
Maternal and Fetal Outcomes after Prior Mid-Trimester Uterine Rupture: A Systematic Review with Our Experience

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Literature Review Approach
2.2. Eligibility Criteria, Information Sources, and Search Strategy
2.3. Study Selection
2.4. Data Extraction
3. Results
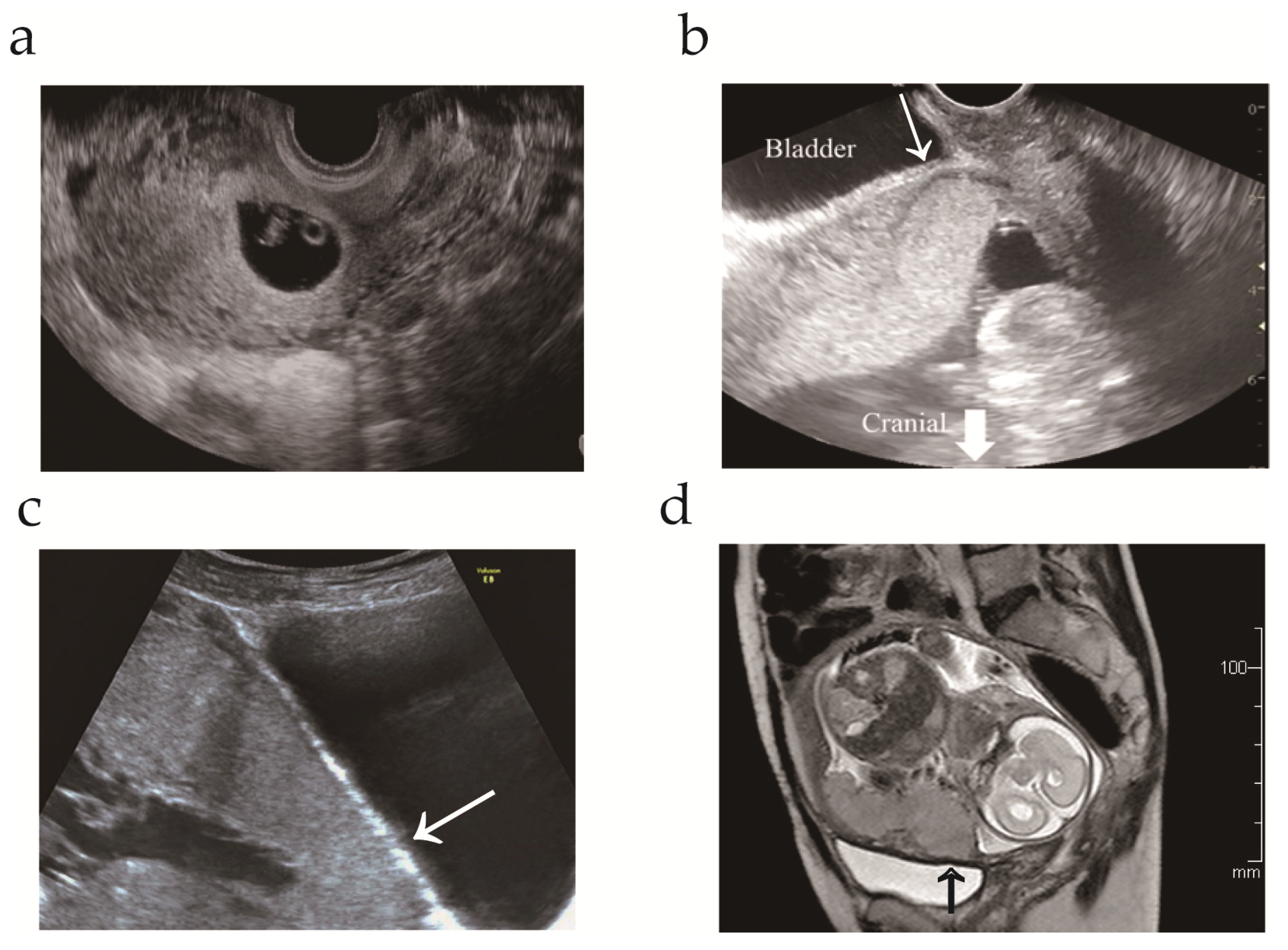
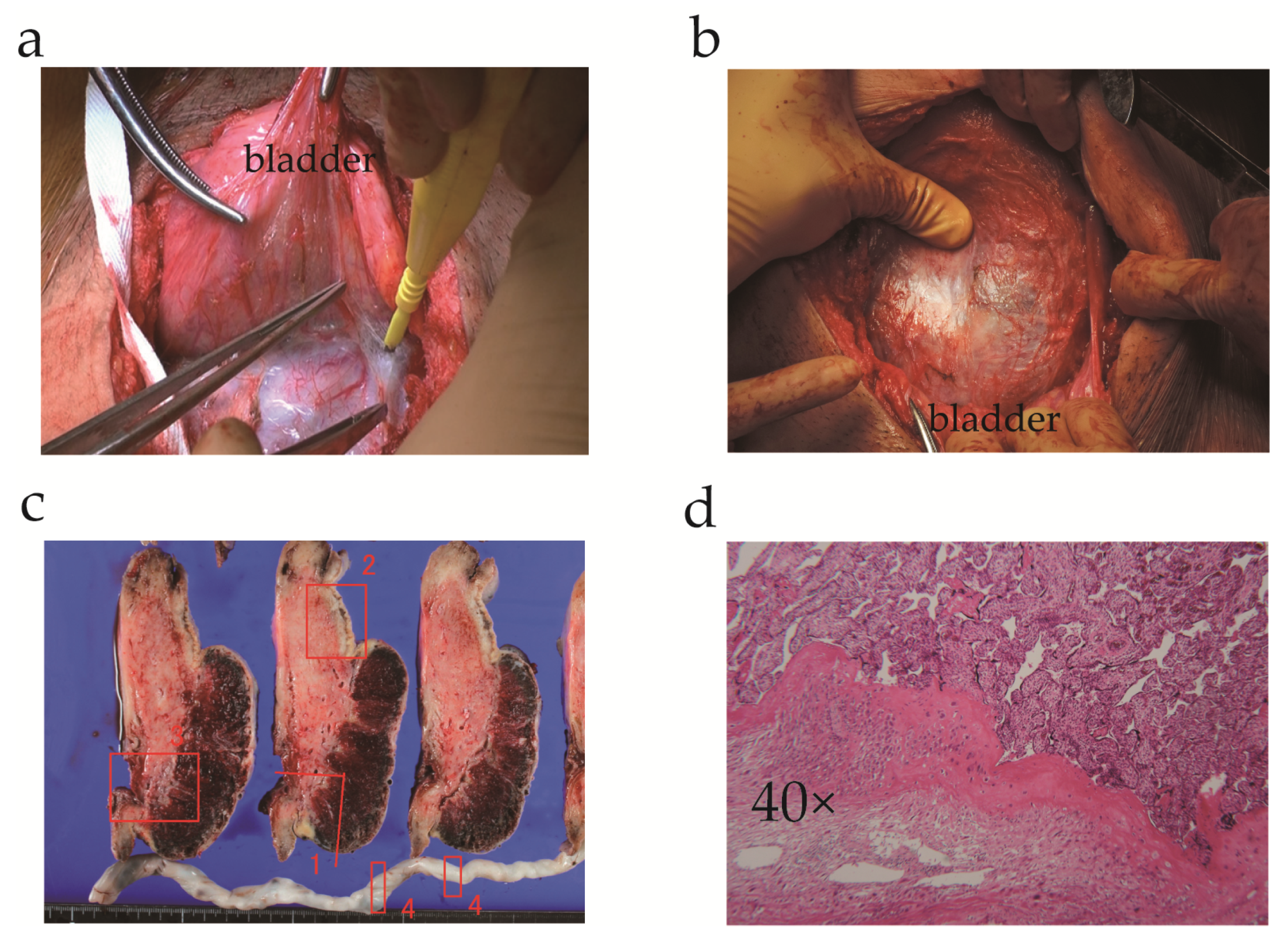
3.1. Case Presentation
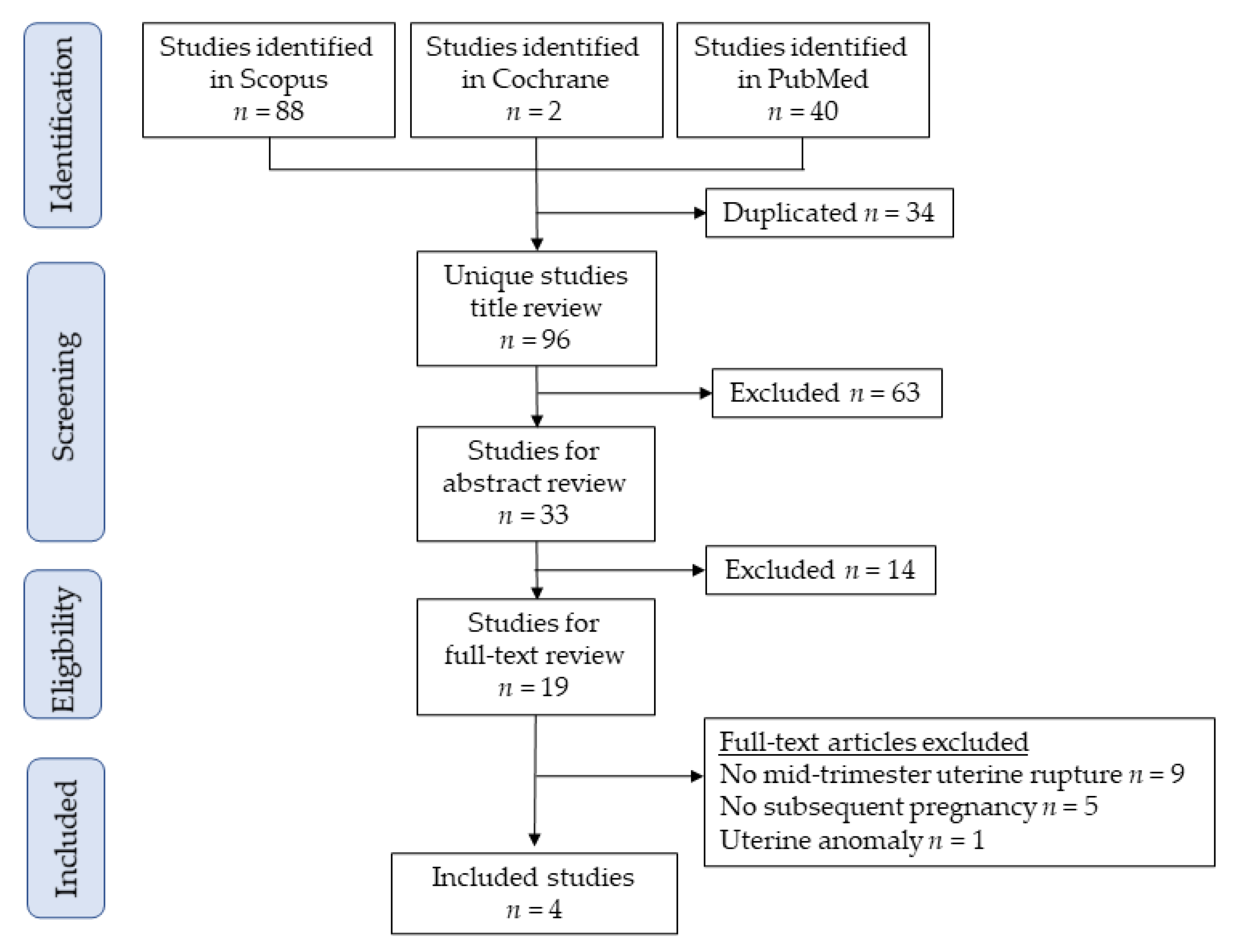
3.2. Study Selection for Systematic Review
3.3. Study Characteristics
3.4. Maternal and Fetal Outcomes
4. Discussion
4.1. Key Findings
4.2. Strengths and Limitations
4.3. Comparison with Existing Literature
4.3.1. Maternal and Fetal Outcomes after Uterine Rupture
4.3.2. Maternal and Fetal Outcomes after Mid-Trimester Uterine Rupture
4.3.3. Timing of Delivery after Mid-Trimester Uterine Rupture
4.3.4. Repair of Uterine Rupture
4.4. Discussion of Our Case
4.5. Conclusions and Implications
4.5.1. Implications for Practice
4.5.2. Implications for Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al Qahtani, N. Fertility after complete uterine rupture. Curr. Opin. Obstet. Gynecol. 2013, 25, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M. Abnormal Placentation: Placenta Previa, Vasa Previa, and Placenta Accreta. Obstet. Gynecol. 2015, 126, 654–668. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Say, L.; Gülmezoglu, A.M. SYSTEMATIC REVIEW: WHO systematic review of maternal mortality and morbidity: The prevalence of uterine rupture. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 1221–1228. [Google Scholar] [CrossRef]
- Cunningham, F.G.; Bangdiwala, S.I.; Brown, S.S.; Dean, T.M.; Frederiksen, M.; Hogue, C.R.; Zimmet, S.C. National Institutes of Health Consensus Development conference statement: Vaginal birth after cesarean: New insights March 8–10, 2010. Obstet Gynecol. 2010, 115, 1279–1295. [Google Scholar] [CrossRef]
