
Medial Calcar Comminution and Intramedullary Nail Failure in Unstable Geriatric Trochanteric Hip Fractures


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Settings
2.1.1. Inclusion
2.1.2. Exclusion
2.2. Data Collection
2.3. Outcomes
2.4. Technical Factors of Fixation
2.5. Sample Size
2.6. Statistical Analysis
3. Results
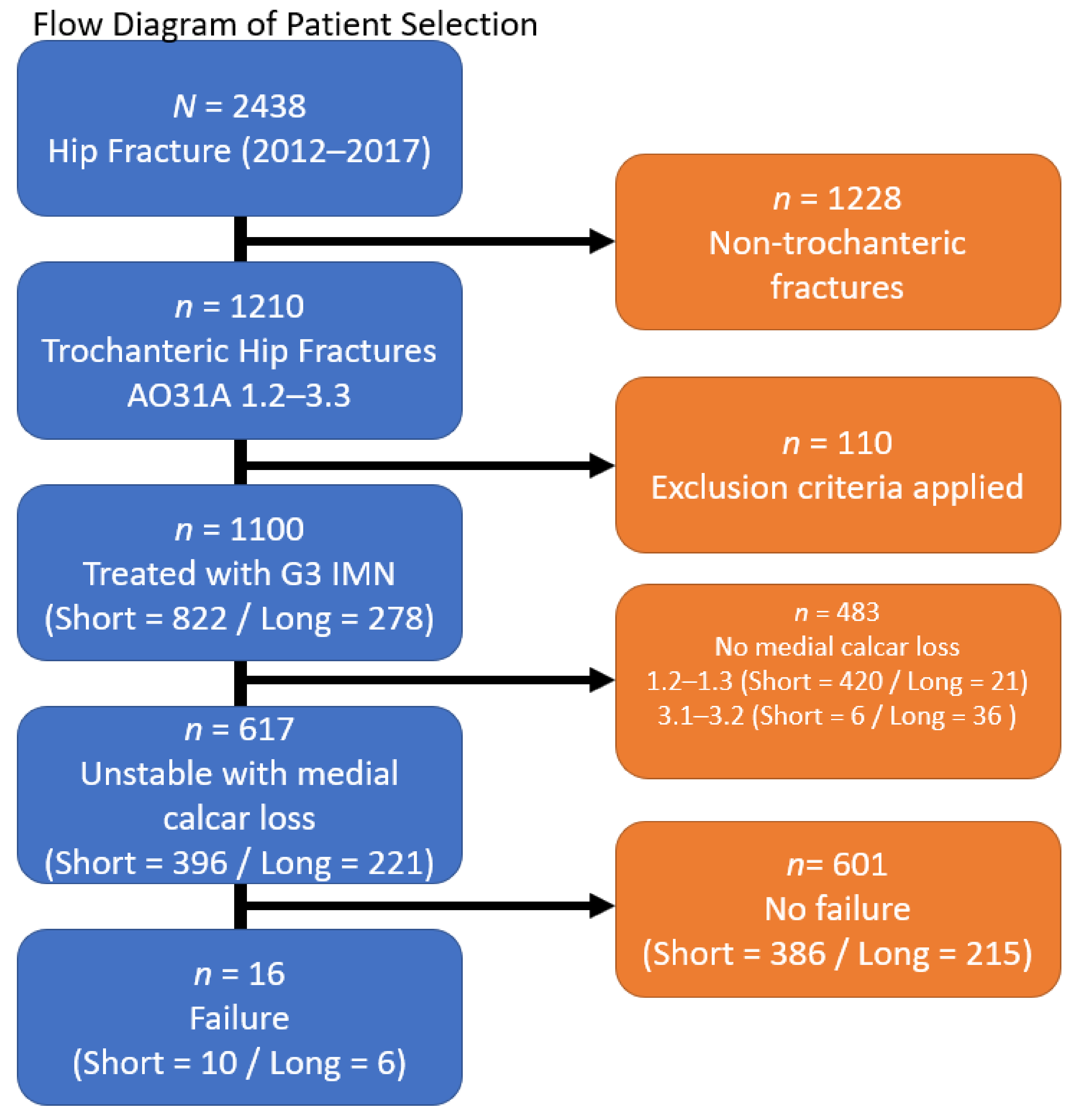
3.1. Patient Selection & Demographics
3.2. Nail Length & Medial Calcar Loss
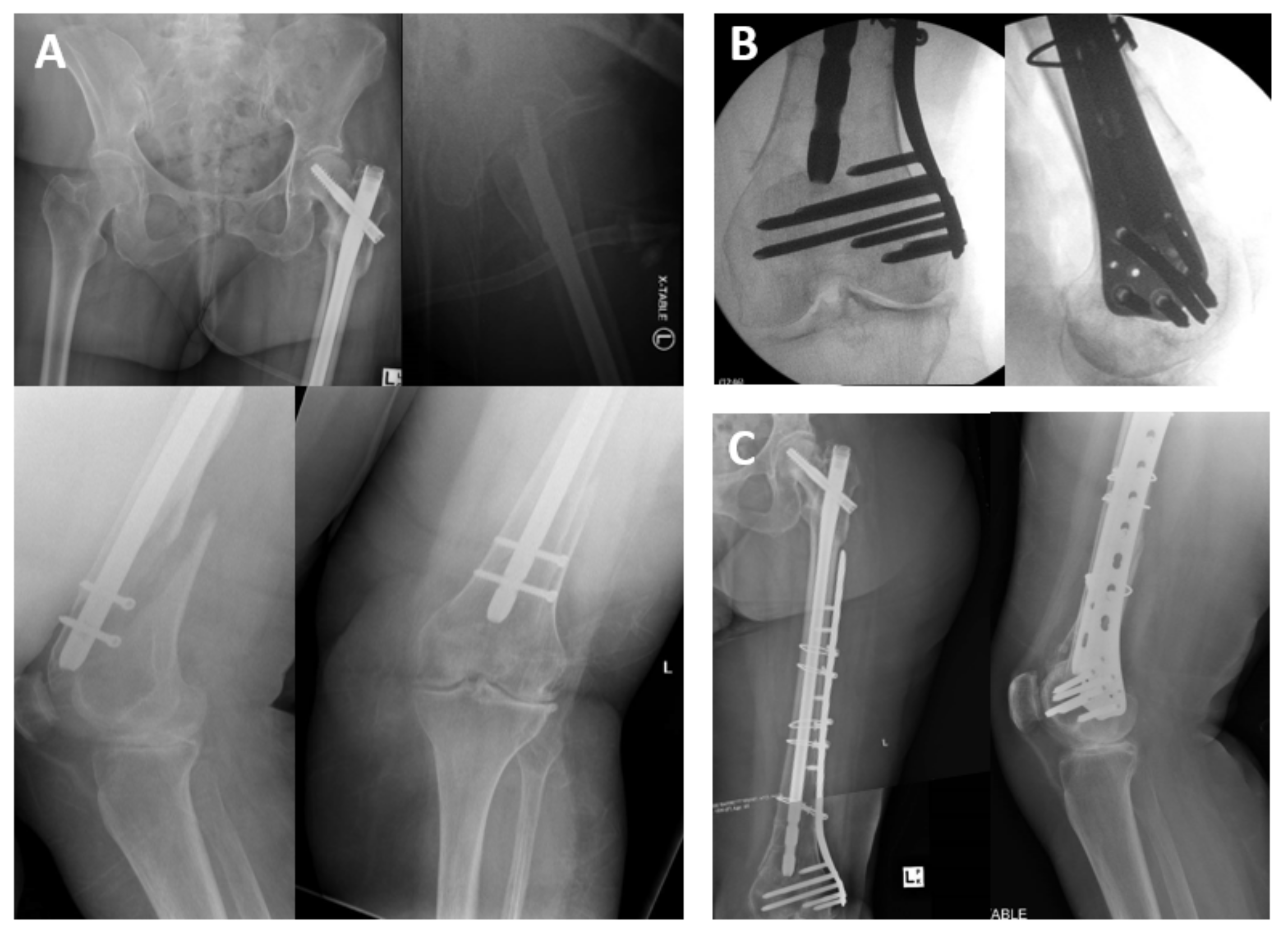
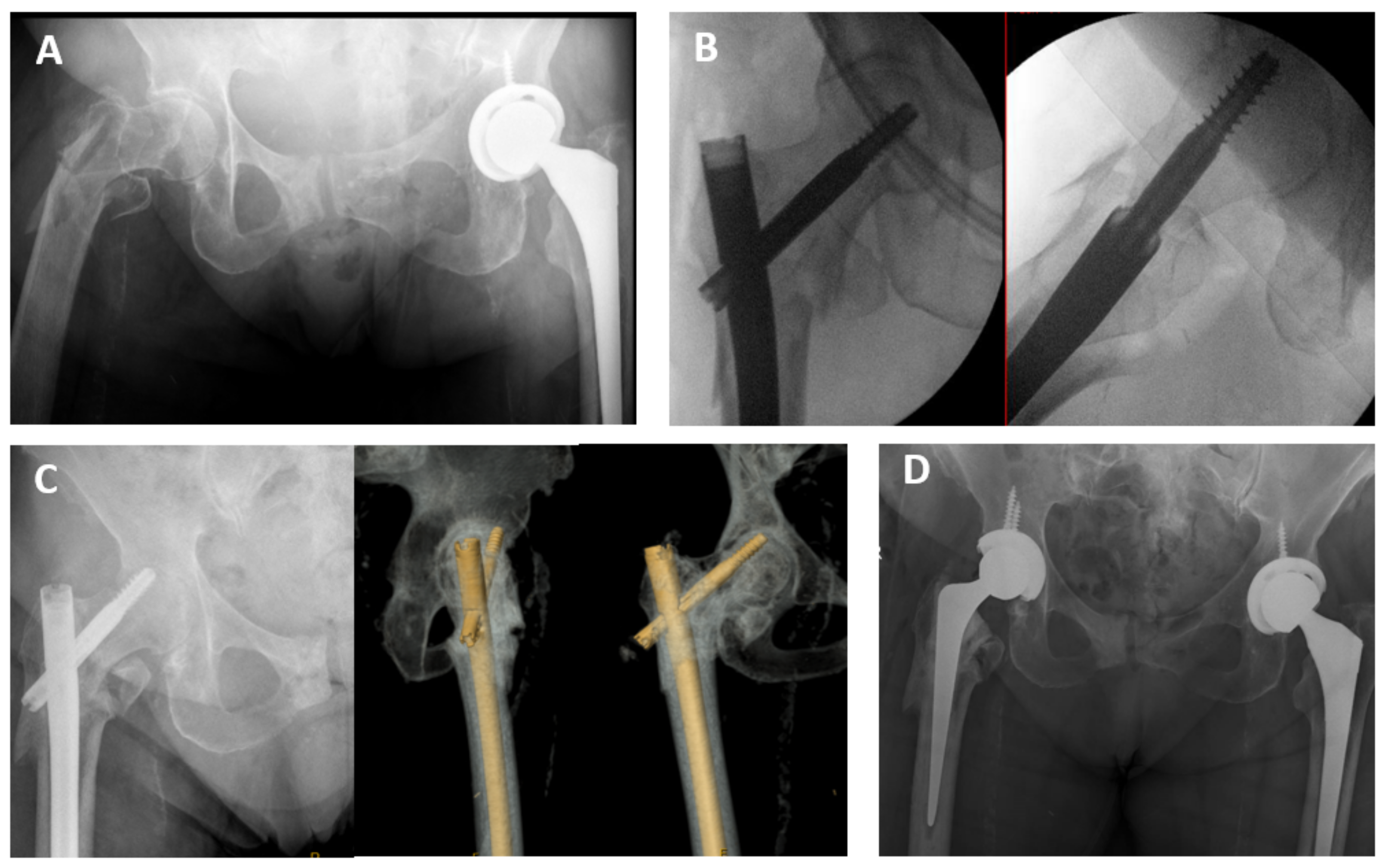
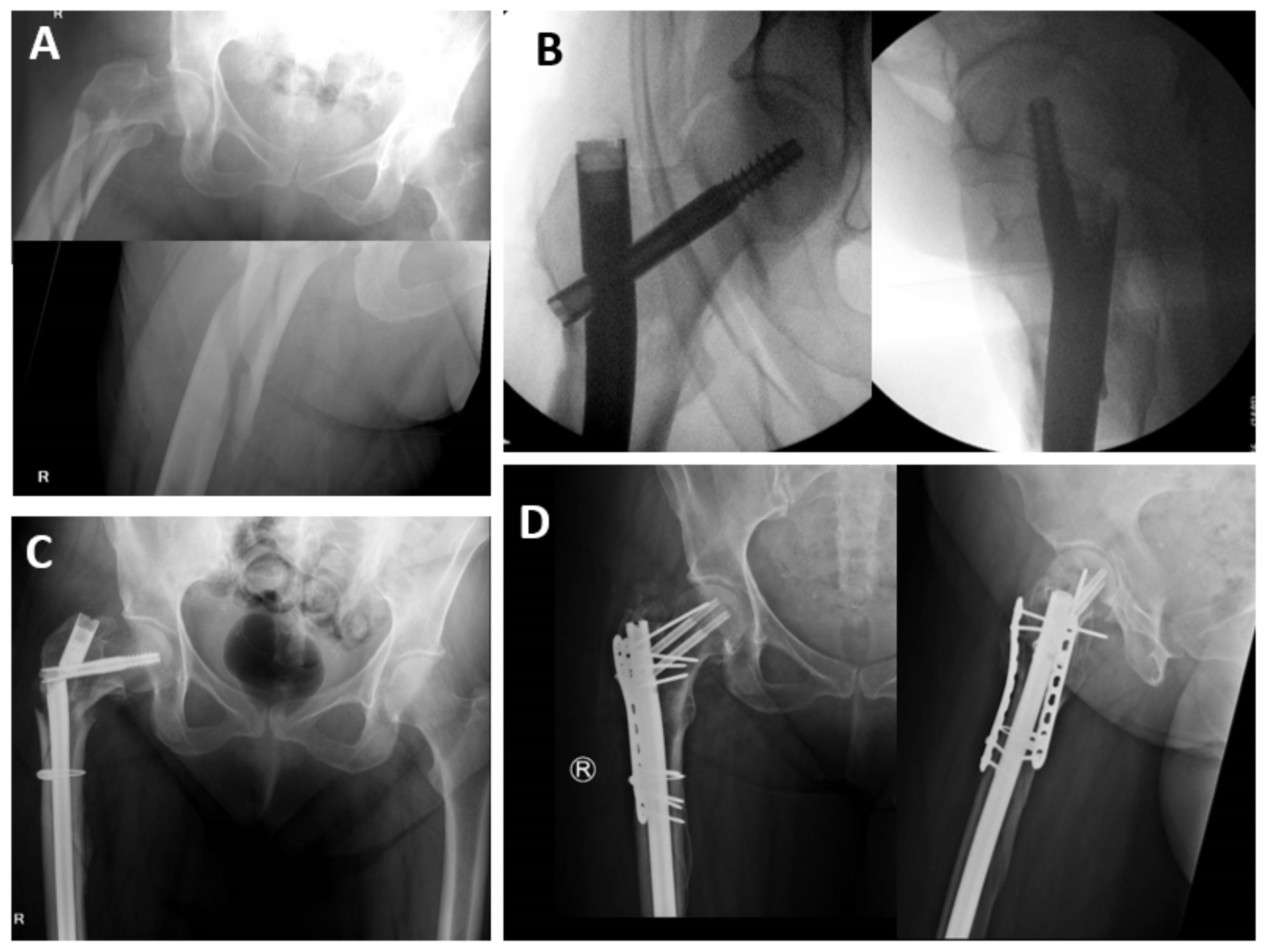
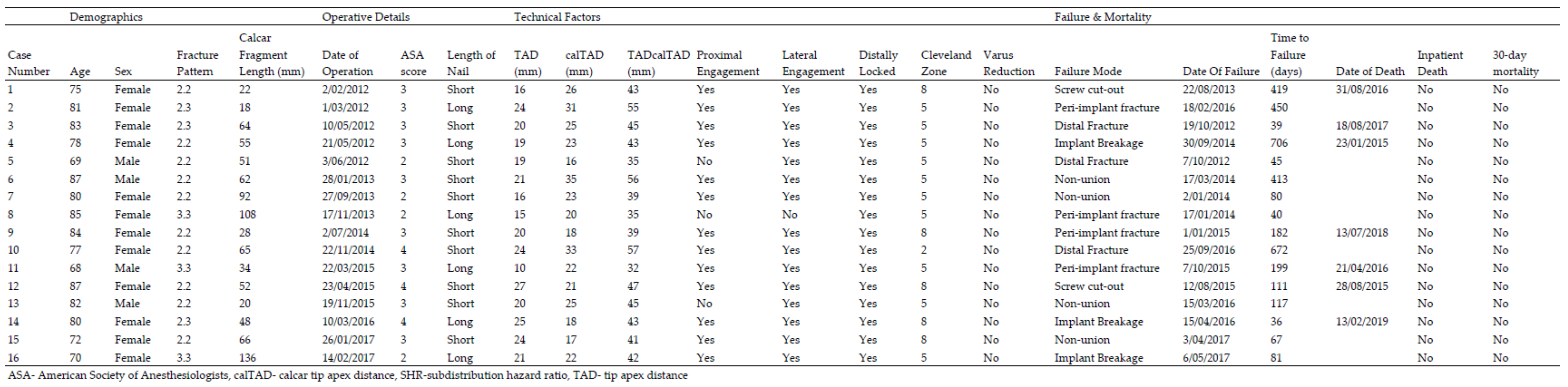
3.3. Modes of Failure
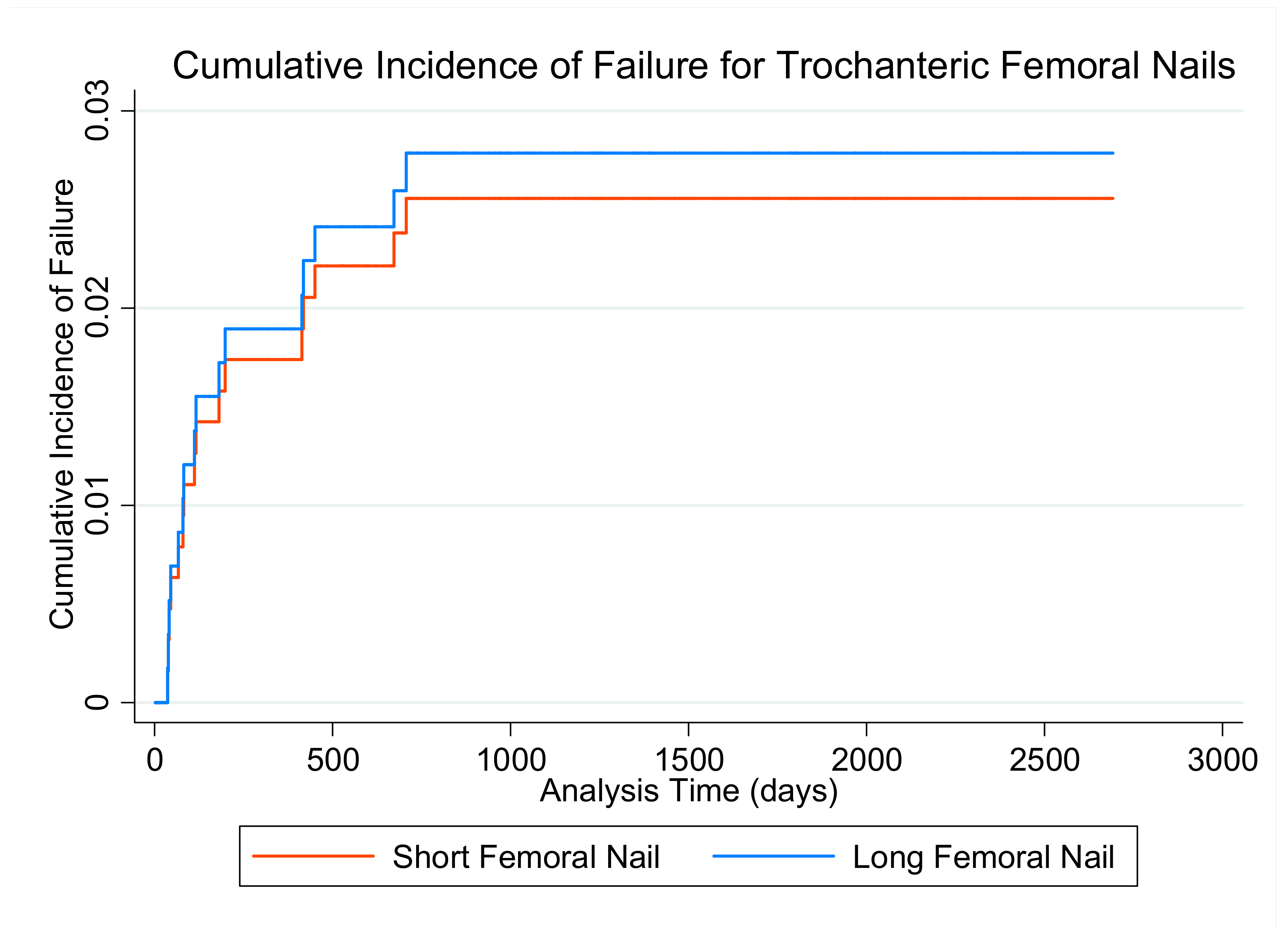
3.4. Failure
4. Discussion
4.1. Rates of Failure
4.2. Nail Length
4.3. Medial Calcar
4.4. Limitations
4.5. Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics & Outcomes | Total (n = 617) | Short (n = 396) | Long (n = 221) |
|---|---|---|---|
| Age (years; mean, SD) | 84.4 (±7.4) | 84.8 (±7.3) | 83.6 (±7.4) |
| Gender (Female; n, %) | 430 (70%) | 282 (71%) | 148 (67%) |
| ASA (score; mean, SD) | |||
| 1 | 7 (0.9%) | 5 (1.3%) | 2 (0.9%) |
| 2 | 92 (15%) | 56 (14%) | 36 (16%) |
| 3 | 360 (59%) | 236 (59%) | 124 (57%) |
| 4 | 154 (25%) | 97 (25%) | 57 (26%) |
| 5 | 1 (0.2%) | 1 (0.3%) | 0 (0%) |
| Unstable Patterns (type; n, %) | |||
| 2.2 | 452 (73%) | 342 (76%) | 110 (50%) |
| 2.3 | 77 (13%) | 47 (12%) | 30 (14%) |
| 3.3 | 88 (14%) | 7 (1.8%) | 81 (37%) |
| Medial Calcar Loss (mm; mean, SD) | 48 (±22) | 43 (±16) | 57 (±27) |
| Transfusion (Y; n, %) | 237 (38%) | 140 (35%) | 97 (43%) |
| Number of units transfused (median, Q1-Q3) | 2 (2–3) | 2 (2–3) | 2 (2–3) |
| Failed Osteosynthesis (n, %) | 16 (2.6%) | 10 (2.5%) | 6 (2.7%) |
| Inpatient death (n, %) | 39 (6.2%) | 24 (6.1%) | 15 (6.8%) |
| 30-day Mortality (n, %) | 75 (12.2%) | 45 (11.4%) | 30 (13.6%) |
Appendix C

Appendix D
| Variables | Fail (n = 16) | Survive (n = 601) | SHR | CI 95% | p Value |
|---|---|---|---|---|---|
| Demographics & Fracture Morphology | |||||
