Determination of Referential Rates for Optical Coherence Tomography and Optical Coherence Tomography Angiography Flow Deficits in the Macular Choriocapillaris in Ophthalmologically Healthy Children


Abstract
:1. Introduction
2. Materials and Methods
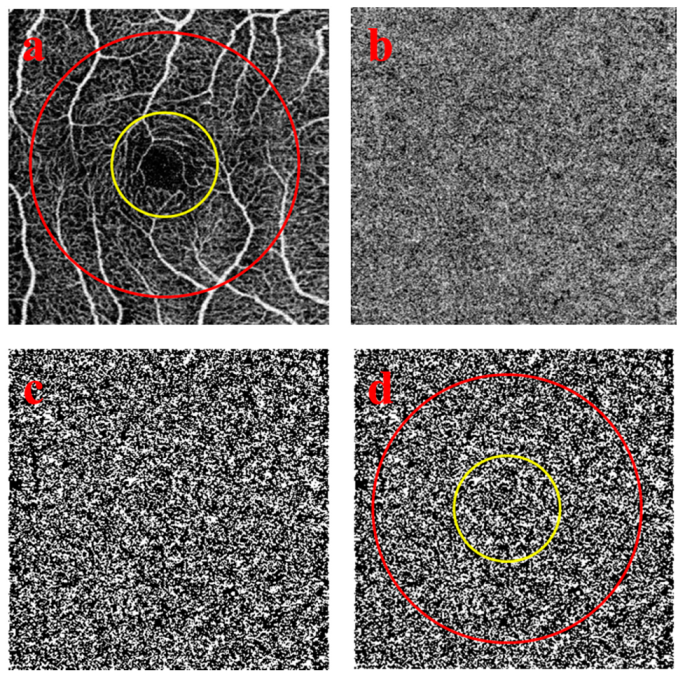
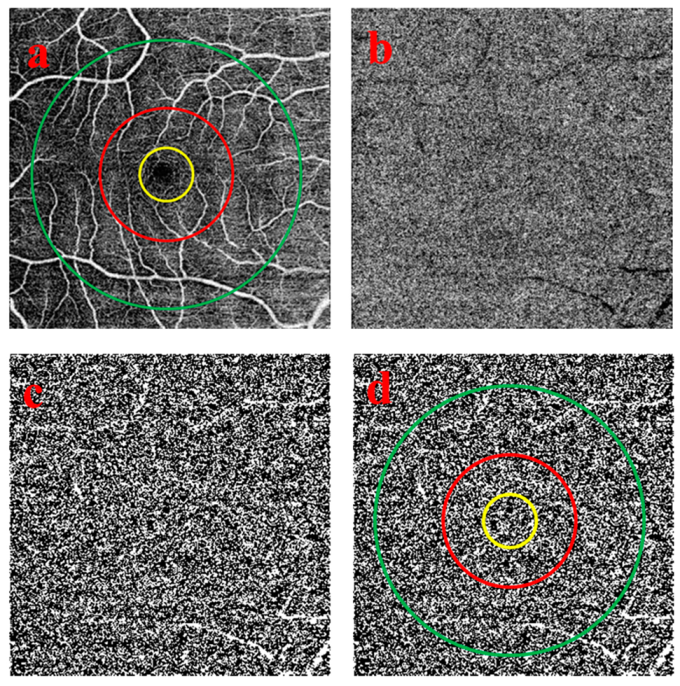
2.1. Quantitative Image Analysis of the Choriocapillaris OCTA Images
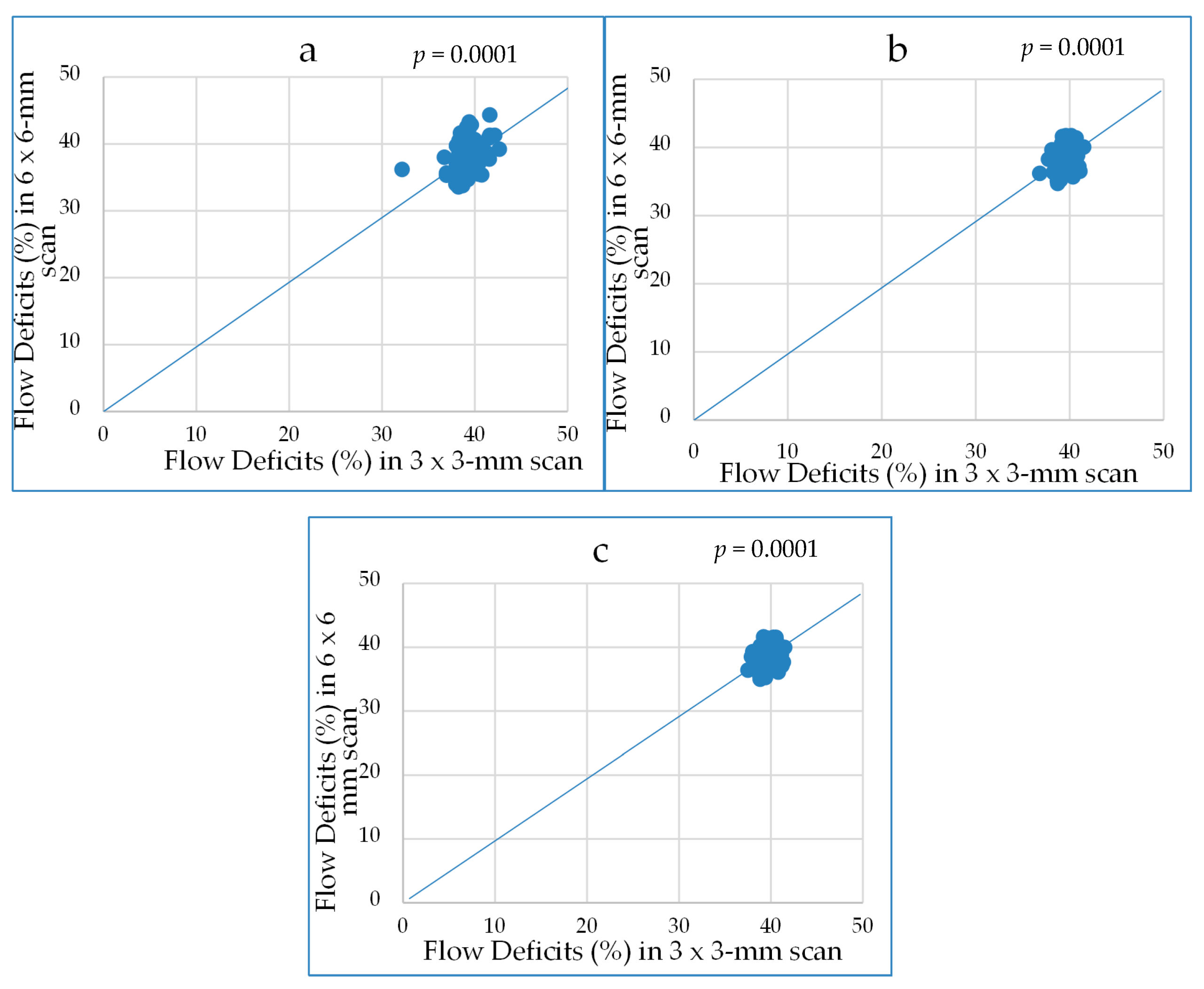
2.2. Statistical Analysis
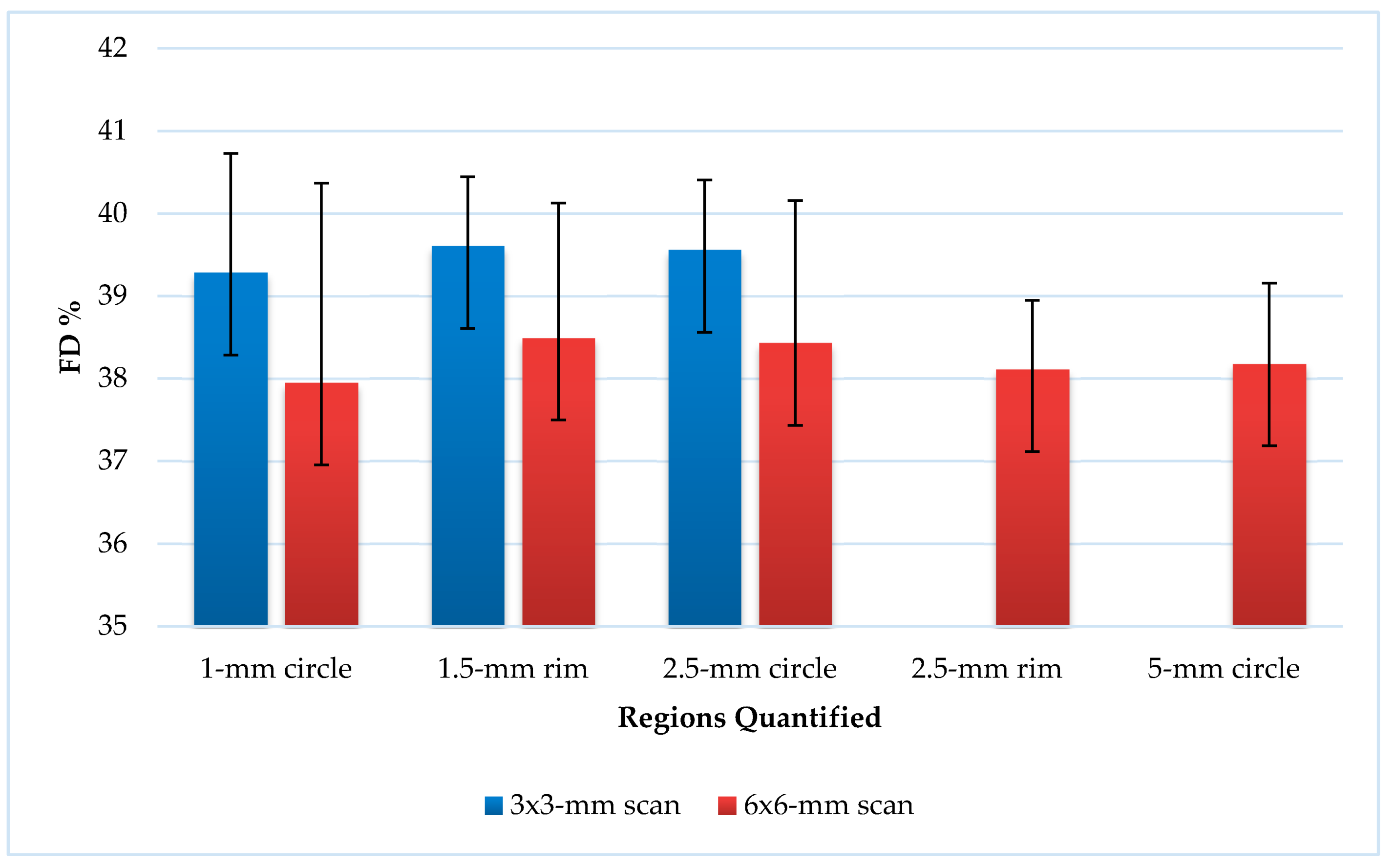
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Maccora, K.A.; Sheth, S.; Ruddle, J.B. Optical coherence tomography in paediatric clinical practice. Clin. Exp. Optom. 2019, 102, 300–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, J.; Jin, J.; Lv, M.; Jiang, W.; Sun, S.; Yao, C.; Zhu, J.; Zou, H.; Wang, L.; He, X.; et al. Distribution of scleral thickness and associated factors in 810 Chinese children and adolescents: A swept-source optical coherence tomography study. Acta Ophthalmol. 2019, 97, e410–e418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, P.H.; Weaver, M.; Lyon, D.; Choi, E.; Fillingim, R.B. Thinner retinal nerve fiber layer in very preterm versus term infants and relationship to brain anatomy and neurodevelopment. Physiol. Behav. 2015, 176, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Braaf, B. Angiography and Polarimetry of the Posterior Eye with Functional Optical Coherence Tomography; VU University: Amsterdam, The Netherlands, 2015; pp. 13–34. [Google Scholar]
- Hashmani, N.; Hashmani, S.; Murad, A.; Baig, N. Macular vascular density at the superficial capillary plexus using the optical coherence tomography angiography. Clin. Ophthalmol. 2019, 13, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Camino, A.; Guo, Y.; You, Q.; Wang, J.; Huang, D.; Bailey, S.T.; Jia, Y. Detecting and measuring areas of choriocapillaris low perfusion in intermediate, non-neovascular age-related macular degeneration. Neurophotonics 2019. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Neto, C.A.; Moult, E.M.; Fujimoto, J.G.; Waheed, N.K.; Ferrara, D. Choriocapillaris loss in advanced age-related macular degeneration. J. Ophthalmol. 2018. [Google Scholar] [CrossRef]
