Full-Endoscopic Lumbar Interbody Fusion for Treating Lumbar Disc Degeneration Involving Disc Height Loss: Technical Report

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
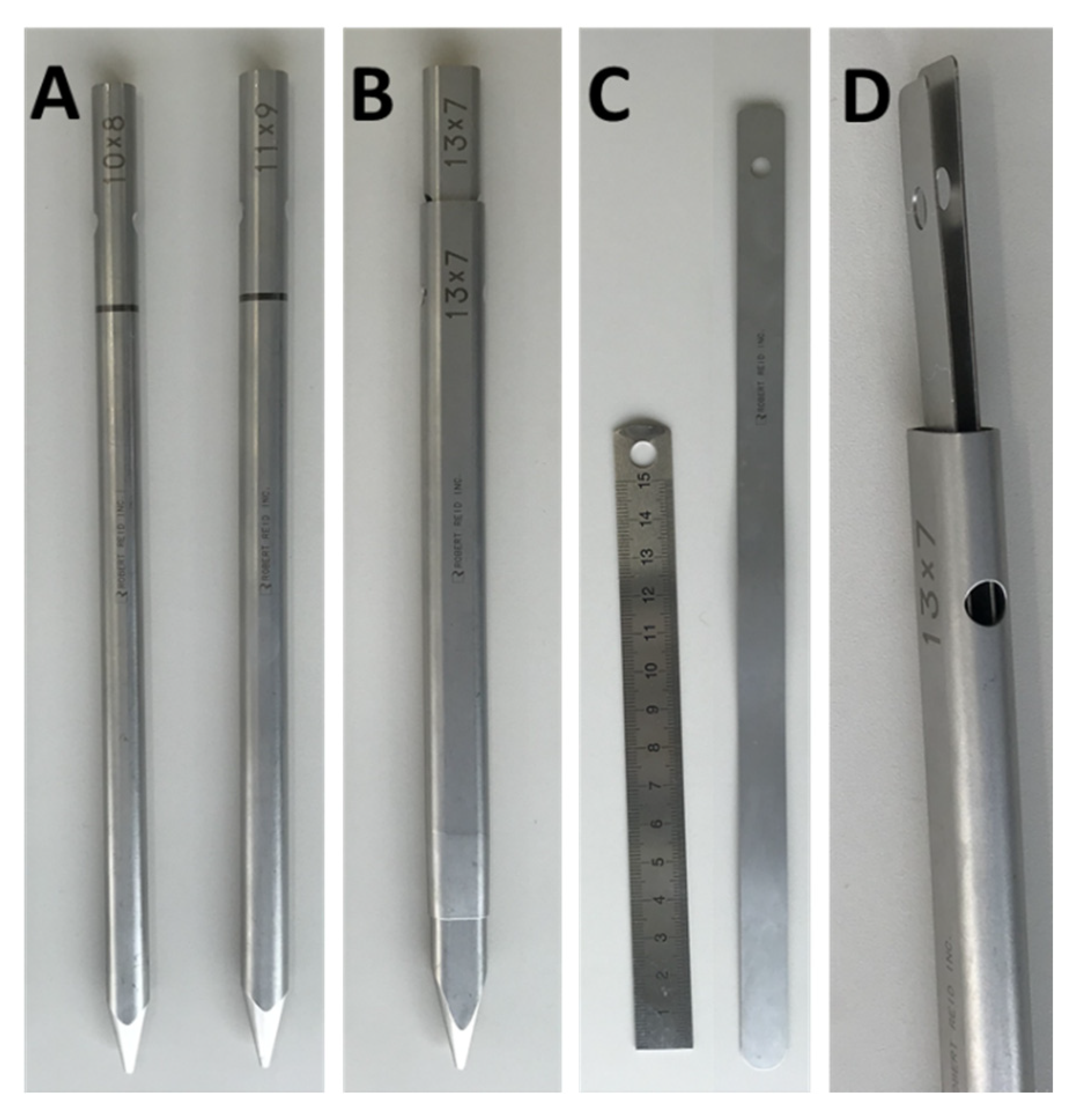
2.2. Surgical Technique
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Standards
References
- Kos, N.; Gradisnik, L.; Velnar, T. A Brief Review of the Degenerative Intervertebral Disc Disease. Med. Arch. 2019, 73, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Doraisamy, R.; Ramaswami, K.; Shanmugam, J.; Subramanian, R.; Sivashankaran, B. Genetic Risk factors for Lumbar Disc Disease. Clin. Anat. 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.F.; Su, G.Y.; Hou, Y.; Chen, S.D.; Zhao, B.D.; He, J.B.; Zhang, J.H.; Chen, Y.J.; Lin, D.K. Mechanics and Biology Interact in Intervertebral Disc Degeneration: A Novel Composite Mouse Model. Calcif. Tissue Int. 2020, 106, 401–414. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.T. Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. Int. J. Mol. Sci. 2020, 21, 2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 2015, 1, 2–18. [Google Scholar]
- Heo, D.H.; Park, C.K. Clinical results of percutaneous biportal endoscopic lumbar interbody fusion with application of enhanced recovery after surgery. Neurosurg. Focus 2019, 46, E18. [Google Scholar] [CrossRef] [Green Version]
- Brusko, G.D.; Wang, M.Y. Endoscopic Lumbar Interbody Fusion. Neurosurg. Clin. N. Am. 2020, 31, 17–24. [Google Scholar] [CrossRef]
- Wang, M.Y.; Grossman, J. Endoscopic minimally invasive transforaminal interbody fusion without general anesthesia: Initial clinical experience with 1-year follow-up. Neurosurg. Focus 2016, 40, E13. [Google Scholar] [CrossRef]
- Ahn, Y.; Youn, M.S.; Heo, D.H. Endoscopic transforaminal lumbar interbody fusion: A comprehensive review. Expert Rev. Med. Devices 2019, 16, 373–380. [Google Scholar] [CrossRef]
- Kyoh, Y. Minimally Invasive Endoscopic-Assisted Lateral Lumbar Interbody Fusion: Technical Report and Preliminary Results. Neurospine 2019, 16, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.E.; Choi, D.J. Biportal Endoscopic Transforaminal Lumbar Interbody Fusion with Arthroscopy. Clin. Orthop. Surg. 2018, 10, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Heo, D.H.; Son, S.K.; Eum, J.H.; Park, C.K. Fully endoscopic lumbar interbody fusion using a percutaneous unilateral biportal endoscopic technique: Technical note and preliminary clinical results. Neurosurg. Focus 2017, 43, E8. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liu, H.; Ao, S.; Zheng, W.; Li, C.; Li, H.; Pan, Y.; Zhang, C.; Zhou, Y. Percutaneous Endoscopic Lumbar Interbody Fusion: Technical Note and Preliminary Clinical Experience with 2-Year Follow-Up. BioMed Res. Int. 2018, 2018, 5806037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Liu, C.; Hai, Y.; Yin, P.; Zhou, L.; Zhang, Y.; Pan, A.; Zhang, Y.; Zhang, L.; Ding, Y.; et al. Percutaneous Endoscopic Transforaminal Lumbar Interbody Fusion for the Treatment of Lumbar Spinal Stenosis: Preliminary Report of Seven Cases with 12-Month Follow-Up. BioMed Res. Int. 2019, 2019, 3091459. [Google Scholar] [CrossRef]