| Age (years; mean, SD) | 78.6 (6.3) | 84.5 (7.4) | 0.90 | (0.86–0.95) | <0.001 |
| Sex (female; n, %) | 12 (75%) | 418 (70%) | 0.77 | (0.25–2.38) | 0.645 |
| Ischaemic Heart Disease (n, %) | 4 (25%) | 165 (27%) | 0.71 | (0.15–3.31) | 0.661 |
| Chronic Renal Failure (n, %) | 3 (19%) | 81 (13%) | 0.81 | (0.25–2.64) | 0.728 |
| Diabetes Mellitus (n, %) | 4 (25%) | 108 (18%) | 0.98 | (0.33–2.88) | 0.968 |
| Current Tobacco Use (n, %) | 0 (0.0%) | 23 (3.8%) | - | ||
| Former Tobacco Use (n, %) | 2 (13%) | 101 (17%) | 1.25 | (0.45–3.50) | 0.672 |
| BMI > 35 (n, %) | 0 (0.0%) | 3 (0.5%) | - | ||
| ASA (score; n, %) | |||||
| 1&2 | 4 (25%) | 95 (16%) | Reference | ||
| 3 | 9 (56%) | 351 (59%) | 0.61 | (0.19–2.00) | 0.416 |
| 4 & 5 | 3 (19%) | 152 (25%) | 0.48 | (0.11–2.17) | 0.342 |
| Fracture Pattern (type; n, %) | |||||
| 2.2 | 10 (63%) | 442 (74%) | Reference | ||
| 2.3 | 3 (19%) | 74 (12%) | 1.81 | (0.50–6.59) | 0.371 |
| 3.3 | 3 (19%) | 85 (14%) | 1.58 | (0.44–5.74) | 0.485 |
| Calcar length (mm; mean, SD) | 58 (±33) | 48 (±22) | 1.02 | (1.00–1.04) | 0.117 |
| Post-operative Full Weight-Bearing (n, %) | 16 (100%) | 297/309 * (96%) | - | ||
| Technical Factors | |||||
| Tip-Apex Distance (mm; mean, SD) | 20 (±4.3) | 18 (±5.2) | 1.06 | (0.99–1.13) | 0.102 |
| calTAD (mm; mean, SD) | 24 (±5.6) | 23 (±4.9) | 1.03 | (0.93–1.14) | 0.531 |
| TADcalTAD (mm; mean, SD) | 44 (±7.4) | 41 (±9.2) | 1.03 | (0.99–1.06) | 0.149 |
| Proximal Engagement (Y; n, %) | 13 (81%) | 508 (85%) | 0.78 | (0.22–2.76) | 0.702 |
| Lateral Engagement (Y; n, %) | 15 (94%) | 497 (83%) | 3.09 | (0.41–23.58) | 0.276 |
| Locked Distally (Y; n, *) | 16 (100%) | 599 (100%) | - | ||
| Varus Malreduction (Y; n, %) | 0 (0.0%) | 30 (5.0%) | - | ||
| Cleveland 5 or 8 (Y; n, %) | 15 (94%) | 544 (91%) | 1.55 | (0.21–11.46) | 0.670 |
| Nail Length (long; n, %) | 6 (37%) | 215 (36%) | 1.09 | (0.40–3.00) | 0.866 |
| Nail Length Interactions | |||||
| Medial Calcar Fragment by Nail Length (mm) | |||||
| Short | 52 (±23) | 43 (±16) | 1.02 | (0.99–1.06) | 0.162 |
