Risk Factors and Management of Osteoporosis Post-Transplant

 , ,
, ,
Abstract
:1. Introduction
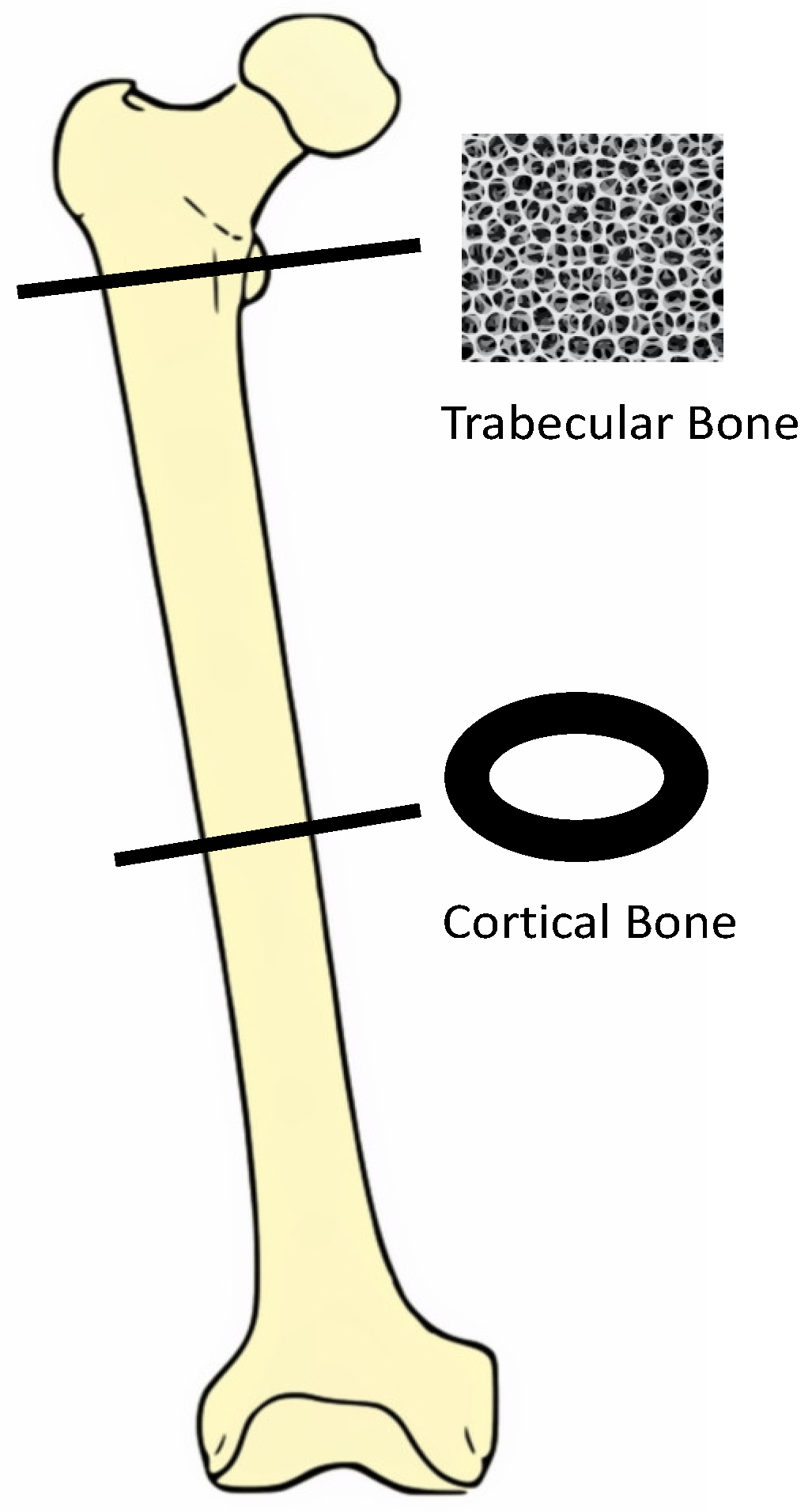
2. Bone Morphology
3. Pathogenesis
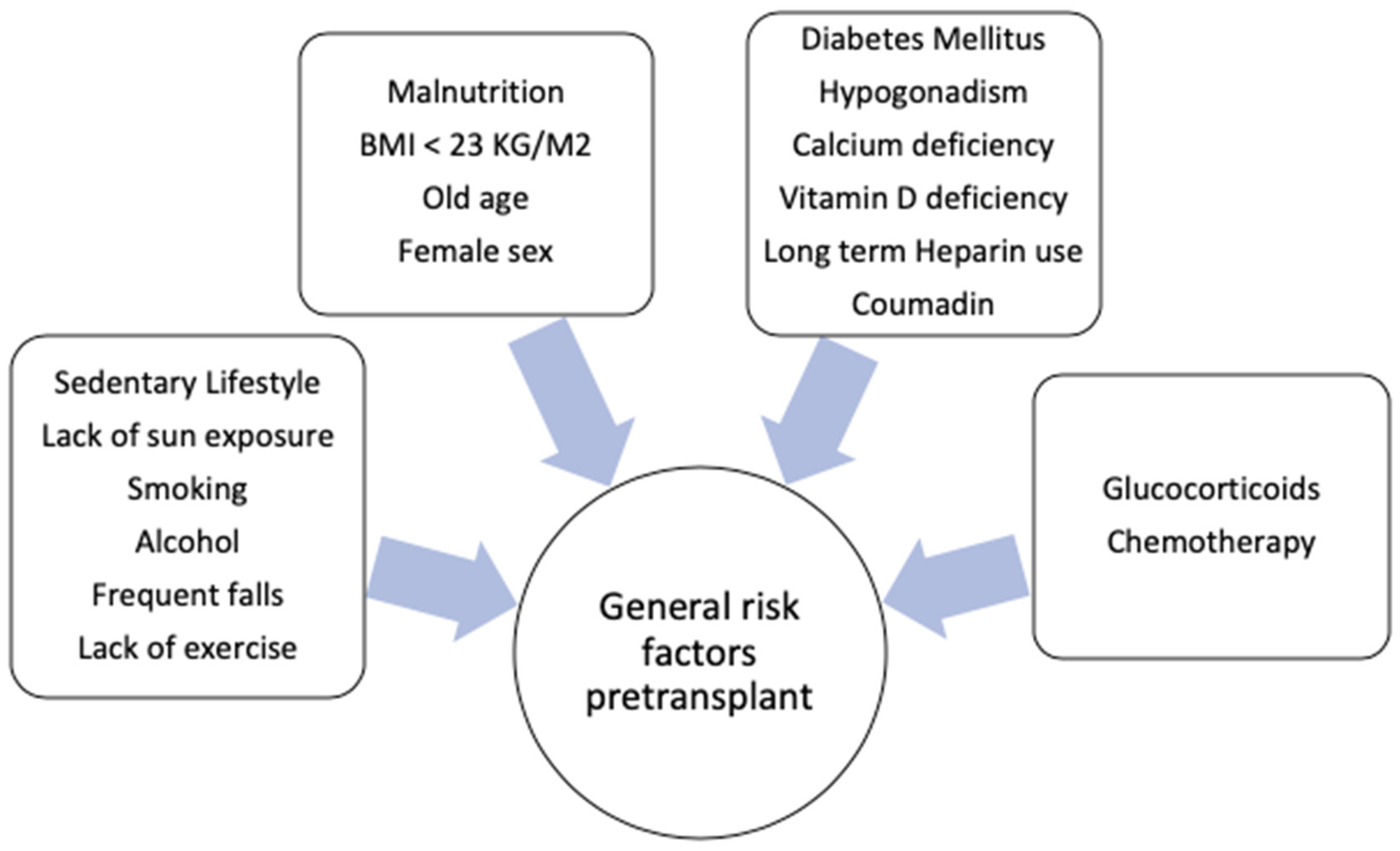
4. Overview of Risk Factors in Transplant Recipients
4.1. Organ-Specific Risk Factors
4.1.1. Solid Organ Transplants
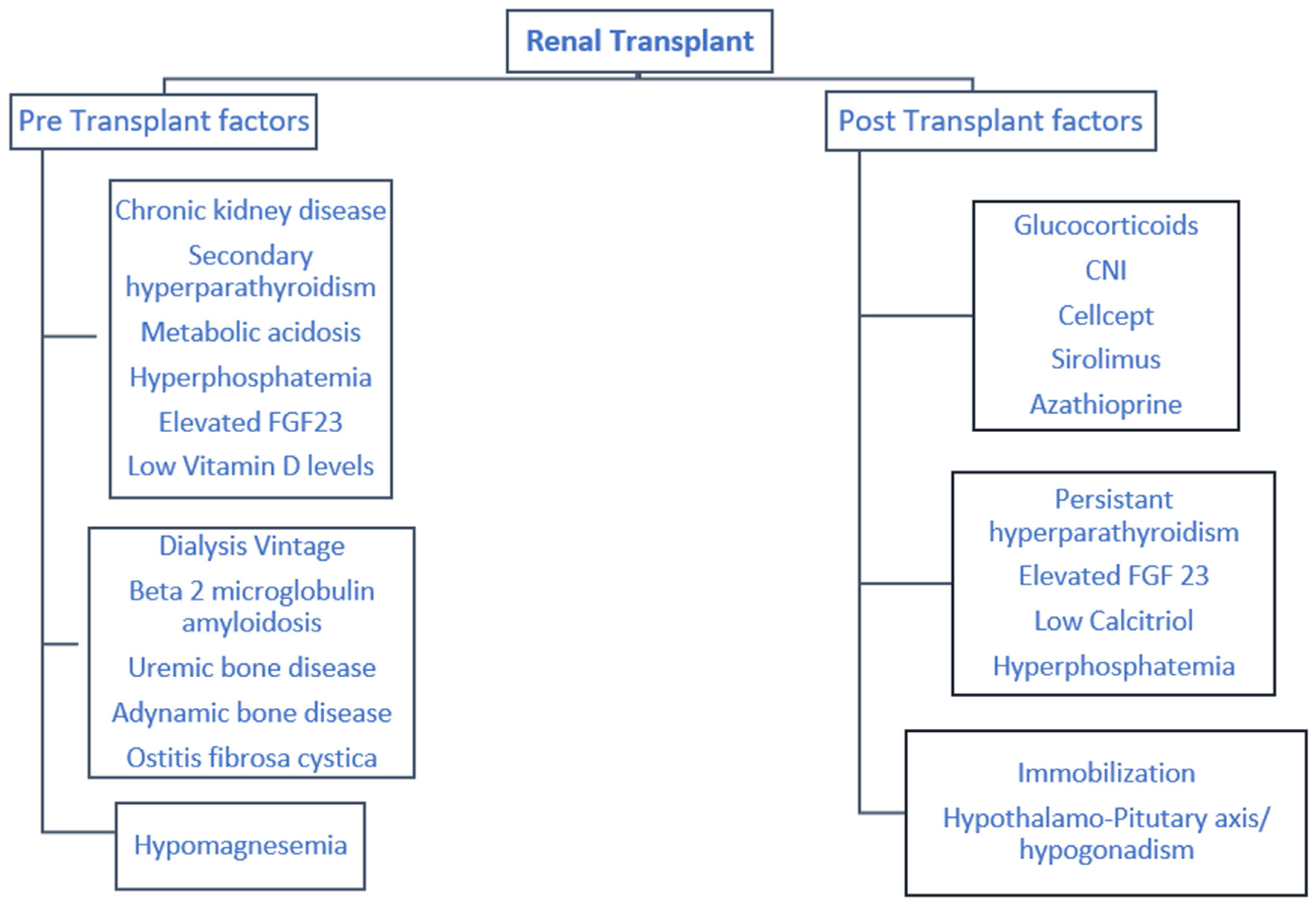
(a) Kidney
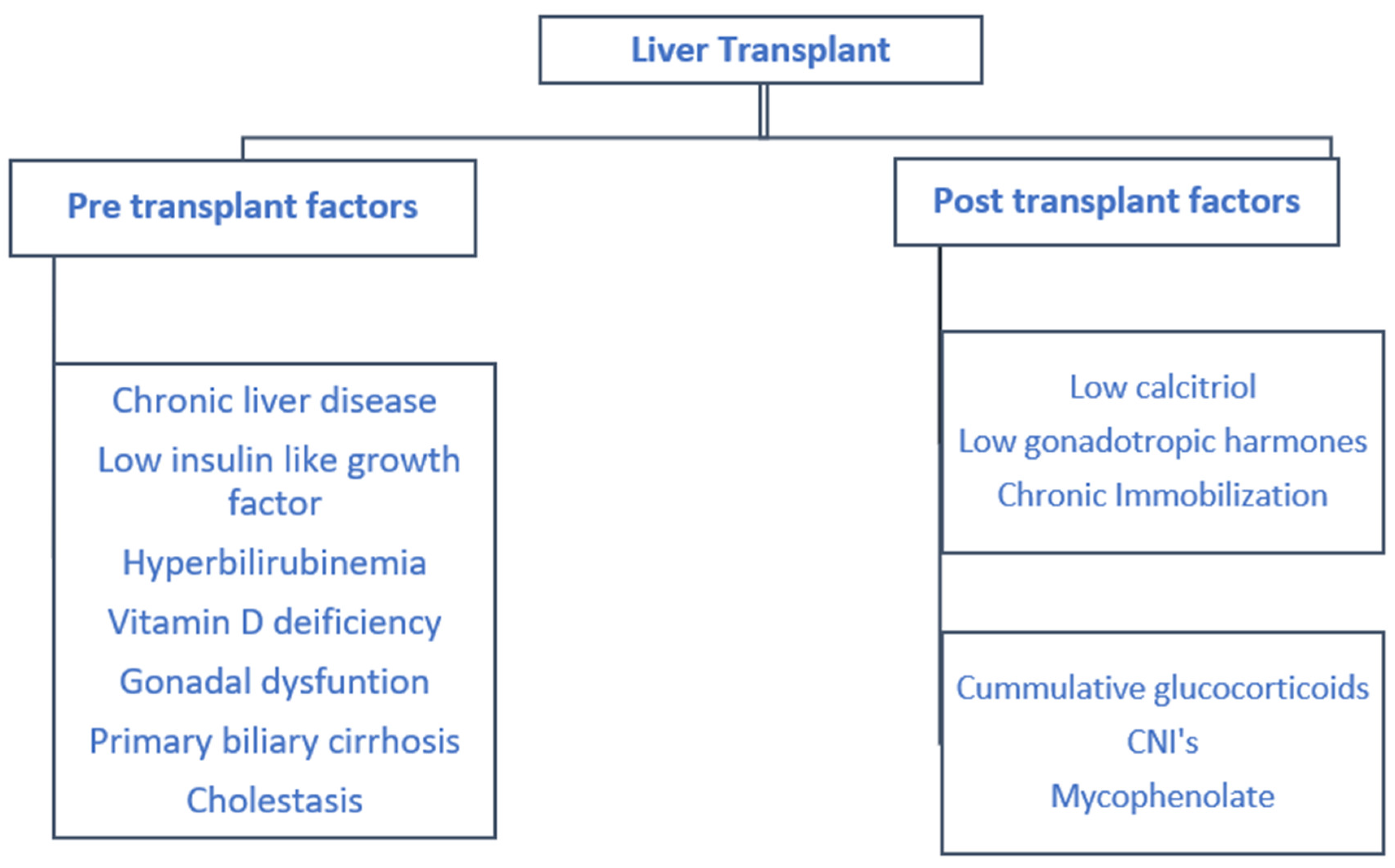
(b) Liver
(c) Heart
(d) Lung
4.1.2. Hematopoietic Stem Cell Transplant
4.2. Post-Transplant Medications
4.2.1. Glucocorticoids
4.2.2. Calcineurin Inhibitors
4.2.3. Other Immunosuppressants
4.3. Endocrine and Mineral Metabolism
4.3.1. PTH
4.3.2. Phosphorous
4.3.3. Calcitriol
4.3.4. Hypothalamic–Pituitary–Gonadal (HPG) Axis Post-Transplant
4.4. Immobilization
5. Evaluation and Diagnosis
5.1. Fracture Risk Assessment (FRAX)
5.2. DEXA Scan
5.3. Bone Biopsy
6. Management
6.1. Renal Transplant
6.2. Other Transplants
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arshad, A.; Anderson, B.; Sharif, A. Comparison of organ donation and transplantation rates between opt-out and opt-in systems. Kidney Int. 2019, 95, 1453–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maalouf, N.M.; Shane, E. Osteoporosis after Solid Organ Transplantation. J. Clin. Endocrinol. Metab. 2005, 90, 2456–2465. [Google Scholar] [CrossRef] [PubMed]
- Kulak, C.A.M.; Borba, V.Z.C.; Júnior, J.K.; Custódio, M.R. Bone disease after transplantation: Osteoporosis and fractures risk. Arq. Bras. De Endocrinol. Metabol. 2014, 58, 484–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.S.; Lim, J.-H.; Cho, J.-H.; Jung, H.-Y.; Choi, J.-Y.; Park, S.-H.; Kim, Y.-L.; Ro, H.; Lee, S.; Han, S.-Y.; et al. Pretransplant Osteoporosis and Osteopenia are Risk Factors for Fractures After Kidney Transplantation. Transplant. Proc. 2019, 51, 2704–2709. [Google Scholar] [CrossRef]
- Ball, A.M.; Gillen, D.L.; Sherrard, D.; Weiss, N.S.; Emerson, S.S.; Seliger, S.L.; Kestenbaum, B.R.; Stehman-Breen, C. Risk of hip fracture among dialysis and renal transplant recipients. JAMA 2002, 288, 3014–3018. [Google Scholar] [CrossRef] [Green Version]
- Brandenburg, V.M.; Politt, D.; Ketteler, M.; Fassbender, W.J.; Heussen, N.; Westenfeld, R.; Freuding, T.; Floege, J.; Ittel, T.H. Early Rapid Loss Followed by Long-Tter Consolidation Characterizes the Development of Lumbar Bone Mineral Density Aafter Kidney Transplant. Transplantion 2004, 77, 1566–1571. [Google Scholar] [CrossRef]
- Nikkel, L.; Hollenbeak, C.S.; Fox, E.J.; Uemura, T.; Ghahramani, N. Risk of Fractures After Renal Transplantation in the United States. Transplant. 2009, 87, 1846–1851. [Google Scholar] [CrossRef]
- Nair, S.S.; Lenihan, C.R.; Montez-Rath, M.E.; Lowenberg, D.W.; Chertow, G.M.; Winkelmayer, W.C. Temporal trends in the incidence, treatment and outcomes of hip fracture after first kidney transplantation in the United States. Arab. Archaeol. Epigr. 2014, 14, 943–951. [Google Scholar] [CrossRef] [Green Version]
- Weisinger, J.R.; Carlini, R.G.; Rojas, E.; Bellorin-Font, E. Bone Disease after Renal Transplantation. Clin. J. Am. Soc. Nephrol. 2006, 1, 1300–1313. [Google Scholar] [CrossRef] [Green Version]
- Susan Standring MBE, P. Functional Anatomy of the Musculoskeletal System; 2016; pp. 81–122. [Google Scholar]
- Melsen, F.; Steiniche, T. Bone histomorphometry. Osteoporos. Int. 1993, 3, 98–99. [Google Scholar] [CrossRef]
- Bouquegneau, A.; Salam, S.; Delanaye, P.; Eastell, R.; Khwaja, A. Bone Disease after Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2016, 11, 1282–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dounousi, E.; Leivaditis, K.; Eleftheriadis, T.; Liakopoulos, V. Osteoporosis after renal transplantation. Int. Urol. Nephrol. 2014, 47, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Tat, S.K.; Pelletier, J.-P.; Lajeunesse, D.; Fahmi, H.; Lavigne, M.; Martel-Pelletier, J. The differential expression of osteoprotegerin (OPG) and receptor activator of nuclear factor kappaB ligand (RANKL) in human osteoarthritic subchondral bone osteoblasts is an indicator of the metabolic state of these disease cells. Clin. Exp. Rheumatol. 2008, 26, 295–304. [Google Scholar]