- Tinelli, A.; Kosmas, I.P.; Carugno, J.; Carp, H.; Malvasi, A.; Cohen, S.B.; Laganà, A.S.; Angelini, M.; Casadio, P.; Chayo, J.; et al. Uterine rupture during pregnancy: The URIDA (uterine rupture international data acquisition) study. Int. J. Gynecol. Obstet. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.S. Pregnancy Outcomes in Patients with Prior Uterine Rupture or Dehiscence: A 5-Year Update. Obstet. Gynecol. 2020, 135, 211–212. [Google Scholar] [CrossRef]
- Fox, N.S.; Gerber, R.S.; Mourad, M.; Saltzman, D.H.; Klauser, C.K.; Gupta, S.; Rebarber, A. Pregnancy Outcomes in Patients With Prior Uterine Rupture or Dehiscence. Obstet. Gynecol. 2014, 123, 785–789. [Google Scholar] [CrossRef] [Green Version]
- Usta, I.M.; Hamdi, M.A.; Abu Musa, A.A.; Nassar, A.H. Pregnancy outcome in patients with previous uterine rupture. Acta Obstet. Gynecol. Scand. 2007, 86, 172–176. [Google Scholar] [CrossRef]
- Eshkoli, T.; Weintraub, A.Y.; Baron, J.; Sheiner, E. The significance of a uterine rupture in subsequent births. Arch. Gynecol. Obstet. 2015, 292, 799–803. [Google Scholar] [CrossRef]
- Deka, D.; Bahadur, A.; Dadhwal, V.; Gurunath, S.; Vaid, A. Successful outcome in pregnancy complicated by prior uterine rupture: A report of two cases. Arch. Gynecol. Obstet. 2010, 283, 45–48. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. What is the placenta? Am. J. Obstet.Gynecol. 2015, 213, S6–e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzaki, S.; Mandelbaum, R.S.; Sangara, R.N.; McCarthy, L.E.; Vestal, N.L.; Klar, M.; Matsushima, K.; Amaya, R.; Ouzounian, J.G.; Matsuo, K. Trends, characteristics, and outcomes of placenta accreta spectrum: A national study in the United States. Am. J. Obstet. Gynecol. 2021, 225, 534.e1–534.e38. [Google Scholar] [CrossRef]
- Jauniaux, E.; Hussein, A.M.; Elbarmelgy, R.M.; Elbarmelgy, R.A.; Burton, G.J. Failure of placental detachment in accreta placentation is associated with excessive fibrinoid deposition at the utero-placental interface. Am. J. Obstet. Gynecol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Erfani, H.; Salmanian, B.; Fox, K.A.; Coburn, M.; Meshinchiasl, N.; Shamshirsaz, A.A.; Kopkin, R.; Gogia, S.; Patel, K.; Jackson, J.; et