| Long | 66 (±46) | 57 (±27) | 1.02 | (0.99–1.04) | 0.139 |
| Fractures Pattern by Nail Length (n, %) | |||||
| 2.2 Short | 9 (2.6%) | 333 (97%) | Reference | ||
| Long | 1 (0.9%) | 109 (99%) | 0.34 | (0.04–2.69) | 0.309 |
| 2.3 Short | 1 (2.1%) | 46 (98%) | Reference | ||
| Long | 2 (6.7%) | 28 (93%) | 3.29 | (0.30–35.82) | 0.327 |
| 3.3 Short | 0 (0%) | 7 (100%) | Reference | ||
| Long | 3 (3.7%) | 78 (96%) | - | - | - |
References
- Johansen, A.; Golding, D.; Brent, L.; Close, J.; Gjertsen, J.E.; Holt, G.; Hommel, A.; Pedersen, A.B.; Röck, N.D.; Thorngren, K. Using national hip fracture registries and audit databases to develop an international perspective. Injury 2017, 48, 2174–2179. [Google Scholar] [CrossRef] [PubMed]
- Whitehouse, M.R.; Berstock, J.R.; Kelly, M.B.; Gregson, C.L.; Judge, A.; Sayers, A.; Chesser, T.J. Higher 30-day mortality associated with the use of intramedullary nails compared with sliding hip screws for the treatment of trochanteric hip fractures. Bone Jt. J. 2019, 101-B, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Palm, H.; Jacobsen, S.; Sonne-Holm, S.; Gebuhr, P.; Hip Fracture Study, G. Integrity of the lateral femoral wall in intertrochanteric hip fractures: An important predictor of a reoperation. J. Bone Jt. Surg. Am. 2007, 89, 470–475. [Google Scholar]
- Physicians RCo. National Hip Fracture Database (NHFD) Annual Report 2017; Physicians RCo: London, UK, 2017. [Google Scholar]
- Meinberg, E.G.; Agel, J.; Roberts, C.S.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium-2018. J. Orthop. Trauma 2018, 32 (Suppl. 1), S1–S170. [Google Scholar] [CrossRef]
- Knobe, M.; Gradl, G.; Ladenburger, A.; Tarkin, I.S.; Pape, H.C. Unstable intertrochanteric femur fractures: Is there a consensus on definition and treatment in Germany? Clin. Orthop. Relat. Res. 2013, 471, 2831–2840. [Google Scholar] [CrossRef] [Green Version]
- Eberle, S.; Bauer, C.; Gerber, C.; von Oldenburg, G.; Augat, P. The stability of a hip fracture determines the fatigue of an intramedullary nail. Proc. Inst. Mech. Eng. Part H 2010, 224, 577–584. [Google Scholar] [CrossRef]
