Early Neurological Assessment and Long-Term Neuromotor Outcomes in Late Preterm Infants: A Critical Review

 ,
, 
Abstract
:1. Introduction
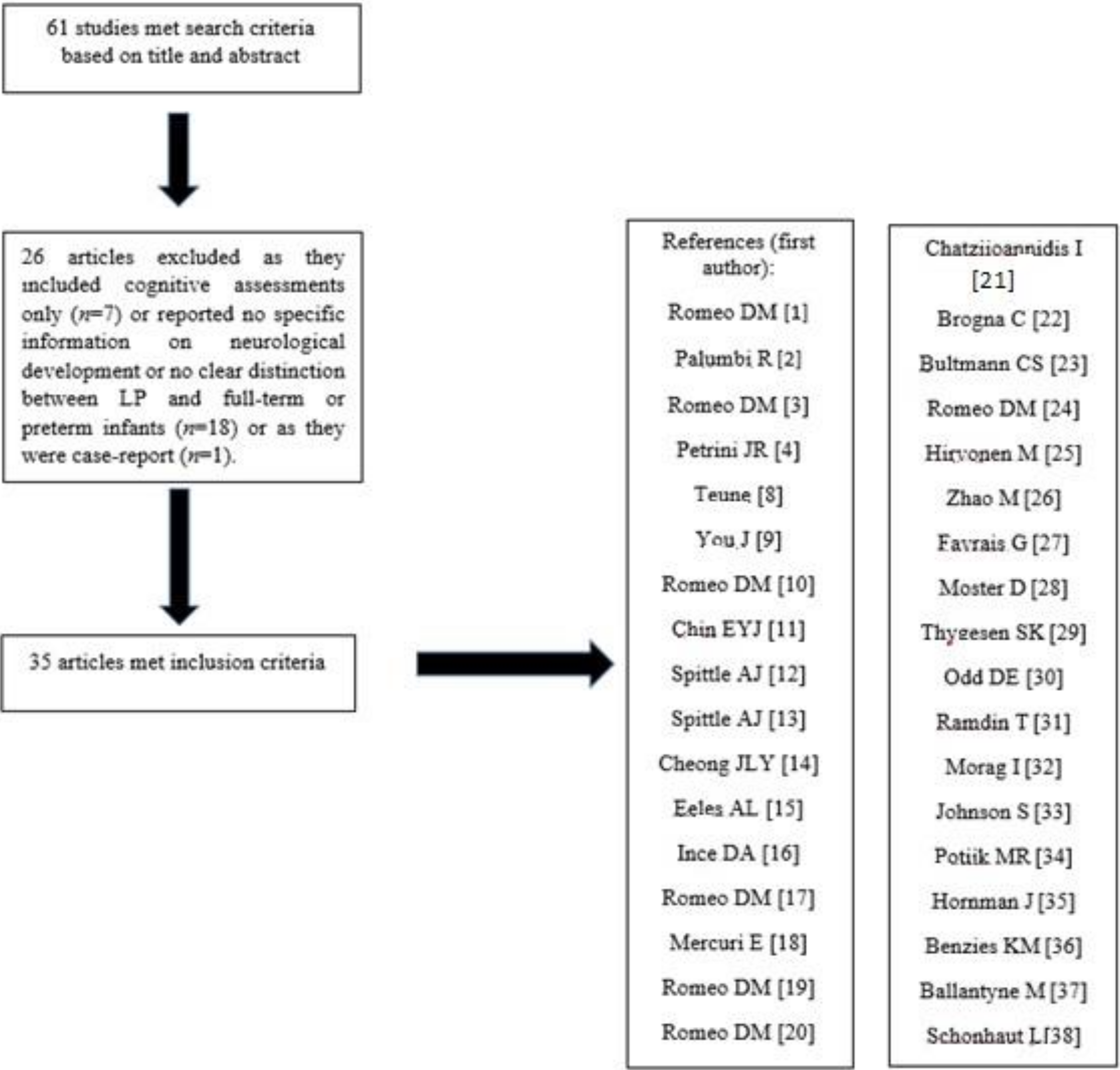
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction and Analysis
- (1)
- studies reporting neonatal neurological examination;
- (2)
- studies reporting data about the neurological examination in the first two years of life;
- (3)
- studies reporting incidence of CP and motor disorders in LP patients.
