, 37, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagoda, A.S.; Bazarian, J.J.; Bruns, J.J., Jr.; Cantrill, S.V.; Gean, A.D.; Howard, P.K.; Ghajar, J.; Riggio, S.; Wright, D.W.; Wears, R.L.; et al. Clinical policy: Neuroimaging and decisionmaking in adult mild traumatic brain injury in the acute setting. Ann. Emerg. Med. 2008, 52, 714–748. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M.; Curio, N.; Jost, S.; Wunderlich, M.T.; Synowitz, H.; Wallesch, C.W. Protein S-100B and neuron specific enolase as early neurobiochemical markers of the severity of traumatic brain injury. Restor. Neurol. Neurosci. 1999, 14, 109–114. [Google Scholar] [PubMed]
- Ingebrigtsen, T.; Waterloo, K.; Jacobsen, E.A.; Langbakk, B.; Romner, B. Traumatic brain damage in minor head injury: Relation of serum S-100 protein measurements to magnetic resonance imaging and neurobehavioral outcome. Neurosurgery 1999, 45, 468–475; discussion 475–476. [Google Scholar] [CrossRef] [PubMed]
- Romner, B.; Ingebrigtsen, T.; Kongstad, P.; Børgesen, S.E. Traumatic brain damage: Serum S-100 protein measurements related to neuroradiological findings. J. Neurotrauma 2000, 17, 641–647. [Google Scholar] [CrossRef]
- Oh, E.-J.; Kim, Y.-M.; Jegal, D.-W.; Kahng, J.; Park, Y.-J.; Han, K. Diagnostic value of Elecsys S100 as a marker of acute brain injury in the emergency department. J. Clin. Lab. Anal. 2007, 21, 387–392. [Google Scholar] [CrossRef]
- Thelin, E.P.; Nelson, D.W.; Bellander, B.-M. Secondary peaks of S100B in serum relate to subsequent radiological pathology in traumatic brain injury. Neurocrit. Care 2014, 20, 217–229. [Google Scholar] [CrossRef]
- Linsenmaier, U.; Wirth, S.; Kanz, K.-G.; Geyer, L.L. Imaging minor head injury (MHI) in emergency radiology: MRI highlights additional intracranial findings after measurement of trauma biomarker S-100B in patients with normal CCT. Br. J. Radiol. 2016, 89, 20150827. [Google Scholar] [CrossRef] [Green Version]
- Marchi, N.; Bazarian, J.J.; Puvenna, V.; Janigro, M.; Ghosh, C.; Zhong, J.; Zhu, T.; Blackman, E.; Stewart, D.; Ellis, J.; et al. Consequences of repeated blood-brain barrier disruption in football players. PLoS ONE 2013, 8, e56805. [Google Scholar] [CrossRef] [PubMed]
- Papa, L.; Silvestri, S.; Brophy, G.M.; Giordano, P.; Falk, J.L.; Braga, C.F.; Tan, C.N.; Ameli, N.J.; Demery, J.A.; Dixit, N.K.; et al. GFAP out-performs S100β in detecting traumatic intracranial lesions on computed tomography in trauma patients with mild traumatic brain injury and those with extracranial lesions. J. Neurotrauma 2014, 31, 1815–1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hol, E.M.; Pekny, M. Glial fibrillary acidic protein (GFAP) and the astrocyte intermediate filament system in diseases of the central nervous system. Curr. Opin. Cell Biol. 2015, 32, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Posti, J.P.; Hossain, I.; Takala, R.S.K.; Liedes, H.; Newcombe, V.; Outtrim, J.; Katila, A.J.; Frantzén, J.; Ala-Seppälä, H.; Coles, J.P.; et al. Glial Fibrillary Acidic Protein and Ubiquitin C-Terminal Hydrolase-L1 Are Not Specific Biomarkers for Mild CT-Negative Traumatic Brain Injury. J. Neurotrauma 2017. [Google Scholar] [CrossRef] [PubMed]