- Do, J.H.; Kim, Y.S.; Lee, S.J.; Jo, M.L.; Han, S.K. Influence of fragment volume on stability of 3-part intertrochanteric fracture of the femur: A biomechanical study. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 371–377. [Google Scholar] [CrossRef]
- Marmor, M.; Liddle, K.; Pekmezci, M.; Buckley, J.; Matityahu, A. The effect of fracture pattern stability on implant loading in OTA type 31-A2 proximal femur fractures. J. Orthop. Trauma 2013, 27, 683–689. [Google Scholar] [CrossRef]
- Ren, H.; Ao, R.; Wu, L.; Jian, Z.; Jiang, X.; Yu, B. Effect of lesser trochanter posteromedial wall defect on the stability of femoral intertrochanteric fracture using 3D simulation. J. Orthop. Surg. Res. 2020, 15, 242. [Google Scholar] [CrossRef] [PubMed]
- Ciufo, D.J.; Zaruta, D.A.; Lipof, J.S.; Judd, K.T.; Gorczyca, J.T.; Ketz, J.P. Risk Factors Associated With Cephalomedullary Nail Cutout in the Treatment of Trochanteric Hip Fractures. J. Orthop. Trauma 2017, 31, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, J.; Cohen, E.; Vopat, B.G.; Kane, P.; Abbood, E.; Born, C. Complications of short versus long cephalomedullary nail for intertrochanteric femur fractures, minimum 1 year follow-up. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 665–670. [Google Scholar] [CrossRef]
- Kleweno, C.; Morgan, J.; Redshaw, J.; Harris, M.; Rodriguez, E.; Zurakowski, D.; Vrahas, M.; Appleton, P. Short versus long cephalomedullary nails for the treatment of intertrochanteric hip fractures in patients older than 65 years. J. Orthop. Trauma 2014, 28, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Abram, S.G.; Pollard, T.C.; Andrade, A.J. Inadequate ’three-point’ proximal fixation predicts failure of the Gamma nail. Bone Jt. J. 2013, 95-B, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Boone, C.; Carlberg, K.N.; Koueiter, D.M.; Baker, K.C.; Sadowski, J.; Wiater, P.J.; Nowinski, G.; Grant, K. Short versus long intramedullary nails for treatment of intertrochanteric femur fractures (OTA 31-A1 and A2). J. Orthop. Trauma 2014, 28, e96–e100. [Google Scholar] [CrossRef]