3. Results
3.1. Studies Reporting Neonatal Neurological Assessment
3.2. Studies Reporting Data after the Neonatal Period, in the First Two Years after Birth
3.3. Studies Reporting Incidence of CP and Motor Disorder During the Infancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Romeo, D.M.; Brogna, C.; Mercuri, E. Neurological assessment of late-preterm infants during the first year of age. Eur. J. Paediatr. Neurol. 2018, 22, 579–580. [Google Scholar] [CrossRef]
- Palumbi, R.; Peschechera, A.; Margari, A.; Craig, F.; Cristella, A.; Petruzzelli, M.G.; Margari, L. Neurodevelopmental and emotional-behavioral outcomes in late-preterm infants: An observational descriptive case study. BMC Pediatr. 2018, 18, 318. [Google Scholar] [CrossRef] [PubMed]
- Romeo, D.M.; Luciano, R.; Corsello, M.; Ricci, D.; Brogna, C.; Zuppa, A.; Romagnoli, C.; Mercuri, E. Neonatal neurological examination of late preterm babies. Early Hum. Dev. 2013, 89, 537–545. [Google Scholar] [CrossRef]
- Petrini, J.R.; Dias, T.; McCormick, M.C.; Massolo, M.L.; Green, N.S.; Escobar, G.J. Increased risk of adverse neurological development for late preterm infants. J. Pediatr. 2009, 154, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Cheong, J.L.; Doyle, L.W.; Burnett, A.C.; Lee, K.J.; Walsh, J.M.; Potter, C.R.; Treyvaud, K.; Thompson, D.K.; Olsen, J.E.; Anderson, P.J.; et al. Association Between Moderate and Late Preterm Birth and Neurodevelopment and Social-Emotional Development at Age 2 Years. JAMA Pediatr. 2017, 171, e164805. [Google Scholar] [CrossRef] [PubMed]
- Woythaler, M.A.; McCormick, M.C.; Smith, V.C. Late preterm infants have worse 24-month neurodevelopmental outcomes than term infants. Pediatrics 2011, 127, e622–e629. [Google Scholar] [CrossRef] [Green Version]
- Morse, S.B.; Zheng, H.; Tang, Y.; Roth, J. Early school-age outcomes of late preterm infants. Pediatrics 2009, 123, e622–e629. [Google Scholar] [CrossRef] [Green Version]
- Teune, M.J.; Bakhuizen, S.; Bannerman, C.G.; Opmeer, B.C.; van Kaam, A.H.; van Wassenaer, A.G.; Morris, J.M.; Mol, B.W.J. A systematic review of severe morbidity in infants born late preterm. Am. J. Obstet. Gynecol. 2011, 205, 374.e1. [Google Scholar] [CrossRef]
- You, J.; Yang, H.; Hao, M.; Zheng, J. Late Preterm Infants’ Social Competence, Motor Development, and Cognition. Front. Psychiatry 2019, 10, 69. [Google Scholar] [CrossRef] [Green Version]
- Romeo, D.M.; Ricci, D.; Brogna, C.; Cilauro, S.; Lombardo, M.E.; Romeo, M.G.; Mercuri, E. Neurological examination of late-preterm infants at term age. Eur. J. Paediatr. Neurol. 2011, 15, 353–360. [Google Scholar] [CrossRef]
- Chin, E.Y.J.; Baral, V.R.; Ereno, I.L.; Allen, J.C.; Low, K.; Yeo, C.L. Evaluation of neurological behaviour in late-preterm newborn infants using the Hammersmith Neonatal Neurological Examination. J. Paediatr. Child Health 2019, 55, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Walsh, J.; Olsen, J.E.; McInnes, E.; Eeles, A.L.; Brown, N.C.; Anderson, P.J.; Doyle, L.W.; Cheong, J.L.Y. Neurobehaviour and neurological development in the first month after birth for infants born between 32–42 weeks’ gestation. Early Hum. Dev. 2016, 96, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Walsh, J.M.; Potter, C.; McInnes, E.; Olsen, J.E.; Lee, K.J.; Anderson, P.J.; Doyle, L.W.; Cheong, J.L.Y. Neurobehaviour at term-equivalent age and neurodevelopmental outcomes at 2 years in infants born moderate-to-late preterm. Dev. Med. Child Neurol. 