- Britze, J.; Frederiksen, J.L. Optical coherence tomography in multiple sclerosis. Eye 2018, 32, 884–888. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Martin, E.; Garcia-Campayo, J.; Puebla-Guedea, M.; Ascaso, F.J.; Roca, M.; Gutierrez-Ruiz, F.; Vilades, E.; Polo, V.; Larrosa, J.M.; Pablo, L.E.; et al. Fibromyalgia is correlated with retinal nerve fiber layer thinning. PLoS ONE 2016. [Google Scholar] [CrossRef]
- Huang, Y.; Zhou, L.; ZhangBao, J.; Cai, T.; Wang, B.; Li, X.; Wang, L.; Lu, C.; Zhao, C.; Lu, J.; et al. Peripapillary and parafoveal vascular network assessment by optical coherence tomography angiography in aquaporin-4 antibody-positive neuromyelitis optica spectrum disorders. Br. J. Ophthalmol. 2018. [Google Scholar] [CrossRef]
- Wang, C.Y.; Zheng, Y.F.; Liu, B.; Meng, Z.W.; Hong, F.; Wang, X.X.; Wang, X.J.; Du, L.; Wang, I.Y.; Zhu, D.; et al. Retinal Nerve Fiber Layer Thickness in Children: The Gobi Desert Children Eye Study. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5285–5291. [Google Scholar] [CrossRef]
- Shin, J.W.; Shin, Y.U.; Uhm, K.B.; Sung, K.R.; Kang, M.H.; Cho, H.Y.; Seong, M. The effect of optic disc center displacement on retinal nerve fiber layer measurement determined by spectral domain optical coherence tomography. PLoS ONE 2016, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Tatham, A.J.; Zangwill, L.M.; Weinreb, R.N.; Zhang, C.; Medeiros, F.A. Diagnostic ability of retinal nerve fiber layer imaging by swept source optical coherence tomography in glaucoma. Am. J. Ophthalmol. 2015, 159, 193–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- North, V.; Gelman, R.; Tsang, S.H. Juvenile-onset macular degeneration and allied disorders. Dev. Ophthalmol. 2014, 53, 44–52. [Google Scholar] [CrossRef] [Green Version]