al. Urologic morbidity associated with placenta accreta spectrum surgeries: Single-center experience with a multidisciplinary team. Am. J. Obstet. Gynecol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Hussein, A.M.; Zosmer, N.; Elbarmelgy, R.M.; Elbarmelgy, R.A.; Shaikh, H.; Burton, G.J. A new methodologic approach for clinico-pathologic correlations in invasive placenta previa accreta. Am. J. Obstet. Gynecol. 2020, 222, 379-e1–379-e11. [Google Scholar] [CrossRef] [PubMed]
- Sawada, M.; Kakigano, A.; Matsuzaki, S.; Takiuchi, T.; Mimura, K.; Kumasawa, K.; Endo, M.; Ueda, Y.; Yoshino, K.; Kimura, T. Obstetric outcome in patients with a unicornuate uterus after laparoscopic resection of a rudimentary horn. J. Obstet. Gynaecol. Res. 2018, 44, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Cahill, A.G.; Beigi, R.; Heine, R.P.; Silver, R.M.; Wax, J.R. Placenta Accreta Spectrum. Am. J. Obstet. Gynecol. 2018, 219, B2–B16. [Google Scholar] [CrossRef] [Green Version]
- Sentilhes, L.; Goffinet, F.; Kayem, G. Management of placenta accreta. Acta. Obstet. Gynecol. Scandinavica 2013, 92, 1125–1134. [Google Scholar] [CrossRef] [Green Version]
- Licon, E.; Matsuzaki, S.; Opara, K.N.; Ng, A.J.; Bender, N.M.; Grubbs, B.H.; Lee, R.H.; Ouzounian, J.G.; Pham, H.Q.; Brunette, L.L.; et al. Implementation of multidisciplinary practice change to improve outcomes for women with placenta accreta spectrum. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 194–196. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Matsuzaki, S.; Ueda, Y.; Tanaka, Y.; Kakuda, M.; Kanagawa, T.; Kimura, T. A Case Report and Literature Review of Midtrimester Termination of Pregnancy Complicated by Placenta Previa and Placenta Accreta. Am. J. Perinatol. Rep. 2014, 5, e6–e11. [Google Scholar] [CrossRef] [Green Version]