- Kou, Z.; Gattu, R.; Kobeissy, F.; Welch, R.D.; O’Neil, B.J.; Woodard, J.L.; Ayaz, S.I.; Kulek, A.; Kas-Shamoun, R.; Mika, V.; et al. Combining biochemical and imaging markers to improve diagnosis and characterization of mild traumatic brain injury in the acute setting: Results from a pilot study. PLoS ONE 2013, 8, e80296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, P.J.; Panczykowski, D.M.; Yue, J.K.; Puccio, A.M.; Inoue, T.; Sorani, M.D.; Lingsma, H.F.; Maas, A.I.R.; Valadka, A.B.; Yuh, E.L.; et al. Measurement of the glial fibrillary acidic protein and its breakdown products GFAP-BDP biomarker for the detection of traumatic brain injury compared to computed tomography and magnetic resonance imaging. J. Neurotrauma 2015, 32, 527–533. [Google Scholar] [CrossRef] [Green Version]
- Gill, J.; Latour, L.; Diaz-Arrastia, R.; Motamedi, V.; Turtzo, C.; Shahim, P.; Mondello, S.; DeVoto, C.; Veras, E.; Hanlon, D.; et al. Glial fibrillary acidic protein elevations relate to neuroimaging abnormalities after mild TBI. Neurology 2018, 91, e1385–e1389. [Google Scholar] [CrossRef]
- Yue, J.K.; Yuh, E.L.; Korley, F.K.; Winkler, E.A.; Sun, X.; Puffer, R.C.; Deng, H.; Choy, W.; Chandra, A.; Taylor, S.R.; et al. Association between plasma GFAP concentrations and MRI abnormalities in patients with CT-negative traumatic brain injury in the TRACK-TBI cohort: A prospective multicentre study. Lancet Neurol. 2019, 18, 953–961. [Google Scholar] [CrossRef]
- Mondello, S.; Jeromin, A.; Buki, A.; Bullock, R.; Czeiter, E.; Kovacs, N.; Barzo, P.; Schmid, K.; Tortella, F.; Wang, K.K.; et al. Glial neuronal ratio: A novel index for differentiating injury type in patients with severe traumatic brain injury. J. Neurotrauma 2012, 29, 1096–1104. [Google Scholar] [CrossRef]
- Day, I.N.M.; Thompson, R.J. UCHL1 (PGP 9.5): Neuronal biomarker and ubiquitin system protein. Prog. Neurobiol. 2010, 90, 327–362. [Google Scholar] [CrossRef]
- Barry, D.M.; Millecamps, S.; Julien, J.-P.; Garcia, M.L. New movements in neurofilament transport, turnover and disease. Exp. Cell Res. 2007, 313, 2110–2120. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, J.; Zetterberg, H.; Mitsis, M.; Blennow, K.; Skoglund, T. Serum Neurofilament Light Protein as a Marker for Diffuse Axonal Injury: Results from a Case Series Study. J. Neurotrauma 2017, 34, 1124–1127. [Google Scholar] [CrossRef] [PubMed]
- Al Nimer, F.; Thelin, E.; Nyström, H.; Dring, A.M.; Svenningsson, A.; Piehl, F.; Nelson, D.W.; Bellander, B.-M. Comparative Assessment of the Prognostic Value of Biomarkers in Traumatic Brain Injury Reveals an Independent Role for Serum Levels of Neurofilament Light. PLoS ONE 2015, 10, e0132177. [Google Scholar] [CrossRef] [PubMed]
- Sandsmark, D.K.; Bogoslovsky, T.; Qu, B.-X.; Haber, M.; Cota, M.R.; Davis, C.; Butman, J.A.; Latour, L.L.; Diaz-Arrastia, R. Changes in Plasma von Willebrand Factor and Cellular Fibronectin in MRI-Defined Traumatic Microvascular Injury. Front. Neurol. 2019, 10, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellani, R.J.; Perry, G. Tau Biology, Tauopathy, Traumatic Brain Injury, and Diagnostic Challenges. J. Alzheimers Dis. 2019, 67, 447–467. [Google Scholar] [CrossRef] [Green Version]
