Maxillary Implant-Supported Overdentures: Mechanical Behavior Comparing Individual Axial and Bar Retention Systems. A Cohort Study of Edentulous Patients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pujol Rodríguez, R.; Abellán García, A.; Pérez Díaz, J.; Ayala García, A. Un Perfil de Las Personas Mayores En España, 2018. Indicadores Estadísticos Básicos 2018, 13, 34. [Google Scholar]
- 2019 World Population Data Sheet—Population Reference Bureau. Available online: https://www.prb.org/worldpopdata/ (accessed on 16 November 2019).
- Isla Pera, P. El Envejecimiento de La Población. Rev. Enferm. 2003, 26, 15–20. [Google Scholar] [PubMed]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Tooth Loss and Oral Health-Related Quality of Life: A Systematic Review and Meta-Analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Driscoll, C.F.; Freilich, M.A.; Guckes, A.D.; Knoernschild, K.L.; Mcgarry, T.J. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [Google Scholar]
- Fernandez-Estevan, L.; Selva-Otaolaurruchi, E.J.; Montero, J.; Sola-Ruiz, F. Oral Health-Related Quality of Life of Implant-Supported Overdentures versus Conventional Complete Prostheses: Retrospective Study of a Cohort of Edentulous Patients. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e450–e458. [Google Scholar] [CrossRef]
- Doundoulakis, J.H.; Eckert, S.E.; Lindquist, C.C.; Jeffcoat, M.K. The Implant-Supported Overdenture as an Alternative to the Complete Mandibular Denture. J. Am. Dent. Assoc. 2003, 134, 1455–1458. [Google Scholar] [CrossRef]
- Kutkut, A.; Bertoli, E.; Frazer, R.; Pinto-sinai, G.; Fuentealba, R.; Studts, J. A Systematic Review of Studies Comparing Conventional Complete Denture and Implant Retained Overdenture. J. Prosthodont. Res. 2018, 62, 1–9. [Google Scholar] [CrossRef]