- O’Brien, C.A.; Jia, D.; Plotkin, L.I.; Bellido, T.; Powers, C.C.; Stewart, S.A.; Manolagas, S.C.; Weinstein, R.S. Glucocorticoids Act Directly on Osteoblasts and Osteocytes to Induce Their Apoptosis and Reduce Bone Formation and Strength. Endocrinology 2004, 145, 1835–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signorelli, S.S.; Scuto, S.; Marino, E.; Giusti, M.; Xourafa, A.; Gaudio, A. Anticoagulants and Osteoporosis. Int. J. Mol. Sci. 2019, 20, 5275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikuls, T.R.; Julian, B.A.; Bartolucci, A.; Saag, K.G. Bone mineral density changes within six months of renal transplantation. Transplantion 2003, 75, 49–54. [Google Scholar] [CrossRef]
- Moe, S.M.; Drüeke, T.; Cunningham, J.; Goodman, W.; Martin, K.; Ølgaard, K.; Ott, S.; Sprague, S.; Lameire, N.; Eknoyan, G.; et al. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006, 69, 1945–1953. [Google Scholar] [CrossRef] [Green Version]
- Jorgetti, V.; Drueke, T.B. Value of the new bone classification system for pediatric patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 1730–1731. [Google Scholar] [CrossRef] [Green Version]
- Kürz, P.; Monier-Faugere, M.-C.; Bognar, B.; Werner, E.; Roth, P.; Vlachojannis, J.; Malluche, H.H. Evidence for abnormal calcium homeostasis in patients with adynamic bone disease. Kidney Int. 1994, 46, 855–861. [Google Scholar] [CrossRef] [Green Version]
- Malluche, H.H.; Monier-Faugere, M.-C.; Herberth, J. Bone disease after renal transplantation. Nat. Rev. Nephrol. 2009, 6, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Heaf, J.; Tvedegaard, E.; Kanstrup, I.-L.; Fogh-Andersen, N. Hyperparathyroidism and long-term bone loss after renal transplantation. Clin. Transplant. 2003, 17, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Rodríguez, A.P.; Concepción, M.T.; García, S.; Rufino, M.; Martín, B.; Pérez, L.; Machado, M.; De Bonis, E.; Losada, M.; et al. Parathyroid function in long-term renal transplant patients: Importance of pre-transplant PTH concentrations. Nephrol. Dial. Transplant. 1998, 13, 94–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grotz, W.H.; A Mundinger, F.; Gugel, B.; Exner, V.M.; Kirste, G.; Schollmeyer, P.J. Bone mineral density after kidney transplantation. A cross-sectional study in 190 graft recipients up to 20 years after transplantation. Transplant. 1995, 59, 982–986. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Molnar, M.Z.; Kovesdy, C.P.; Mucsi, I.; Bunnapradist, S. Management of mineral and bone disorder after kidney transplantation. Curr. Opin. Nephrol. Hypertens. 2012, 21, 389–403. [Google Scholar] [CrossRef] [PubMed]
- Scarpioni, R.; Ricardi, M.; Albertazzi, V.; De Amicis, S.; Rastelli, F.; Zerbini, L. Dialysis-related amyloidosis: Challenges and solutions. Int. J. Nephrol. Renov. Dis. 2016, 9, 319–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bathla, G.; Savage, E.; Fang, M. An Unusual Presentation of Amyloidosis. J. Gen. Intern. Med. 2014, 30, 373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julian, B.A.; Laskow, D.A.; Dubovsky, J.; Dubovsky, E.V.; Curtis, J.J.; Quarles, L.D. Rapid Loss of Vertebral Mineral Density after Renal Transplantation. New. Engl. J. Med. 1991, 325, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Almond, M.; Kwan, J.; Evans, K.; Cunningham, J. Loss of Regional Bone Mineral Density in the First 12 Months following Renal Transplantation. Nephron 1994, 66, 52–57. [Google Scholar] [CrossRef]
- Lai, J.; Shoback, D.M.; Zipperstein, J.; Lizaola, B.; Tseng, S.; Terrault, N.A. Bone Mineral Density, Bone Turnover, and Systemic Inflammation in Non-cirrhotics with Chronic Hepatitis, C. Dig. Dis. Sci. 2015, 60, 1813–1819. [Google Scholar] [CrossRef] [Green Version]
- Cemborain, A.; Castilla-Cortazar, I.; García, M.; Quirog, J.; Muguerza, B.; Picardi, A.; Santidrián, S.; Prieto, J. Osteopenia in rats with liver cirrhosis: Beneficial effects of IGF-I treatment. J. Hepatol. 1998, 28, 122–131. [Google Scholar] [CrossRef]