- Hirad, A.A.; Bazarian, J.J.; Merchant-Borna, K.; Garcea, F.E.; Heilbronner, S.; Paul, D.; Hintz, E.B.; van Wijngaarden, E.; Schifitto, G.; Wright, D.W.; et al. A common neural signature of brain injury in concussion and subconcussion. Sci. Adv. 2019, 5, eaau3460. [Google Scholar] [CrossRef] [Green Version]
- Tomita, K.; Nakada, T.-A.; Oshima, T.; Motoshima, T.; Kawaguchi, R.; Oda, S. Tau protein as a diagnostic marker for diffuse axonal injury. PLoS ONE 2019, 14, e0214381. [Google Scholar] [CrossRef]
- Ye, L.; Zhang, D.; Shao, M.; Zhao, P.; Yin, B.; Zhuang, J.; Wang, F.; Yan, Z.; Bai, G. Lower Posttraumatic α-Synuclein Level Associated With Altered Default Mode Network Connectivity Following Acute Mild Traumatic Brain Injury. Front. Neural Circuits 2019, 13, 26. [Google Scholar] [CrossRef]
- Goforth, P.B.; Ellis, E.F.; Satin, L.S. Enhancement of AMPA-mediated current after traumatic injury in cortical neurons. J. Neurosci. 1999, 19, 7367–7374. [Google Scholar] [CrossRef]
- Spaethling, J.M.; Klein, D.M.; Singh, P.; Meaney, D.F. Calcium-permeable AMPA receptors appear in cortical neurons after traumatic mechanical injury and contribute to neuronal fate. J. Neurotrauma 2008, 25, 1207–1216. [Google Scholar] [CrossRef]
- Dimou, S.; Lagopoulos, J. Toward objective markers of concussion in sport: A review of white matter and neurometabolic changes in the brain after sports-related concussion. J. Neurotrauma 2014, 31, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Dambinova, S.A.; Shikuev, A.V.; Weissman, J.D.; Mullins, J.D. AMPAR peptide values in blood of nonathletes and club sport athletes with concussions. Mil. Med. 2013, 178, 285–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). Available online: https://www.cdc.gov/ (accessed on 12 December 2019).
- Pearson, W.S.; Sugerman, D.E.; McGuire, L.C.; Coronado, V.G. Emergency department visits for traumatic brain injury in older adults in the United States: 2006-08. West. J. Emerg. Med. 2012, 13, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Yuh, E.L.; Mukherjee, P.; Lingsma, H.F.; Yue, J.K.; Ferguson, A.R.; Gordon, W.A.; Valadka, A.B.; Schnyer, D.M.; Okonkwo, D.O.; Maas, A.I.R.; et al. Magnetic resonance imaging improves 3-month outcome prediction in mild traumatic brain injury. Ann. Neurol. 2013, 73, 224–235. [Google Scholar] [CrossRef]
- Despotović, I.; Goossens, B.; Philips, W. MRI segmentation of the human brain: Challenges, methods, and applications. Comput. Math. Methods Med. 2015, 2015, 450341. [Google Scholar] [CrossRef] [Green Version]
- Rheault, F.; De Benedictis, A.; Daducci, A.; Maffei, C.; Tax, C.M.W.; Romascano, D.; Caverzasi, E.; Morency, F.C.; Corrivetti, F.; Pestilli, F.; et al. Tractostorm: The what, why, and how of tractography dissection reproducibility. Hum. Brain Mapp. 2020. [Google Scholar] [CrossRef] [Green Version]
- Seabury, S.A.; Gaudette, É.; Goldman, D.P.; Markowitz, A.J.; Brooks, J.; McCrea, M.A.; Okonkwo, D.O.; Manley, G.T.; Adeoye, O.; Badjatia, N.; et al. Assessment of Follow-up Care After Emergency Department Presentation for Mild Traumatic Brain Injury and Concussion: Results From the TRACK-TBI Study. JAMA Netw. Open 2018, 1, e180210. [Google Scholar] [CrossRef]