- Boven, G.C.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A. Improving Masticatory Performance, Bite Force, Nutritional State and Patient’s Satisfaction with Implant Overdentures: A Systematic Review of the Literature. J. Oral Rehabil. 2015, 42, 220–233. [Google Scholar] [CrossRef]
- von der Gracht, I.; Derks, A.; Haselhuhn, K.; Wolfart, S. EMG Correlations of Edentulous Patients with Implant Overdentures and Fixed Dental Prostheses Compared to Conventional Complete Dentures and Dentates: A Systematic Review and Meta-Analysis. Clin. Oral Implants Res. 2017, 28, 765–773. [Google Scholar] [CrossRef]
- Sivaramakrishnan, G.; Sridharan, K. Comparison of Implant Supported Mandibular Overdentures and Conventional Dentures on Quality of Life: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. Aust. Dent. J. 2016, 61, 482–488. [Google Scholar] [CrossRef]
- Rohlin, M.; Nilner, K.; Davidson, T.; Norlund, A.; Tranæus, S.; Gynther, G.; Nordenram, G.; Hultin, M.; Jemt, T.; Lekholm, U.; et al. Treatment of Adult Patients with Edentulous Arches: A Systematic Review. Int. J. Prosthodont. 2012, 25, 553–567. [Google Scholar] [PubMed]
- Srinivasan, M.; Meyer, S.; Mombelli, A.; Müller, F. Dental Implants in the Elderly Population: A Systematic Review and Meta-Analysis. Clin. Oral Implants Res. 2017, 28, 920–930. [Google Scholar] [CrossRef]
- Koller, B.; Att, W.; Strub, J.-R. Survival Rates of Teeth, Implants, and Double Crown-Retained Removable Dental Prostheses: A Systematic Literature Review. Int. J. Prosthodont. 2012, 24, 109–117. [Google Scholar]
- Slot, W.; Raghoebar, G.M.; Vissink, A.; Huddleston Slater, J.J.; Meijer, H.J.A. A Systematic Review of Implant-Supported Maxillary Overdentures after a Mean Observation Period of at Least 1 Year: Review Article. J. Clin. Periodontol. 2010, 37, 98–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feine, J.S.; Carlsson, G.E.; Awad, M.A.; Chehade, A.; Duncan, W.J.; Gizani, S.; Head, T.; Lund, J.P.; MacEntee, M.; Mericske-Stern, R.; et al. The McGill Consensus Statement on Overdentures. Int. J. Oral Maxillofac. Implants 2002, 17, 601–602. [Google Scholar] [PubMed]
