The Relationship between Selected Bioelements and Depressiveness Associated with Testosterone Deficiency Syndrome in Aging Men

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Material and Methods
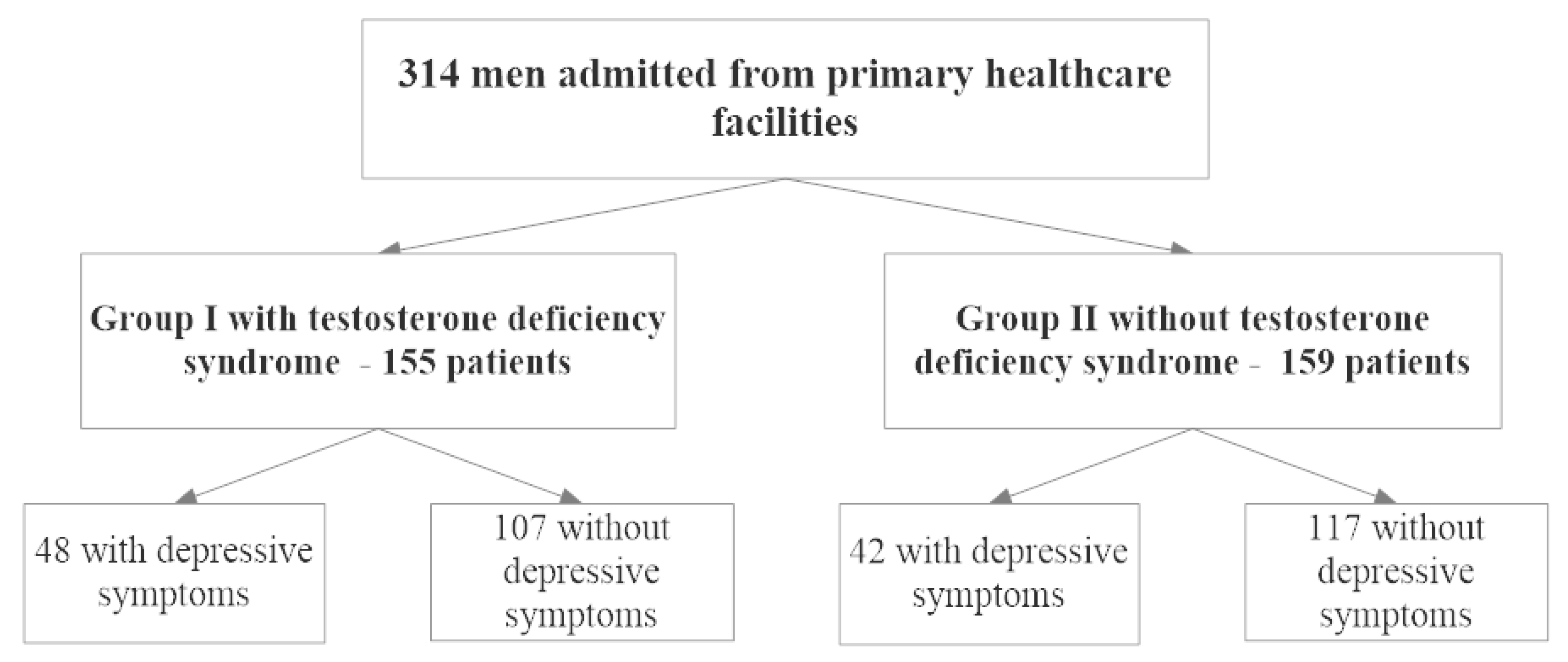
2.1. Characteristics of the Study Group
2.2. Ethical Considerations
2.3. Study Questionnaires
2.4. Bioelement Analysis by Spectrophotometry
2.5. Hormone Level Determination and Diagnosis of Testosterone Deficiency Syndrome
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Blazer, D.; Burchett, B.; Service, C.; George, L.K. The association of age and depression among the elderly: An epidemiological exploration. J. Gerontol. 1991, 46, 210–215. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Greer, T.L. Cognitive dysfunction in unipolar depression: Implications for treatment. J. Affect. Disord. 2014, 152, 19–27. [Google Scholar] [CrossRef]
- Jarema, M.; Dudek, D.; Czernikiewicz, A. Dysfunkcje poznawcze w depresji—Niedoszacowany objaw czy nowy wymiar? Psychiatr. Pol. 2014, 48, 1105–1116. [Google Scholar] [CrossRef]
- Dobrzyńska, E.; Rymaszewska, J.; Kiejna, A. Depresje u osób w wieku podeszłym. Depressions in the elderly. Psychogeriatria Pol. 2007, 4, 51–60. [Google Scholar]
- Ucak, S.; Basat, O.; Karatemiz, G. Functional and nutritional state in elderly men with compensated hypogonadism. J. Am. Med. Dir. Assoc. 2013, 14, 433–436. [Google Scholar] [CrossRef]
- Saad, F.; Röhrig, G.; von Haehling, S.; Traish, A. Testosterone Deficiency and Testosterone Treatment in Older Men. Gerontology 2017, 63, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, M.; Faber, S.; Nieschlag, E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J. Clin. Endocrinol. Metab. 2006, 91, 4335–4343. [Google Scholar] [CrossRef] [PubMed]
- Roumequere, T. Rationale for androgens and erectile dysfunction in 2006. Eur. Urol. 2006, 50, 898–900. [Google Scholar] [CrossRef] [PubMed]
- Gold, S.; Voskuhl, R. Estrogen and Testosterone Therapies in Multiple Sclerosis. Prog. Brain Res. 2009, 175, 239–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogata, T.; Nakamura, Y.; Tsuji, K.; Shibata, T.; Kataoka, K. Steroid hormones protect spinal cord neurons from glutamate toxicity. Neuroscience 1993, 55, 445–449. [Google Scholar] [CrossRef]
- Manev, H.; Favaron, M.; Guidotti, A.; Costa, E. Delayed increase of Ca2+ influx elicited by glutamate: Role in neuronal death. Mol. Pharmacol. 1989, 36, 106–112. [Google Scholar]
- Khera, M. Patients with testosterone deficit syndrome and depression. Arch. Esp. Urol. 2013, 66, 729–736. [Google Scholar] [PubMed]