- Trifan, G.; Gattu, R.; Haacke, E.M.; Kou, Z.; Benson, R.R. MR imaging findings in mild traumatic brain injury with persistent neurological impairment. Magn. Reson. Imaging 2017, 37, 243–251. [Google Scholar] [CrossRef]
- Stein, M.B.; Jain, S.; Giacino, J.T.; Levin, H.; Dikmen, S.; Nelson, L.D.; Vassar, M.J.; Okonkwo, D.O.; Diaz-Arrastia, R.; Robertson, C.S.; et al. Risk of Posttraumatic Stress Disorder and Major Depression in Civilian Patients After Mild Traumatic Brain Injury: A TRACK-TBI Study. JAMA Psychiatry 2019, 76, 249–258. [Google Scholar] [CrossRef]
- Yue, J.K.; Burke, J.F.; Upadhyayula, P.S.; Winkler, E.A.; Deng, H.; Robinson, C.K.; Pirracchio, R.; Suen, C.G.; Sharma, S.; Ferguson, A.R.; et al. Selective Serotonin Reuptake Inhibitors for Treating Neurocognitive and Neuropsychiatric Disorders Following Traumatic Brain Injury: An Evaluation of Current Evidence. Brain Sci. 2017, 7, 93. [Google Scholar] [CrossRef] [Green Version]
- Yue, J.K.; Vassar, M.J.; Lingsma, H.F.; Cooper, S.R.; Okonkwo, D.O.; Valadka, A.B.; Gordon, W.A.; Maas, A.I.R.; Mukherjee, P.; Yuh, E.L.; et al. Transforming research and clinical knowledge in traumatic brain injury pilot: Multicenter implementation of the common data elements for traumatic brain injury. J. Neurotrauma 2013, 30, 1831–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Y.S.; Schuster, J.M.; Smith, D.H.; Stein, S.C. Cost-Effectiveness of Biomarker Screening for Traumatic Brain Injury. J. Neurotrauma 2019, 36, 2083–2091. [Google Scholar] [CrossRef] [PubMed]
- Calcagnile, O.; Anell, A.; Undén, J. The addition of S100B to guidelines for management of mild head injury is potentially cost saving. BMC Neurol. 2016, 16, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, R.D.; Ayaz, S.I.; Lewis, L.M.; Unden, J.; Chen, J.Y.; Mika, V.H.; Saville, B.; Tyndall, J.A.; Nash, M.; Buki, A.; et al. Ability of Serum Glial Fibrillary Acidic Protein, Ubiquitin C-Terminal Hydrolase-L1, and S100B To Differentiate Normal and Abnormal Head Computed Tomography Findings in Patients with Suspected Mild or Moderate Traumatic Brain Injury. J. Neurotrauma 2016, 33, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Papa, L.; Brophy, G.M.; Welch, R.D.; Lewis, L.M.; Braga, C.F.; Tan, C.N.; Ameli, N.J.; Lopez, M.A.; Haeussler, C.A.; Mendez Giordano, D.I.; et al. Time Course and Diagnostic Accuracy of Glial and Neuronal Blood Biomarkers GFAP and UCH-L1 in a Large Cohort of Trauma Patients With and Without Mild Traumatic Brain Injury. JAMA Neurol. 2016, 73, 551–560. [Google Scholar] [CrossRef] [Green Version]
- Bazarian, J.J.; Biberthaler, P.; Welch, R.D.; Lewis, L.M.; Barzo, P.; Bogner-Flatz, V.; Gunnar Brolinson, P.; Büki, A.; Chen, J.Y.; Christenson, R.H.; et al. Serum GFAP and UCH-L1 for prediction of absence of intracranial injuries on head CT (ALERT-TBI): A multicentre observational study. Lancet Neurol. 2018, 17, 782–789. [Google Scholar] [CrossRef]
- Evaluation of Automatic Class III Designation For Banyan Brain Trauma Indicator: Decision Memorandum. Available online: https://www.accessdata.fda.gov/cdrh_docs/reviews/DEN170045.pdf (accessed on 19 December 2019).