- Thomason, J.M.; Feine, J.; Exley, C.; Moynihan, P.; Müller, F.; Naert, I.; Ellis, J.S.; Barclay, C.; Butterworth, C.; Scott, B.; et al. Mandibular Two Implant-Supported Overdentures as the First Choice Standard of Care for Edentulous Patients—The York Consensus Statement. Br. Dent. J. 2009, 207, 185–186. [Google Scholar] [CrossRef]
- Cehreli, M.C.; Karasoy, D.; Kokat, A.M.; Akca, K.; Eckert, S.E. Systematic Review of Prosthetic Maintenance Requirements for Implant-Supported Overdentures. Int. J. Oral Maxillofac. Implants 2010, 25, 163–180. [Google Scholar] [PubMed]
- Stoumpis, C.; Kohal, R.-J. To Splint or Not to Splint Oral Implants in the Implant-Supported Overdenture Therapy? A Systematic Literature Review. J. Oral Rehabil. 2011, 38, 857–869. [Google Scholar] [CrossRef]
- Andreiotelli, M. Prosthodontic Complications with Implant Overdentures. Int. J. Prosthodont. 2010, 23, 195–203. [Google Scholar]
- Osman, R.B.; Payne, A.G.T.; Ma, S. Prosthodontic Maintenance of Maxillary Implant Overdentures: A Systematic Literature Review. Int. J. Prosthodont. 2012, 25, 381–391. [Google Scholar]
- Leão, R.S.; Moraes, S.L.D.; Vasconcelos, B.C.E.; Lemos, C.A.A.; Pellizzer, E.P. Splinted and Unsplinted Overdenture Attachment Systems: A Systematic Review and Meta-Analysis. J. Oral Rehabil. 2018, 45, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Anas El-Wegoud, M.; Fayyad, A.; Kaddah, A.; Nabhan, A. Bar versus Ball Attachments for Implant-Supported Overdentures in Complete Edentulism: A Systematic Review. Clin. Implant Dent. Relat. Res. 2018, 20, 243–250. [Google Scholar] [CrossRef]