- Li, Z.; Wang, W.; Xin, X.; Song, X.; Zhang, D. Association of total zinc, iron, copper and selenium intakes with depression in the US adults. J. Affect. Disord. 2018, 228, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Maserejian, N.N.; Hall, S.A.; McKinlay, J.B. Low dietary or supplemental zinc is associated with depression symptoms among women, but not men, in a population-based epidemiological survey. J. Affect. Disord. 2012, 136, 781–788. [Google Scholar] [CrossRef] [Green Version]
- Miki, T.; Kochi, T.; Eguchi, M.; Kuwahara, K.; Tsuruoka, H.; Kurotani, K.; Ito, R.; Akter, S.; Kashino, I.; Pham, N.M.; et al. Dietary intake of minerals in relation to depressive symptoms in Japanese employees: The Furukawa Nutrition and Health Study. Nutrition 2015, 31, 686–690. [Google Scholar] [CrossRef]
- Nguyen, T.; Miyagi, S.; Tsujiguchi, H.; Kambayashi, Y.; Hara, A.; Nakamura, H.; Suzuki, K.; Yamada, Y.; Shimizu, Y.; Nakamura, H. Association between lower intake of minerals and depressive symptoms among elderly japanese women but not men: Findings from shika study. Nutrients 2019, 11, 389. [Google Scholar] [CrossRef] [Green Version]
- Serefko, A.; Szopa, A.; Poleszak, E. Magnesium and depression. Magnes. Res. 2016, 29, 112–119. [Google Scholar] [CrossRef]
- Mlyniec, K.; Davies, C.L.; de Aguero Sanchez, I.G.; Pytka, K.; Budziszewska, B.; Nowak, G. Essential elements in depression and anxiety. Part I. Pharmacol. Rep. 2014, 66, 534–544. [Google Scholar] [CrossRef]
- Mlyniec, K.; Gaweł, M.; Doboszewska, U.; Starowicz, G.; Pytka, K.; Davies, C.L.; Budziszewska, B.; Jarosz, M. Essential elements in depression and anxiety. Part II. Pharmacol. Rep. 2015, 67, 187–194. [Google Scholar] [CrossRef]
- Neala, A.; Guilarte, T. Mechanisms of lead and manganese neurotoxicity. Toxicol. Res. 2013, 2, 99–114. [Google Scholar] [CrossRef]
- Bouabid, S.; Tinakoua, A.; Lakhdar-Ghazal, N.; Benazzouz, A. Manganese neurotoxicity: Behavioral disorders associated with dysfunctions in the basal ganglia and neurochemical transmission. J. Neurochem. 2016, 136, 677–691. [Google Scholar] [CrossRef] [PubMed]
- Rotter, I.; Kosik-Bogacka, D.; Dołęgowska, B.; Safranow, K.; Lubkowska, A.; Laszczyńska, M. Analysis of the relationship between the blood concentration of several metals, macro- and micronutrients and endocrine disorders associated with male aging. Environ. Geochem. Health 2016, 38, 749–761. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, O.; Freundlich, R.E.; Dakik, H.K.; Grober, E.D.; Najari, B.; I Lipshultz, L.; Khera, M. The quantitative ADAM questionnaire: A new tool in quantifying the severity of hypogonadism. Int. J. Impot. Res. 2010, 22, 20–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, P.; Werner, J.; Heerlein, A.; Kraus, A.; Sauer, H. On the validity of the Beck Depression Inventory. A review. Psychopathology 1998, 31, 160–168. [Google Scholar] [CrossRef]