- Janes, C.H.; Dickson, E.R.; Okazaki, R.; Bonde, S.; McDonagh, A.F.; Riggs, B.L. Role of hyperbilirubinemia in the impairment of osteoblast proliferation associated with cholestatic jaundice. J. Clin. Investig. 1995, 95, 2581–2586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, J. Bone disease in cholestatic liver disease. Gastroenterology 1995, 108, 276–283. [Google Scholar] [CrossRef]
- Bagur, A.; Mautalen, C.; Findor, J.; Sorda, J.; Somoza, J. Risk factors for the development of vertebral and total skeleton osteoporosis in patients with primary biliary cirrhosis. Calcif. Tissue Int. 1998, 63, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Pisani, B.; Mullen, G.M. Prevention of osteoporosis in cardiac transplant recipients. Curr. Opin. Cardiol. 2002, 17, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.H.; Mull, R.L.; Keenan, G.F.; Callegari, P.E.; Dalinka, M.K.; Eisen, H.J.; Mancini, N.M.; Disesa, V.J.; Attie, M.F. Osteoporosis and bone morbidity in cardiac transplant recipients. Am. J. Med. 1994, 96, 35–41. [Google Scholar] [CrossRef]
- Shane, E.; Mancini, D.; Aaronson, K.; Silverberg, S.J.; Seibel, M.J.; Addesso, V.; McMahon, D.J. Bone mass, vitamin D deficiency, and hyperparathyroidism in congestive heart failure. Am. J. Med. 1997, 103, 197–207. [Google Scholar] [CrossRef]
- Kulak, C.A.; Borba, V.C.; Jorgetti, V.; Dos Reis, L.M.; Liu, X.S.; Kimmel, D.B.; Kulak, J.; Rabelo, L.M.; Zhou, H.; Guo, X.E.; et al. Skeletal microstructural abnormalities in postmenopausal women with chronic obstructive pulmonary disease. J. Bone Miner. Res. 2010, 25, 1931–1940. [Google Scholar] [CrossRef]
- Ionescu, A.A.; Nixon, L.S.; Evans, W.D.; Stone, M.; Lewis-Jenkins, V.; Chatham, K.; Shale, D.J. Bone Density, Body Composition, and Inflammatory Status in Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2000, 162, 789–794. [Google Scholar] [CrossRef]
- Aris, R.M.; Ontjes, D.A.; Buell, H.E.; Blackwood, A.D.; Lark, R.K.; Caminiti, M.; Brown, S.A.; Renner, J.B.; Chalermskulrat, W.; Lester, G.E. Abnormal Bone Turnover in Cystic Fibrosis Adults. Osteoporos. Int. 2002, 13, 151–157. [Google Scholar] [CrossRef]
- Wang, T.K.M.; O’Sullivan, S.; Gamble, G.D.; Ruygrok, P. Bone Density in Heart or Lung Transplant Recipients-A Longitudinal Study. Transplant. Proc. 2013, 45, 2357–2365. [Google Scholar] [CrossRef]
- Spira, A.; Gutierrez, C.; Chaparro, C.; A Hutcheon, M.; Chan, C.K. Osteoporosis and lung transplantation: A prospective study. Chest 2000, 117, 476–481. [Google Scholar] [CrossRef] [Green Version]
- McClune, B.L.; E Polgreen, L.; Burmeister, L.A.; Blaes, A.H.; A Mulrooney, D.; Burns, L.J.; Majhail, N.S. Screening, prevention and management of osteoporosis and bone loss in adult and pediatric hematopoietic cell transplant recipients. Bone Marrow Transplant. 2010, 46, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weilbaecher, K.N. Mechanisms of osteoporosis after hematopoietic cell transplantation. Boil. Blood Marrow Transplant. 2000, 6, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Bakker, B.; Massa, G.G.; Van Rijn, A.M.; Mearadji, A.; Van Der Kamp, H.J.; Niemer-Tucker, M.M.; Van Der Hage, M.H.; Broerse, J.J.; Wit, J.M. Effects of total-body irradiation on growth, thyroid and pituitary gland in rhesus monkeys. Radiother. Oncol. 1999, 51, 187–192. [Google Scholar] [CrossRef]
- Ebeling, P.R.; Thomas, D.M.; Erbas, B.; Hopper, J.L.; Szer, J.; Grigg, A.P. Mechanisms of Bone Loss Following Allogeneic and Autologous Hemopoietic Stem Cell Transplantation. J. Bone Miner. Res. 1999, 14, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Serio, B.; Pezzullo, L.; Fontana, R.; Annunziata, S.; Rosamilio, R.; Sessa, M.; Giudice, V.; Ferrara, I.; Rocco, M.; De Rosa, G.; et al. Accelerated Bone Mass Senescence After Hematopoietic Stem Cell Transplantation. Transl. Med. UniSa 2013, 5, 7–13. [Google Scholar]