- Udhayaraja, P.; Ariga, P.; Jain, A.R. Retention and Stability of Overdentures with Ball, Bar, or Magnet Attachments: A Systematic Review. Drug Invent. Today 2018, 10, 723–727. [Google Scholar]
- Simon, H.; Roy, T.Y. Terminology for implant prostheses. Int. J. Oral. Maxillofac. Implants 2003, 18, 539–543. [Google Scholar] [CrossRef]
- Mericske-Stern, R. Treatment Outcomes with Implant-Supported Overdentures: Clinical Considerations. J. Prosthet. Dent. 1998, 79, 66–73. [Google Scholar] [CrossRef]
- Zou, D.; Wu, Y.; Huang, W.; Wang, F.; Wang, S.; Zhang, Z.; Zhang, Z. A 3-Year Prospective Clinical Study of Telescopic Crown, Bar, and Locator Attachments for Removable Four Implant–Supported Maxillary Overdentures. Int. J. Prosthodont. 2013, 26, 566–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balaguer, J.; Ata-Ali, J.; Peñarrocha-Oltra, D.; García, B.; Peñarrocha-Diago, M. Long-Term Survival Rates of Implants Supporting Overdentures. J. Oral Implantol. 2015, 41, 173–177. [Google Scholar] [CrossRef]
- Wang, F.; Monje, A.; Huang, W.; Zhang, Z.; Wang, G.; Wu, Y. Maxillary Four Implant-Retained Overdentures via Locator® Attachment: Intermediate-Term Results from a Retrospective Study. Clin. Implant Dent. Relat. Res. 2016, 18, 571–579. [Google Scholar] [CrossRef]
- Kern, J.S.; Kern, T.; Wolfart, S.; Heussen, N. A Systematic Review and Meta-Analysis of Removable and Fixed Implant-Supported Prostheses in Edentulous Jaws: Post-Loading Implant Loss. Clin. Oral Implants Res. 2016, 27, 174–195. [Google Scholar] [CrossRef]
- ELsyad, M.; Denewar, B.; Elsaih, E. Clinical and Radiographic Evaluation of Bar, Telescopic, and Locator Attachments for Implant-Stabilized Overdentures in Patients with Mandibular Atrophied Ridges: A Randomized Controlled Clinical Trial. Int. J. Oral Maxillofac. Implants 2018, 33, 1103–1111. [Google Scholar] [CrossRef]