- Kula, K.; Słowikowska–Hilczer, J. Hipogonadyzm późny u mężczyzn. Endokrynol. Pol. 2012, 63, 15–19. [Google Scholar]
- Dukhande, V.; Malthankar-Phatak, G.; Hugus, J.; Daniels, C.; Lai, J. Manganese-induced neurotoxicity is differentially enhanced by glutathione depletion in astrocytoma and neuroblastoma cells. Neurochem. Res. 2006, 31, 1349–1357. [Google Scholar] [CrossRef]
- Lee, E.-S.Y.; Sidoryk, M.; Jiang, H.; Yin, Z.; Aschner, M. Estrogen and tamoxifen reverse manganese-induced glutamate transporter impairment in astrocytes. J. Neurochem. 2009, 110, 530–544. [Google Scholar] [CrossRef] [Green Version]
- Erikson, K.M.; Suber, R.L.; Aschner, M. Glutamate/Aspartate Transporter (GLAST), Taurine Transporter and Metallothionein mRNA Levels are Differentially Altered in Astrocytes Exposed to Manganese Chloride, Manganese Phosphate or Manganese Sulfate. Neurotoxicology 2002, 23, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Sidoryk-Wegrzynowicz, M.; Aschner, M. Manganese toxicity in the central nervous system: The glutamine/glutamate-γ-aminobutyric acid cycle. J. Intern. Med. 2013, 273, 466–477. [Google Scholar] [CrossRef] [Green Version]
- Sidoryk-Węgrzynowicz, M.; Lee, E.; Albrecht, J.; Aschner, M. Manganese disrupts astrocyte glutamine transporter expression and function. J. Neurochem. 2009, 110, 822–830. [Google Scholar] [CrossRef]
- Santos, V.; Bisen-Hersh, E.; Yu, Y.; Cabral, I.S.R.; Nardini, V.; Culbreth, M.; Da Rocha, J.; Barbosa, F.; Aschner, M. Anthocyanin-rich acai (Euterpe oleracea Mart.) extract attenuates manganese-induced oxidative stress in rat primary astrocyte cultures. J. Toxicol. Environ. Health 2014, 77, 390–404. [Google Scholar] [CrossRef] [PubMed]
- Karki, P.; Smith, K.; Johnson, J., Jr.; Aschner, M.; Lee, E. Role of transcription factor yin yang 1 in manganese-induced reduction of astrocytic glutamate transporters: Putative mechanism for manganese-induced neurotoxicity. Neurochem. Int. 2015, 88, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fordahl, S.C.; Erikson, K.M. Manganese accumulation in membrane fractions of primary astrocytes is associated with decreased γ-aminobutyric acid (GABA) uptake, and is exacerbated by oleic acid and palmitate. Environ. Toxicol. Pharmacol. 2014, 37, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Oulhote, Y.; Mergler, D.; Barbeau, B.; Bellinger, D.; Bouffard, T. Neurobehavioral Function in School-Age Children Exposed to Manganese in Drinking Water. Environ. Health Perspect. 2014, 122, 1343–1350. [Google Scholar] [CrossRef]