- Melton, L.J.; A Kyle, R.; Achenbach, S.J.; Oberg, A.L.; Rajkumar, S.V. Fracture Risk with Multiple Myeloma: A Population-Based Study. J. Bone Miner. Res. 2004, 20, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Pundole, X.; Barbo, A.G.; Lin, H.; Champlin, R.E.; Lu, H. Increased Incidence of Fractures in Recipients of Hematopoietic Stem-Cell Transplantation. J. Clin. Oncol. 2015, 33, 1364–1370. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.-N.; Chen, H.-J.; Yang, C.-H.; Lai, C.-H.; Lin, H.-H.; Chang, C.-S.; Liang, J.-A. Risk of osteoporosis and pathologic fractures in cancer patients who underwent hematopoietic stem cell transplantation: A nationwide retrospective cohort study. Oncotarget 2017, 8, 34811–34819. [Google Scholar] [CrossRef] [Green Version]
- Stern, J.M.; Chesnut, C.H.; Bruemmer, B.; Sullivan, K.M.; Lenssen, P.; Aker, S.N.; Sanders, J. Bone density loss during treatment of chronic GVHD. Bone Marrow Transplant. 1996, 17, 395–400. [Google Scholar]
- Tauchmanovà, L.; Colao, A.; Lombardi, G.; Rotoli, B.; Selleri, C. REVIEW: Bone Loss and Its Management in Long-Term Survivors from Allogeneic Stem Cell Transplantation. J. Clin. Endocrinol. Metab. 2007, 92, 4536–4545. [Google Scholar] [CrossRef] [Green Version]
- Rojas, E.; Carlini, R.G.; Clesca, P.; Arminio, A.; Suniaga, O.; De Elguezabal, K.; Weisinger, J.R.; Hruska, K.A.; Bellorin-Font, E. The pathogenesis of osteodystrophy after renal transplantation as detected by early alterations in bone remodeling. Kidney Int. 2003, 63, 1915–1923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canalis, E.; Mazziotti, G.; Giustina, A.; Bilezikian, J.P. Glucocorticoid-induced osteoporosis: Pathophysiology and therapy. Osteoporos. Int. 2007, 18, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Ichikawa, Y.; Saito, E.; Homma, M. Importance of increased urinary calcium excretion in the development of secondary hyperparathyroidism of patients under glucocorticoid therapy. Metabolism 1983, 32, 151–156. [Google Scholar] [CrossRef]
- Horber, F.F.; Hoppeler, H.; Herren, D.; Claassen, H.; Howald, H.; Gerber, C.; Frey, F.J. Altered skeletal muscle ultrastructure in renal transplant patients on prednisone. Kidney Int. 1986, 30, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Ben, R.; Mikuls, T.; Moore, D.; Julian, B.; Bernreuter, W.; Elkins, M.; Saag, K. Incidence of hip osteonecrosis among renal transplantation recipients: A prospective study. Clin. Radiol. 2004, 59, 431–438. [Google Scholar] [CrossRef]
- Nikkel, L.; Mohan, S.; Zhang, A.; McMahon, D.J.; Boutroy, S.; Dube, G.; Tanriover, B.; Cohen, D.; Ratner, L.; Hollenbeak, C.S.; et al. Reduced fracture risk with early corticosteroid withdrawal after kidney transplant. Arab. Archaeol. Epigr. 2011, 12, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Bozkaya, G.; Nart, A.; Uslu, A.; Önman, T.; Aykas, A.; Dogan, M.; Karaca, B. Impact of Calcineurin Inhibitors on Bone Metabolism in Primary Kidney Transplant Patients. Transplant. Proc. 2008, 40, 151–155. [Google Scholar] [CrossRef]
- Schlosberg, M.; Movsowitz, C.; Epstein, S.; Ismail, F.; Fallon, M.D.; Thomas, S. The Effect of Cyclosporin A Administration and Its Withdrawal on Bone Mineral Metabolism in the Rat. Endocrinology 1989, 124, 2179–2184. [Google Scholar] [CrossRef]
- Vautour, L.M.; Melton, L.J.; Clarke, B.L.; Achenbach, S.J.; Oberg, A.L.; McCarthy, J.T. Long-term fracture risk following renal transplantation: A population-based study. Osteoporos. Int. 2003, 15, 160–167. [Google Scholar] [CrossRef]