- Slot, W.; Raghoebar, G.M.; Cune, M.S.; Vissink, A.; Meijer, H.J.A. Four or Six Implants in the Maxillary Posterior Region to Support an Overdenture: 5-Year Results from a Randomized Controlled Trial. Clin. Oral Implants Res. 2019, 30, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercruyssen, M.; Quirynen, M. Long-Term, Retrospective Evaluation (Implant and Patient-Centred Outcome) of the Two-Implant-Supported Overdenture in the Mandible. Part 2: Marginal Bone Loss. Clin. Oral Implants Res. 2010, 21, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Raghoebar, G.M.; Meijer, H.J.A.; Slot, W.; Slater, J.J.R.; Vissink, A. A Systematic Review of Implant-Supported Overdentures in the Edentulous Maxilla, Compared to the Mandible: How Many Implants? Eur. J. Oral Implantol. 2014, 7, S191–S201. [Google Scholar] [PubMed]
- Keller, E.E.; Tolman, D.E.; Eckert, S. Surgical-Prosthodontic Reconstruction of Advanced Maxillary Bone Compromise with Autogenous Onlay Block Bone Grafts and Osseointegrated Endosseous Implants: A 12-Year Study of 32 Consecutive Patients. Int. J. Oral Maxillofac. Implants 1999, 14, 197–209. [Google Scholar] [PubMed]
- Ferrigno, N.; Laureti, M.; Fanali, S.; Grippaudo, G. A Long-Term Follow-up Study of Non-Submerged ITI Implants in the Treatment of Totally Edentulous Jaws. Part 1: Ten-Year Life Table Analysis of a Prospective Multicenter Study with 1286 Implants. Clin. Oral Implants Res. 2002, 12, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Smedberg, J.I.; Nilner, K.; Frykholm, A. A Six-Year Follow-up Study of Maxillary Overdentures on Osseointegrated Implants. Eur. J. Prosthodont. Restor. Dent. 1999, 7, 51–56. [Google Scholar] [PubMed]
- Visser, A.; Raghoebar, G.M.; Meijer, H.J.A. Implant-Retained Maxillary Overdentures on Milled Bar Suprastructures: A 10-Year Follow-up of Surgical and Prosthetic Care and Aftercare. J. Prosthet. Dent. 2009, 102, 384. [Google Scholar]