- Hou, Z.; Bowen, T.R.; Irgit, K.S.; Matzko, M.E.; Andreychik, C.M.; Horwitz, D.S.; Smith, W.R. Treatment of pertrochanteric fractures (OTA 31-A1 and A2): Long versus short cephalomedullary nailing. J. Orthop. Trauma 2013, 27, 318–324. [Google Scholar] [CrossRef]
- Hulet, D.A.; Whale, C.S.; Beebe, M.J.; Rothberg, D.L.; Gililland, J.M.; Zhang, C.; Presson, A.; Stuart, A.; Kubiak, E. Short Versus Long Cephalomedullary Nails for Fixation of Stable Versus Unstable Intertrochanteric Femur Fractures at a Level 1 Trauma Center. Orthopedics 2019, 42, e202–e209. [Google Scholar] [CrossRef]
- Bjorgul, K.; Reikeras, O. Outcome after treatment of complications of Gamma nailing: A prospective study of 554 trochanteric fractures. Acta Orthop. 2007, 78, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Horner, N.S.; Samuelsson, K.; Solyom, J.; Bjorgul, K.; Ayeni, O.R.; Ostman, B. Implant-Related Complications and Mortality After Use of Short or Long Gamma Nail for Intertrochanteric and Subtrochanteric Fractures: A Prospective Study with Minimum 13-Year Follow-up. JB JS Open Access. 2017, 2, e0026. [Google Scholar] [CrossRef]
- Okcu, G.; Ozkayin, N.; Okta, C.; Topcu, I.; Aktuglu, K. Which implant is better for treating reverse obliquity fractures of the proximal femur: A standard or long nail? Clin. Orthop. Relat. Res. 2013, 471, 2768–2775. [Google Scholar] [CrossRef] [Green Version]
- Shannon, S.F.; Yuan, B.J.; Cross, W.W., III; Barlow, J.D.; Torchia, M.E.; Holte, P.K.; Sems, S. Short Versus Long Cephalomedullary Nails for Pertrochanteric Hip Fractures: A Randomized Prospective Study. J. Orthop. Trauma 2019, 33, 480–486. [Google Scholar] [CrossRef]
- Williams, N.; Hardy, B.M.; Tarrant, S.; Enninghorst, N.; Attia, J.; Oldmeadow, C.; Balogh, Z. Changes in hip fracture incidence, mortality and length of stay over the last decade in an Australian major trauma centre. Arch. Osteoporos. 2013, 8, 150. [Google Scholar] [CrossRef] [PubMed]