- Kirino, S.; Fukunaga, J.; Ikegami, S.; Tsuboi, H.; Kimata, M.; Nakata, N.; Nakano, M.; Ueno, T.; Mizukawa, N.; Sugahara, T. Regulation of bone metabolism in immunosuppressant (FK506)-treated rats. J. Bone Miner. Metab. 2004, 22, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Monegal, A.; Navasa, M.; Guañabens, N.; Peris, P.; Pons, F.; De Osaba, M.J.M.; Rimola, A.; Rodes, J.; Muñoz-Gómez, J. Bone mass and mineral metabolism in liver transplant patients treated with FK506 or cyclosporine A. Calcif. Tissue Int. 2001, 68, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Dissanayake, I.R.; Goodman, G.R.; Bowman, A.R.; Pun, S.; Jee, W.S.; Epstein, S. Mycophenolate Mofetil: A Promising New Immunosuppressant that does not cause Bone Loss in the Rat1,2. Transplantion 1998, 65, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Singha, U.K.; Jiang, Y.; Yu, S.; Luo, M.; Lu, Y.; Zhang, J.; Xiao, G. Rapamycin inhibits osteoblast proliferation and differentiation in MC3T3-E1 cells and primary mouse bone marrow stromal cells. J. Cell. Biochem. 2008, 103, 434–446. [Google Scholar] [CrossRef]
- Kneissel, M.; Luong-Nguyen, N.-H.; Baptist, M.; Cortesi, R.; Zumstein-Mecker, S.; Kossida, S.; O’Reilly, T.; Lane, H.; Susa, M. Everolimus suppresses cancellous bone loss, bone resorption, and cathepsin K expression by osteoclasts. Bone 2004, 35, 1144–1156. [Google Scholar] [CrossRef]
- Wolf, M.; Weir, M.R.; Kopyt, N.; Mannon, R.B.; Von Visger, J.; Deng, H.; Yue, S.; Vincenti, F. A Prospective Cohort Study of Mineral Metabolism After Kidney Transplantation. Transplantion 2016, 100, 184–193. [Google Scholar] [CrossRef] [Green Version]
- Lou, I.; Foley, D.; Odorico, S.K.; Leverson, G.; Schneider, D.F.; Sippel, R.; Chen, H. How Well Does Renal Transplantation Cure Hyperparathyroidism. Ann. Surg. 2015, 262, 653–659. [Google Scholar] [CrossRef] [Green Version]
- Evenepoel, P.; Claes, K.; Kuypers, D.; Maes, B.; Bammens, B.; Vanrenterghem, Y. Natural history of parathyroid function and calcium metabolism after kidney transplantation: A single-centre study. Nephrol. Dial. Transplant. 2004, 19, 1281–1287. [Google Scholar] [CrossRef] [Green Version]
- Perrin, P.; Caillard, S.; Javier, R.M.; Braun, L.; Heibel, F.; Borni-Duval, C.; Muller, C.; Olagne, J.; Moulin’, B. Persistent Hyperparathyroidism Is a Major Risk Factor for Fractures in the Five Years After Kidney Transplantation. Arab. Archaeol. Epigr. 2013, 13, 2653–2663. [Google Scholar] [CrossRef]
- Reynolds, J.L.; Joannides, A.J.; Skepper, J.N.; McNair, R.; Schurgers, L.J.; Proudfoot, D.; Jahnen-Dechent, W.; Weissberg, P.L.; Shanahan, C.M. Human Vascular Smooth Muscle Cells Undergo Vesicle-Mediated Calcification in Response to Changes in Extracellular Calcium and Phosphate Concentrations: A Potential Mechanism for Accelerated Vascular Calcification in ESRD. J. Am. Soc. Nephrol. 2004, 15, 2857–2867. [Google Scholar] [CrossRef] [Green Version]
- Stein, E.M.; Shane, E. Vitamin D in organ transplantation. Osteoporos. Int. 2011, 22, 2107–2118. [Google Scholar] [CrossRef] [PubMed]
- McGregor, R.; Li, G.; Penny, H.; Lombardi, G.; Afzali, B.; Goldsmith, D. Vitamin D in Renal Transplantation —from Biological Mechanisms to Clinical Benefits. Arab. Archaeol. Epigr. 2014, 14, 1259–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.R.; Dadhania, D.; August, P.; Lee, J.B.; Suthanthiran, M.; Muthukumar, T. Circulating levels of 25-hydroxyvitamin D and acute cellular rejection in kidney allograft recipients. Transplant. 2014, 98, 292–299. [Google Scholar] [CrossRef] [Green Version]
- Shane, E.; Rivas, M.; McMahon, D.J.; Staron, R.B.; Silverberg, S.J.; Seibel, M.J.; Mancini, D.; Michler, R.E.; Aaronson, K.; Addesso, V.; et al. Bone loss and turnover after cardiac transplantation. J Clin Endocrinol. Metab. 1997, 82, 1497–1506. [Google Scholar] [CrossRef]
- Guechot, J.; Chazouilleres, O.; Loria, A.; Hannoun, L.; Balladur, P.; Parc, R.; Giboudeau, J.; Poupon, R. Effect of liver transplantation on sex-hormone disorders in male patients with alcohol-induced or post-viral hepatitis advanced liver disease. J. Hepatol. 1994, 20, 426–430. [Google Scholar] [CrossRef]
- Saha, M.-T.; Saha, H.H.; Niskanen, L.K.; Salmela, K.T.; Pasternack, A.I. Time course of serum prolactin and sex hormones following successful renal transplantation. Nephron 2002, 92, 735–737. [Google Scholar] [CrossRef]
- Vintro, A.Q.; Krasnoff, J.B.; Painter, P. Roles of Nutrition and Physical Activity in Musculoskeletal Complications Before and After Liver Transplantation. AACN Clin. Issues: Adv. Pr. Acute Crit. Care 2002, 13, 333–347. [Google Scholar] [CrossRef]