- Fortin, Y.; Sullivan, R.M.; Rangert, B.R. The Marius Implant Bridge: Surgical and Prosthetic Rehabilitation for the Completely Edentulous Upper Jaw with Moderate to Severe Resorption: A 5-Year Retrospective Clinical Study. Clin. Implant Dent. Relat. Res. 2002, 4, 69–77. [Google Scholar] [CrossRef]
- Widbom, C.; Söderfeldt, B.; Kronström, M. A Retrospective Evaluation of Treatments with Implant-Supported Maxillary Overdentures. Clin. Implant Dent. Relat. Res. 2005, 7, 166–172. [Google Scholar] [CrossRef]
- Jemt, T.; Chai, J.; Harnett, J.; Heath, M.R.; Hutton, J.E.; Johns, R.B.; McKenna, S.; McNamara, D.C.; van Steenberghe, D.; Taylor, R.; et al. A 5-Year Prospective Multicenter Follow-up Report on Overdentures Supported by Osseointegrated Implants. Int. J. Oral Maxillofac. Implants 1996, 11, 291–298. [Google Scholar]
- Marinis, A.; Afshari, F.S.; Yuan, J.C.C.; Lee, D.J.; Syros, G.; Knoernschild, K.L.; Campbell, S.D.; Sukotjo, C. Retrospective Analysis of Implant Overdenture Treatment in the Advanced Prosthodontic Clinic at the University of Illinois at Chicago. J. Oral Implantol. 2016, 42, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, M.; Zhao, K.; Wang, F.; Huang, W.; Zhang, X.; Wu, Y. Stud vs Bar Attachments for Maxillary Four-Implant–Supported Overdentures: 3- to 9-Year Results from a Retrospective Study. Int. J. Oral Maxillofac. Implants 2019, 34, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Guédat, C.; Nagy, U.; Schimmel, M.; Müller, F.; Srinivasan, M. Clinical Performance of LOCATOR® Attachments: A Retrospective Study with 1–8 Years of Follow-Up. Clin. Exp. Dent. Res. 2018, 4, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Ekfeldt, A.; Johansson, L.A.; Isaksson, S. Implant-Supported Overdenture Therapy: A Retrospective Study. Int. J. Prosthodont. 1997, 10, 366–374. [Google Scholar] [PubMed]