2017, 59, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Cheong, J.L.Y.; Thompson, D.K.; Olsen, J.E.; Spittle, A.J. Late preterm births: New insights from neonatal neuroimaging and neurobehaviour. Semin. Fetal Neonatal Med. 2019, 24, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Eeles, A.L.; Walsh, J.M.; Olsen, J.E.; Cuzzilla, R.; Thompson, D.K.; Anderson, P.K.J.; Doyle, L.W.; Cheong, J.L.Y.; Spittle, A.J. Continuum of neurobehaviour and its associations with brain MRI in infants born preterm. BMJ Paediatr. Open 2017, 1, e000136. [Google Scholar] [CrossRef] [Green Version]
- Ince, D.A.; Ecevit, A.; Yıldız, M.; Tugcu, A.U.; Ceran, B.; Tekindal, M.A.; Turan, O.; Tarcan, A. Evaluation of Moro reflex with an objective method in late preterm and term infants. Early Hum. Dev. 2019, 129, 60–64. [Google Scholar] [CrossRef]
- Romeo, D.M.; Ricci, D.; Serrao, F.; Gallini, F.; Olivieri, G.; Cota, F.; Romagnoli, C.; Mercuri, E. Visual function assessment in late-preterm newborns. Early Hum. Dev. 2012, 88, 301–305. [Google Scholar] [CrossRef]
- Mercuri, E.; Ricci, D.; Romeo, D.M. Neurological and visual assessments in very and late low-risk preterm infants. Early Hum. Dev. 2012, 88, S31–S33. [Google Scholar] [CrossRef]
- Romeo, D.M.; Cioni, M.; Guzzetta, A.; Scoto, M.; Conversano, M.; Palermo, F.; Romeo, M.G.; Mercuri, E. Application of a scorable neurological examination to near-term infants: Longitudinal data. Neuropediatrics 2007, 38, 233–238. [Google Scholar] [CrossRef]
- Romeo, D.M.; Brogna, C.; Sini, F.; Romeo, M.G.; Cota, F.; Ricci, D. Early psychomotor development of low-risk preterm infants: Influence of gestational age and gender. Eur. J. Paediatr. Neurol. 2016, 20, 518–523. [Google Scholar] [CrossRef]
- Chatziioannidis, I.; Kyriakidou, M.; Exadaktylou, S.; Antoniou, E.; Zafeiriou, D.; Nikolaides, N. Neurological outcome at 6 and 12 months corrected age in hospitalised late preterm infants -a prospective study. Eur. J. Paediatr. Neurol. 2018, 22, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Brogna, C.; Romeo, D.M.; Cervesi, C.; Scrofani, L.; Romeo, M.G.; Mercuri, E.; Guzzetta, A. Prognostic value of the qualitative assessments of general movements in late-preterm infants. Early Hum. Dev. 2013, 89, 1063–1066. [Google Scholar] [CrossRef] [PubMed]
- Bultmann, C.S.; Orlikowsky, T.; Häusler, M.; Trepels-Kottek, S.; Disselhorst-Klug, C.; Schoberer, M. Spontaneous movements in the first four months of life: An accelerometric study in moderate and late preterm infants. Early Hum. Dev. 2019, 130, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Romeo, D.M.; Cioni, M.; Scoto, M.; Palermo, F.; Pizzardi, A.; Sorge, A.; Romeo, M.G. Development of the forward parachute reaction and the age of walking in near term infants: A longitudinal observational study. BMC Pediatr. 2009, 9, 13. [Google Scholar] [CrossRef] [Green Version]
- Hirvonen, M.; Ojala, R.; Korhonen, P.; Haataja, P.; Eriksson, K.; Gissler, M.; Luukkaala, T.; Tammela, O. Cerebral palsy among children born moderately and late preterm. Pediatrics 2014, 134, e1584–e1593. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Dai, H.; Deng, Y.; Zhao, L. SGA as a Risk Factor for Cerebral Palsy in Moderate to Late Preterm Infants: A System Review and Meta-analysis. Sci. Rep. 2016, 6, 38853. [Google Scholar] [CrossRef]
- Favrais, G.; Saliba, E. Neurodevelopmental outcome of late-preterm infants: Literature review. Arch. Pediatr. 2019, 26, 492–496. [Google Scholar] [CrossRef]