- Registry AaNZHF. Annual Report of Hip Fracture Care 2020; Registry AaNZHF: Sydney, Australia, 2020. [Google Scholar]
- Elliott, D.S.; Newman, K.J.; Forward, D.P.; Hahn, D.M.; Ollivere, B.; Kojima, K.; Handley, R.; Rossiter, N.; Wixted, J.; Smith, M.; et al. A unified theory of bone healing and nonunion: BHN theory. Bone Jt. J. 2016, 98-B, 884–891. [Google Scholar] [CrossRef] [Green Version]
- Cleveland, M.; Bosworth, D.M.; Thompson, F.R.; Wilson, H.J., Jr.; Ishizuka, T. A ten-year analysis of intertrochanteric fractures of the femur. J. Bone Jt. Surg. Am. 1959, 41-A, 1399–1408. [Google Scholar] [CrossRef]
- Kashigar, A.; Vincent, A.; Gunton, M.J.; Backstein, D.; Safir, O.; Kuzyk, P.R. Predictors of failure for cephalomedullary nailing of proximal femoral fractures. Bone Jt. J. 2014, 96-B, 1029–1034. [Google Scholar] [CrossRef]
- Aicale, R.; Maffulli, N. Greater rate of cephalic screw mobilisation following proximal femoral nailing in hip fractures with a tip-apex distance (TAD) and a calcar referenced TAD greater than 25 mm. J. Orthop. Surg. Res. 2018, 13, 106. [Google Scholar] [CrossRef] [Green Version]
- Johnson, N.A.; Uzoigwe, C.; Venkatesan, M.; Burgula, V.; Kulkarni, A.; Davison, J.N.; Ashford, R.U. Risk factors for intramedullary nail breakage in proximal femoral fractures: A 10-year retrospective review. Ann. R. Coll. Surg. Engl. 2017, 99, 145–150. [Google Scholar] [CrossRef]
- Tsai, S.W.; Lin, C.J.; Tzeng, Y.H.; Lin, C.C.; Huang, C.K.; Chang, M.C.; Chiang, C. Risk factors for cut-out failure of Gamma3 nails in treating unstable intertrochanteric fractures: An analysis of 176 patients. J. Chin. Med. Assoc. 2017, 80, 587–594. [Google Scholar] [CrossRef]
- Guo, X.F.; Zhang, K.M.; Fu, H.B.; Cao, W.; Dong, Q. A comparative study of the therapeutic effect between long and short intramedullary nails in the treatment of intertrochanteric femur fractures in the elderly. Chin. J. Traumatol. 2015, 18, 332–335. [Google Scholar] [CrossRef]