- Kotfis, K.; Szylińska, A.; Listewnik, M.; Strzelbicka, M.; Brykczyński, M.; Rotter, I.; Żukowski, M. Early delirium after cardiac surgery: An analysis of incidence and risk factors in elderly (≥65 years) and very elderly (≥80 years) patients. Clin. Interv. Aging 2018, 13, 1061–1070. [Google Scholar] [CrossRef] [Green Version]
- Kotfis, K.; Marra, A.; Ely, E.W. ICU delirium—A diagnostic and therapeutic challenge in the intensive care unit. Anaesthesiol. Intensive Ther. 2018, 50, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Rajizadeh, A.; Mozaffari-Khosravi, H.; Yassini-Ardakani, M.; Dehghani, A. Effect of magnesium supplementation on depression status in depressed patients with magnesium deficiency: A randomized, double-blind, placebo-controlled trial. Nutrition 2017, 35, 56–60. [Google Scholar] [CrossRef]
- Rotter, I.; Kosik-Bogacka, D.; Dołęgowska, B.; Safranow, K.; Karakiewicz, B.; Laszczyńska, M. Relationship between serum magnesium concentration and metabolic and hormonal disorders in middle-aged and older men. Magnes Res. 2015, 28, 99–107. [Google Scholar] [CrossRef]
- Ni, M.; You, Y.; Chen, J.; Zhang, L. Copper in depressive disorder: A systematic review and meta-analysis of observational studies. Psychiatry Res. 2018, 267, 506–515. [Google Scholar] [CrossRef]
- Chang, C.; Choi, J.; Kim, H.; Park, S. Correlation between serum testosterone level and concentrations of copper and zinc in hair tissue. Biol. Trace Elem. Res. 2011, 144, 264–271. [Google Scholar] [CrossRef]
- Bajpai, A.; Verma, A.K.; Srivastava, M.; Srivastava, R. Oxidative stress and major depression. J. Clin. Diagn. Res. 2014, 8, CC04–CC07. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhong, S.; Liao, X.; Chen, J.; He, T.; Lai, S.; Jia, Y. A meta-analysis of oxidative stress markers in depression. PLoS ONE 2015, 10, e0138904. [Google Scholar] [CrossRef] [PubMed]
- Doboszewska, U.; Wlaź, P.; Nowak, G.; Radziwoń-Zaleska, M.; Cui, R.; Mlyniec, K. Zinc in the Monoaminergic Theory of Depression: Its Relationship to Neural Plasticity. Neural Plast. 2017, 2017, 3682752. [Google Scholar] [CrossRef] [PubMed]
- Doboszewska, U.; Szewczyk, B.; Sowa-Kucma, M.; Noworyta-Sokołowska, K.; Misztak, P.; Gołębiowska, J.; Mlyniec, K.; Ostachowicz, B.; Krosniak, M.; Wojtanowska-Krosniak, A.; et al. Alterations of Bio-elements, Oxidative, and Inflammatory Status in the Zinc Deficiency Model in Rats. Neurotox. Res. 2016, 29, 143–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olechnowicz, J.; Tinkov, A.; Skalny, A.; Suliburska, J. Zinc status is associated with inflammation, oxidative stress, lipid, and glucose metabolism. J. Physiol. Sci. 2018, 68, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Spark, R.F. Testosterone, diabetes mellitus, and the metabolic syndrome. Curr. Urol. Rep. 2007, 8, 467–471. [Google Scholar] [CrossRef]