- Matsuzaki, S.; Nagase, Y.; Ueda, Y.; Kakuda, M.; Maeda, M.; Matsuzaki, S.; Kamiura, S. Placenta Previa Complicated with Endometriosis: Contemporary Clinical Management, Molecular Mechanisms, and Future Research Opportunities. Biomedicines 2021, 9, 1536. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Endo, M.; Ueda, Y.; Mimura, K.; Kakigano, A.; Egawa-Takata, T.; Kumasawa, K.; Yoshino, K.; Kimura, T. A case of acute Sheehan’s syndrome and literature review: A rare but life-threatening complication of postpartum hemorrhage. BMC Pregnancy Childbirth 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Obstetricians and Gynecologists, Society for Maternal-Fetal Medicine. Obstetric Care Consensus No. 7: Placenta Accreta Spectrum. Obstet. Gynecol. 2018, 132, e259–e275. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.R.M.; Alfirevic, Z.; Bhide, A.G.; Belfort, M.A.; Burton, G.J.; Collins, S.L.; Dornan, S.; Jurkovic, D.; Kayem, G.; Silver, R.; et al. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. BJOG Int. J. Obstet. Gynaecol. 2019, 126, e1–e48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, J.M.; Barton, J.R.; Donaldson, E.S. The management of placenta percreta: Conservative and operative strategies. Am. J. Obstet.Gynecol. 1996, 175, 1632–1638. [Google Scholar] [CrossRef]
- Collins, S.L.; Alemdar, B.; van Beekhuizen, H.J.; Bertholdt, C.; Braun, T.; Calda, P.; Delorme, P.; Duvekot, J.J.; Gronbeck, L.; Kayem, G.; et al. Evidence-based guidelines for the management of abnormally invasive placenta: Recommendations from the International Society for Abnormally Invasive Placenta. Am. J. Obstet. Gynecol. 2019, 220, 511–526. [Google Scholar] [CrossRef] [Green Version]
- Matsuzaki, S.; Jitsumori, M.; Hara, T.; Matsuzaki, S.; Nakagawa, S.; Miyake, T.; Takiuchi, T.; Kakigano, A.; Kobayashi, E.; Tomimatsu, T.; et al. Systematic review on the needle and suture types for uterine compression sutures: A literature review. BMC Surg. 2019, 19, 1–6. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Matsuzaki, S.; Chang, E.J.; Yasukawa, M.; Roman, L.D.; Matsuo, K. Surgical and oncologic outcomes of hyperthermic intraperitoneal chemotherapy for uterine leiomyosarcoma: A systematic review of literature. Gynecol. Oncol. 2021, 161, 70–77. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Nagase, Y.