- He, M.S.; Chang, F.L.; Lin, H.Z.; Wu, J.L.; Hsieh, T.C.; Lee, Y.C. The association between diabetes and age-related macular degeneration among the elderly in Taiwan. Diabetes Care 2018, 41, 2202–2211. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Huang, X.; Meng, X.; Chen, T.; Gu, Y.; Wu, Y.; Wu, Z. In vivo assessment of macula in eyes of healthy children 8 to 16 years old using optical coherence tomography angiography. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uji, A.; Balasubramanian, S.; Lei, J.; Baghdasaryan, E.; Al-Sheikh, M.; Sadda, S.V.R. Choriocapillaris imaging using multiple en face optical coherence tomography angiography image averaging. JAMA Ophthalmol. 2017, 135, 1197–1204. [Google Scholar] [CrossRef]
- Wang, Q.; Chan, S.; Yang, J.Y.; You, B.; Wang, Y.X.; Jonas, J.B.; Wei, W.B. Vascular Density in Retina and Choriocapillaris as Measured by Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2016, 168, 95–109. [Google Scholar] [CrossRef]
- Zhang, Q.; Zheng, F.; Motulsky, E.H.; Gregori, G.; Chu, Z.; Chen, C.L.; Li, C.; de Sisternes, L.; Durbin, M.; Rosenfeld, P.J.; et al. A novel strategy for quantifying choriocapillaris flow voids using swept-source OCT angiography. Investig. Ophthalmol. Vis. Sci. 2018, 59, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Proudlock, F.A.; Gottlob, I. Pediatric optical coherence tomography in clinical practice-recent progress. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT69–OCT79. [Google Scholar] [CrossRef]
- Chu, Z.; Chen, C.L.; Zhang, Q.; Pepple, K.; Durbin, M.; Gregori, G. Complex signal-based optical coherence tomography angiography enables in vivo visualization of choriocapillaris in human choroid. J. Biomed. Opt. 2017. [Google Scholar] [CrossRef]
- Monroy, G.L.; Won, J. Clinical translation of handheld optical coherence tomography: Practical considerations and recent advancements. J. Biomed. Opt. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotruck, J.C.; House, R.J.; Freedman, S.F.; Kelly, M.P.; Enyedi, L.B.; Prakalapakorn, S.G.; Lim, M.E.; El-Dairi, M.A. Optical Coherence Tomography normative peripapillary retinal nerve fiber layer and macular data in children ages 0–5 years. Am. J. Ophthalmol. 