- Kwan, J.T.; Almond, M.K.; Evans, K.; Cunningham, J. Changes in total body bone mineral content and regional bone mineral density in renal patients following renal transplantation. Miner. Electrolyte Metab. 1992, 18, 166–168. [Google Scholar]
- Kidney Disease: Improving Global Outcomes (KDIGO). CKD-MBD Update Work Group KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef] [Green Version]
- Crippin, J.S. Bone disease after liver transplantation. Liver Transplant. 2001, 7, S27–S35. [Google Scholar] [CrossRef]
- Naylor, K.L.; Leslie, W.D.; Hodsman, A.B.; Rush, D.; Garg, A.X. FRAX Predicts Fracture Risk in Kidney Transplant Recipients. Transplantation 2014, 97, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Brandenburg, V.M.; Ketteler, M.; Heussen, N.; Politt, D.; Frank, R.D.; Westenfeld, R.; Ittel, T.H.; Floege, J. Lumbar bone mineral density in very long-term renal transplant recipients: Impact of circulating sex hormones. Osteoporos. Int. 2005, 16, 1611–1620. [Google Scholar] [CrossRef] [PubMed]
- Akaberi, S.; Simonsen, O.; Lindergård, B.; Nyberg, G. Can DXA Predict Fractures in Renal Transplant Patients? Arab. Archaeol. Epigr. 2008, 8, 2647–2651. [Google Scholar] [CrossRef] [PubMed]
- Cueto-Manzano, A.M.; Konel, S.; Hutchison, A.J.; Crowley, V.; France, M.W.; Freemont, A.; Adams, J.E.; Mawer, B.; Gokal, R. Bone loss in long-term renal transplantation: Histopathology and densitometry analysis. Kidney Int. 1999, 55, 2021–2029. [Google Scholar] [CrossRef] [Green Version]
- Van Staa, T.; Laan, R.F.; Barton, I.P.; Cohen, S.; Reid, D.M.; Cooper, C. Bone density threshold and other predictors of vertebral fracture in patients receiving oral glucocorticoid therapy. Arthritis Rheum. 2003, 48, 3224–3229. [Google Scholar] [CrossRef]
- Isakova, T.; Nickolas, T.L.; Denburg, M.; Yarlagadda, S.; Weiner, D.E.; Gutiérrez, O.M.; Bansal, V.; Rosas, S.E.; Nigwekar, S.; Yee, J.; et al. KDOQI US Commentary on the 2017 KDIGO Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Am. J. Kidney Dis. 2017, 70, 737–751. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, K.; Pauchard, Y.; Nikkel, L.; Iyer, S.; Zhang, C.; McMahon, D.; Cohen, D.; Boyd, S.K.; Shane, E.; Nickolas, T.L. Longitudinal HR-pQCT and Image Registration Detects Endocortical Bone Loss in Kidney Transplantation Patients. J. Bone Miner. Res. 2015, 30, 554–561. [Google Scholar] [CrossRef]
- Komaba, H.; Tanaka, M.; Fukagawa, M. Treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Intern. Med. 2008, 47, 989–994. [Google Scholar] [CrossRef] [Green Version]
- Kulak, C.A.M.; Borba, V.Z.C.; Kulak, J.; Custódio, M.R. Osteoporosis after solid organ transplantation. Minerva Endocrinol. 2012, 37, 221–231. [Google Scholar]
- Bonomini, V.; Bortolotti, G.C.; Feletti, C.; Scolari, M.P. Serial histomorphometric and histochemical bone biopsy studies in dialysis and transplantation. J. d’urologie et de Nephrol. 1975, 81, 941–950. [Google Scholar]
- Vangala, C.; Pan, J.; Cotton, R.T.; Ramanathan, V. Mineral and Bone Disorders After Kidney Transplantation. Front. Med. 2018, 5, 211. [Google Scholar] [CrossRef]
- Leidig-Bruckner, G.; Hosch, S.; Dodidou, P.; Ritschel, D.; Conradt, C.; Klose, C.; Otto, G.; Lange, R.; Theilmann, L.; Zimmerman, R.; et al. Frequency and predictors of osteoporotic fractures after cardiac or liver transplantation: A follow-up study. Lancet 2001, 357, 342–347. [Google Scholar] [CrossRef]
- Elder, G. Pathophysiology and Recent Advances in the Management of Renal Osteodystrophy. J. Bone Miner. Res. 2002, 17, 2094–2105. [Google Scholar] [CrossRef] [PubMed]
- De Sévaux, R.G.L.; Hoitsma, A.J.; Corstens, F.H.M.; Wetzels, J.F.M. Treatment with vitamin D and calcium reduces bone loss after renal transplantation: A randomized study. J. Am. Soc. Nephrol. 2002, 13, 1608–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponticelli, C.; Sala, G. Vitamin D: A new player in kidney transplantation? Expert Rev. Clin. Immunol. 2014, 10, 1375–1383. [Google Scholar] [CrossRef]