- Kolcun, J.P.G.; Brusko, G.D.; Basil, G.W.; Epstein, R.; Wang, M.Y. Endoscopic transforaminal lumbar interbody fusion without general anesthesia: Operative and clinical outcomes in 100 consecutive patients with a minimum 1-year follow-up. Neurosurg. Focus 2019, 46, E14. [Google Scholar] [CrossRef] [Green Version]
- Jin, M.; Zhang, J.; Shao, H.; Liu, J.; Huang, Y. Percutaneous Transforaminal Endoscopic Lumbar Interbody Fusion for Degenerative Lumbar Diseases: A Consecutive Case Series with Mean 2-Year Follow-Up. Pain Physician 2020, 23, 165–174. [Google Scholar]
- Nagahama, K.; Ito, M.; Abe, Y.; Murota, E.; Hiratsuka, S.; Takahata, M. Early Clinical Results of Percutaneous Endoscopic Transforaminal Lumbar Interbody Fusion: A New Modified Technique for Treating Degenerative Lumbar Spondylolisthesis. Spine Surg. Relat. Res. 2018, 3, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, S.; Taguchi, M. Full Percutaneous Lumbar Interbody Fusion: Technical Note. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2017, 78, 601–606. [Google Scholar]
- Osman, S.G. Endoscopic transforaminal decompression, interbody fusion, and percutaneous pedicle screw implantation of the lumbar spine: A case series report. Int. J. Spine Surg. 2012, 6, 157–166. [Google Scholar] [CrossRef] [Green Version]
- Lener, S.; Wipplinger, C.; Hernandez, R.N.; Hussain, I.; Kirnaz, S.; Navarro-Ramirez, R.; Schmidt, F.A.; Kim, E.; Härtl, R. Defining the MIS-TLIF: A Systematic Review of Techniques and Technologies Used by Surgeons Worldwide. Glob. Spine J. 2020, 10 (Suppl. 2), 151S–167S. [Google Scholar] [CrossRef]
- Brandner, M.E. Normal values of the vertebral body and intervertebral disk index in adults. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1972, 114, 411–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, M.; Kawano, H.; Kitagawa, T.; Iwai, H.; Takano, Y.; Inanami, H.; Koga, H. Preoperative Design for the Posterolateral Approach in Full-Endoscopic Spine Surgery for the Treatment of L5/S1 Lumbar Disc Herniation. Neurospine 2019, 16, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokosuka, J.; Oshima, Y.; Kaneko, T.; Takano, Y.; Inanami, H.; Koga, H. Advantages and disadvantages of posterolateral approach for percutaneous endoscopic lumbar discectomy. J. Spine Surg. 2016, 2, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inanami, H.; Saiki, F.; Oshima, Y. Microendoscope-assisted posterior lumbar