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Lee, M.; Matsuzaki, S.; Ueda, Y.; Tomimatsu, T.; Endo, M.; et al. Antenatal diagnosis of placenta accreta spectrum after in vitro fertilization-embryo transfer: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Kanao, S.; Fukuda, H.; Miyamoto, M.; Marumoto, E.; Furuya, K.; Nishiyama, R.; Ohyagi, C.; Ogawa, H.; Fukuda, A. Spontaneous Uterine Rupture at 15 Weeks’ Gestation in a Patient with a History of Cesarean Delivery after Removal of Shirodkar Cerclage. Am. J. Perinatol. Rep. 2013, 4, 001–004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzaki, S.; Yoshino, K.; Mimura, K.; Kanagawa, T.; Kimura, T. Cesarean delivery via a transverse uterine fundal incision for the successful management of a low-lying placenta and aplastic anemia. Clin. Exp. Obstet. Gynecol. 2016, 43, 262–264. [Google Scholar] [PubMed]
- Matsuzaki, S.; Yoshino, K.; Kumasawa, K.; Satou, N.; Mimura, K.; Kanagawa, T.; Ueda, Y.; Kimura, T. Placenta percreta managed by transverse uterine fundal incision with retrograde cesarean hysterectomy: A novel surgical approach. Clin. Case Rep. 2014, 2, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Bouzari, Z.; Mohammadnataj, M.; Ghanbarpour, A. Successful Pregnancy and Delivery after Uterine Rupture in Previous Pregnancy: A Case Report. J. Babol. Univ. Med. Sci. 2019, 21, 345–348. [Google Scholar]
- Champion de Crespigny, C.; Shetty, P.; Inglis, E.; Anpalagan, A.; Chatterjee, U.; Alahakoon, T.I. Successful pregnancy with fundal placenta percreta replacing the myometrial defect from previous uterine rupture. J. Obstet. Gynaecol. 2019, 39, 853–855. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Lee, M.; Nagase, Y.; Jitsumori, M.; Matsuzaki, S.; Maeda, M.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Ueda, Y.; et al. A systematic review and meta-analysis of obstetric and maternal outcomes after prior uterine artery embolization. Sci. Rep. 2021, 11, 1–13. [Google Scholar]