- Weber, T.J.; Quarles, L.D. Preventing bone loss after renal transplantation with bisphosphonates: We can… but should we? Kidney Int. 2000, 57, 735–737. [Google Scholar] [CrossRef] [Green Version]
- Bonani, M.; Frey, D.; Brockmann, J.; Fehr, T.; Mueller, T.; Saleh, L.; Von Eckardstein, A.; Graf, N.; Wüthrich, R. Effect of twice-yearly denosumab on prevention of bone mineral density loss in de novo kidney transplant recipients: A randomized controlled trial. Arab. Archaeol. Epigr. 2016, 16, 1882–1891. [Google Scholar] [CrossRef] [Green Version]
- Amer, H.; Griffin, M.D.; Stegall, M.D.; Cosio, F.G.; Park, W.D.; Kremers, W.K.; Heilman, R.L.; Mazur, M.J.; Hamawi, K.; Larson, T.S.; et al. Oral Paricalcitol Reduces the Prevalence of Posttransplant Hyperparathyroidism: Results of an Open Label Randomized Trial. Arab. Archaeol. Epigr. 2013, 13, 1576–1585. [Google Scholar] [CrossRef] [Green Version]
- Mitterbauer, C.; Schwarz, C.; Haas, M.; Oberbauer, R. Effects of bisphosphonates on bone loss in the first year after renal transplantation—a meta-analysis of randomized controlled trials. Nephrol. Dial. Transplant. 2006, 21, 2275–2281. [Google Scholar] [CrossRef] [Green Version]
- El-Agroudy, A.E.; El-Husseini, A.A.; El-Sayed, M.; Mohsen, T.; Ghoneim, M.A.; El-Agroudy, A.A.E.-H.A.E. A prospective randomized study for prevention of postrenal transplantation bone loss. Kidney Int. 2005, 67, 2039–2045. [Google Scholar] [CrossRef] [Green Version]
- Kan, S.-L.; Ning, G.-Z.; Chen, L.-X.; Zhou, Y.; Sun, J.-C.; Feng, S. Efficacy and Safety of Bisphosphonates for Low Bone Mineral Density after Kidney Transplantation. Medicine 2016, 95, e2679. [Google Scholar] [CrossRef] [PubMed]
- Coco, M. Prevention of Bone Loss in Renal Transplant Recipients: A Prospective, Randomized Trial of Intravenous Pamidronate. J. Am. Soc. Nephrol. 2003, 14, 2669–2676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonani, M.; Frey, D.; Meyer, U.; Graf, N.; A Bischoff-Ferrari, H.; Wüthrich, R.P. Effect of Denosumab on Peripheral Compartmental Bone Density, Microarchitecture and Estimated Bone Strength in De Novo Kidney Transplant Recipients. Kidney Blood Press. Res. 2016, 41, 614–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamy, O.; Gonzalez-Rodriguez, E.; Stoll, D.; Hans, D.; Aubry-Rozier, B. Faculty Opinions recommendation of Severe Rebound-Associated Vertebral Fractures After Denosumab Discontinuation: 9 Clinical Cases Report. Fac. Opin.—Post-Publ. Peer Rev. Biomed. Lit. 2017, 102, 354–358. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Acharya, P.; Acharya, C.; Chenbhanich, J.; Bathini, T.; Boonpheng, B.; Sharma, K.; Wijarnpreecha, K.; Ungprasert, P.; Suarez, M.G.; et al. Hypocalcemia and bone mineral density changes following denosumab treatment in end-stage renal disease patients: A meta-analysis of observational studies. Osteoporos. Int. 2018, 29, 1737–1745. [Google Scholar] [CrossRef]
- Zhao, J.; Wang, C.; Hu, Z. Efficacy and Safety of Bisphosphonates for Osteoporosis or Osteopenia in Cardiac Transplant Patients: A Meta-Analysis. Transplant. Proc. 2015, 47, 2957–2964. [Google Scholar] [CrossRef] [PubMed]
- Kananen, K.; Volin, L.; Laitinen, K.; Alfthan, H.; Ruutu, T.; Valimaki, M.J. Prevention of Bone Loss after Allogeneic Stem Cell Transplantation by Calcium, Vitamin D, and Sex Hormone Replacement with or without Pamidronate. J. Clin. Endocrinol. Metab. 2005, 90, 3877–3885. [Google Scholar] [CrossRef] [Green Version]
- Grigg, A.P.; Shuttleworth, P.; Reynolds, J.; Schwarer, A.P.; Szer, J.; Bradstock, K.; Hui, C.; Herrmann, R.; Ebeling, P.R. Pamidronate Reduces Bone Loss after Allogeneic Stem Cell Transplantation. J. Clin. Endocrinol. Metab. 2006, 91, 3835–3843. [Google Scholar] [CrossRef] [Green Version]
- Atamaz, F.C.; Hepguler, S.; Akyildiz, M.; Karasu, Z.; Kılıç, M. Özgür; Kılıç, M. Effects of alendronate on bone mineral density and bone metabolic markers in patients with liver transplantation. Osteoporos. Int. 2006, 17, 942–949. [Google Scholar] [CrossRef]