interbody fusion: A technical note. J. Spine Surg. 2018, 4, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Basil, G.W.; Wang, M.Y. Technical Considerations of Endoscopic Kambin’s Triangle Lumbar Interbody Fusion. World Neurosurg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tezuka, F.; Sakai, T.; Nishisho, T.; Takata, Y.; Higashino, K.; Takao, S.; Harada, M.; Sairyo, K. Variations in arterial supply to the lower lumbar spine. Eur. Spine J. 2016, 25, 4181–4187. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major Symptom * | Level | Approach * | Cage Size | Operative Time (min) | Hospital Stay (Days) | Follow-Up Periods (m) | NRS Preope | NRS Postope | Previous Operation ** | Interval (m) |
|---|---|---|---|---|---|---|---|---|---|---|
| L L4 radiculopathy | L4/5 | L | 10 × 12 × 30 mm | 106 | 9 | 10 | 6 | 0 | L4/5 FEL | 4 |
| cauda equina syndrome | L4/5 | R | 10 × 12 × 35 mm | 88 | 7 | 9 | 7 | 1 | ||
| cauda equina syndrome | L4/5 | L | 8 × 12 × 35 mm | 91 | 7 | 8 | 8 | 2 | L4/5 MEL | 13 |
| R L4 radiculopathy | L4/5 | R | 8 × 12 × 35 mm | 114 | 8 | 8 | 6 | 1 | L4/5 FED | 6 |
| R L5 radiculopathy | L5/S1 | R | 8 × 12 × 30 mm | 151 | 8 | 7 | 8 | 0 | L5/S1 FEL | 9 |
| cauda equina syndrome | L3/4 | R | 8 × 12 × 35 mm | 80 | 7 | 6 | 5 | 5 | L4/5-L5/S1 PLF | 18 |
| L L5 radiculopathy | L5/S1 | L | 8 × 12 × 35 mm | 82 | 7 | 6 | 8 | 0 | L5/S1 Open discectomy | 13 |
| R L4 radiculopathy | L4/5 | R | 8 × 12 × 35 mm | 140 | 5 | 5 | 10 | 0 | L3/4/5 MEL | 62 |
| L L4 radiculopathy | L3/4 | L | 8 × 12 × 35 mm | 73 | 7 | 5 | 7 | 0 | L3/4 MEL | 10 |
| R L5 radiculopathy | L5/S1 | R | 8 × 12 × 30 mm | 131 | 6 | 2 | 4 | 0 | L5/S1 FEL | 13 |
| L L5 radiculopathy | L5/S1 | L | 8 × 12 × 35 mm | 97 | 6 | 2 | 8 | 0 | L5/S1 FEL | 8 |
| low back pain | L3/4 | L | 8 × 12 × 35 mm | 160 | 15 | 6 | 1 | 5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harakuni, T.; Iwai, H.; Oshima, Y.; Inoue, H.; Kitagawa, T.; Inanami, H.; Koga, H. Full-Endoscopic Lumbar Interbody Fusion for Treating Lumbar Disc Degeneration Involving Disc Height Loss: Technical Report. Medicina 2020, 56, 478. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56090478
Harakuni T, Iwai H, Oshima Y, Inoue H, Kitagawa T, Inanami H, Koga H. Full-Endoscopic Lumbar Interbody Fusion for Treating Lumbar Disc Degeneration Involving Disc Height Loss: Technical Report. Medicina. 2020; 56(9):478. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56090478
Chicago/Turabian StyleHarakuni, Tsuyoshi, Hiroki Iwai, Yasushi Oshima, Hirokazu Inoue, Tomoaki Kitagawa, Hirohiko Inanami, and Hisashi Koga. 2020. "Full-Endoscopic Lumbar Interbody Fusion for Treating Lumbar Disc Degeneration Involving Disc Height Loss: Technical Report" Medicina 56, no. 9: 478. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56090478