- Cunningham, K.; Anwar, A.; Lindow, S. The recurrence risk of placenta accreta following uterine conserving management. J. Neonatal-Perinatal Med. 2016, 8, 293–296. [Google Scholar] [CrossRef]
- Sharon, N.; Maymon, R.; Pekar-Zlotin, M.; Betser, M.; Melcer, Y. Midgestational pre-labor spontaneous uterine rupture: A SYSTEMATIC review. J. Matern. Neonatal Med. 2021, 2021, 1–6. [Google Scholar] [CrossRef]
- Guise, J.M.; Denman, M.A.; Emeis, C.; Marshall, N.; Walker, M.; Fu, R.; Janik, R.; Nygren, P.; Eden, K.B.; McDonagh, M. Vaginal birth after cesarean: New insights on maternal and neonatal outcomes. Obstet. Gynecol. 2010, 115, 1267–1278. [Google Scholar] [CrossRef]
- Di Spiezio Sardo, A.; Saccone, G.; McCurdy, R.; Bujold, E.; Bifulco, G.; Berghella, V. Risk of Cesarean scar defect following single- vs double-layer uterine closure: Systematic review and meta-analysis of randomized controlled trials. Ultrasound Obstet. Gynecol. 2017, 50, 578–583. [Google Scholar] [CrossRef] [Green Version]
- Palacios-Jaraquemada, J.; Fiorillo, Á.; Von Petery, F.; Colaci, D.; Leguizamón, G. Uterine repair and successful pregnancy after myometrial and placental rupture with massive haemoperitoneum. BJOG Int. J. Obstet. Gynaecol. 2009, 116, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Al-Zirqi, I.; Vangen, S. Prelabour uterine rupture: Characteristics and outcomes. BJOG: Int. J. Obstet. Gynaecol. 2020, 127, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Gibbins, K.J.; Weber, T.; Holmgren, C.M.; Porter, T.F.; Varner, M.W.; Manuck, T.A. Maternal and fetal morbidity associated with uterine rupture of the unscarred uterus. Am. J. Obstet. Gynecol. 2015, 213, 382.e1–382.e6. [Google Scholar] [CrossRef] [PubMed]
- Samuels, T.A.; Awonuga, A. Second-trimester rudimentary uterine horn pregnancy: Rupture after labor induction with misoprostol. Obstet. Gynecol. 2005, 106, 1160–1162. [Google Scholar] [CrossRef]
- Ozdemir, I.; Yucel, N.; Yucel, O. Rupture of the pregnant uterus: A 9-year review. Arch. Gynecol. Obstet. 2005, 272, 229–231. [Google Scholar] [CrossRef]