- Monegal, A.; Guañabens, N.; Suárez, M.J.; Suarez, F.; Clemente, G.; García-González, M.; De La Mata, M.; Serrano, T.; Casafont, F.; Torne, S.; et al. Pamidronate in the prevention of bone loss after liver transplantation: A randomized controlled trial. Transpl. Int. 2008, 22, 198–206. [Google Scholar] [CrossRef]
- Grigg, A.; on behalf of the Australasian Leukaemia and Lymphoma Group (ALLG); Butcher, B.; Khodr, B.; Bajel, A.; Hertzberg, M.; Patil, S.; D’Souza, A.B.; Ganly, P.; Ebeling, P.; et al. An individualised risk-adapted protocol of pre- and post transplant zoledronic acid reduces bone loss after allogeneic stem cell transplantation: Results of a phase II prospective trial. Bone Marrow Transplant. 2017, 52, 1288–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, E.M.; Ortiz, D.; Jin, Z.; McMahon, N.J.; Shane, E. Prevention of fractures after solid organ transplantation: A meta-analysis. J. Clin. Endocrinol. Metab. 2011, 96, 3457–3465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.; Addesso, V.; McMahon, D.; Staron, R.B.; Namerow, P.; Maybaum, S.; Mancini, D.; Shane, E. Discontinuing Antiresorptive Therapy One Year after Cardiac Transplantation: Effect on Bone Density and Bone Turnover. Transplant. 2006, 81, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Sambrook, P.; Henderson, N.K.; Keogh, A.; Macdonald, P.; Glanville, A.; Spratt, P.; Bergin, P.; Ebeling, P.; Eisman, J. Effect of Calcitriol on Bone Loss After Cardiac or Lung Transplantation. J. Bone Miner. Res. 2000, 15, 1818–1824. [Google Scholar] [CrossRef] [Green Version]
- Bianda, T.; Linka, A.; Junga, G.; Brunner, H.; Steinert, H.; Kiowski, W.; Schmid, C. Prevention of osteoporosis in heart transplant recipients: A comparison of calcitriol with calcitonin and pamidronate. Calcif. Tissue Int. 2000, 67, 116–121. [Google Scholar] [CrossRef]
- Isoniemi, H.; Appelberg, J.; Nilsson, C.-G.; Mäkelä, P.; Risteli, J.; Höckerstedt, K. Transdermal oestrogen therapy protects postmenopausal liver transplant women from osteoporosis. A 2-year follow-up study. J. Hepatol. 2001, 34, 299–305. [Google Scholar] [CrossRef]
- Brunova, J.; Kratochvílová, S.; Stepankova, J. Osteoporosis Therapy with Denosumab in Organ Transplant Recipients. Front. Endocrinol. 2018, 9, 162. [Google Scholar] [CrossRef] [Green Version]
- Cejka, D.; Benesch, T.; Krestan, C.; Roschger, P.; Klaushofer, K.; Pietschmann, P.; Haas, M. Effect of Teriparatide on Early Bone Loss After Kidney Transplantation. Arab. Archaeol. Epigr. 2008, 8, 1864–1870. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Heart | Lung | Bone Marrow | |
|---|---|---|---|
| Organ-specific risk factors |
|
|
|
| Evaluation |
|---|
| (a) History/Physical |
| H/O recent fracture |
| Back pain/bone pain |
| Family H/O osteoporosis |
| Exercise |
| Smoking cessation |
| Alcohol cessation |
| (b) Serologies |
| Serum calcium level |
| Serum phosphorous level |
| Serum parathyroid level |
| Estrogen levels |
| Progesterone level |
| TSH level |
| (c) FRAX |
| Predicts 10% fracture risk |
| (d) DEXA-scan Annually |
| General Measures |
|---|
|
| Renal Transplant | Other Transplants | |
|---|---|---|
| Treatment options |
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovvuru, K.; Kanduri, S.R.; Vaitla, P.; Marathi, R.; Gosi, S.; Garcia Anton, D.F.; Cabeza Rivera, F.H.; Garla, V. Risk Factors and Management of Osteoporosis Post-Transplant. Medicina 2020, 56, 302. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060302
Kovvuru K, Kanduri SR, Vaitla P, Marathi R, Gosi S, Garcia Anton DF, Cabeza Rivera FH, Garla V. Risk Factors and Management of Osteoporosis Post-Transplant. Medicina. 2020; 56(6):302. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060302
Chicago/Turabian StyleKovvuru, Karthik, Swetha Rani Kanduri, Pradeep Vaitla, Rachana Marathi, Shiva Gosi, Desiree F. Garcia Anton, Franco H. Cabeza Rivera, and Vishnu Garla. 2020. "Risk Factors and Management of Osteoporosis Post-Transplant" Medicina 56, no. 6: 302. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060302