- Moster, D.; Lie, R.T.; Markestad, T. Long-term medical and social consequences of preterm birth. N. Engl. J. Med. 2008, 359, 262–273. [Google Scholar] [CrossRef] [Green Version]
- Thygesen, S.K.; Olsen, M.; Østergaard, J.R.; Sørensen, H.T. Respiratory distress syndrome in moderately late and late preterm infants and risk of cerebral palsy: A population-based cohort study. BMJ Open 2016, 6, e011643. [Google Scholar] [CrossRef] [Green Version]
- Odd, D.E.; Lingam, R.; Emond, A.; Whitelaw, A. Movement outcomes of infants born moderate and late preterm. Acta Paediatr. 2013, 102, 876–882. [Google Scholar] [CrossRef]
- Ramdin, T.; Ballot, D.; Rakotsoane, D.; Madzudzo, L.; Brown, N.; Chirwa, T.; Cooper, P.; Davies, V. Neurodevelopmental outcome of late preterm infants in Johannesburg. South Africa. BMC Pediatr. 2018, 18, 326. [Google Scholar] [CrossRef] [Green Version]
- Morag, I.; Bart, O.; Raz, R.; Shayevitz, S.; Simchen, M.J.; Strauss, T.; Zangen, S.; Kuint, J.; Gabis, L. Developmental characteristics of late preterm infants at six and twelve months: A prospective study. Infant Behav. Dev. 2013, 36, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Evans, T.A.; Draper, E.S.; Field, D.J.; Manktelow, B.N.; Marlow, N.; Matthews, R.; Petrou, S.; Seaton, S.E.; Smith, L.K.; et al. Neurodevelopmental outcomes following late and moderate prematurity: A population-based cohort study. Arch. Dis. Child Fetal Neonatal Ed. 2015, 100, F301–F308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potijk, M.R.; Kerstjens, J.M.; Bos, A.F.; Reijneveld, S.A.; de Winter, A.F. Developmental Delay in Moderately Preterm-Born Children With Low Socioeconomic Status: Risks Multiply. J. Pediatr. 2013, 163, 1289–1295. [Google Scholar] [CrossRef]
- Hornman, J.; de Winter, A.F.; Kerstjens, J.M.; Bos, A.F.; Reijneveld, S.A. Stability of Developmental Problems After School Entry of Moderately-Late Preterm and Early Preterm-Born Children. J. Pediatr. 2017, 187, 73–79. [Google Scholar] [CrossRef]
- Benzies, K.M.; Magill-Evans, J.; Ballantyne, M.; Kurilova, J. Longitudinal Patterns of Early Development in Canadian Late Preterm Infants: A Prospective Cohort Study. J. Child Health Care 2017, 21, 85–93. [Google Scholar] [CrossRef]
- Ballantyne, M.; Benzies, K.M.; McDonald, S.; Magill-Evans, J.; Tough, S. Risk of Developmental Delay: Comparison of Late Preterm and Full Term Canadian Infants at Age 12 Months. Early Hum. Dev. 2016, 101, 27–32. [Google Scholar] [CrossRef]
- Schonhaut, L.; Armijo, I.; Pérez, M. Gestational Age and Developmental Risk in Moderately and Late Preterm and Early Term Infants. Pediatrics 2015, 135, e835–e841. [Google Scholar] [CrossRef] [Green Version]
- Adams-Chapman, I. Neurodevelopmental outcome of the late preterm infant. Clin. Perinatol. 2006, 33, 947–964. [Google Scholar] [CrossRef] [PubMed]
- Engle, W.A.; Tomashek, K.M.; Wallman, C. Committee on Fetus and Newborn, American Academy of Pediatrics. “Late-preterm” infants: A population at risk. Pediatrics 2007, 120, 1390–1401. [Google Scholar] [CrossRef] [Green Version]