- Undén, L.; Calcagnile, O.; Undén, J.; Reinstrup, P.; Bazarian, J. Validation of the Scandinavian guidelines for initial management of minimal, mild and moderate traumatic brain injury in adults. BMC Med. 2015, 13, 292. [Google Scholar] [CrossRef] [Green Version]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [Green Version]
- Winter, C.; Bell, C.; Whyte, T.; Cardinal, J.; Macfarlane, D.; Rose, S. Blood-brain barrier dysfunction following traumatic brain injury: Correlation of K(trans) (DCE-MRI) and SUVR (99mTc-DTPA SPECT) but not serum S100B. Neurol. Res. 2015, 37, 599–606. [Google Scholar] [CrossRef]
- Rubenstein, R.; Chang, B.; Yue, J.K.; Chiu, A.; Winkler, E.A.; Puccio, A.M.; Diaz-Arrastia, R.; Yuh, E.L.; Mukherjee, P.; Valadka, A.B.; et al. Comparing Plasma Phospho Tau, Total Tau, and Phospho Tau-Total Tau Ratio as Acute and Chronic Traumatic Brain Injury Biomarkers. JAMA Neurol. 2017, 74, 1063–1072. [Google Scholar] [CrossRef]


{kind=link}
| S100B | |||||||
| Author and Year | Study Type | N | MRI Acquisition Parameters | Description | Outcome Measures | Timing of Serum Sampling | Results |
| Ingebrigtsen et al., 1999 | Prospective Cohort | 50 TBI | 0.5 T magnet; T1/T2 FLAIR | Validation of S100 as a serum biomarker for brain injury. | Serum S100B | On admission and 12 h post-injury | In total, 14/50 (28%) of patients had detected serum S100 (mean 0.4 ug/L ± 0.3), with levels being highest immediately after injury and declining each hour after. S100B not detectable in 36% of patients after 6 h of initial detection. There were five MRI+ patients with brain contusions—of which have had elevated S100B. |
| Linsenmaier et al., 2016 | Prospective Cohort | 41 TBI | 1.5 T magnet; T1/T2; GRE; DWI | Feasibility study of S100B as biomarker in mTBI with MRI. | Serum S100B CT; MRI | Hourly, until 12 h post-injury | In total, 27/32 (84%) of patients with very high serum S100B serum were MRI-negative and 4/27 with high S100B were CT+. Five MRI+ patients had elevated S100B. S100B sensitivity 100% with specificity of 81%. |
| Marchi et al., 2013 | Prospective Cohort | 15 athletes | 3 T magnet; DTI | Serum S100B in college football players with MRI. | Serum S100B; MRI; neurocognitive tests | Before and after sports season | S100B post-game was elevated (0.51 ± 0.05 ng/mL) compared to baseline. Higher number of impacts correlated with increased S100B (p = 0.03). High S100B auto-antibodies correlated (r = 0.58, p = 0.07) with errors in impulse control |
| Oh et al., 2007 | Prospective Cohort | 101 TBI | unspecified | Serum S100B in patients admitted to EDt for TBI with CT/MRI. | Serum S100B; CT; MRI | On admission | Healthy controls had serum S100B 0.080 ug/L (0.049–0.094) compared to 0.150 ug/L (0.088–0.358) in acute TBI. 66/101 CT/MRI+ patients had higher S100B compared to CT/MRI-negative (p = 0.028). AT cutoff of 0.105 ug/L, sensitivity 84.8% and specificity 74.3% for detecting acute TBI. |
| Romner et al., 2000 | Prospective Cohort | 278 TBI | unspecified | Neurotrauma patients were evaluated for S100B levels on admission and compared with pathological findings on CT scan. | Serum S100B; CT; MRI | On admission | 108/278 (39%) had elevated serum S100 and 25 (9%) were CT+. Serum S100B was higher in severe compared to mild-to-moderate TBI (p < 0.001). S100B was higher in those with intracranial pathology (p < 0.01). Sensitivity for CT/MRI+ was 92%, specificity was 66%. |
| Thelin et al., 2014 | Retrospective Cohort | 199 TBI | T1/T2; FLAIR; GRE | An analysis of serum increases in S100B levels post-TBI in addition to pathological imaging. | Serum S100B; CT; MRI | Three samples, with 1/3 taken > 48 h after injury | Secondary increases in S100B with a cutoff of 0.05 ug/L had sensitivity 80% and specificity 89%, while cutoff of 0.5 ug/L has sensitivity 16% and specificity 98% for imaging findings of TBI. |