- Miedel, R.; Tornkvist, H.; Ponzer, S.; Tidermark, J. Musculoskeletal function and quality of life after an unstable trochanteric fracture treated with the trochanteric gamma nail. Arch. Orthop. Trauma Surg. 2012, 132, 1495–1503. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.; Kusnezov, N.; Bader, J.; Waterman, B.R.; Orr, J.; Belmont, P.J. Long versus short cephalomedullary nail for trochanteric femur fractures (OTA 31-A1, A2 and A3): A systematic review. J. Orthop. Traumatol. Off. J. Ital. Soc. Orthop. Traumatol. 2016, 17, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Sun, Q.; Ge, W.; Hu, H.; Li, G.; Wu, J.; Lu, G.; Cai, M. The Influence of Position of the Displaced Lesser Trochanter on Clinical Outcome of Unstable Trochanteric Femur Fractures in the Elderly. Biomed Res. Int. 2018, 2018, 5013646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.W.; Kent, W.T.; Yoon, Y.C.; Kim, Y.; Kim, H.; Jha, A.; Durai, S.K.; Oh, J. Fracture morphology of AO/OTA 31-A trochanteric fractures: A 3D CT study with an emphasis on coronal fragments. Injury 2017, 48, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Bojan, A.J.; Beimel, C.; Speitling, A.; Taglang, G.; Ekholm, C.; Jonsson, A. 3066 consecutive Gamma Nails. 12 years experience at a single centre. BMC Musculoskelet. Disord. 2010, 11, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gausden, E.B.; Sin, D.; Levack, A.E.; Wessel, L.E.; Moloney, G.; Lane, J.M.; Lorich, D.G. Gait Analysis After Intertrochanteric Hip Fracture: Does Shortening Result in Gait Impairment? J. Orthop. Trauma 2018, 32, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.D.; Ngo, L.; Samelson, E.J.; Kiel, D.P. Competing risk of death: An important consideration in studies of older adults. J. Am. Geriatr. Soc. 2010, 58, 783–787. [Google Scholar] [CrossRef] [Green Version]




| Medial Calcar Loss (mm) | All Patients | Short Nail | Long Nail |
|---|---|---|---|
| (n = 617) | (n = 396) | (n = 221) | |
| All fracture types (n = 617) | 48 (±22) | 43 (±16) | 57 (±27) |
| Subtypes | |||
| 2.2 (n = 452) | 48 (±19) | 44 (±16) | 60 (±23) |