- Kelishadi, R.; Hashemipour, M.; Adeli, K.; Tavakoli, N.; Movahedian-Attar, A.; Shapouri, J.; Poursafa, P.; Rouzbahani, A. Effect of zinc supplementation on markers of insulin resistance, oxidative stress, and inflammation among prepubescent children with metabolic syndrome. Metab. Syndr. Relat. Disord. 2010, 8, 505–510. [Google Scholar] [CrossRef]
- Cohen, P.G. Obesity in men: The hypogonadal-estrogen receptor relationship and its effect on glucose homeostasis. Med. Hypotheses 2008, 70, 358–360. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Data | ||
| Age (years), (mean ± SD; Me) | 61.36 ± 6.37; 62 | |
| BMI (kg/m2), (mean ± SD; Me) | 28.27 ± 4.37; 27.73 | |
| BMI classification | norm | 63 (20.06%) |
| overweight | 164 (52.23%) | |
| first degree obesity | 65 (20.70%) | |
| second degree obesity | 15 (4.78% | |
| third degree obesity | 7 (2.23%) | |
| Hips (cm), (mean ± SD; Me) | 103.26 ± 7.71; 103 | |
| Waist (cm), (mean ± SD; Me) | 102.07 ± 12.04; 100 | |
| WHR classification | norm | 208 (66.24%) |
| abdominal obesity | 106 (33.76%) | |
| Education (n, %) | primary | 17 (5.42%) |
| vocational | 54 (17.20% | |
| secondary | 128 (40.76%) | |
| higher | 115 (36.62%) | |
| Smoking (n, %) | non-smoker | 263 (83.76%) |
| smoker | 51 (16.24%) | |
| Occupational activity (n, %) | employed | 19 (6.05%) |
| pensioner (due to health condition) | 137 (43.63%) | |
| pensioner (due to age) | 37 (11.78%) | |
| unemployed | 121 (38.54%) | |
| Marital status (n, %) | married | 48 (15.29%) |
| unmarried | 266 (84.71%) | |
| Statin treatment (n, %) | 50 (15.92%) | |
| Diabetes (n, %) | 54 (17.20%) | |
| Hypertension (n, %) | 172 (54.78%) | |
| Depressive symptoms (n, %) | 90 (28.66%) | |
| Total testosterone deficiency (n, %) | 155 (49.36%) | |
| Serum Bioelements | ||
| Mn (mg/L), (mean ± SD; Me) | 0.002 ± 0.001; 0.002 | |
| Zn (mg/L) (mean ± SD; Me) | 0.889 ± 0.131; 0.880 | |
| Cu (mg/L) (mean ± SD; Me) | 1.083 ± 0.179; 1.065 | |
| Cr (mg/L) (mean ± SD; Me) | 0.0005 ± 0.0002; 0.0004 | |
| Mg (mg/L) (mean ± SD; Me) | 0.002 ± 0.001; 0.002 | |
| Serum Bioelements | Group I—TDS (n = 155) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| No Depressive Symptoms (n = 107) | Depressive Symptoms (n = 48) | ||||||
| Mean | Median | ±SD | Mean | Median | ±SD | ||
| Mn (mg/L) *10−3 | 1.822 | 1.630 | 1.203 | 2.181 | 1.970 | 1.055 | 0.005 |