| GFAP, UCH-L1 | |||||||
| Author and Year | Study Type | N | MRI Acquisition Parameters | Description | Outcome Measures | Timing of Serum Sampling | Results |
| Gill et al., 2018 | Prospective Cohort | 277 mTBI | T1/T2; FLAIR; 3D-T1; DTI | Plasma biomarkers were correlated with MRI data. | Plasma GFAP; tau; NFL; UCH-L1 | Within 48 h of injury | mTBI had higher plasma GFAP, tau, and NF-L (p < 0.01). Patients with MRI findings had significantly higher concentrations of plasma GFAP, tau, and NF-L compared to MRI- and CT- mTBI patients (p < 0.05). |
| Kou et al., 2013 | Prospective Cohort | Nine mTBI | 3 T magnet; T1/T2; GRE; FLAIR; DTI | Feasibility testing of the utilization of both biomarkers and MRI to detect mTBI. | Serum UCH-L1 and GFAP levels; MRI data | Within 6 h of injury, and q6 h until 24 h post-injury | UCH-L1 (4.9-fold) and GFAP (10.6-fold) were elevated on admission in comparison to lab reference values. Patients with intracranial hemorrhages had higher GFAP compared to non-hemorrhage (p = 0.002). GFAP/UCH-L1 did not associate with MRI findings. |
| McMahon et al., 2015 | Prospective Cohort | 215 TBI | unspecified | Plasma GFAP-BDPs were used to predict CT/MRI+ TBI. | Plasma GFAP-BDPs; MRI | Within 24 h of injury | In total, 35% had evidence of TBI on MRI (n = 21). On admission, MRI+ patients had significantly higher GFAP-BDPs (1.3 ± 1.8 ng/m; p = 0.001 L) than MRI− (0.28 ± 0.57). Plasma concentrations of GFAP-BDPs predicted evidence of MRI pathology (OR 2.7; 95% CI 1.2–5.7). |
| Posti et al., 2017 | Prospective Cohort | 94 mTBI | 3 T magnet; T1/T2; FLAIR; DTI; 3D-T1 | Plasma GFAP, UCH-L1 in TBI were compared to orthopedic trauma. | Serum GFAP and UCH-L1; CT/MRI | On days 1,2,3,7 post-admission | None in the mTBI group showed signs of TBI on MRI. GFAP was initially higher in acute orthopedic trauma compared to acute CT−/MRI− mTBI (p = 0.026) with no difference days later. No difference in UCH-L1. |
| Yue et al., 2019 | Prospective Cohort | 450 TBI, 122 orthopedic and 207 healthy controls | T1/T2; FLAIR; GRE | Patients with negative initial CT, with MRI at 7–18 days, vs. orthopedic trauma controls and healthy controls. | Plasma GFAP and MRI | Within 24 h of injury | CT−/MRI+ (414.5 pg/mL; p < 0.001) patients had the highest plasma GFAP, compared to CT−/MRI− (74.0), orthopedic trauma (13.1) and healthy controls (8.0). AUC for discriminating MRI+ in CT− population was 0.852. GFAP was notably elevated for DAI on MRI, compared to other types of intracranial pathology. |
| Tau | |||||||
| Author and Year | Study Type | N | MRI Acquisition Parameters | Description | Outcome Measures | Timing of Serum Sampling | Results |
| Hirad et al., 2019 | Retrospective Cohort | 29 mTBI | 3 T magnet; 3D-T1; DTI | NCAA contact sport athletes with mTBI were monitored for concussion with plasma sampling and cognitive testing pre-/post-season. | White matter structural integrity using FA pre- and post-season, vs. age-matched controls, correlation between plasma tau and midbrain FA | Before and after sports season; mTBI patients had venipuncture within 72 h of injury | FA reduced in the right midbrain in concussed athletes compared to controls. Of 13/29 mTBI patients with blood samples, Tau was inversely related to midbrain FA (r = −0.60, p = 0.033). |
| Tomita et al., 2019 | Prospective Observational | 40 TBI | T2 FLAIR; DWI | TBI patients with acute symptoms < 6 h and patients with MRI evidence of DAI on T2WI/DWI regardless of symptoms. | Serum tau in DAI vs. non-DAI groups; sensitivity and specificity of Tau for DAI | Within 6 h of injury | All patients had high intensity areas on MRI within corpus callosum, brainstem and cerebrum with T2WI/DWI. Tau was higher in DAI (25.3 pg/mL; 0–99.1) vs. non-DAI (0.0 pg/mL; 0–44.4). At cutoff 1.5 pg/mL, sensitivity 74.1% and specificity 69.2% for DAI. |