- Cakarer, S.; Can, T.; Yaltirik, M.; Keskin, C. Complications Associated with the Ball, Bar and Locator Attachments for Implant-Supported Overdentures. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e953–e959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boven, G.C.; Slot, J.W.A.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A. Maxillary Implant-Supported Overdentures Opposed by (Partial) Natural Dentitions: A 5-Year Prospective Case Series Study. J. Oral Rehabil. 2017, 44, 988–995. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prostheses | Implant Survival (%) | Prosthesis Survival (%) | Mechanical Complications | ||||||
|---|---|---|---|---|---|---|---|---|---|
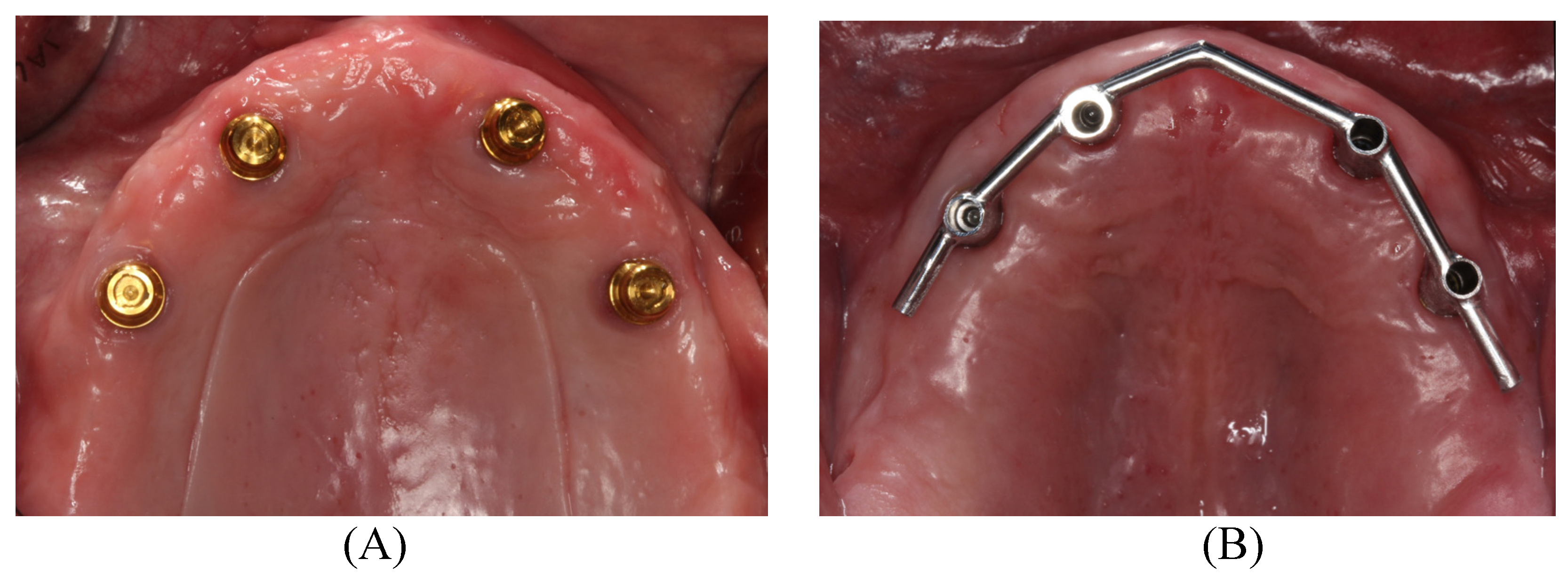
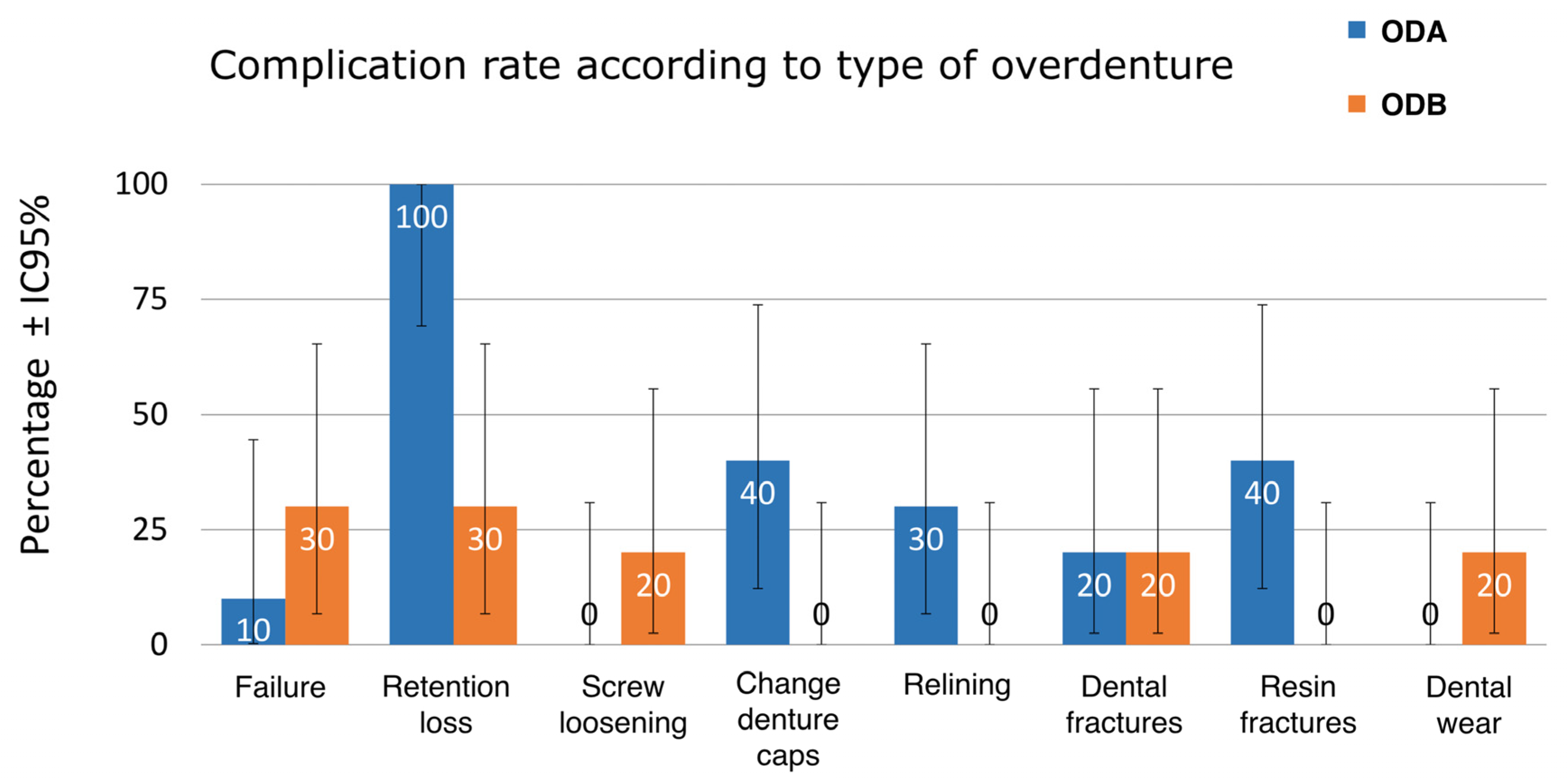
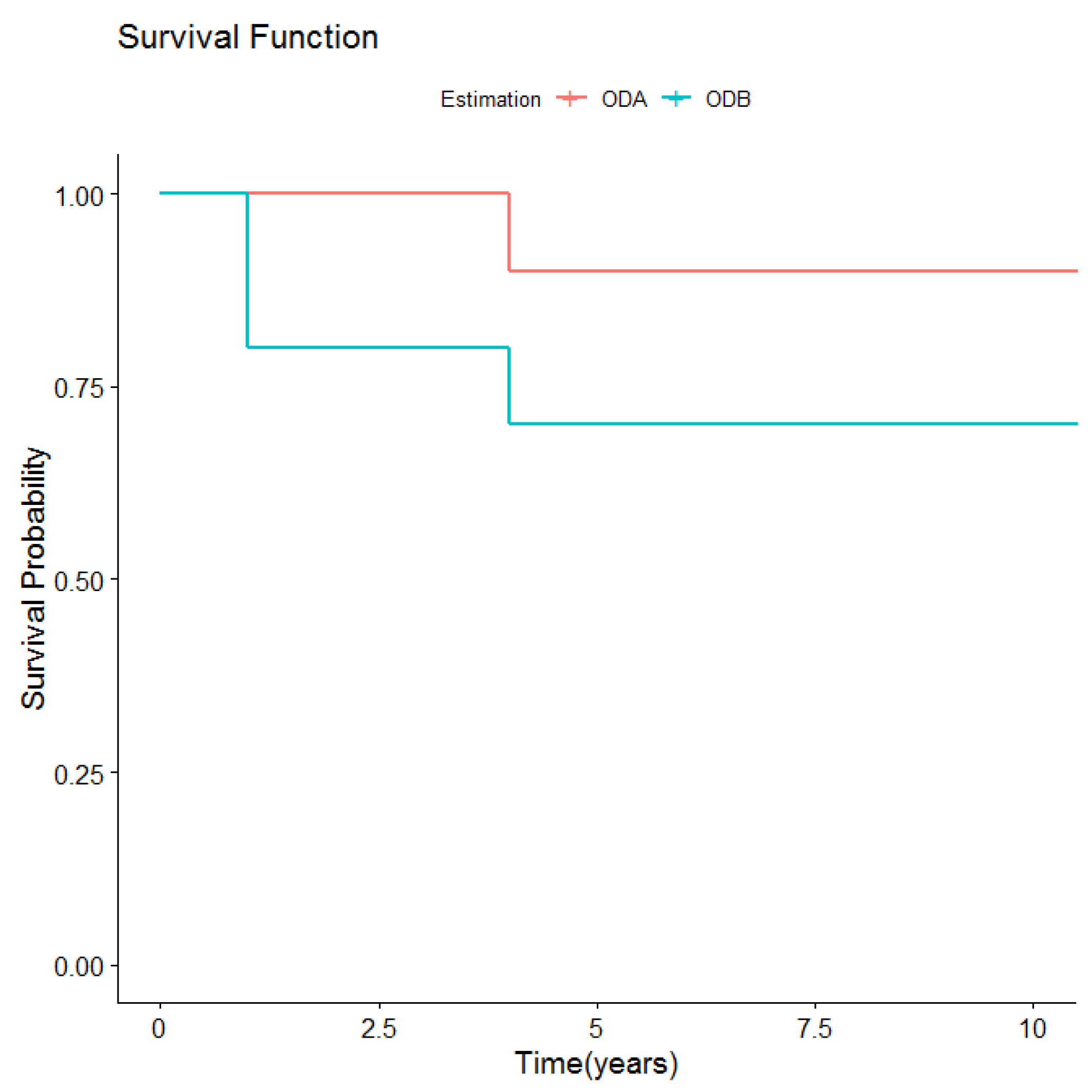
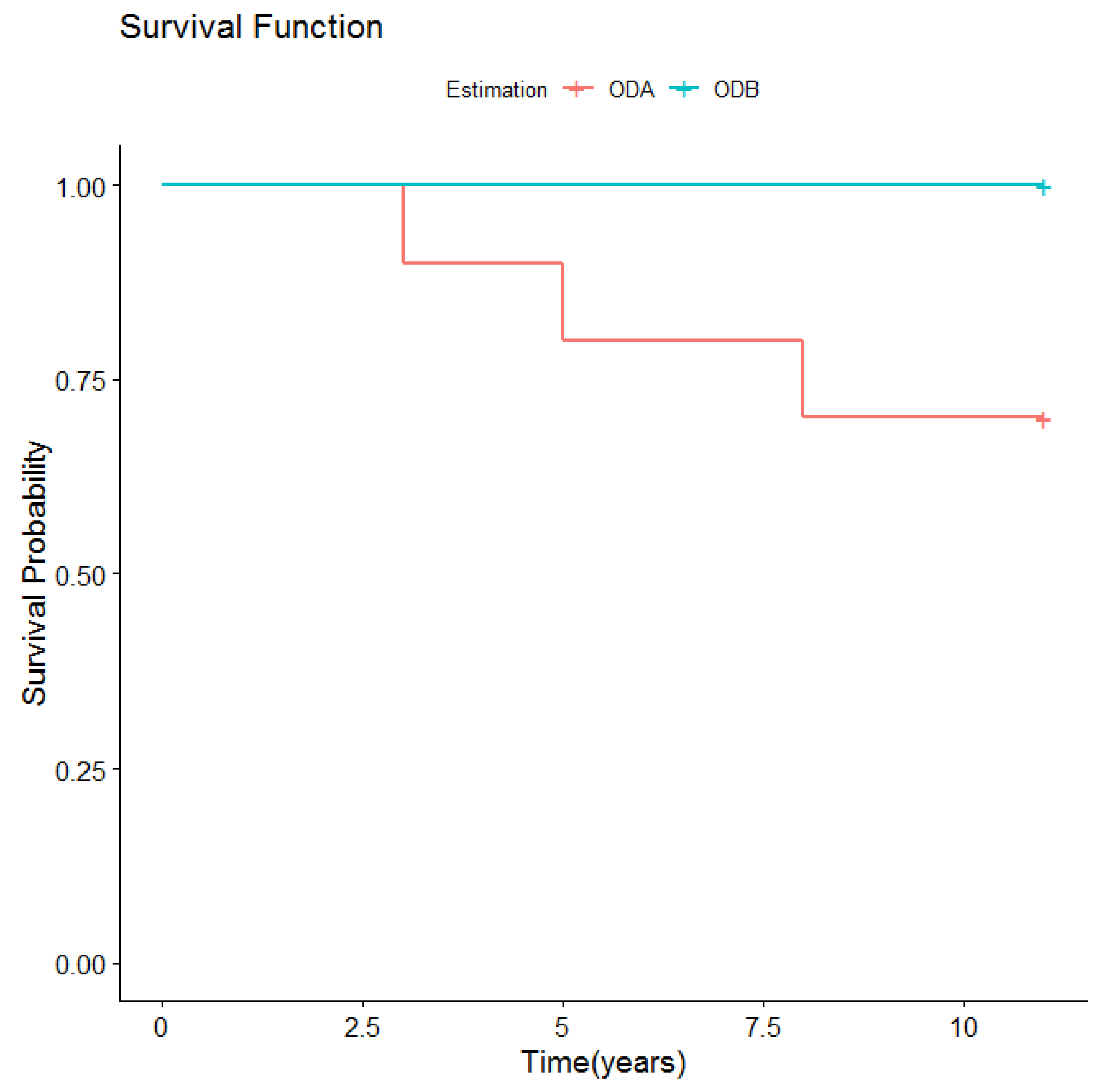
| ODA Prostheses N = 10 Number of implants supporting each prosthesis: 4 Total number of implants N=40 | Of 40 implants, 11 failed: 5 in the first year, four in the 4th year, and 2 in the 11th year. | 90%: of 10 prostheses, 1 failed after 4 years. | 100% Retention loss (changing inserts every 3 years) Change of abutment: 5 due to wear (after 6, 10 and 11 years) 2 due to fracture (after 5 and 8 years) | 40% Change of inserts: 6 changes (one after 3 years, three after 7 years, two after 8 years) | 30% Relining: 3 patients (after 2,3, 5 and 8 years) | 20% Dental fracture: 3 fractures (1 patient with 2 fractures after 5 and 8 years, the other after 8 years) | 40% Resin fracture: 4 fractures (after 6 months, 3, 6 and 8 years) | ||