- De Vries, L.S.; van Haastert, I.C.; Benders, M.J.; Groenendaal, F. Myth: Cerebral palsy cannot be predicted by neonatal brain imaging. Semin. Fetal Neonatal Med. 2011, 16, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, M.; Ramenghi, L.A.; De Carli, A.; Bassi, L.; Farè, P.; Dessimone, F.; Pisoni, S.; Sirgiovanni, I.; Groppo, M.; Ometto, A.; et al. Cranial ultrasound findings in late preterm infants and correlation with perinatal risk factors. Ital. J. Pediatr. 2015, 41, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, J.M.; Doyle, L.W.; Anderson, P.J.; Lee, K.L.; Cheong, J.L.Y. Moderate and late preterm birth: Effect on brain size and maturation at term-equivalent age. Radiology 2014, 273, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Romeo, D.M.; Chorna, O.; Novak, I.; Galea, C.; Del Secco, S.; Guzzetta, A. The Pooled Diagnostic Accuracy of Neuroimaging, General Movements, and Neurological Examination for Diagnosing Cerebral Palsy Early in High-Risk Infants: A Case Control Study. J. Clin. Med. 2019, 8, 1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors | No. of Patients | Ga (Weeks) | M:F | Age of Assessment | Tool | Main Results |
|---|---|---|---|---|---|---|
| Romeo et al. [10] | 375 | 34–36 | 1.09 | Term-age | HNNE | Differences in scoring among the GAs |
| Romeo et al. [3] | 118 | 34–36 | 1.18 | 48–72 h after birth | HNNE | Similar distribution of the scores among the GAs |
| Chin et al. [11] | 79 | 34–36 | 1.19 | 12–72 h after birth and at term-age | HNNE | Differences in ‘tone’ and ‘movement’ items between LP and FT |
| Spittle et al. [12] | 129 | 34–36 | 1 | 2 days–2 weeks after birth | HNNE, NNNS, GMA | Lower scores in most of the items for LP population compared to FT |
| Spittle et al. [13] | 197 | 32–36 | 0.95 | Term-age and at 2 years CA | HNNE, NNNS, Bayley Scales | Low scores on HNNE and NNNS were associated with cognitive delay |
| Cheong et al. [14] | NR | 34–36 | NR | NR | Review: newborn neurobehavioral assessments | Suboptimal scores in LP compared with FT |
| Eeles et al. [15] | 196 | 32–36 | 0.9 | Term-age | HNNE, NNNS, GMA | Significant relationship between MRI abnormalities and suboptimal scores on the NNNS and the HNNE, and abnormal GMA |
| Ince et al. [16] | 35 | 34–36 | 0.59 | 48 h of birth | Moro reflex | Significant difference for latency interval in the complete Moro response between LP and FT |
| Romeo et al. [17] | 80 | 34–36 | 0.9 | 48–72 h after birth and at term-age | Neurovisual functions | More mature skills in LP at term-age |
| Mercuri et al. [18] | NR | 34–36 | NR | NR | Review: HNNE and neurovisual functions | LP had more immature responses than FT |
| Authors | No. of Patients | Ga (Weeks) | M:F | Age of Assessment | Tool | Main Results |
|---|---|---|---|---|---|---|
| Romeo et al. [19] | 448 | 35–36 | 1 | 6–9–12 months CA | HINE | HINE score were lower in LT than in FT, especially for tone and reflex items |
| Romeo et al. [20] | 71 | 33–36 | 1.2 | 3–6–9–12 months CA | HINE | Lower global and tone scores in LP than FT |
| Chatzioanidis et al. [21] | 134 | 34–36 | 1.2 | 6–12 months CA | HINE | Differences in scores among the GAs |
| Romeo et al. [1] | NR | 34–36 | NR | NR | Review | LP had a different development during the first year of life |
| Brogna et al. [22] | 574 | 34–36 | NR | 1–3 months CA | GMA | Significant correlation between GMA and neuromotor outcome |
| Bultmann et al. [23] | 23 | 32–36 | 1.5 | Term-age and at 3 months CA | GMA | Substantial changes in most of the parameters between the first and the second measurement |
| Romeo et al. [24] | 484 | 35–37 | 1.03 | 3–6–9–12 months CA | Forward parachute reaction (FPR) | Similar development between LP and FT |
| Authors | No. of Patients | Ga (Weeks) | M:F | Age of Assessment | Tool | Main Results |
|---|---|---|---|---|---|---|
| Hirvonen et al. [25] | 39,932 | 34–36 | NR | First 4 years of life | Neuro-imaging and clinical multidisciplinary evaluation | LP had a higher risk of developing CP compared to FT |