- Ridgeway, J.J.; Weyrich, D.L.; Benedetti, T.J. Fetal Heart Rate Changes Associated With Uterine Rupture. Obstet. Gynecol. 2004, 103, 506–512. [Google Scholar] [CrossRef]
- Kakigano, A.; Matsuzaki, S.; Kinose, Y.; Kimura, T.; Kimura, T. Stinging abdominal pain at 32 gestational weeks with prior classical uterine incision: Careful assessment or emergency cesarean delivery? Clin. Case Rep. 2021, 9, e04344. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Timing | Site | No. | Cause | GA | Maternal Outcome | Site of PAS | Fetal Outcome | Repair |
|---|---|---|---|---|---|---|---|---|---|---|
| Present case | 2021 | 15 | CD scar | 1 | CD | 34 | Increta | CD scar | No comp | Double-layer |
| Bouzari [34] | 2019 | 26 | Fundus | 1 | Myomectomy | - | No comp | - | No comp | - |
| Crespigny [35] | 2019 | 23 | Fundus † | 2 | Spontaneous | 30 | CD | - | - | * |
| 23 | Rupture | - | CP | Three-layer | ||||||
| 28 | Percreta | Fundus | No comp | |||||||
| Deka [10] | 2011 | 16 | Fundus | 1 | Spontaneous | 32 | Percreta | Fundus | No comp | Three-layer |
| Usta [8] | 2007 | 17 | Transverse | 1 | - | 38 | No comp | - | No comp | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuzaki, S.; Takiuchi, T.; Kanagawa, T.; Matsuzaki, S.; Lee, M.; Maeda, M.; Endo, M.; Kimura, T. Maternal and Fetal Outcomes after Prior Mid-Trimester Uterine Rupture: A Systematic Review with Our Experience. Medicina 2021, 57, 1294. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121294
Matsuzaki S, Takiuchi T, Kanagawa T, Matsuzaki S, Lee M, Maeda M, Endo M, Kimura T. Maternal and Fetal Outcomes after Prior Mid-Trimester Uterine Rupture: A Systematic Review with Our Experience. Medicina. 2021; 57(12):1294. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121294
Chicago/Turabian StyleMatsuzaki, Shinya, Tsuyoshi Takiuchi, Takeshi Kanagawa, Satoko Matsuzaki, Misooja Lee, Michihide Maeda, Masayuki Endo, and Tadashi Kimura. 2021. "Maternal and Fetal Outcomes after Prior Mid-Trimester Uterine Rupture: A Systematic Review with Our Experience" Medicina 57, no. 12: 1294. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121294