| 2.3 (n = 77) | 48 (±19) | 40 (±17) | 57 (±27) |
| 3.3 (n = 88) | 52 (±32) | 33 (±9.0) | 53 (±33) |
| Failure Mode | Total (n = 617) | Short (n = 396) | Long (n = 221) |
|---|---|---|---|
| Screw Cut-out | 2 (0.2%) | 2 (0.5%) | 0 (0%) |
| Implant Breakage (Delayed Union) | 3 (0.3%) | 1 (0.3%) | 2 (0.9%) |
| Fracture Distal to Implant | 3 (0.3%) | 3 (0.8%) | 0 (0%) |
| Peri-implant Fracture | 4 (0.6%) | 1 (0.3%) | 3 (1.3%) |
| Non-union | 4 (0.6%) | 3 (0.8%) | 1 (0.5%) |
| Independent Variable | SHR | CI 95% | p | Coefficient | Standard Error |
|---|---|---|---|---|---|
| Age (years) | 0.91 | (0.86–0.96) | 0.001 | −0.10 | 0.03 |
| Tip-Apex Distance (mm) | 1.04 | (0.97–1.11) | 0.270 | 0.04 | 0.04 |
| Calcar Length & Nail Length (mm) | |||||
| Short Nail | 1.03 | (0.98–1.07) | 0.204 | 0.03 | 0.02 |
| Long Nail | 0.98 | (0.93–1.04) | 0.518 | −0.02 | 0.03 |
| Fracture Pattern & Nail Length | |||||
| 2.2 Short Nail | Reference | ||||
| Long Nail | 0.65 | (0.01–32.24) | 0.830 | −0.43 | 1.30 |
| 2.3 Short Nail | 1.05 | (0.11–9.61) | 0.967 | 0.05 | 1.18 |
| Long Nail | 11.14 | (0.44–280.80) | 0.143 | 2.41 | 18.35 |
| 3.3 Short Nail | - | ||||
| Long Nail | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarrant, S.M.; Graan, D.; Tarrant, D.J.; Kim, R.G.; Balogh, Z.J. Medial Calcar Comminution and Intramedullary Nail Failure in Unstable Geriatric Trochanteric Hip Fractures. Medicina 2021, 57, 338. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57040338
Tarrant SM, Graan D, Tarrant DJ, Kim RG, Balogh ZJ. Medial Calcar Comminution and Intramedullary Nail Failure in Unstable Geriatric Trochanteric Hip Fractures. Medicina. 2021; 57(4):338. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57040338
Chicago/Turabian StyleTarrant, Seth M., David Graan, Drew J. Tarrant, Raymond G. Kim, and Zsolt J. Balogh. 2021. "Medial Calcar Comminution and Intramedullary Nail Failure in Unstable Geriatric Trochanteric Hip Fractures" Medicina 57, no. 4: 338. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57040338