| Zhao et al. [26] | 135,650 | 32–36 | NR | NR | Neuro-imaging and clinical multidisciplinary evaluation | Significant association between small for gestational age and CP in LP |
| Petrini et al. [4] | 8341 | 34–36 | 1.19 | NR | ICD-9 | 3-fold increased risk of CP in LP infants population |
| Teune et al. [8] | 40,416 | 34–36 | NR | NR | Review | LP had a higher risk of developing CP compared to FT |
| Favrais et al. [27] | NR | 34–36 | NR | NR | Review | LP had a higher risk of developing CP compared to FT |
| Moster et al. [28] | 31,169 | 34–36 | 1.22 | NR | National registry | LP had a higher risk of developing CP compared to FT |
| Thygesen et al. [29] | 39,420 | 32–36 | 1.18 | First 5 years of age | National Cerebral Palsy Registry | Increased risk of CP in infants with respiratory distress syndrome |
| Johnson et al. [33] | 638 | 32–36 | 1.16 | 2 years CA | Questionnaire proposed to parents | No difference in incidence of CP between LP and FT |
| Odd et al. [30] | 741 | 32–36 | 1.3 | 7–8 years of age | ALSPAC coordination test | Higher incidence of CP and coordination problems in LP |
| Palumbi et al. [2] | 68 | 34–36 | 1.95 | Mean age: 7.5 years | DSM-5 | Coordination disorder in 19.1% of LP |
| You et al. [9] | 112 | 34–36 | 1.19 | 2–2.5 years | Chinese versions of the Gesell Development Diagnosis scale and a neurological examination | Higher incidence of motor disorder in LP than FT |
| Ramdin et al. [31] | 56 | 34–36 | 0.6 | Mean age: 16.5 months | Bayley scales | No difference between LP and FT |
| Morag et al. [32] | 124 | 34–36 | 1.06 | 6 and 12 months | Alberta Infant Motor Scale and Griffiths Scales | LP had lower scores in all subscales then FT, using CA |
| Potijk et al. [34] | 926 | 32–35 | NR | 2 years | ASQ | Decreasing gestational age was associated with an increased risk of delay in general development, motor and communication skills |
| Hornman et al. [35] | 688 | 32–35 | 1.4 | 4 and 5 years | ASQ | MP and LP showed a trend comparable with FT. The whole preterm group had more emerging motor problems. |
| Benzies et al. [36] | 82 | 34–36 | 1.2 | 4, 8 and 18 months CA | ASQ | LP had lower scores in fine motor domain at 4 months CA, in gross motor and communication domains at 8 months CA, but no significant differences with normative sample at 18 months CA. |
| Ballantyne et al. [37] | 52 | 34–36 | 1.5 | 12 months | ASQ | LP had an increased risk of developmental delay in the gross motor and communication domains. |
| Schonhaut et al. [38] | 165 | 34–36 | 1.1 | 8 and 18 months | Chilean validated version of the ASQ | LP showed increased impairment in fine and gross motor domains |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeo, D.M.; Ricci, M.; Picilli, M.; Foti, B.; Cordaro, G.; Mercuri, E. Early Neurological Assessment and Long-Term Neuromotor Outcomes in Late Preterm Infants: A Critical Review. Medicina 2020, 56, 475. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56090475
Romeo DM, Ricci M, Picilli M, Foti B, Cordaro G, Mercuri E. Early Neurological Assessment and Long-Term Neuromotor Outcomes in Late Preterm Infants: A Critical Review. Medicina. 2020; 56(9):475. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56090475
Chicago/Turabian StyleRomeo, Domenico M., Martina Ricci, Maria Picilli, Benedetta Foti, Giorgia Cordaro, and Eugenio Mercuri. 2020. "Early Neurological Assessment and Long-Term Neuromotor Outcomes in Late Preterm Infants: A Critical Review" Medicina 56, no. 9: 475. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56090475