| NF-L | |||||||
| Author and Year | Study Type | N | MRI Acquisition Parameters | Description | Outcome Measures | Timing of Serum Sampling | Results |
| Ljungqvist et al., 2017 | Prospective Cohort | Nine TBI | 1.5 T; T1/T2; DTI | Serum NF-L levels in severe TBI patients were correlated with MRI and health outcomes. | Serum NF-L; MRI; GOSE | Within 24 h | All patients had DAI on MRI. NF-L ranged from 87.5–851.6 pg/mL. Severely disabled patients (GOSE 3–4) had higher serum NF-L (411 ± 263) than moderate (GOSE 5–6; 277 ± 80; p > 0.05) |
| Al Nimer et al., 2015 | Prospective Cohort | 182 TBI | echo-planar diffusion; FLAIR; GRE; T1/T2 | Serum and CSF-NF-L levels were assessed in relation to imaging and outcomes. | Serum NF-L; CT; MRI; GCS; mortality | Sampled twice daily | In total, 159/182 patients survived, outcome data were available for 73% (116/159), GCS scores over time were significantly correlated with serum NF-L (p = 0.006) and weakly to CSF-NF-L (p > 0.05). Midline shift on MRI correlated with NF-L serum levels (p = 0.012). |
| Sandsmark et al., 2019 | Prospective Cohort | 30 controls, 56 TBI | 1.5 T; T1/T2; SWI; DTI; FLAIR; GRE | Presence of traumatic hemorrhage or traumatic vascular injury correlated with serum NF-H. | Serum NF-H; MRI; GOS-E | Within 48 h of injury | Plasma NF-H was increased in both the traumatic hemorrhage and traumatic vascular injury groups compared to the MRI-negative group ≤ 48 h from injury and continued to stay increased in traumatic vascular injury cohort even 48 h after injury. |
| Alpha-Synuclein | |||||||
| Author and Year | Study Type | N | Age and Sex | Description | Outcome Measures | Timing of Serum Sampling | Results |
| Ye et al., 2019 | Prospective cohort | 52 | FLAIR; SWI; 3D-T1 | Comparison of serum a-synuclein levels and brain connectivity in mTBI patients. | Serum a-synuclein; fMRI; PCS | On admission | All patients were CT-negative. Low levels of a-synuclein were associated with more severe PCS symptoms (p = 0.013) and depression (p = 0.022). Patients with decreased connectivity on fMRI had higher a-synuclein levels (p < 0.05). |
| AMPAR | |||||||
| Author and Year | Study Type | N | MRI Acquisition Parameters | Description | Outcome Measures | Timing of Serum Sampling | Results |
| Dambinova et al., 2013 | Prospective cohort | 33 Concussion | 1.5 T magnet; T1/T2 FLAIR | AMPAR peptide was measured in healthy controls and athletes with concussion to study its feasibility as a biomarker for TBI. | Serum AMPAR; MRI | On admission and again within 6 months of injury | AMPAR levels in controls were 0.05–0.40 ng/mL and 1.0–8.5 ng/mL in concussed athletes. AMPAR as a biomarker had a sensitivity of 91% and specificity 92% with 0.4 ng/mL cuff-off. Athletes having experienced multiple concussions had increased AMPAR levels (2.0–12.0 ng/mL) which was associated with MRI findings, though minor. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yue, J.K.; Upadhyayula, P.S.; Avalos, L.N.; Deng, H.; Wang, K.K.W. The Role of Blood Biomarkers for Magnetic Resonance Imaging Diagnosis of Traumatic Brain Injury. Medicina 2020, 56, 87. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56020087
Yue JK, Upadhyayula PS, Avalos LN, Deng H, Wang KKW. The Role of Blood Biomarkers for Magnetic Resonance Imaging Diagnosis of Traumatic Brain Injury. Medicina. 2020; 56(2):87. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56020087
Chicago/Turabian StyleYue, John K., Pavan S. Upadhyayula, Lauro N. Avalos, Hansen Deng, and Kevin K. W. Wang. 2020. "The Role of Blood Biomarkers for Magnetic Resonance Imaging Diagnosis of Traumatic Brain Injury" Medicina 56, no. 2: 87. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56020087