2019, 208, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Passani, A.; Sframeli, A.T.; Posarelli, C.; Lisi, D.; Guidi, G.; Casini, G.; Ferreras, A.; Figus, M. Macular spectral-domain optical coherence tomography values and correlations in healthy children. Int. Ophthalmol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bhoiwala, D.L.; Simon, J.W.; Raghu, P.; Krishnamoorthy, M.; Todani, A.; Gandham, S.B.; Simmons, S. Optic nerve morphology in normal children. J. AAPOS 2015, 19, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Gürağaç, F.B.; Totan, Y.; Güler, E.; Tenlik, A.; Ertuğrul, İ.G. Normative spectral domain optical coherence tomography data in healthy turkish children. Semin. Ophthalmol. 2017, 32, 216–222. [Google Scholar] [CrossRef] [PubMed]
- El-Dairi, M.A.; Asrani, S.G.; Enyedi, L.B.; Freedman, S.F. Optical coherence tomography in the eyes of normal children. Arch. Ophthalmol. 2009, 127, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Cubuk, M.; Sahinoglu-Keskek, N.; Keskek, S.O. Retinal nerve fiber layer thickness in a healthy Turkish population measured by optical coherence tomography. Ann. Saudi Med. 2016, 36, 409–413. [Google Scholar] [CrossRef] [Green Version]
- Zheng, F.; Zhang, Q.; Shi, Y.; Russell, J.F.; Motulsky, E.H.; Banta, J.T.; Chu, Z.; Zhou, H.; Patel, N.A.; de Sisternes, L.; et al. Age-dependent changes in the macular choriocapillaris of normal eyes imaged with swept-source optical coherence tomography angiography. Am. J. Ophthalmol. 2019, 200, 110–122. [Google Scholar] [CrossRef]
- Dimitrova, G.; Chihara, E.; Takahashi, H.; Amano, H.; Okazaki, K. Quantitative retinal optical coherence tomography angiography in patients with diabetes without diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 190–196. [Google Scholar] [CrossRef]
- Shi, Y.; Zhang, Q.; Zheng, F.; Russell, J.F.; Motulsky, E.H.; Banta, J.T.; Chu, Z.; Zhou, H.; Patel, N.A.; de Sisternes, L.; et al. Correlations between different choriocapillaris flow deficit parameters in normal eyes using swept source OCT angiography. Am. J. Ophthalmol. 2020, 209, 18–26. [Google Scholar] [CrossRef]