| ODB Prostheses N = 10; Number of implants supporting each prosthesis: 4; Total number of implants N = 40 | Of 40 implants, 8 failed: 7 in the first year, and 1 during the 4th year. | 70%: of 10 prostheses, 2 failed within the first year and one after 4 years. | 30% Retention loss of rider clips: 3 times in 3 (after 6, 9 and 10 years) | 20% Screw loosening or fracture: 4 in 2 patients (after 3 and 4 years) | 20% Dental fractures: 2 fractures in two patients (after 3 and 4 years) | 20% Dental wear: 2 patients (teeth were changed in one patient after 7 years, and another after 8 years) | |||
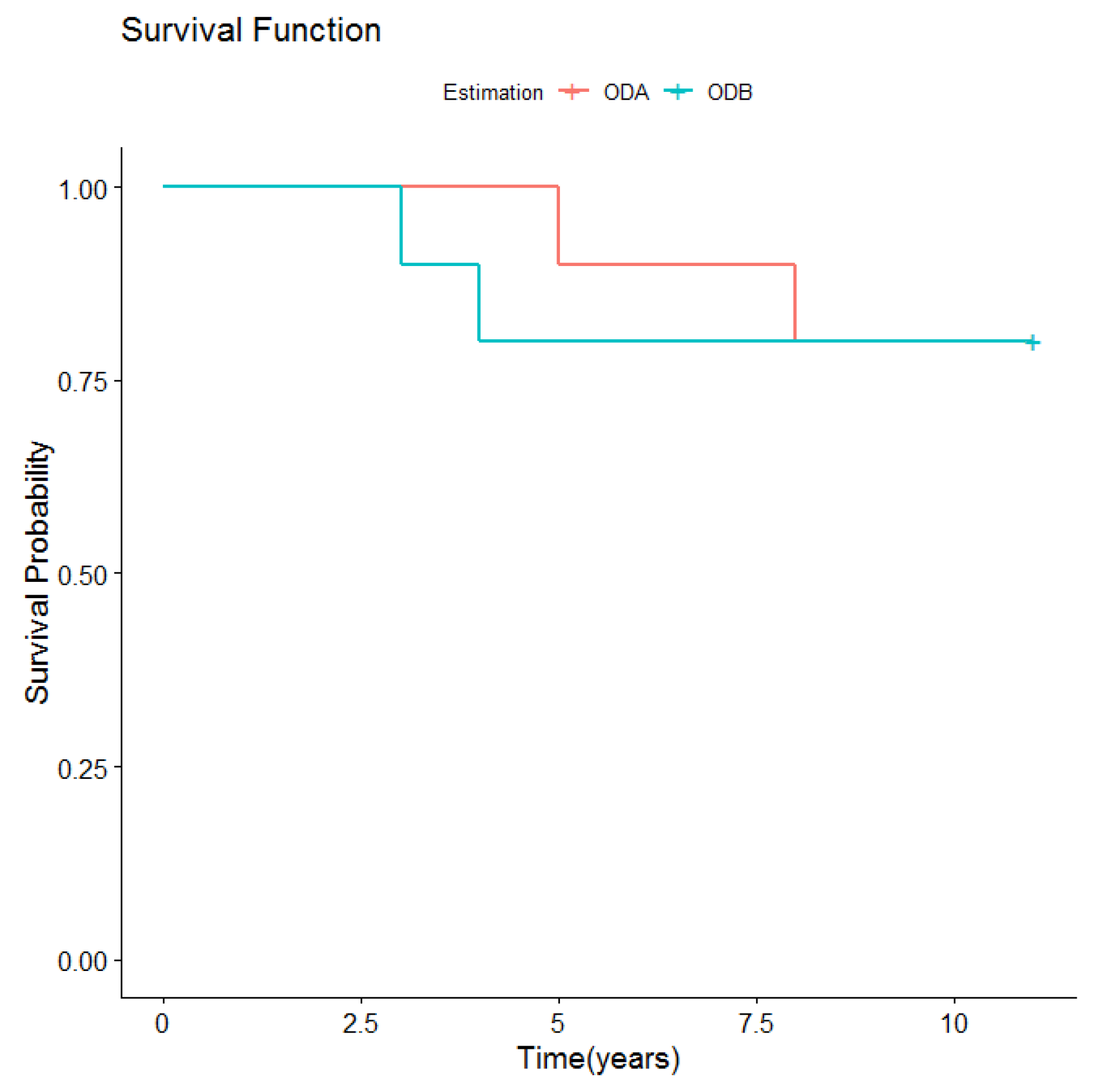
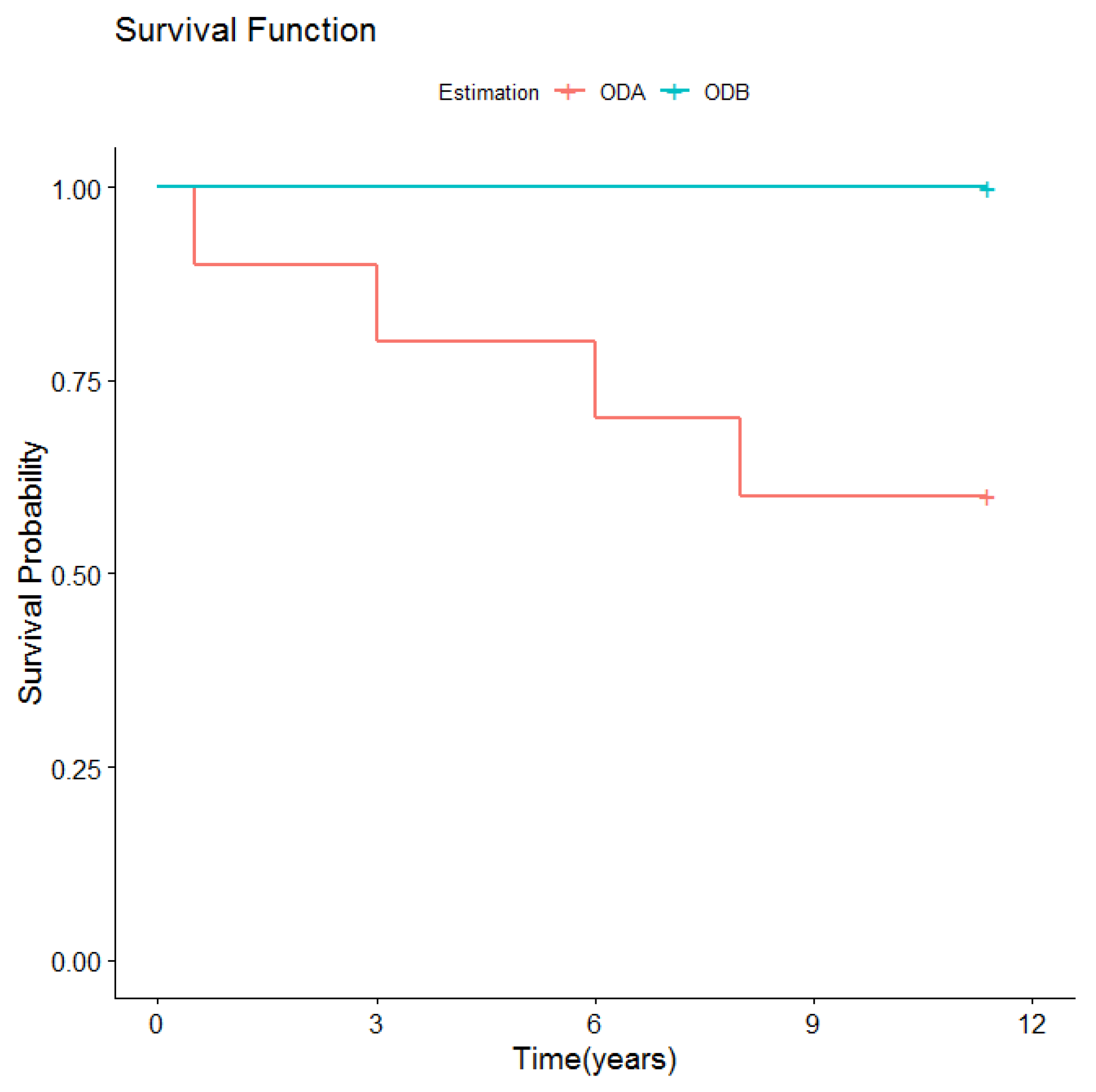
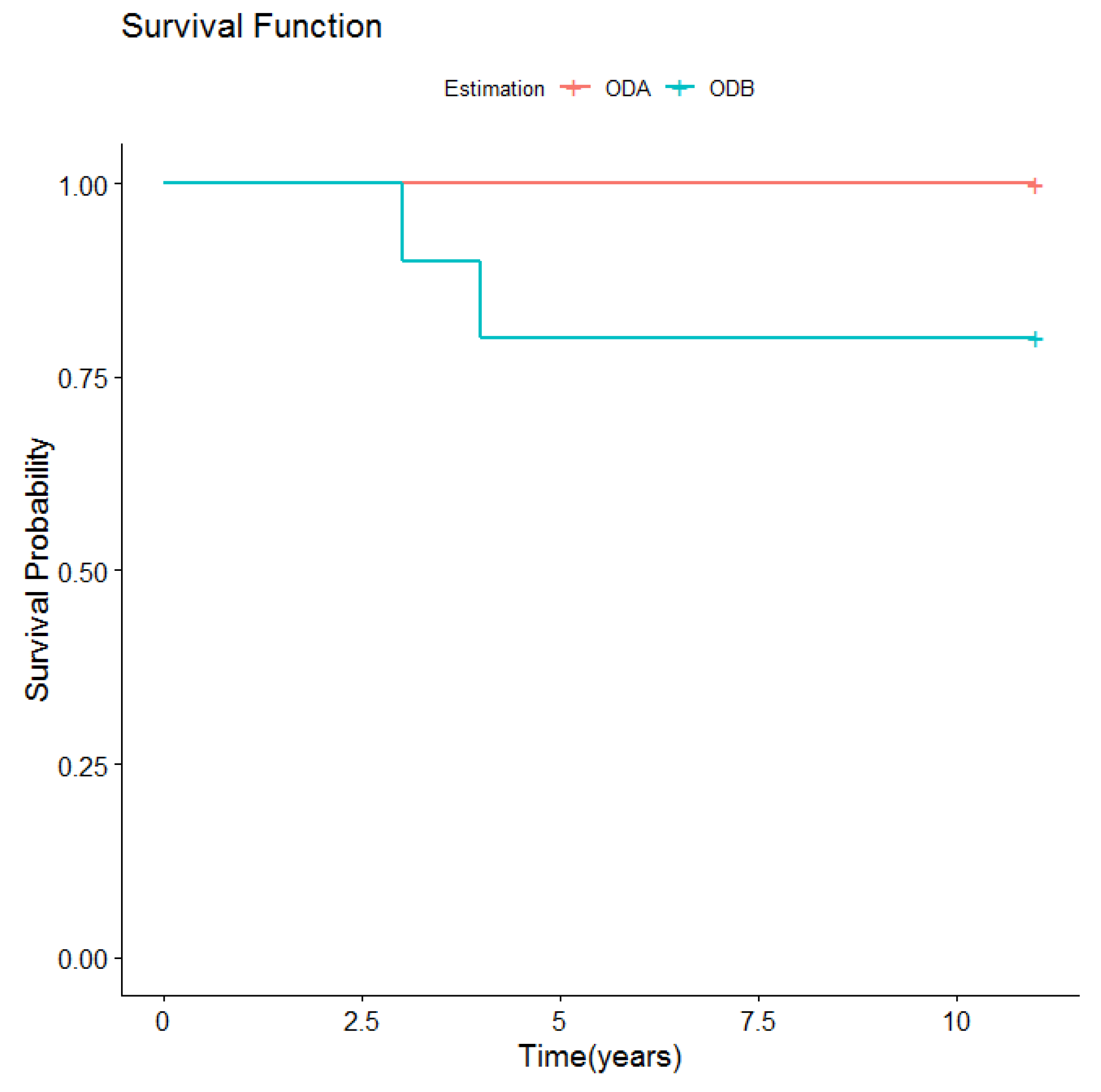
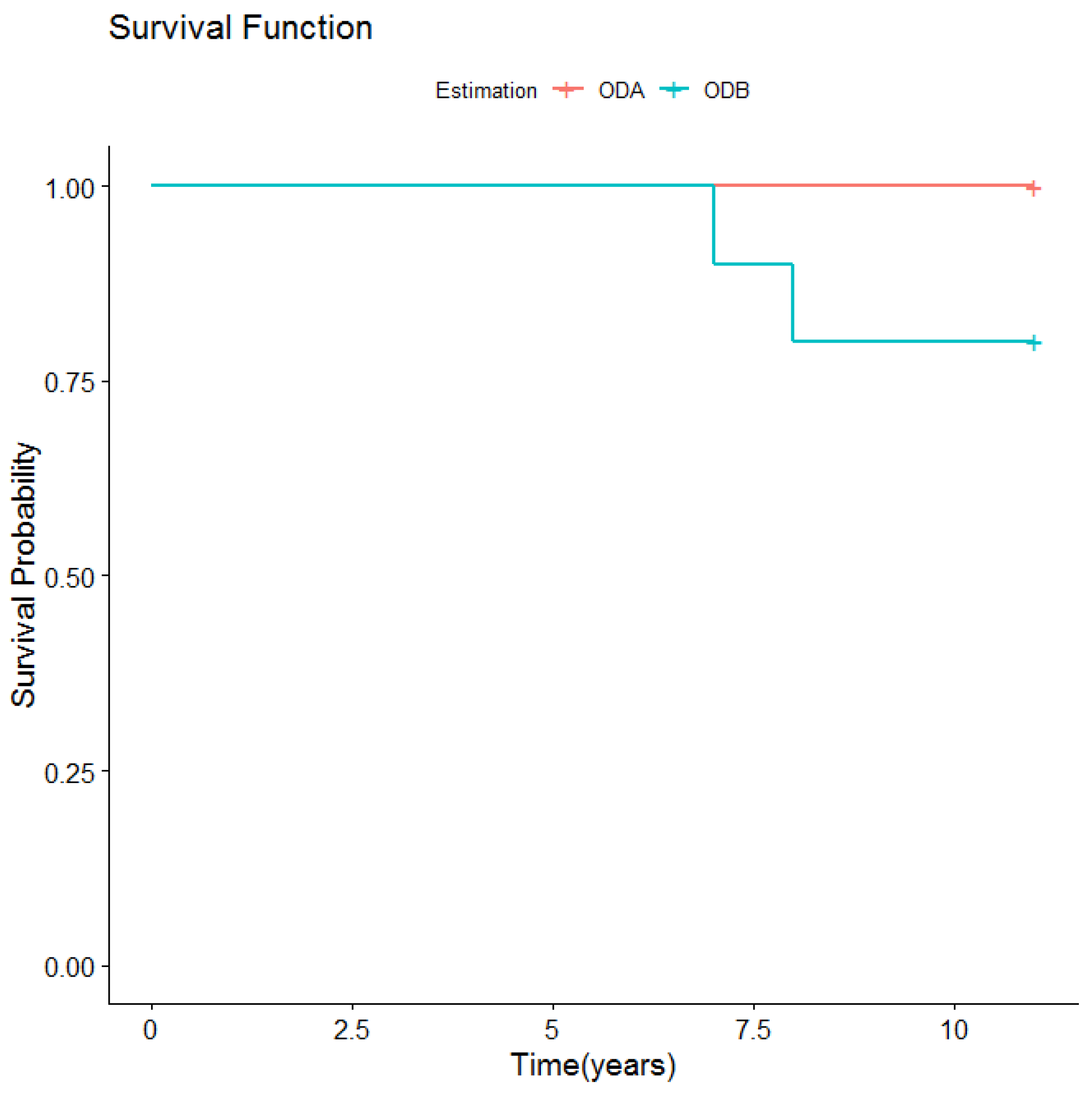
| Survival according to mechanical behavior | p-Value |
| Retention type | 0.251 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mañes Ferrer, J.F.; Fernández-Estevan, L.; Selva-Otaolaurruchi, E.; Labaig-Rueda, C.; Solá-Ruíz, M.F.; Agustín-Panadero, R. Maxillary Implant-Supported Overdentures: Mechanical Behavior Comparing Individual Axial and Bar Retention Systems. A Cohort Study of Edentulous Patients. Medicina 2020, 56, 139. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030139
Mañes Ferrer JF, Fernández-Estevan L, Selva-Otaolaurruchi E, Labaig-Rueda C, Solá-Ruíz MF, Agustín-Panadero R. Maxillary Implant-Supported Overdentures: Mechanical Behavior Comparing Individual Axial and Bar Retention Systems. A Cohort Study of Edentulous Patients. Medicina. 2020; 56(3):139. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030139
Chicago/Turabian StyleMañes Ferrer, José Félix, Lucía Fernández-Estevan, Eduardo Selva-Otaolaurruchi, Carlos Labaig-Rueda, María Fernanda Solá-Ruíz, and Rubén Agustín-Panadero. 2020. "Maxillary Implant-Supported Overdentures: Mechanical Behavior Comparing Individual Axial and Bar Retention Systems. A Cohort Study of Edentulous Patients" Medicina 56, no. 3: 139. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030139