| Zn (mg/L) | 0.895 | 0.885 | 0.144 | 0.873 | 0.869 | 0.119 | 0.649 |
| Cu (mg/L) | 1.078 | 1.050 | 0.175 | 1.116 | 1.098 | 0.204 | 0.186 |
| Cr (mg/L) *10−3 | 0.459 | 0.398 | 0.267 | 0.504 | 0.481 | 0.191 | 0.022 |
| Mg (mg/L) | 20.697 | 20.550 | 2.323 | 20.389 | 20.550 | 2.407 | 0.782 |
| Serum Bioelements | Group II—No TDS (n = 159) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| No Depressive Symptoms (n = 117) | Depressive Symptoms (n = 42) | ||||||
| Mean | Median | ±SD | Mean | Median | ±SD | ||
| Mn (mg/L) *10−3 | 1.723 | 1.580 | 1.010 | 1.866 | 1.515 | 1.327 | 0.874 |
| Zn (mg/L) | 0.893 | 0.880 | 0.128 | 0.878 | 0.904 | 0.119 | 0.980 |
| Cu (mg/L) | 1.082 | 1.070 | 0.161 | 1.058 | 1.055 | 0.213 | 0.629 |
| Cr (mg/L) *10−3 | 0.466 | 0.446 | 0.178 | 0.439 | 0.399 | 0.197 | 0.240 |
| Mg (mg/L) | 21.338 | 21.280 | 1.801 | 20.876 | 20.985 | 2.680 | 0.095 |
| Serum Bioelements | Group I—TDS (n = 155) | Group II—No TDS (n = 159) | ||
|---|---|---|---|---|
| Depressive Symptoms (n = 48) | Depressive Symptoms (n = 42) | |||
| R | p-Value | R | p-Value | |
| Mn (mg/L) | 0.225 | 0.005 | −0.013 | 0.873 |
| Zn (mg/L) | −0.037 | 0.649 | −0.002 | 0.978 |
| Cu (mg/L) | 0.107 | 0.187 | −0.039 | 0.630 |
| Cr (mg/L) | 0.185 | 0.022 | −0.094 | 0.240 |
| Mg (mg/L) | −0.022 | 0.782 | −0.133 | 0.095 |
| Odds Ratio | 95% CI | p-Value | |
|---|---|---|---|
| Mn (mg/L) | 1.394 | 1.008–1.928 | 0.045 |
| Zn (mg/L) | 0.999 | 0.996–1.002 | 0.473 |
| Cu (mg/L) | 1.001 | 0.999–1.004 | 0.206 |
| Cr (mg/L) | 3.531 | 0.791–15.766 | 0.098 |
| Mg (mg/L) | 1.000 | 1.000–1.000 | 0.452 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rotter, I.; Wiatrak, A.; Rył, A.; Kotfis, K.; Ciosek, Ż.; Laszczyńska, M.; Sipak-Szmigiel, O.; Szylińska, A. The Relationship between Selected Bioelements and Depressiveness Associated with Testosterone Deficiency Syndrome in Aging Men. Medicina 2020, 56, 125. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030125
Rotter I, Wiatrak A, Rył A, Kotfis K, Ciosek Ż, Laszczyńska M, Sipak-Szmigiel O, Szylińska A. The Relationship between Selected Bioelements and Depressiveness Associated with Testosterone Deficiency Syndrome in Aging Men. Medicina. 2020; 56(3):125. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030125
Chicago/Turabian StyleRotter, Iwona, Adrian Wiatrak, Aleksandra Rył, Katarzyna Kotfis, Żaneta Ciosek, Maria Laszczyńska, Olimpia Sipak-Szmigiel, and Aleksandra Szylińska. 2020. "The Relationship between Selected Bioelements and Depressiveness Associated with Testosterone Deficiency Syndrome in Aging Men" Medicina 56, no. 3: 125. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030125