- Siegfried, F.; Rommel, F.; Rothe, M.; Brinkmann, M.P.; Sochurek, J.A.M.; Freitag, J.; Grisanti, S.; Ranjbar, M. Evaluating diurnal changes in choroidal sublayer perfusion using optical coherence tomography angiography. ACTA Ophthalmol. 2019, 97, e1062–e1068. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.S.; Ouyang, Y.; Ruiz, H.; Sadda, S.R. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 261–266. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RNFL | Minimum | Maximum | Mean | Standard Deviation |
|---|---|---|---|---|
| RNFL 1 | 100 | 190 | 147.89 | 21.469 |
| RNFL 2 | 63 | 166 | 89.88 | 16.991 |
| RNFL 3 | 48 | 98 | 63.95 | 8.935 |
| RNFL 4 | 51 | 128 | 76.93 | 14.693 |
| RNFL 5 | 108 | 196 | 149.23 | 19.888 |
| RNFL 6 | 82 | 204 | 146.88 | 24.644 |
| RNFL 7 | 71 | 161 | 108.35 | 19.814 |
| RNFL 8 | 45 | 121 | 80.68 | 15.197 |
| RNFL 9 | 46 | 95 | 63.78 | 10.852 |
| RNFL 10 | 69 | 145 | 100.22 | 17.084 |
| RNFL 11 | 86 | 163 | 123.66 | 18.763 |
| RNFL 12 | 65 | 183 | 121.66 | 24.826 |
| RNFL inferior | 99 | 169 | 134.85 | 15.459 |
| RNFL nasal | 54 | 115 | 81.62 | 11.932 |
| RNFL temporal | 56 | 128 | 76.95 | 11.825 |
| RNFL superior | 96 | 166 | 131.04 | 14.126 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakstytė, V.; Šniurevičiūtė, L.; Šimienė, E.; Skruodytė, J.; Janulevičienė, I. Determination of Referential Rates for Optical Coherence Tomography and Optical Coherence Tomography Angiography Flow Deficits in the Macular Choriocapillaris in Ophthalmologically Healthy Children. Medicina 2020, 56, 238. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56050238
Bakstytė V, Šniurevičiūtė L, Šimienė E, Skruodytė J, Janulevičienė I. Determination of Referential Rates for Optical Coherence Tomography and Optical Coherence Tomography Angiography Flow Deficits in the Macular Choriocapillaris in Ophthalmologically Healthy Children. Medicina. 2020; 56(5):238. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56050238
Chicago/Turabian StyleBakstytė, Viktorija, Liveta Šniurevičiūtė, Evelina Šimienė, Justina Skruodytė, and Ingrida Janulevičienė. 2020. "Determination of Referential Rates for Optical Coherence Tomography and Optical Coherence Tomography Angiography Flow Deficits in the Macular Choriocapillaris in Ophthalmologically Healthy Children" Medicina 56, no. 5: 238. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56050238